
Abstract
Objective
The existing literature on the combination of acute pancreatitis (AP) and COVID-19 is scarce. The objective of our study is to compare the clinical outcomes and occurrence of long COVID syndrome in AP patients with and without COVID-19, while investigating the potential impact of COVID-19 on the severity, mortality rate, and long COVID syndrome in these patients.
Methods
This retrospective, observational study was conducted at a single center. It included patients aged 18 years and above who were diagnosed with AP during the pandemic. Patients were categorized into two groups based on the results of RT-qPCR testing: the SARS-CoV-2-positive group and the SARS-CoV-2-negative group. The study aimed to compare the severity of AP, mortality rate, and occurrence of long COVID syndrome between these two groups.
Result
A retrospective review was conducted on 122 patients diagnosed with acute pancreatitis between December 1, 2022, and January 31, 2023. Out of these patients, 100 were included in the study. The analysis revealed no significant differences in mortality rate, severity, and sequelae between AP patients with COVID-19 and those without COVID-19 (p > 0.005). However, a statistically significant difference was observed in the occurrence of long COVID syndrome, specifically in the presence of cough (p = 0.04).
Conclusion
This study demonstrates that the presence of COVID-19 in patients with pancreatitis does not lead to an increase in the mortality and severity rate of pancreatitis.
Similar content being viewed by others


Background
Acute pancreatitis (AP) is a common gastrointestinal disease that typically requires hospitalization [1]. Severe AP accompanied by organ failure is closely associated with poor patient prognosis and increased risk of mortality [2, 3].
In late December 2019, a novel respiratory syndrome emerged in Wuhan, China. Subsequent testing confirmed it to be severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). A few months later, the World Health Organization declared it a major public health concern. The clinical manifestations of COVID-19, the disease caused by SARS-CoV-2, are wide-ranging and include fever, cough, and dyspnea [4]. Additionally, less common symptoms encompass loss of smell and taste, gastrointestinal symptoms, headache, and rash [5,6,7,8]. Since the onset of the pandemic, there has been a growing body of literature focused on exploring treatment strategies and reducing mortality associated with COVID-19 [9,10,11]. As of January 2023, there have been more than 850 million reported cases of COVID-19 worldwide, resulting in over 6.6 million deaths [12]. However, COVID-19 remains a substantial global health threat. Apart from its mortality rate, COVID-19 presents an unparalleled risk to the mental well-being of individuals worldwide. Numerous patients with COVID-19 encounter emotional disorders and exhibit symptoms of depression [13,14,15].
Although strict epidemic prevention measures have led to a decline in the number of COVID-19 infections, China made adjustments to its epidemic prevention policy on December 7, 2022, resulting in a surge in cases from December 2022 to January 2023. During this period, the primary variant circulating in China was Omicron [16]. Previous studies have shown a significantly increased risk of adverse outcomes and a mortality rate close to 20% in patients with concurrent AP and COVID-19 [17]. Numerous studies have reported an increase in pancreatic enzymes in patients with COVID-19 [18], indicating potential pancreatic damage associated with the disease. However, with the increasing coverage of vaccines, the mortality rate of COVID-19 patients continues to decline [19]. The mortality rate of patients with concurrent acute pancreatitis and COVID-19 may undergo changes in the near future. However, there has been a scarcity of articles in this research area over the past 2 years, highlighting the need for further investigation to address this knowledge gap.
Therefore, we conducted a retrospective review of all hospitalized patients with AP in our hospital, comparing the clinical outcomes and short-term outcomes between patients with COVID-19-associated AP and those with SARS-CoV-2-negative AP.
Materials and methods
Study design
This is a single-center, retrospective, and observational study.
Population and study time
We screened patients who visited the emergency department of our hospital from December 1, 2022, to January 31, 2023, using the hospital electronic system.
Inclusion and exclusion criteria
The inclusion criteria were all patients with acute pancreatitis (AP) in the entire hospital, with available reverse transcriptase real-time (RT-qPCR) results, laboratory tests, and imaging results. If a patient had multiple admissions due to AP during the study period, only the last admission was considered for eligibility.
Setting
General population in Luzhou City, Sichuan Province.
Assessments
The clinical diagnosis of COVID-19 is primarily based on epidemiological history, clinical manifestations, and laboratory testing methods. The laboratory testing method involves using an oropharyngeal swab sample for RT-qPCR [20]. Based on the RT-qPCR test results, patients are categorized into positive and negative groups.
Data collection
We analyzed the mortality rates of COVID-19 patients as reported in relevant studies [21]. In order to ensure sufficient statistical power and precision, we excluded studies that did not meet the predetermined sample size threshold of 81. This threshold was calculated using PASS 15 software, with a confidence level of 0.95, a confidence interval width of 0.227, and an assumed proportion of 0.454. The purpose of this sample size threshold was to ensure that the included studies had enough power to achieve a margin of error of at least 0.05 on the estimated prevalence. Considering an estimated loss of follow-up rate of 10%, it is recommended that the final sample size should not be less than 89. This adjustment accounts for potential attrition and ensures that an adequate number of participants remain in the study for reliable analysis.
Upon admission, clinical laboratory tests including white blood cell (WBC) count, lymphocyte (Lym) count, neutrophil (Neu) count, neutrophil-to-lymphocyte ratio (NLR), hematocrit (HCT), red cell distribution width (RDW), platelet (PLT) count, C-reactive protein (CRP), D-dimer levels, and imaging findings are recorded (Table 1). Patient history regarding alcohol consumption, family history (genetic diseases), laboratory tests (hyperlipidemia), and diagnostic procedures such as computed tomography (CT), endoscopic ultrasound, magnetic resonance cholangiopancreatography (MRCP), and endoscopic retrograde cholangiopancreatography (ERCP) are examined to determine the etiology of the patient's condition. Patients in whom no cause is identified after evaluation are documented as having “unknown etiology”.
Patients who underwent interventional treatments (ERCP, PTC), surgical interventions (such as cholecystectomy), and pharmacological treatment for AP are documented. The length of hospital stay (intensive care/service), AP-related complications, and mortality rate are recorded. During the month of March 2023, a telephone follow-up was conducted for all patients to inquire about the presence of long COVID syndrome. Refusal to participate in the telephone follow-up or patient refusal to answer relevant questions is considered as loss to follow-up.
Research definition
The diagnosis of acute pancreatitis (AP) is based on the revised Atlanta criteria [22]. Comorbidities are classified using the Charlson Comorbidity Index (CCI) [23]. Long COVID syndrome is defined as the presence of persistent symptoms and/or delayed or long-term complications lasting for more than 4 weeks after symptom onset [24]. The severity of AP is determined using the Bedside Index for Severity in Acute Pancreatitis (BISAP) score [25]. A BISAP score of ≥ 3 indicates severe AP, while a score of ≤ 2 indicates mild AP [26]. We also utilize the Balthazar CT Severity Index (CTSI) to assess the severity of AP, with severity categorized as mild (0–3 points) or moderate to severe (4–10 points) [27].
Organ failure is defined as a Marshall score [28] of ≥ 2 in one or more of the three organ systems (respiratory, renal, and cardiovascular) initially described. The organ failure score is calculated based on the most extreme laboratory values or clinical measurements within the first 72 h prior to hospital admission for all patients. The duration of organ failure is defined as transient (≤ 48 h) or persistent (> 48 h).
Statistical analysis
The research data were evaluated using IBM SPSS Statistics version 27. The normality of quantitative data was analyzed using the one-sample Kolmogorov–Smirnov test, which helped determine whether to use parametric or non-parametric tests. Descriptive statistics were computed for frequency and percentage distributions, as well as for continuous variables, including mean, standard deviation, median, minimum, and maximum values. For comparing categorical variables between groups, the Pearson chi-square test and Fisher’s exact test were employed. The Mann–Whitney U test was used to analyze differences between laboratory values and SARS-CoV-2 test results. Additionally, laboratory parameters were evaluated by comparing SARS-CoV-2 positive and negative patients with acute pancreatitis. A significance level of p < 0.05 was considered statistically significant.
Ethical issues
This retrospective and observational study did not provide any additional interventions to the included patients. The retrospective study design has been approved by the Clinical Trial Ethics Committee of the Affiliated Hospital of Southwest Medical University, China (Approval No: KY2023190).
This study was conducted in accordance with the Helsinki Declaration. A written informed consent form has been exempted by the ethics review committee, because we only retrospectively extracted anonymous data without any protected information. Each patient participating in this study was assigned a unique identifier, and all anonymous patient data were recorded and analyzed in relation to this identifier.
Results
We conducted a retrospective analysis of 122 patients diagnosed with acute pancreatitis (AP) between December 1, 2022, and January 31, 2023. Among these patients, there were 100 individuals who met the inclusion criteria and had sufficient data recorded. The positivity rate for SARS-CoV-2 was found to be 26%. Among the included patients, 47.6% were male, with a mean age of 54.56 ± 16.90 years, while 52.4% were female, with a mean age of 55.24 ± 19.00 years.
The patients were divided into two groups: the SARS-CoV-2 positive group (n = 26) and the SARS-CoV-2 negative groups (n = 74). There were no significant differences in baseline characteristics between the two groups (Table 2). In terms of comorbidity distribution, there was no significant difference in the proportion of patients with a CCI score ≥ 5 between the positive and negative groups (Table 3). When comparing short-term organ failure between the two groups, there was no statistically significant difference (p = 0.69). Similarly, there was no statistically significant difference in the occurrence of persistent organ failure between the positive group (3.85%) and the negative group (4.05%) (p = 1.0). The BISAP score and Balthazar CT index also showed no statistically significant difference (p = 0.88, p = 0.43), indicating no significant difference in disease severity between the two groups. After analyzing the mortality rate among hospitalized patients, it was found that the mortality rate was 3.85% for the positive group and 4.05% for the negative group, with no statistically significant difference (p = 1.0).
A telephone follow-up was conducted for all AP patients (Table 4), and it was found that 16 individuals were lost to follow-up, resulting in a loss to follow-up rate of 16%. Regarding long COVID syndrome, only coughing showed a statistically significant difference (p = 0.04).
Discussion
We present here the clinical and short-term outcomes of patients with acute pancreatitis (AP) admitted during the outbreak of the novel coronavirus pneumonia in China. We found that SARS-CoV-2-positive AP patients had similar mortality rates and disease severity compared to SARS-CoV-2-negative AP patients, with no statistically significant differences observed across various scoring systems. Follow-up at 1–2 months revealed that AP patients who tested positive for SARS-CoV-2 were more likely to experience cough symptoms (p = 0.04). Although there was a higher proportion of positive cases reporting abdominal pain, the difference was not statistically significant (p = 0.088).
A meta-analysis has indicated a high risk of adverse outcomes, with a mortality rate close to 20%, in patients with both AP and COVID-19 [17]. However, in our study, we found no statistically significant difference in the mortality rates between AP patients with and without COVID-19 (p = 1.0). The mortality rate among AP patients with COVID-19 was 3.85%, which is considerably lower than the mortality rate reported in the literature.
The lower mortality rate observed in our study may be attributed to the fact that a majority of patients (91.7%) received vaccination. Research has shown that vaccines provide a significant level of protection against severe COVID-19, reducing hospitalization rates and mortality [19, 29]. As of April 7, 2021, a total of 710 million vaccine doses have been administered globally, with at least one dose of an approved vaccine given to 5% of the world’s population [30]. The studies included in the article by Yang et al. [17] were published between 2020 and 2021, with most of the patients being admitted in 2020. Therefore, it can be inferred that the vaccine coverage among the patients included in Yang et al.'s article was extremely low, which could explain the lower mortality rate observed in our patients.
The potential of SARS-CoV-2 to induce acute pancreatitis remains unclear [31,32,33,34]. Indeed, there is evidence suggesting that SARS-CoV-2 has the ability to infect the pancreas and induce pancreatic injury [18, 35,36,37,38]. According to our study, there was no significant difference in disease severity between the two groups as indicated by the BISAP score and Balthazar CT index. This may be due to the limited extent of pancreatic damage caused by the current strain of SARS-CoV-2, resulting in no statistically significant difference in disease severity and mortality rates between the two groups.
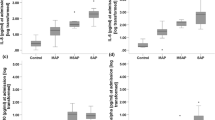
In our comparison of the initial laboratory test results between SARS-CoV-2-positive and -negative patients on the day of admission, we found statistically significant differences (p < 0.05) in the counts of white blood cells, neutrophils, and eosinophils, while other results showed no statistically significant differences (p > 0.05). These differences may be attributed to the viral infection.
After a short-term follow-up of 1 month post-discharge, we found that the most commonly reported symptoms of long COVID syndrome among SARS-CoV-2-positive patients were fatigue (35%) followed by abdominal pain (30%). Although both symptoms were relatively high in proportion compared to SARS-CoV-2-negative patients, there was no statistically significant difference (p > 0.05). The only symptom that showed a statistically significant difference was cough (p = 0.04). The prevalence of cough in our COVID-19 patients after discharge (15%) was similar to what has been reported in other studies [39]. Research has shown that vaccinated individuals and those infected with the Omicron variant have a lower risk of developing long COVID syndrome [40]. This may explain why there was no difference in long COVID syndrome among our patients.
Additionally, studies have reported that even post-infection vaccination can alleviate long COVID syndrome [41]. Therefore, it is recommended that patients who have not received the vaccine after infection should consider getting vaccinated to mitigate the symptoms of long COVID syndrome.
Limitations
As this study is retrospective, there may be selection bias, and the results may not fully reflect the overall outcomes of patients with COVID-19-associated pancreatitis. Our follow-up was conducted via telephone, which introduces the possibility of recall bias. Additionally, a small proportion of patients were lost to follow-up, which could potentially impact the results. The sample size of our study was relatively small, with only 100 patients. This study was conducted at a single center, which may limit the generalizability of the results. The follow-up period was relatively short (1–2 months), and longer term follow-up was not conducted. Long COVID-19 syndrome typically lasts for 4–8 weeks or longer. Therefore, it is possible that some patients who tested negative for SARS-CoV-2 upon admission may have been infected prior to admission or after discharge, which could introduce bias in the follow-up results of long COVID-19 syndrome.
Conclusion
Our research findings indicate that there is no significant difference in clinical outcomes and short-term prognosis between patients with COVID-19-related pancreatitis and those without SARS-CoV-2 infection. Furthermore, we observed that individuals who have been vaccinated against COVID-19 and subsequently contract COVID-19-related pancreatitis generally do not require additional medical care.
Availability of data and materials
The datasets utilized and/or analyzed during the present study are accessible from the corresponding author upon reasonable request.
References
Boxhoorn L, Voermans RP, Bouwense SA, Bruno MJ, Verdonk RC, Boermeester MA, et al. Acute pancreatitis. Lancet. 2020;396(10252):726–34.
Schepers NJ, Bakker OJ, Besselink MG, Ahmed Ali U, Bollen TL, Gooszen HG, et al. Impact of characteristics of organ failure and infected necrosis on mortality in necrotising pancreatitis. Gut. 2019;68(6):1044–51.
He W, Chen P, Lei Y, Xia L, Liu P, Zhu Y, et al. Randomized controlled trial: neostigmine for intra-abdominal hypertension in acute pancreatitis. Crit Care. 2022;26(1):52.
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China [published correction appears in Lancet. 2020 Jan 30;:]. Lancet. 2020;395(10223):497–506. https://doi.org/10.1016/S0140-6736(20)30183-5
Vaira LA, Deiana G, Fois AG, Pirina P, Madeddu G, De Vito A, et al. Objective evaluation of anosmia and ageusia in COVID-19 patients: Single-center experience on 72 cases. Head Neck. 2020;42(6):1252–8. https://doi.org/10.1002/hed.26204.
De Vito A, Geremia N, Fiore V, Princic E, Babudieri S, Madeddu G. Clinical features, laboratory findings and predictors of death in hospitalized patients with COVID-19 in Sardinia. Italy Eur Rev Med Pharmacol Sci. 2020;24(14):7861–8. https://doi.org/10.26355/eurrev_202007_22291.
Guarneri C, Rullo EV, Pavone P, Berretta M, Ceccarelli M, Natale A, et al. Silent COVID-19: what your skin can reveal. Lancet Infect Dis. 2021;21(1):24–5. https://doi.org/10.1016/S1473-3099(20)30402-3.
Guarneri C, VenanziRullo E, Gallizzi R, Ceccarelli M, Cannavò SP, Nunnari G. Diversity of clinical appearance of cutaneous manifestations in the course of COVID-19. J Eur Acad Dermatol Venereol. 2020;34(9):e449–50. https://doi.org/10.1111/jdv.16669.
Rodriguez-Guerra M, Jadhav P, Vittorio TJ. Current treatment in COVID-19 disease: a rapid review. Drugs Context. 2021. https://doi.org/10.7573/dic.2020-10-3.
Fiore V, De Vito A, Bagella P, Princic E, Mariani AA, Denti L, et al. Effectiveness of vitamin D supplements among patients hospitalized for COVID-19: results from a monocentric matched-cohort study. Healthcare (Basel). 2022;10(5):956. https://doi.org/10.3390/healthcare10050956.
De Vito A, Poliseno M, Colpani A, Zauli B, Puci MV, Santantonio T, et al. Reduced risk of death in people with SARS-CoV-2 infection treated with remdesivir: a nested case-control study. Curr Med Res Opin. 2022;38(12):2029–33. https://doi.org/10.1080/03007995.2022.2129801.
Hromić-Jahjefendić A, Barh D, Uversky V, Aljabali AA, Tambuwala MM, Alzahrani KJ, et al. Can COVID-19 vaccines induce premature non-communicable diseases: where are we heading to? Vaccines (Basel). 2023;11(2):208.
Fiore V, De Vito A, Fanelli C, Geremia N, Princic E, Nivoli A, et al. Mood reactive disorders among COVID-19 inpatients: experience from a monocentric cohort. Med Princ Pract. 2021;30(6):535–41. https://doi.org/10.1159/000518490.
Xiong J, Lipsitz O, Nasri F, Lui LMW, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. 2020;277:55–64. https://doi.org/10.1016/j.jad.2020.08.001.
Gadermann AC, Thomson KC, Richardson CG, Gagné M, McAuliffe C, Hirani S, et al. Examining the impacts of the COVID-19 pandemic on family mental health in Canada: findings from a national cross-sectional study. BMJ Open. 2021;11(1):e042871. https://doi.org/10.1136/bmjopen-2020-042871.
Ma E, Ai J, Zhang Y, Zheng J, Gao X, Xu J, et al. Omicron infections profile and vaccination status among 1881 liver transplant recipients: a multi-centre retrospective cohort. Emerg Microbes Infect. 2022;11(1):2636–44.
Yang F, Huang Y, Li T, Fu Y, Sun C, Xu Y, et al. Prevalence and outcomes of acute pancreatitis in COVID-19: a meta-analysis. Gut. 2022;71(7):1451–3.
Wang F, Wang H, Fan J, Zhang Y, Wang H, Zhao Q. Pancreatic injury patterns in patients with coronavirus disease 19 pneumonia. Gastroenterology. 2020;159(1):367–70. https://doi.org/10.1053/j.gastro.2020.03.055.
Watson OJ, Barnsley G, Toor J, Hogan AB, Winskill P, Ghani AC. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infect Dis. 2022;22(9):1293–302.
Rai P, Kumar BK, Deekshit VK, Karunasagar I, Karunasagar I. Detection technologies and recent developments in the diagnosis of COVID-19 infection. Appl Microbiol Biotechnol. 2021;105(2):441–55.
Akarsu C, Karabulut M, Aydin H, et al. Association between acute pancreatitis and COVID-19: could pancreatitis be the missing piece of the puzzle about increased mortality rates? J Invest Surg. 2022;35(1):119–25. https://doi.org/10.1080/08941939.2020.1833263.
Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis–2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–11.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83.
Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, et al. Post-acute COVID-19 syndrome. Nat Med. 2021;27(4):601–15.
Wu BU, Johannes RS, Sun X, Tabak Y, Conwell DL, Banks PA. The early prediction of mortality in acute pancreatitis: a large population-based study. Gut. 2008;57(12):1698–703.
Singh VK, Wu BU, Bollen TL, Repas K, Maurer R, Johannes RS, et al. A prospective evaluation of the bedside index for severity in acute pancreatitis score in assessing mortality and intermediate markers of severity in acute pancreatitis. Am J Gastroenterol. 2009;104(4):966–71.
Cheng T, Han TY, Liu BF, Pan P, Lai Q, Yu H, et al. Use of modified balthazar grades for the early prediction of acute pancreatitis severity in the emergency department. Int J Gen Med. 2022;15:1111–9.
Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, Sibbald WJ. Multiple organ dysfunction score: a reliable descriptor of a complex clinical outcome. Crit Care Med. 1995;23(10):1638–52.
Lai FTT, Yan VKC, Ye X, Ma T, Qin X, Chui CSL, et al. Booster vaccination with inactivated whole-virus or mRNA vaccines and COVID-19-related deaths among people with multimorbidity: a cohort study. CMAJ. 2023;195(4):E143–52.
Mathieu E, Ritchie H, Ortiz-Ospina E, Roser M, Hasell J, Appel C, et al. A global database of COVID-19 vaccinations. Nat Hum Behav. 2021;5(7):947–53.
Hadi A, Werge M, Kristiansen KT, Pedersen UG, Karstensen JG, Novovic S, et al. Coronavirus Disease-19 (COVID-19) associated with severe acute pancreatitis: case report on three family members. Pancreatology. 2020;20(4):665–7. https://doi.org/10.1016/j.pan.2020.04.021.
Madaria E, Capurso G. COVID-19 and acute pancreatitis: examining the causality. Nat Rev Gastroenterol Hepatol. 2021;18(1):3–4. https://doi.org/10.1038/s41575-020-00389-y.
Brikman S, Denysova V, Menzal H, Dori G. Acute pancreatitis in a 61-year-old man with COVID-19. CMAJ. 2020;192(30):E858–9. https://doi.org/10.1503/cmaj.201029.
Fiore V, Beretta R, De Vito A, Barac A, Maida I, Joeseph Kelvin DD, et al. Emerging clinical features of COVID-19 related pancreatitis: case reports and review of the literature. Front Med (Lausanne). 2022;8:779118. https://doi.org/10.3389/fmed.2021.779118.
Zheng L, Zhang L, Zheng Y, An J, Wen G, Jin H, et al. Digestive system infection by SARS-CoV-2: entry mechanism, clinical symptoms and expression of major receptors (Review). Int J Mol Med. 2023;51(3):1–11.
Liu F, Long X, Zhang B, Zhang W, Chen X, Zhang Z. ACE2 expression in pancreas may cause pancreatic damage after SARS-CoV-2 infection. Clin Gastroenterol Hepatol. 2020;18(9):2128-2130.e2. https://doi.org/10.1016/j.cgh.2020.04.040.
Lakshmanan S, Malik A. Acute pancreatitis in mild COVID-19 infection. Cureus. 2020;12(8):e9886. https://doi.org/10.7759/cureus.9886.
Aloysius MM, Thatti A, Gupta A, Sharma N, Bansal P, Goyal H. COVID-19 presenting as acute pancreatitis. Pancreatology. 2020;20(5):1026–7. https://doi.org/10.1016/j.pan.2020.05.003.
Carfì A, Bernabei R, Landi F. Persistent symptoms in patients after acute COVID-19. JAMA. 2020;324(6):603–5.
Howe S, Szanyi J, Blakely T. The health impact of long COVID during the 2021–2022 Omicron wave in Australia: a quantitative burden of disease study. Int J Epidemiol. 2023;52(3):677–89.
Richard SA, Pollett SD, Fries AC, Berjohn CM, Maves RC, Lalani T, et al. Persistent COVID-19 symptoms at 6 months after onset and the role of vaccination before or after SARS-CoV-2 infection. JAMA Netw Open. 2023;6(1): e2251360.
Funding
This study was supported by the National Natural Science Foundation of China (No. U22A2039).
Author information
Authors and Affiliations
Contributions
Data collection and organization were carried out by JZ and MK. JZ and DL performed the statistical analysis and completed the writing of this manuscript. BL provided valuable suggestions for the manuscript’s revisions, while SS was responsible for the editing and final review of the manuscript. JZ, DL, and MK have made equal contributions to this work and should be acknowledged as co-first authors. All authors rigorously assessed the research design, contributed to manuscript editing, and read and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The retrospective study design has been approved by the Clinical Trial Ethics Committee of the Affiliated Hospital of Southwest Medical University, China (Approval No: KY2023190).
Consent for publication
The research findings presented in this work have not been previously published, and the publication of this manuscript has received approval from all co-authors.
Competing interests
The authors declare that there is no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, J., Luo, D., Kang, M. et al. Clinical characteristics and short-term outcomes of acute pancreatitis among patients with COVID-19. Eur J Med Res 28, 283 (2023). https://doi.org/10.1186/s40001-023-01252-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01252-x