
Abstract
Background
Cardiovascular disease (CVD) is a significant contributor to morbidity and mortality worldwide, with CVD and post-acute COVID-19 associated CVD increasing. It remains unknown whether COVID-19 patients with weight gain are at a high risk for CVD events. Therefore, the primary objective of this study is to investigate the association between weight control and the risk of CVD following COVID-19.
Methods
The study included 2,024,728 adults who participated in two rounds of health screening between 2017 and 2020. The final cohort, which included 70,996 participants in the COVID-19 group and 212,869 participants in the control group. The adjusted hazard ratio of BMI change to CVD risk was calculated using Cox proportional hazards regression.
Results
We identified a total of 2869 cases of CVD (861 events for COVID-19 group and 2,008 events for the control group). Compared to individuals with a stable BMI, COVID-19 patients without obesity had an increased risk of CVD (adjusted hazard ratio [aHR] = 2.28; 95% confidence interval [CI], 1.15–4.53; p-value = 0.018). Additionally, non-COVID-19 patients with obesity also exhibited a higher risk of CVD (aHR = 1.58; 95% CI, 1.01–2.47; p-value = 0.046).
Conclusion
In conclusion, people who gained weight during the pandemic, regardless of their weight category, had a significantly higher risk of CVD associated with COVID-19 compared to those who maintained their weight before the pandemic.
Similar content being viewed by others


Introduction
Cardiovascular disease (CVD) is one of the largest contributors to morbidity and mortality worldwide [1]. CVD accounts for 40.8 million disability-adjusted life years (DALYs) each year in the Americas, which measure the years of healthy life lost due to disease or death [2], and CVD, including coronary heart disease (CHD) and stroke associated with post-acute COVID-19, is steadily increasing [3]. A higher risk of death and incident CVD from 30 days after the diagnosis of COVID-19 until 4 months was found associated with COVID-19 [4, 5].
Along with traditional and novel risk factors for COVID-19-related CVD, obesity is a major public health concern associated with an increased risk of CVD [6]. It has been a growing epidemic over the past 50 years, resulting in enormous healthcare costs of over $700 billion annually and a high association with developing diabetes, CVD, hypertension, and hyperlipidemia [7]. The updated American Heart Association (AHA) Scientific Statement on Obesity and CVD and the European Heart Association (ESC) Expert Position Report highlight the detrimental effects of obesity on cardiovascular health, independently of other cardiovascular risk factors [6]. Although the underlying biological mechanisms and predisposing risk factors that lead to cardiovascular sequelae in COVID-19 survivors are not yet fully understood [8], a prospective cohort study in the UK identified systemic inflammation and obesity as possible factors associated with long-term COVID-19 sequelae [9].
The obesity paradox is supported by empirical studies demonstrating that among patients with acute myocardial infarction, atrial fibrillation, and coronary artery disease, people with overweight or obesity have a lower risk of death from CVD than those with normal weight [10,11,12]. These studies suggest that obesity may have a protective effect on some cardiovascular outcomes, but the mechanisms and implications of this effect are not fully understood. There are multiple types of weight gain, such as an increase in body fat distribution and weight gain after smoking cessation rather than just an increase in BMI, that may derive differential risks of CVD. However, there is limited evidence regarding the types of weight gain and cardiovascular outcomes in relation to weight gain in patients with COVID-19.
To address this evidence gap, we investigated the association of weight management with the risk of CVD after COVID-19 using a nationwide cohort.
Methods
Study design
Through the requirement of health insurance enrollment, the Korean National Health Insurance Service (NHIS) covers 97.2% of the country's population [13]. When the medical expenses are invoiced to it by medical institutions, every medical record—including health screening, qualifying, and treatment records—is gathered into the NHIS database. Only authorized researchers have access to the NHIS's gathered health-related data for any relevant study. Other descriptions of NHIS are provided elsewhere [14]. In order to actively advance the scientific basis for the prevention and treatment of infectious diseases, including COVID-19, the NHIS and the Korea Disease Control and Prevention Agency (KDCA) have established the K-COV-N cohort and matched COVID-19 patients to non-COVID-19 patients using propensity scores derived from age and sex and matched to a 1:10 ratio. Therefore, the 6.3 million people in the K-COV-N cohort data have the following characteristics: (1) demographic data (age, gender, income), medical data (diagnosis, treatment, drug prescriptions, interventions), health-related behavior (alcohol, smoking, exercise), and other clinical data from health screenings (serological data, anthropometric measurements) obtained between January 1, 2009, and December 31, 2021; (2) data on COVID-19 patients (age, sex, confirmed date, and transmission route).
Study population
Participants in the South Korean health screening must be 20 years of age or older. Those who participated in both health screenings between period I (2017–2018) and period II (2019–2020) were initially included in the analysis (n = 2,024,728). Those who developed SARS-CoV-2 in 2021 were included in the COVID-19 group (n = 162,976), whereas those who did not receive a diagnosis of SARS-CoV-2 infection until December 31, 2021 were included in the control group (n = 1,849,462). The participants were exactly matched to a 1:3 ratio using age, sex, income, and Charlson Comorbidity Index (CCI) between the COVID-19 group and the control group. The income level was calculated by their monthly premium and was categorized as upper half or lower half. The International Classification of Diseases, 10th edition (ICD-10) codes used in the NHIS diagnosis data were used to determine CCI, which was then categorized as 0, 1, or 2. [15]. As a result, 81,273 participants of the COVID-19 group and 243,819 participants of the control group were matched. The index date was chosen for the COVID-19 group as the confirmed date of SARS-CoV-2 infection, and the matched control subjects used the same date. To avoid bias in the examination of the association, those with underweight (BMI < 18.5 kg/m2) from the COVID-19 (n = 1,752) and the control group (n = 6,055) were excluded [16]. Additionally, those with a history of CVD before the follow-up period were eliminated from the COVID-19 (n = 3,153) and control (n = 9,012) groups. Moreover, participants with pregnancy (n = 1,315), eating disorders (n = 52), sleep disorders (n = 3,615), other variables (n = 390) were not included in the COVID group. The participants from the control group excluded those with pregnancy (n = 3,438), eating disorders (n = 157), sleep disorders (n = 10,923), other variables (n = 1,225), or died before the follow-up (n = 140). Pregnancy, eating disorder, and sleep disorder was defined by the ICD-10 code of O, F50, F51, respectively. Finally, the analytic cohort contained 70,996 participants from the COVID-19 group and 212,869 participants from the control group (Fig. 1). This study was carried out in accordance with the STROBE recommendations and authorized by the Institutional Review Board of CHA University Hospital (No.: CHAMC 2022–05-052) [17]. The anonymity of the K-COV-N cohort data allowed for the waiver of the informed consent requirements.

Flow diagram for the inclusion of study population
Exposures
BMI was measured by the weight (kg) divided by the height in meters squared from the biennial health screenings. Changes in BMI was defined by subtracting the BMI value from period II to I. If the change was within 1 kg/m2, we classified it as BMI stable. If the change was > 1 kg/m2 or > −1 kg/m2 then it was classified as BMI gain or BMI loss, respectively. In addition, to analyze the association of various factors that influence weight gain, we additionally calculated muscle mass index and fat mass index based on age, height, weight, waist circumference, and serum creatinine [9]. Therefore, the increase in muscle mass index and fat mass index was defined by the measurement from each period.
Outcomes
The primary result of this study was an incident CVD after diagnosis of COVID-19. The incident CVD was defined based on the ICD-10 codes with at least 2 day of hospital admission or visit. The composite CVD events included any coronary heart disease (CHD; I20-I25) or stroke (I60-I69) occurrences [18]. Previous studies used same definition with our study using the NHIS database [19].
Key variables
Age, sex, income, physical activity, alcohol consumption, smoking status, history of hypertension, diabetes mellitus, dyslipidemia, and CCI score from period II were used as covariates. Smoking status was categorized as current, former, and non-smoker. Alcohol consumption was categorized as a drinker or a non-drinker. Physical activity was calculated based on the frequency (day) of moderate- or vigorous-physical activity per week. The history of hypertension, diabetes, and dyslipidemia was defined by the record from medical experts during health screenings.
Statistical analysis
To investigate the association of post COVID-19 CVD risk with weight change, we analyzed the association between BMI changes from period I (2017–2018) to period II (2019–2020) and the risk of CVD stratified by the diagnosis of COVID-19 and obesity. The participants with obesity were defined as those with BMI ≥ 25 kg/m2 following the Asia criteria of World Health Organization [16]. The eligible participants were followed-up from each index date until any event CVD diagnosis, death, or December 31, 2021, whichever happened first. For each continuous or categorical variable, the mean (standard deviation [SD]) or n (%) were provided, respectively. To compare the difference between groups, independent t-test analysis for continuous variables and chi-squared test for categorical data were used. In the primary analysis, we used Cox proportional hazard regression to determine the hazard ratio of BMI change with post COVID-19 CVD risk. The participants with stable BMI were used as reference value. Plotting the scaled Schoenfeld residuals were tested for a visual evaluation of the Cox regression model's proportionality assumption. In order to reduce the upwardly skewed risk estimates, we additionally computed subdistribution hazard ratio (sHR) using Fine-Gray subdistribution hazard model regression. The competing event was established as a pre-CVD death that occurred at least one month after SARS-CoV-2 infection, while the event of interest was set as an incident CVD. All covariates including age, sex, income, CCI, alcohol consumption, smoking status, history of diabetes mellitus, hypertension, and dyslipidemia were adjusted for the regression models. The regression models were stratified as follows: (1) COVID-19 patients without obesity, (2) COVID-19 patients with obesity, (3) non-COVID-19 patients without obesity, (4) non-COVID-19 patients with obesity. Both the sHR and the adjusted hazard ratio (aHR) were rounded to two decimal places. In addition, the participants that have factors that influence BMI gain (physical activity [active or inactive], comorbidity [no or moderate], increase in muscle mass index and fat mass index) were compared with those with stable BMI. To evaluate subgroup differences, we stratified the risk by age (65 or 65), history of hypertension (yes or no), diabetes (yes or no), and dyslipidemia (yes or no). All reported P values were two-sided and P values of < 0.05 were considered as statistically significant. All statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC).
Results
Baseline characteristics
We identified 70,996 COVID-19 group and 212,869 control group in the analytic cohort. After the exclusion, there were 285 incident post COVID-19 CVD occurred from the analytic cohort. The mean BMI at period II was 24.8 (3.3) and 24.6 (3.3) for COVID-19 and no COVID-1 group, respectively. Similarly, the mean BMI at period I was 24.6 (3.3) and 24.4 (3.3) for COVID-19 and no COVID-1 group, respectively. The participants with COVID-19 exhibited higher physical activity levels, lower smoking rates, and a higher prevalence of hypertension, diabetes, and dyslipidemia history. However, these differences were not significant. The observed statistical significance seems attributable to the exceptionally large sample size. However, this minor difference implies little bias in the selection of the non-COVID-19 control group. Other baseline characteristics of two groups are described in Table 1.
The unexpectedly higher smoking rate of 16.8% in the non-COVID-19 group compared to 11.8% in the COVID-19 group contradicts expectations given smoking's substantial risk factor status for COVID-19 infection. Smokers may be less likely to seek medical attention or get tested for COVID-19, either because they have milder symptoms, or because they fear stigma or discrimination [20]. This could result in underreporting bias regarding the prevalence of smoking among COVID-19 patients. Therefore, the complete SARS-CoV-2 positivity rate among smokers in the entire dataset might have been underestimated owing to incomplete smoking status data. Moreover, bias in selection might influence the outcomes since smokers are prone to respiratory symptoms such as cough, expectoration, and sore throat, potentially prompting more frequent testing and a higher proportion of smokers showing negative SARS-CoV-2 results [21].
Association of changes in BMI with risk of overall cardiovascular disease in the post COVID-19
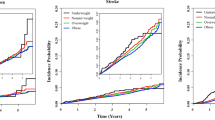
Compared to those with stable BMI, those with BMI gain among COVID-19 patients without obesity (aHR, 2.28; 95% CI, 1.15–4.53; P value 0.018;) and non-COVID-19 patients with obesity (aHR, 1.58; 95% CI, 1.01–2.47; P value 0.046; Fig. 2) showed an increased risk of CVD. However, the results of the competing risk analysis only maintained the association with the participants among COVID-19 patients without obesity (sHR, 2.21; 95% CI, 1.11–4.41; P value 0.024; Fig. 3). This seems to be linked to a low occurrence rate of actual CVD events. To prevent an overestimation of the incidence rate of the event of interest in competing risk analysis, the cumulative incidence function is used, which requires an adequate number of observations for estimation [22]. If the incidence rate of a particular event is extremely low, the estimation of the cumulative incidence function for that event can become unstable, leading to wider confidence intervals [23, 24]. Consequently, it might be challenging to identify statistically significant differences. The association with coronary heart disease and stroke was not significant with BMI change (Additional file 1: Table S2).

Forest plot of hazard ratios estimated by the BMI change with the risk of cardiovascular disease stratified by the diagnosis of COVID-19 and obesity. Adjusted hazard ratio was calculated using Cox proportional hazards regression after adjustments for age, household income, hypertension, diabetes mellitus, dyslipidemia, smoking, alcohol consumption, physical activity and the Charlson comorbidity index. COVID-19, coronavirus disease 2019; HR, hazard ratio; CI, confidence interval; aHR, adjusted hazard ratio

Forest plots of subdistribution hazard ratios estimated by the BMI change with the risk of cardiovascular disease stratified by the diagnosis of COVID-19 and obesity. Adjusted hazard ratio was calculated using Cox proportional hazards regression after adjustments for age, household income, hypertension, diabetes mellitus, dyslipidemia, smoking, alcohol consumption, physical activity and the Charlson comorbidity index. COVID-19, coronavirus disease 2019; HR, hazard ratio; CI, confidence interval; aHR, adjusted hazard ratio
Association of changes in BMI with risk of overall cardiovascular disease in the post COVID-19 by various factors influencing BMI gain
Among those with COVID-19 patients without obesity, those who were physically inactive (aHR, 3.23; 95% CI, 1.26–8.29; P value 0.015), moderate comorbidities (aHR, 3.72; 95% CI, 1.68–8.26; P value 0.001), increased muscle mass index (aHR, 2.33; 95% CI, 1.17–4.63; P value 0.016), and increased fat mass index (aHR, 2.31; 95% CI, 1.16–4.59; P value 0.017) showed an increased risk for CVD. Similarly, among those with no-COVID-19-obese, those with moderate comorbidities (aHR, 1.89; 95% CI, 1.10–3.26; P value 0.022; Additional file 1: Table S3) and increased muscle mass index (aHR, 1.57; 95% CI, 1.00–2.45; P value 0.049; Table 2) showed an increased risk for CVD.
Subgroup analyses
Subgroup analyses were conducted by stratifying age, hypertension, diabetes, and dyslipidemia. The trend of increased CVD risk among COVID-19 patients without obesity was maintained with those with hypertension (aHR, 3.14; 95% CI, 1.31–7.52; P value 0.010; Additional file 1: Table S4). However, no significant differences were detected by other subgroups or other participant groups.
Discussion
In individuals without obesity, who have COVID-19, the risk of developing CVD after COVID-19 in the group exposed to weight gain was significantly higher by 2.28 times compared to the weight maintenance group. On the other hand, in people with obesity without COVID-19, the risk of CVD incidence in the group exposed to weight gain was significantly higher by 1.58 times compared to the weight maintenance group. COVID-19 and obesity are both risk factors for CVD with established evidence. Even in people without obesity, weight gain can increase the risk of CVD, so it is important to manage your weight well. The results were consistent even in individuals with obesity, who do not have COVID-19. Moreover, the risk of CVD after COVID-19 appears to be higher among individuals without obesity who gain weight compared to those who maintain their weight. However, since obesity is a known risk factor for CVD incidence, the risk of developing CVD in the weight gain group of individuals with obesity compared to the weight maintenance group is relatively lower than that in individuals without obesity. Therefore, people who gained weight before COVID-19, whether obese or not, may be a high-risk group exposed to long-term CVD risk.
Our findings that COVID-19 patients who gained weight had a higher risk of CVD compared to those who maintained their weight, are in line with the well-established evidence linking weight gain to an increased risk of CVD. A study involving 73,435 non-hospitalized patients utilizing the health services of the US Department of Veterans Affairs revealed that all subgroups, including individuals with obesity, are at a higher risk of developing CVD after being infected with COVID-19 [3]. Furthermore, the group without obesity had a higher hazard ratio than the people with obesity when compared to the contemporary control group in terms of developing CVD after being infected with COVID-19 [25].
Chen et al. (2023) conducted a long-term cardiovascular study and found that COVID-19 did not increase the risk of CVD events, including heart failure, stroke, and myocardial infarction, despite adjusting for potential confounding factors such as age, gender, co-morbidities, and medications. However, the study did find a higher risk of CVD events among people who had obesity or diabetes before contracting COVID-19 [25]. Another study, which used data from the American Heart Association COVID-19 Cardiovascular Disease Registry, indicated that COVID-19 patients with obesity or had a higher BMI were more susceptible to cardiovascular events [26]. Nevertheless, the study did not address the combined impact of weight gain and CVD risk resulting from the complex interaction of factors such as various health behaviors, medical history, and weight categories associated with weight gain. In addition, previous studies mainly focused only on adults with overweight or obesity and did not consider weight change as a risk factor for CVD after COVID-19 in various populations, including populations without obesity [27].
The mechanism of weight gain and CVD risk is complicated and involves multiple factors [28], which is why people who are exposed to weight gain have a higher risk of developing CVD when infected with COVID-19 compared to those who maintain their weight. COVID-19 and CVD have a bidirectional relationship, but the exact cause of this interaction is not yet fully understood [29]. High levels of systemic inflammation due to COVID-19 can increase pre-existing CVD risk or cause new cardiovascular damage [18, 30]. COVID-19 is thought to cause inflammation and damage to the endothelial cells that line blood vessels, leading to blood clots that can cause heart attacks and strokes [31]. Studies conducted on animals suggest that ACE2, a surface protein that allows the virus to enter cells, and part of the renin–angiotensin–aldosterone system (RAAS), may be involved in this interaction [18, 30, 32].
Weight gain can increase the risk of developing CVD in general [33]. The mechanism of weight gain and CVD risk is complicated and involves multiple factors [6]. Our analysis of the NHIS cohort further extends the evidence for cardiovascular risk after COVID-19 associated with weight gain before COVID-19, using large population-level data and ascertained CVD events in the general population, including people with obesity.
A recent joint opinion from the World Heart Federation, American College of Cardiology, AHA, and the ESC emphasize that it is essential to provide unambiguous public health advice and strictly follow COVID-19 prevention procedures among all individuals with obesity [34]. The weight gain of individuals who are overweight or have a normal weight is not originally a major focus of research, unlike for individuals with obesity. However, our study stratified the population into two groups based on the risk factor of BMI(those with obesity and those without obesity) increase along with the CVD risk associated with COVID-19, and compared the risk of CVD due to weight gain with that of a group that maintained their weight. We suggest the importance of weight management for primary prevention of long-term CVD risk due to COVID-19 even in populations without obesity. The observational nature of our study prevents a definitive conclusion on the causal relationship between weight gain exposure, COVID-19, and CVD risk in the overall population, including obesity. Therefore, evidence for the effectiveness of weight management to alleviate CVD risk in population stratified by obesity status and COVID-19 needs to be further supported by controlled randomized studies.
Limitations
We studied COVID-19’s long-term effects using real-world data, but had limitations. We couldn't gather individual weight change post-COVID-19 due to inconsistent body weight measurements, potentially causing errors and biases in estimating weight change and its link to cardiovascular outcomes. Utilizing pre-pandemic weight gain data from the last two years may not fully reflect the pandemic's impact on weight change and cardiovascular risk, potentially affecting our estimates of their association. Additionally, the follow-up time and the inability to stratify by COVID type can be considered limitations. In our study, we specifically evaluated the risk of cardiovascular disease during the short-term period following COVID-19, potentially explaining the observed low incidence. The emphasis on the follow-up time in our study aligns with previous research, consistently reporting a higher risk of cardiovascular disease within the first 30 days after COVID-19 infection [35]. However, the actual incidence and relative risk of CVD after COVID-19 infection are still uncertain, as data are limited and heterogeneous. Different data sources, methods, and definitions of COVID-19 and CVD may affect the estimates and comparisons of the long-term effects of COVID-19 on cardiovascular health [36].
Defining COVID type based on respiratory symptoms may not reflect infection severity or duration. Variability in viral variants or strains affecting clinical outcomes wasn't considered, limiting study population heterogeneity and generalizability to diverse settings or populations. The study did not account for the vaccination status of the COVID-19 patients, which may affect their prognosis and cardiovascular complications. Vaccination can lower the severity and mortality of COVID-19, and may also alter the obesity-cardiovascular disease link in COVID-19 patients [37]. At a similar time, the proportion of unvaccinated individuals among those infected with COVID-19 is approximately around 40% according to previous studies [38, 39]. Our NHIS claims data study extensively controlled for confounding factors (age, sex, habits, comorbidities, medications), boosting causal inference. Our population-based study covers 97% of Koreans, has high-quality validation and robustness. However, limitations persist in real-world data, including clinical coding ambiguity, incomplete symptom capture, and biases in claims data, demanding careful consideration for a comprehensive understanding of COVID-19's long-term effects.
Conclusions
In conclusion, according to the NHIS cohort study, individuals with weight gain, including populations with overweight or obesity, as well as those with normal weight, had a significantly higher risk of developing the COVID-19-associated CVD than those who maintained their pre-pandemic weight. However, further studies are needed to evaluate the ongoing risk of COVID-19-related cardiovascular diseases resulting from weight gain in the general population. Long-term observational studies are needed for this purpose. Additionally, analyses that include other essential information such as vaccination status will be required.
Data availability
No additional data available. Only authorized researchers received permission to access the National Health Insurance Service (NHIS) database at the Big Data Research Center of the Big Data Steering Department in the Republic of Korea.
References
Faghy MA, et al. Cardiovascular disease prevention and management in the COVID-19 era and beyond: an international perspective. Prog Cardiovasc Dis. 2023;76:102–11.
Cardiovascular disease burden in the Region of the Americas, 2000–2019. ENLACE data portal. Pan American Health Organization. . 2021; https://www.paho.org/en/enlace/cardiovascular-disease-burden.
Raman B, et al. Long COVID: post-acute sequelae of COVID-19 with a cardiovascular focus. Eur Heart J. 2022;43(11):1157–72.
Al-Aly Z, Xie Y, Bowe B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature. 2021;594(7862):259–64.
Ayoubkhani D, et al. Post-covid syndrome in individuals admitted to hospital with covid-19: retrospective cohort study. BMJ. 2021;372: n693.
Powell-Wiley TM, et al. Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;143(21):e984–1010.
Panuganti KK, N.M., Kshirsagar RK., Obesity. Aug 8. In: StatPearls [Internet]. ed. T.I. (FL). Vol. 2023 Jan–. PMID. 2022, StatPearls Publishing.
Mohamed MO, Banerjee A. Long COVID and cardiovascular disease: a learning health system approach. Nat Rev Cardiol. 2022;19(5):287–8.
Clinical characteristics with inflammation profiling of long COVID and association with 1-year recovery following hospitalisation in the UK: a prospective observational study. Lancet Respir Med, 2022. 10(8): 761–775.
Elagizi A, et al. An overview and update on obesity and the obesity paradox in cardiovascular diseases. Prog Cardiovasc Dis. 2018;61(2):142–50.
Qiao S, et al. Gut Parabacteroides merdae protects against cardiovascular damage by enhancing branched-chain amino acid catabolism. Nat Metab. 2022;4(10):1271–86.
Lv Y, et al. The obesity paradox is mostly driven by decreased noncardiovascular disease mortality in the oldest old in China: a 20-year prospective cohort study. Nat Aging. 2022;2:1–8.
Kim HK, et al. Data configuration and publication trends for the korean national health insurance and health insurance review & assessment database. Diabetes Metab J. 2020;44(5):671–8.
Seong SC, et al. Cohort profile: the National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open. 2017;7(9): e016640.
Kankowski L, et al. The impact of maternal obesity on offspring cardiovascular health: a systematic literature review. Front Endocrinol (Lausanne). 2022;13: 868441.
Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet, 2004. 363(9403): 157–63.
Vandenbroucke JP, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. PLoS Med. 2007;4(10):e297.
Alexeeff SE, et al. Long-Term PM(2.5) exposure and risks of ischemic heart disease and stroke events: review and meta-analysis. J Am Heart Assoc. 2021;10(1):e016890.
Chen GC, et al. Association between regional body fat and cardiovascular disease risk among postmenopausal women with normal body mass index. Eur Heart J. 2019;40(34):2849–55.
Ryu S, et al. Prevalence and predictors of perceived COVID-19 stigma within a population-based sample of adults with COVID-19. BMC Public Health. 2023;23(1):2110.
de Lusignan S, et al. Risk factors for SARS-CoV-2 among patients in the Oxford Royal College of general practitioners research and surveillance centre primary care network: a cross-sectional study. Lancet Infect Dis. 2020;20(9):1034–42.
Schuster NA, et al. Ignoring competing events in the analysis of survival data may lead to biased results: a nonmathematical illustration of competing risk analysis. J Clin Epidemiol. 2020;122:42–8.
Austin PC, Lee DS, Fine JP. Introduction to the analysis of survival data in the presence of competing risks. Circulation. 2016;133(6):601–9.
Zhang Z. Survival analysis in the presence of competing risks. Ann Transl Med. 2016;5(3):47.
Gordon BR, et al. Light-intensity and moderate-to-vigorous intensity physical activity among older adult breast cancer survivors with obesity: a narrative review. Cancer Med. 2022;11(23):4602–11.
Hendren NS, et al. Association of body mass index and age with morbidity and mortality in patients hospitalized with covid-19: results from the american heart association COVID-19 cardiovascular disease registry. Circulation. 2021;143(2):135–44.
Iyen B, et al. Long-term body mass index changes in overweight and obese adults and the risk of heart failure, cardiovascular disease and mortality: a cohort study of over 260,000 adults in the UK. BMC Public Health. 2021;21(1):576.
Jayedi A, et al. Adult weight gain and the risk of cardiovascular disease: a systematic review and dose-response meta-analysis of prospective cohort studies. Eur J Clin Nutr. 2020;74(9):1263–75.
Nishiga M, et al. COVID-19 and cardiovascular disease: from basic mechanisms to clinical perspectives. Nat Rev Cardiol. 2020;17(9):543–58.
Madjid M, et al. Potential effects of coronaviruses on the cardiovascular system: a review. JAMA Cardiol. 2020;5(7):831–40.
Chávez-Castillo M, et al. Exploring phytotherapeutic alternatives for obesity, insulin resistance and diabetes mellitus. Curr Pharm Des. 2020;26(35):4430–43.
Ding L, et al. Smoking, heavy drinking, physical inactivity, and obesity among middle-aged and older adults in China: cross-sectional findings from the baseline survey of CHARLS 2011–2012. BMC Public Health. 2020;20(1):1062.
Husby A, Køber L. COVID-19 mRNA vaccination and myocarditis or pericarditis. Lancet. 2022;399(10342):2168–9.
Razavi AC, et al. Cardiovascular disease prevention and implications of coronavirus disease 2019: an evolving case study in the crescent city. J Am Heart Assoc. 2020;9(13): e016997.
Xie Y, et al. Long-term cardiovascular outcomes of COVID-19. Nat Med. 2022;28(3):583–90.
Zhang HG, et al. Potential pitfalls in the use of real-world data for studying long COVID. Nat Med. 2023;29(5):1040–3.
van der Klaauw AA, et al. Accelerated waning of the humoral response to COVID-19 vaccines in obesity. Nat Med. 2023;29(5):1146–54.
Lim Y, et al. Association of physical activity with SARS-CoV-2 infection and severe clinical outcomes among patients in South Korea. JAMA Netw Open. 2023;6(4): e239840.
Yoon SS, et al. Association of weight changes with SARS-CoV-2 infection and severe COVID-19 outcomes: a nationwide retrospective cohort study. J Infect Public Health. 2023;16(12):1918–24.
Acknowledgements
This study used the database of the KDCA and the NHIS for policy and academic research. The research number of this study is KDCA-NHIS-2022-1-573. The KDCA is the Korea Disease Control and Prevention Agency, Republic of Korea. The NHIS is the National Health Insurance Service, Republic of Korea. This study protocol was approved by the Institutional Review Board of CHA University Hospital (No.: CHAMC 2022-05-052)
We thank the NHIS and KDCA for sharing national cohorts for research purposes and every frontline healthcare worker for the commitment and dedication in this pandemic era.
Funding
This work was supported by the research program of the Korea Medical Institute in 2023. This work was supported by the Korean Society of Medical Informatics.
Author information
Authors and Affiliations
Contributions
Conceptualization: SKL and SJ. Data curation: SKL, SJ, and YL. Formal analysis: SKL and SJ. Methodology: SKL and SJ. Supervision: HWH. Writing – original draft: SKL and SJ. Writing – review & editing: SKL, SJ, YL, and HWH.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Institutional Review Board of CHA University Hospital (No.: CHAMC 2022–05-052).
Consent for publication
The requirement for informed consent was waived because of anonymous data retrieved from the NHIS-KDCA.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Additional tables.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lee, S.K., Lim, Y., Jeong, S. et al. COVID-19-related cardiovascular disease risk due to weight gain: a nationwide cohort study. Eur J Med Res 29, 2 (2024). https://doi.org/10.1186/s40001-023-01569-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01569-7