
Abstract
Background
Metabolic dysfunction-associated fatty liver disease (MAFLD) is the most common chronic liver disease in China. Our study aimed to evaluate the screening value of the fatty liver index (FLI), hepatic steatosis index (HSI), lipid accumulation product (LAP), visceral adiposity index (VAI), and Zhejiang University index (ZJU), as well as other single indicators for MAFLD. We aimed to find the optimal screening tool and its appropriate cut-off values for rural Uyghur adults.
Methods
We completed a survey of 14,321 Uyghur adults in 51 groups in Kashgar, Xinjiang, in 2016 using a typical sampling method, with 12,794 patients ultimately included in statistical analyses. Fatty liver was diagnosed using ultrasonography.
Results
The prevalence of fatty liver disease (FLD) and MAFLD was 16.73% and 16.55%, respectively, and the FLI, HSI, LAP, VAI, and ZJU were all independently associated with an increased risk of MAFLD. The areas under the receiver operating characteristic curves (AUCs) of the FLI for diagnosing MAFLD in men and women were 0.853 and 0.847, respectively. The AUCs of the body mass index (BMI) for diagnosing MAFLD in men and women were 0.850 and 0.852, respectively. Compared with other metabolic-related markers, FLI had the largest AUC. In men, the optimal cut-off values of FLI and BMI for diagnosing MAFLD were 45 (sensitivity 84.83%, specificity 69.57%) and 27.4 (sensitivity 78.47%, specificity 76.30%), respectively. In women, the optimal cut-off values of FLI and BMI for diagnosing MAFLD were 45 (sensitivity 80.11%, specificity 74.23%) and 28.0 (sensitivity 79.56%, specificity 75.41%), respectively. In men and women, an FLI score of < 30 ruled out MAFLD, while a score of ≥ 50 was a basis for diagnosis.
Conclusion
FLI and BMI had good screening ability for MAFLD and were superior to HSI, LAP, VAI, and ZJU in both sexes.
Similar content being viewed by others


Introduction
In 2020, non-alcoholic fatty liver disease (NAFLD) was renamed metabolic-associated fatty liver disease (MAFLD) [1]. MAFLD is a chronic disease characterized by hepatic fat accumulation and underlying metabolic dysregulation. The condition is a significant public health issue, affecting more than a quarter of adult populations worldwide [2]. Studies have shown that MAFLD induces hepatic lipotoxicity and mitochondrial dysfunction leading to hepatocyte apoptosis, inflammation, and fibrosis [3]. In addition to its close association with liver disease, MAFLD also plays an important role in the progression of various extrahepatic diseases, including cardiovascular disease, diabetes, and chronic kidney disease [4]. In China, the disease burden of MAFLD has surpassed that of other chronic liver diseases [5, 6]. However, the current diagnosis and treatment rates of MAFLD are low, and interventions geared to its harmful effects may be insufficient [7]. Therefore, to optimize the management of patients with MAFLD, simple and effective early screening tools are necessary.
Among the non-invasive indicators currently used for NAFLD screening, the fatty liver index (FLI), hepatic steatosis index (HSI), lipid accumulation product (LAP), visceral adiposity index (VAI) and Zhejiang University index (ZJU) are widely used and have been validated in different populations [8,9,10]. However, the screening value of these indices may need further verification under the new definition of MAFLD. The above indexes are established based on routine measurements in clinical practice, and compared with liver biopsy and ultrasonography, may reduce medical burdens. However, differences in the cut-off values in different populations and regions exist, and the cut-off values in previous studies may not apply to the Uyghur population in rural Xinjiang. These values may require adjustments through external verification prior to practical application.
Therefore, this study aimed to evaluate the accuracy of non-invasive indicators in diagnosing MAFLD in rural Uyghur populations in Xinjiang as well as determine their optimal cut-off values and ranges.
Materials and methods
Study population
This cross-sectional study was conducted in Kashgar, Xinjiang, from August to September 2016. Our research is based on the 51st Regiment of the Farm, which is the only regiment with Uyghurs as its main inhabitants. Using the typical sampling method, the sixth, eighth, 11th, 12th, and 13th companies of the 51st Regiment of the Farm were selected as the survey sites. The sixth, eighth, 11th, 12th, and 13th companies are one level below the farm. If farms are like towns, companies are like villages. We chose these companies with a large number of Uyghurs to carry out the investigation and research in a concentrated way. A total of 14,321 permanent Uyghur residents aged ≥ 18 years were interviewed after obtaining informed consent. We excluded a total of 1527 participants, including long-term migrants, pregnant women, those who could not cooperate with the investigation (n = 317), participants with incomplete basic information (n = 971), and participants with missing ultrasound information (n = 239). Ultimately, 12,794 participants were included in statistical analyses.
Data collection
The questionnaire survey and physical examination were conducted by uniformly trained investigators through on-site centralized interviews. The questionnaire included general demographic information, medical history, and family history. Physical examinations included height, weight, body mass index (BMI), waist circumference (WC), hip circumference (HC), systolic blood pressure (SBP), and diastolic blood pressure (DBP). Before the measurement, participants were required to remove excess clothing, hats, and shoes. Waist circumference was measured with an inelastic band at the midpoint of the line between the anterior superior iliac crest and the inferior margin of the 12th costal. Hip circumference was measured around the hip through the most prominent part of the gluteus maximus. Blood pressure was measured after participants had rested in a sitting position for 5 min. Each measurement required an interval of one minute, and the mean value after three measurements was used. These measurement methods were consistent with existing research among this group [11]. Type 2 diabetes mellitus (T2DM) was diagnosed according to the American Diabetes Association 2012 criteria [12].
Venous blood samples were collected from all participants after overnight fasting. All parameters, including fasting plasma glucose (FPG), triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), aspartate aminotransferase (AST), alanine aminotransferase (ALT), and gamma-glutamyl transferase (GGT), were measured using an automatic biochemical analyzer (Olympus Diagnostics, Hamburg, Germany) at our laboratory department.
The calculation formula used in this study was as follows:
\(\mathrm{FLI}=\frac{{\mathrm{e}}^{0.953\times \mathrm{loge }\left (\mathrm{TG}\right)+0.139\times \mathrm{BMI}+0.718\times \mathrm{loge } (\mathrm{GGT})+0.053\times \mathrm{WC }-15.745}}{1+{\mathrm{e}}^{0.953\times \mathrm{loge }\left (\mathrm{TG}\right)+0.139\times \mathrm{BMI}+0.718\times \mathrm{loge } (\mathrm{GGT})+0.053\times \mathrm{WC}-15.745} }\times 100\) [13];
HIS = 8× (ALT/AST ratio)+BMI (+2,if women; +2,if diabetes mellitus) [14];
LAP for men = (WC [cm] - 65) × (TG[mmol/L]); LAP for women = (WC [cm] - 58) × (TG [mmol/L]) [15]
ZJU = BMI (kg/m2) + FPG (mmol/L) + TG (mmol/L) + (3 × ALT/AST Ratio) (+2, If Women) [16]
VAI = (WC/ (39.68 + (1.88 × BMI)))× (TG/1.03) × (1.31/HDL-C) for Men; (WC/ (36.58 + (1.89 × BMI))) × (TG/0.81) × (1.52/HDL-C) for Women [17]
Definition of MAFLD
MAFLD [18] was defined as the presence of one of the following three criteria based on hepatic steatosis: (1) overweight/obesity (BMI ≥ 23 kg/m2); (2) presence of T2DM (FPG ≥ 7.1 mmol/L); (3) lean/normal weight (BMI < 23 kg/m2) with metabolic dysregulation. Metabolic dysregulation was defined as the presence of at least two of the following metabolic risk abnormalities: (a) WC ≥ 90/80 cm in men and women, respectively; (b) blood pressure ≥ 130/85 mmHg; (c) TG ≥ 1.70 mmol/L; (d) HDL-C < 1.0 mmol/L in men and < 1.3 mmol/L in women; (e) Prediabetes: FPG level of 5.6–6.9 mmol/L. Hepatic steatosis was determined by ultrasound examination performed by a specialist clinician.
Statistical analyses
Categorical and continuous variables were expressed as frequency (percentage) and mean ± standard deviation, respectively, and the Chi-square test and Mann–Whitney U test were used for comparison between groups. Factors influencing MAFLD were determined using univariate analyses. Except for the MAFLD components, the remaining influencing factors were included in the multivariate analyses. Logistic regression models were constructed using the step-forward method to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) for FLI, HSI, and MAFLD. The final model was adjusted for age, sex, and HC, TC, LDL-C, AST, ALT, and GGT levels. Areas under the receiver operating characteristic (ROC) curve (AUC), sensitivity, specificity, positive likelihood ratio (LR+), negative likelihood ratio (LR-), positive predictive value (PPV), negative predictive value (NPV), and Youden index were used to evaluate the screening ability of non-invasive markers for MAFLD. All analyses were performed using two-sided tests, with p < 0.05 considered statistically significant. The Delong test was used to compare whether the AUC differences of the different receiver operating characteristic (ROC) curves were statistically significant. All statistical analyses were performed using SPSS 26.0 and R 4.1.1.
Results
Basic demographic characteristics
Among the 12,794 Uyghur adults included, the mean age was 38.10 ± 14.09 years, and 6448 (50.40%) men participated. Of these patients, 2141 (16.73%) had fatty liver disease (FLD) and 2118 (16.55%) had MAFLD. Compared with the non-MAFLD group, the MAFLD group was older; had higher BMI, WC, HC, SBP, DBP, TG, TC, LDL-C, AST, ALT, GGT, FPG, FLI, HSI, LAP, VAI, and ZJU levels; included more female patients; had a higher prevalence of T2DM (all p < 0.001); and had lower HDL-C levels (p < 0.001) (Table 1).
Relationship between non-invasive indicators and MAFLD
In the interaction analysis, we considered the indicators that were not involved in the definition of liver steatosis indexes and MAFLD: age, hip circumference, total cholesterol, and sex. The results showed that the OR value was 1 for all indicators except sex. Further analyses were stratified by sex due to the interaction between steatosis indexes (FLI, HSI, LAP, VAI and ZJU) and sex on the prevalence of MAFLD (p < 0.001). After multivariate adjustment, FLI, HSI, BMI, TG, LDL-C, HC, FPG, WC, TC, AST, GGT, LAP, VAI, ZJU, ALT, and HDL-C variables remained significantly associated with MAFLD in men, while the correlation between ALT, HDL-C, and MAFLD was not statistically significant in women (p > 0.05). In both men and women, associations with LDL-C, ZJU, HC, and MAFLD were stronger compared with other variables, with the exception of the MAFLD components of BMI and TG (Table 2).
Screening value of non-invasive indicators for MAFLD
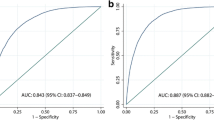
ROC curve analyses showed that FLI had the strongest screening ability for MAFLD in men, with an AUC greater than those of BMI, ZJU, WC, LAP, HSI, HC, TG, VAI, AST, TC, GGT, FPG, ALT, HDL-C, and LDL-C. In women, the FLI was second only to BMI in terms of AUC for diagnosing MAFLD, but the AUC was not statistically different (Z = 1.039, p = 0.30 > 0.05) (Fig. 1). AUCs for the FLI and BMI were 0.853 (0.841–0.865) and 0.850 (0.838–0.862) in men, and 0.847 (0.835–0.859) and 0.852 (0.840–0.864) in women, respectively (Table 2).

ROC curves for FLI, BMI, ZJU, WC, LAP, HSI, and VAI in predicting the occurrence of metabolic dysfunction-associated fatty liver disease in men and women. (ROC receiver operating characteristic, FLI fatty liver index, BMI body mass index, ZJU Zhejiang University Index, WC waist circumference, LAP lipid accumulation product, HSI hepatic steatosis index, VAI visceral adiposity index, MAFLD metabolic dysfunction-associated fatty liver)
Selection of optimal critical value and diagnostic range of FLI and BMI for diagnosing MAFLD
Table 3 shows the sensitivity and specificity of cut-off points at 5-point intervals for the FLI. The optimal critical value was determined using the maximum Youden index method. The optimal cut-off values of FLI and BMI for diagnosing MAFLD in men were 45 (sensitivity, 84.83%; specificity, 69.57%) and 27.4 (sensitivity, 78.47%; specificity, 76.30%), respectively. Additionally, the optimal cut-off values for FLI and BMI in women were 45 (sensitivity, 80.11%; specificity, 74.23%) and 28.0 (sensitivity, 79.56%; specificity, 75.41%), respectively.
The sensitivity and specificity did not reach 100% at the optimal cut-off value, indicating an area of overlap between patients and non-patients. Therefore, we determined the diagnostic range of the FLI according to the method described by Chen et al. [19], where an FLI < 30 (men, LR− = 0.13; women, LR− = 0.18) ruled out MAFLD, while an FLI ≥ 50 (men, LR+ = 3.05; women, LR+ = 3.37) was a basis for its diagnosis (Table 3).
Discussion
In this cross-sectional study conducted among 12,794 Uyghur adults in rural Xinjiang, we assessed the association and screening ability of five steatosis indexes (FLI, HSI, LAP, VAI, ZJU) for MAFLD. We also compared them with traditional indicators, including BMI, WC, LAP, HC, TC, AST, GGT, and LDL-C. The results indicated that higher steatosis index levels were positively associated with an increased risk of MAFLD. The FLI, HSI, LAP, and ZJU have good screening values for MAFLD in both men and women, among which the FLI had the best screening ability.
MAFLD is the hepatic manifestation of metabolic syndrome, which is complex and has many risk factors. A recent study showed that MAFLD tended to coexist with systemic metabolic disorders [20]. Similarly, our study found that MAFLD was affected by various metabolism-related factors, such as WC, HC, blood lipid level, AST, ALT, GGT, LAP, and T2DM. The risk of developing MAFLD has also been reported to vary widely according to race and geographic area [21]. Preliminary studies have found that compared with other ethnic groups, Uyghur residents eat fewer vegetables and have a higher intake of staple foods, red meat, dairy products, vegetable oil, and salt [22, 23]. Although the study population was from a rural area with a backward economy, the BMI and WC were significantly higher than those of the Chinese average [24, 25], and the prevalence of MAFLD was lower than that of the Chinese average [21]. This may be related to the fact that Uyghurs have a fat distribution that is beneficial to metabolic health [26, 27], the average age of the study population is lower, and most of them are engaged in physical labor-related occupations.
In this study, after adjusting for age, sex, HC, TC, LDL-C, AST, ALT, and GGT, high FLI, HSI, LAP, VAI, and ZJU scores remained significantly associated with MAFLD. The FLI is independently associated with an increased risk of hypertension, cardiometabolic disease, atherosclerosis, T2DM, and worsening renal function [28,29,30,31]. Moreover, HSI has been associated with carotid atherosclerosis and chronic kidney disease [32, 33]. Both the LAP and VAI have been strongly associated with metabolic syndrome, T2DM, and cardiovascular events [17, 34, 35], and the ZJU has been associated with insulin resistance [36]. These findings suggest that the five steatosis indexes may be used for both MAFLD screening as well as identifying high-risk metabolic-related and cardiovascular diseases groups. Therefore, patients with high steatosis indexes should undergo more precise clinical examinations. Additionally, conducting early lifestyle interventions, and preventing cardiovascular disease are vital.
Among the existing non-invasive evaluation indicators of hepatic steatosis, the FLI is the most widely used and has been recommended by international guidelines to be used in large epidemiological studies [1], followed by HSI and ZJU. The LAP and VAI, as new body fat indicators, have also attracted increasing attention. The FLI was developed by Bedogni et al. [13] in an Italian population with a mean age of 58 years, and the AUC for the diagnosis of FLD by ultrasound was 0.84 (95% CI 0.81–0.87). This study showed that FLI scores of < 30 and ≥ 60 were cut-offs for the presence or absence of FLD, respectively. At present, the ability of the FLI to screen for FLD or NAFLD has been validated in some populations, with AUCs of 0.813 for White and elderly populations [37]; 0.827 for Taiwanese populations [38]; and 0.834 for middle-aged and elderly populations in Shanghai [39]. Similarly, our study found that the FLI had the best screening power compared with the other single indicators and that FLI appeared to perform better in the diagnosis of MAFLD compared with that of FLD or NAFLD. However, not all studies support that FLI is optimal for its diagnostic value. For example, Kim et al. [40] showed that the FLI had an AUC of 0.785 in Korean populations, and that its diagnostic value was weaker than that of BMI and WC. This may have been due to lower BMI and WC levels and higher TG and GGT levels in the Korean populations compared with Italian populations. Our study showed that the screening power of BMI for MAFLD was comparable to that of FLI in women, possibly due to BMI being an essential component of MAFLD. These results also strongly suggest that being overweight or obese is the primary cause of the current MAFLD epidemic [20, 41]. The original study of the HSI and ZJU showed good accuracy in predicting NAFLD. Kenichiro et al. [42] found that the AUCs of the HSI and ZJU in Japanese health examiners were 0.874 and 0.886, respectively. Duan et al. [8] showed that the AUCs of LAP and VAI in different sex and body weight subgroups was > 0.7. Compared with these findings, the AUCs of the ZJU and VAI in this study were slightly lower, which may be due to the differences in the included population and diagnostic criteria of diseases. We also found that the diagnostic value of the FLI was significantly better than that of the HSI, LAP, VAI, and ZJU, consistent with reports from related studies [43]. Although the results of this study suggest that the diagnostic value of FLI was slightly higher than that of BMI, considering that BMI does not require any blood tests, it may be more convenient and practical as a simple screening tool for MAFLD in the general population.
This study had high sensitivity and specificity at the optimal cut-off value of the FLI for screening MAFLD. However, the low PPV and high NPV of the FLI and HSI may have been due to the low prevalence of MAFLD in this study population. Moreover, compared with the study by Duan et al. [8], the sensitivity and specificity at the optimal cut-off value of BMI in this study were higher, which may be related to the differences in the population and sample sizes.
Currently, approximately 36.11% of China's population lives in rural areas [44]. Simplifying the diagnosis of MAFLD could help achieve health equity and close gaps in the quality of primary health care [5]. No specific treatment for MAFLD exists [45]; however, the risk of MAFLD can be significantly reduced by reducing BMI and WC, which may be accomplished through furthering public knowledge and dietary interventions. In addition, early screening for MAFLD in young populations may prevent further progression of the disease, which may in turn reduce the burden of disease involved with a declining workforce and loss of social value. Therefore, validation of the simple screening tools for MAFLD in this study may have important implications for clinical practice and the development of primary health care services.
Strengths and limitations
This study was the first to evaluate the screening value of the FLI and HSI for MAFLD in large-scale Uyghur populations. However, there were some limitations. First, a lack of liver biopsy data for classifying the severity of hepatic steatosis was evident. Second, this study only included only Uyghur populations, and results could not be extrapolated to other populations. Then, the overall study population was young, and the results could not be extrapolated to older populations. Finally, we did not intend to use these hepatic steatosis indexes to replace the gold standard or other clinical tests. These indicators were non-invasive and were more economical and convenient to obtain in large populations. The hope was to help a wider population recognize possible disease risks ahead of time in larger screenings.
Conclusions
The FLI, HSI, ZJU, LAP, and VAI were associated with the risk of MAFLD in rural Uyghurs in Xinjiang. Among them, the FLI, HSI, ZJU, and LAP had good screening values for MAFLD. In conclusion, both the FLI and BMI could be used as simple screening tools for MAFLD in Uyghur populations of rural Xinjiang. These parameters may be used in large-scale epidemiological studies, which may help improve healthcare services in rural areas.
Availability of data and materials
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- MAFLD:
-
Metabolic dysfunction-associated fatty liver
- FLI:
-
Fatty liver index
- ZJU:
-
Zhejiang University Index
- LAP:
-
Lipid accumulation product
- HIS:
-
Hepatic steatosis index
- VAI:
-
Visceral adiposity index
- ROC:
-
Receiver operating characteristic
- AUC:
-
Areas under the receiver operating characteristic curve
- BMI:
-
Body mass index
- WC:
-
Waist circumference
- HC:
-
Hip circumference
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- T2DM:
-
Type 2 diabetes mellitus
- FPG:
-
Fasting plasma glucose
- TG:
-
Triglycerides
- TC:
-
Total cholesterol
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- AST:
-
Aspartate aminotransferase
- ALT:
-
Alanine aminotransferase
- GGT:
-
Gamma-glutamyl transferase
- LR + :
-
Positive likelihood ratio
- LR-:
-
Negative likelihood ratio
- PPV:
-
Positive predictive value
- NPV:
-
Negative predictive value
- OR:
-
Odds ratio
- CI:
-
Confidence interval
References
Eslam M, Newsome PN, Sarin SK, Anstee QM, Targher G, Romero-Gomez M, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73 (1):202–9.
Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64 (1):73–84.
Pierantonelli I, Svegliati-Baroni G. Nonalcoholic fatty liver disease: basic pathogenetic mechanisms in the progression from NAFLD to NASH. Transplantation. 2019;103 (1):e1–13.
National Workshop on Fatty Liver and Alcoholic Liver Disease, Chinese Society of Hepatology, Chinese Medical Association; Fatty Liver Expert Committee, Chinese Medical Doctor Association. Guidelines of prevention and treatment for nonalcoholic fatty liver disease: a 2018 update. J Pract Hepatol. 2018;2018 (21):177–86.
Nan Y, An J, Bao J, Chen H, Chen Y, Ding H, et al. The Chinese Society of Hepatology position statement on the redefinition of fatty liver disease. J Hepatol. 2021;75 (2):454–61.
Zhang J, Lin S, Jiang D, Li M, Chen Y, Li J, et al. Chronic hepatitis B and non-alcoholic fatty liver disease: conspirators or competitors? Liver Int. 2020;40 (3):496–508.
Jiangao F, Jing Z. Epidemic status and harm of non alcoholic fatty liver disease. Chin J Dig. 2020;40 (9):577–80.
Shaojie D, Zunjing L, Jialiang C, Shukun Y. Value of lipid accumulation product and visceral fat index in predicting nonalcoholic fatty liver disease. J Clin Hepatol. 2022;38 (01):129–34.
Xiaolian G, Mingzhong X, Junxiu T, Yating A. Characteristics analysis of predictive models of nonalcoholic fatty liver disease. Chin Gen Pract. 2021;24 (30):3888–92, 99.
Ismaiel A, Jaaouani A, Leucuta DC, Popa SL, Dumitrascu DL. The visceral adiposity index in non-alcoholic fatty liver disease and liver fibrosis-systematic review and meta-analysis. Biomedicines. 2021. https://doi.org/10.3390/biomedicines9121890.
Jia H, Shuxia G, Jiaming L, Mei Z, Yusong D. Ethnic differences in prevalence of general obesity and abdominal obesity among low-income rural Kazakh and Uyghur adults in far western China and implications in preventive public health. PLoS ONE. 2014;9 (9): e106723.
American Diabetes Association. Executive summary: standards of medical care in diabetes–2012. Diabetes Care. 2012;35 (Suppl 1):S4–10.
Bedogni G, Bellentani S, Miglioli L, Masutti F, Passalacqua M, Castiglione A, et al. The Fatty Liver Index: a simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006;6:33.
Lee JH, Kim D, Kim HJ, Lee CH, Yang JI, Kim W, et al. Hepatic steatosis index: a simple screening tool reflecting nonalcoholic fatty liver disease. Dig Liver Dis. 2010;42 (7):503–8.
Bedogni G, Henry SK, Bellentani S, Tiribelli C. A simple index of lipid overaccumulation is a good marker of liver steatosis. BMC Gastroenterol. 2010;10:98.
Wang J, Xu C, Xun Y, Lu Z, Shi J, Yu C, et al. ZJU index: a novel model for predicting nonalcoholic fatty liver disease in a Chinese population. Sci Rep. 2015;5:16494.
Amato MC, Giordano C, Galia M, Criscimanna A, Vitabile S, Midiri M, et al. Visceral Adiposity Index: a reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care. 2010;33 (4):920–2.
Yamamura S, Eslam M, Kawaguchi T, Tsutsumi T, Nakano D, Yoshinaga S, et al. MAFLD identifies patients with significant hepatic fibrosis better than NAFLD. Liver Int. 2020;40 (12):3018–30.
Chen WZ, Ni ZZ, Pan XP, Liu YY, Xia Y. Receiver operating characteristic curves to determine the optimal operating point and doubtable value interval. Mod Prevent Med. 2005;7:729–31.
Chen YL, Li H, Li S, Xu Z, Tian S, Wu J, et al. Prevalence of and risk factors for metabolic associated fatty liver disease in an urban population in China: a cross-sectional comparative study. BMC Gastroenterol. 2021;21 (1):212.
Zhou F, Zhou J, Wang W, Zhang XJ, Ji YX, Zhang P, et al. Unexpected rapid increase in the burden of NAFLD in China from 2008 to 2018: a systematic review and meta-analysis. Hepatology. 2019;70 (4):1119–33.
Wang WQ, Wei B, Song YP, Guo H, Zhang XH, Wang XP, et al. Metabolically healthy obesity and unhealthy normal weight rural adults in Xinjiang: prevalence and the associated factors. BMC Public Health. 2021;21 (1):1940.
Zhai F, He Y, Wang Z, Hu Y. Status and characteristic of dietary intake of 12 minority nationalities in China. Wei Sheng Yan Jiu. 2007;36 (5):539–41.
Wang Y, Zhang L, He J, Yan Y. Relationship between blood pressure and obesity in adults of remote rural areas of Xinjiang. Chin J Hypertens. 2016;24 (07):650–6.
He J, Guo H, Ding Y, Liu J, Zhang M, Ma R, et al. Epidemiological study on overweight and obesity among rural adult residents in Hazakh, Uygur and Han populations in Xinjiang. Chin J Epidemiol. 2013;34 (12):1164–8.
Frayn KN. Visceral fat and insulin resistance: causative a correlative. Br J Nutr. 2000;83 (Suppl. 1):S71–7.
Abate N, Garg A, Peshock RM, Stray-Gundersen J, Grundy SM. Relationship of generalized and regional adiposity to insulin sensitivity in man. J Clin Invest. 1995;96:88–98.
Olubamwo OO, Virtanen JK, Pihlajamaki J, Mantyselka P, Tuomainen TP. Fatty liver index as a predictor of increased risk of cardiometabolic disease: finding from the Kuopio Ischaemic Heart Disease Risk Factor Study Cohort. BMJ Open. 2019;9 (9): e031420.
Olubamwo OO, Virtanen JK, Pihlajamaki J, Tuomainen TP. Association of fatty liver index with risk of incident type 2 diabetes by metabolic syndrome status in an Eastern Finland male cohort: a prospective study. BMJ Open. 2019;9 (7): e026949.
Higashiura Y, Furuhashi M, Tanaka M, Takahashi S, Mori K, Miyamori D, et al. Elevated fatty liver index is independently associated with new onset of hypertension during a 10-year period in both male and female subjects. J Am Heart Assoc. 2021;10 (14): e021430.
Takahashi S, Tanaka M, Furuhashi M, Moniwa N, Koyama M, Higashiura Y, et al. Fatty liver index is independently associated with deterioration of renal function during a 10-year period in healthy subjects. Sci Rep. 2021;11 (1):8606.
Ochiai H, Shirasawa T, Yoshimoto T, Nagahama S, Sakamoto K, Azuma M, et al. Hepatic steatosis index and chronic kidney disease among middle-aged individuals: a large-scale study in Japan. Dis Markers. 2021;2021:9941834.
Wang C, Cai Z, Deng X, Li H, Zhao Z, Guo C, et al. Association of hepatic steatosis index and fatty liver index with carotid atherosclerosis in type 2 diabetes. Int J Med Sci. 2021;18 (14):3280–9.
Ozcabi B, Demirhan S, Akyol M, Ozturkmen Akay H, Guven A. Lipid accumulation product is a predictor of nonalcoholic fatty liver disease in childhood obesity. Korean J Pediatr. 2019;62 (12):450–5.
Zhang M, Zheng L, Li P, Zhu Y, Chang H, Wang X, et al. 4-Year trajectory of visceral adiposity index in the development of type 2 diabetes: a prospective cohort study. Ann Nutr Metab. 2016;69 (2):142–9.
Ji B, Qu H, Wang H, Wei H, Deng H. The ZJU index: a useful indicator for recognizing insulin resistance in the Chinese general population. Acta Diabetol. 2016;53 (5):817–23.
Koehler EM, Schouten JN, Hansen BE, Hofman A, Stricker BH, Janssen HL. External validation of the fatty liver index for identifying nonalcoholic fatty liver disease in a population-based study. Clin Gastroenterol Hepatol. 2013;11 (9):1201–4.
Yang BL, Wu WC, Fang KC, Wang YC, Huo TI, Huang YH, et al. External validation of fatty liver index for identifying ultrasonographic fatty liver in a large-scale cross-sectional study in Taiwan. PLoS ONE. 2015;10 (3): e0120443.
Huang X, Xu M, Chen Y, Peng K, Huang Y, Wang P, et al. Validation of the fatty liver index for nonalcoholic fatty liver disease in middle-aged and elderly Chinese. Medicine (Baltimore). 2015;94 (40): e1682.
Kim JH, Kwon SY, Lee SW, Lee CH. Validation of fatty liver index and lipid accumulation product for predicting fatty liver in Korean population. Liver Int. 2011;31 (10):1600–1.
Foschi FGBG, Domenicali M, et al. Prevalence of and risk factors for fatty liver in the general population of Northern Italy: the Bagnacavallo Study. BMC Gastroenterol. 2018;18 (1):177.
Murayama K, Okada M, Tanaka K, Inadomi C, Yoshioka W, Kubotsu Y, et al. Prediction of nonalcoholic fatty liver disease using noninvasive and non-imaging procedures in Japanese health checkup examinees. Diagnostics (Basel). 2021. https://doi.org/10.3390/diagnostics11010132.
Han AL, Lee HK. Comparison of the diagnostic performance of steatosis indices for discrimination of CT-diagnosed metabolic dysfunction-associated fatty liver disease. Metabolites. 2022. https://doi.org/10.3390/metabo12070664.
National Bureau of statistics of the People's Republic of China. China Statistical Yearbook 2021. China Statistic Publishing House 2021. p. 31.
Shi J, Su Q, Fan JG, Yang Z. Progress in drug treatment of metabolic associated fatty liver disease. Word Clin Drugs. 2021;42:607–11.
Acknowledgements
We sincerely thank these rural residents for their willingness to participate in the study. We are grateful to the 51st Regiment Hospital for providing study facilities and other assistance.
Funding
This research was funded by the Key science and technology project of Xinjiang Production and Construction Corps (No. 2018AB022).
Author information
Authors and Affiliations
Contributions
GYB, HYH, YJ, MRL, ZXH, GH, WXP, LY, PXY, ZSJ, HJ and GSX participated in data collection for the baseline and follow-up surveys, with GSX and HJ organizing the team and PXY managing the clinical ultrasound. GYB and HYH were major contributors to writing the manuscript. All authors have read and agreed to the version of the manuscript. The manuscript has been read and approved by all the authors. The requirements for authorship as stated earlier in this document have been met. And each author believes that the manuscript represents honest work.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Review Board (IERB) of the First Affiliated Hospital of Shihezi University School of Medicine (IERB no.: SHZ2010LL01). Informed consent was obtained from all subjects involved in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Guo, Y., Hu, Y., Yang, J. et al. Validation of non-invasive indicators in the screening of metabolic dysfunction-associated fatty liver disease: a cross-sectional study among Uighurs in rural Xinjiang. Eur J Med Res 28, 555 (2023). https://doi.org/10.1186/s40001-023-01536-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01536-2