
Abstract
Background
Human papillomavirus (HPV) has been proposed as a potential pathogenetic organism involved in prostate cancer (PCa), but the association between HPV infection and relevant genomic changes in PCa is poorly understood.
Methods
To evaluate the relationship between HPV genotypes and genomic alterations in PCa, HPV capture sequencing of DNA isolated from 59 Han Chinese PCa patients was performed using an Illumina HiSeq2500. Additionally, whole-exome sequencing of DNA from these 59 PCa tissue samples and matched normal tissues was carried out using the BGI DNBSEQ platform. HPV infection status and genotyping were determined, and the genetic disparities between HPV-positive and HPV-negative PCa were evaluated.
Results
The presence of the high-risk HPV genome was identified in 16.9% of our cohort, and HPV16 was the most frequent genotype detected. The overall mutational burden in HPV-positive and HPV-negative PCa was similar, with an average of 2.68/Mb versus 2.58/Mb, respectively, in the targeted whole-exome region. HPV-negative tumors showed a mutational spectrum concordant with published PCa analyses with enrichment for mutations in SPOP, FOXA1, and MED12. HPV-positive tumors showed more mutations in KMT2C, KMT2D and ERCC2. Copy number alterations per sample were comparable between the two groups. However, the significantly amplified or deleted regions of the two groups only partially overlapped. We identified amplifications in oncogenes, including FCGR2B and CCND1, and deletions of tumor suppressors, such as CCNC and RB1, only in HPV-negative tumors. HPV-positive tumors showed unique deletions of tumor suppressors such as NTRK1 and JAK1.
Conclusions
The genomic mutational landscape of PCa differs based on HPV infection status. This work adds evidence for the direct involvement of HPV in PCa etiology. Different genomic features render HPV-positive PCa a unique subpopulation that might benefit from virus-targeted therapy.
Similar content being viewed by others

Background
Prostate cancer (PCa) is the second most common cancer in men worldwide [1]. The incidence and mortality have increased rapidly in China during the last decade [2]. The firmly established risk factors include advanced age, family history of this malignancy, certain genetic mutations (e.g., BRCA1 and BRCA2) and conditions (e.g., Lynch syndrome). High-risk human papillomavirus (hrHPV) infection has also been suggested as a risk factor for PCa [3]. To date, studies have identified the presence of hrHPV in PCa tissue and an increased odds ratio (OR) of HPV infection in PCa compared with controls [4]. However, the dominant detection method of previous studies was PCR-based, focusing only on specific HPV types rather than comprehensive detection of all hrHPV types, which may result in variations in reported HPV infection rates across studies [5].
Further investigations revealed that HPV infection can impact the development of PCa by triggering chronic inflammatory processes, resulting in DNA damage [6, 7]. HPV-driven cancers possess a widely distributed exogenous virus that creates a specific mutagenic environment. HPV genes can disrupt crucial pathways responsible for preserving genome integrity. Eventually, this disruption gives rise to additional genetic mutations, allowing the initiation of cancer [8]. PCa is regarded as being closely associated with accumulation of somatic mutations in the prostate epithelial cell genome, and the Cancer Genome Atlas (TCGA) taxonomy [9] for PCa is based on seven important oncogenic drivers, including ERG, ETV1, ETV4, FLI1, SPOP, FOXA1, and IDH1. In total, 68.4% of Chinese PCa cases can be attributed to one of the TCGA taxonomies [10]. However, whether HPV infection in PCa causes genomic alterations and subsequently contributes to tumor initiation and progression has not been fully investigated.
In this study, we investigated hrHPV prevalence using capture sequencing in 59 Chinese PCa patients, and performed whole-exome sequencing (WES) to evaluate the association between the HPV status and genomic alterations. This study aimed to characterize the distinct molecular landscape of hrHPV-positive and hrHPV-negative PCas. We believe that elucidating the causative role of hrHPV in PCa will help to strengthen calls for cancer screening and vaccination programs.
Methods
Patients and samples
The study was approved by the Ethics Committee of the Central Hospital of Wuhan in China (WHZXKYL2022-047). We recruited 59 PCa patients admitted to our hospital from January 2019 to December 2020. Formalin-fixed, paraffin-embedded (FFPE) tissue blocks were examined by an experienced pathologist to select tumor samples with malignant cell purities over 70% and adjacent normal tissues. All patients provided signed informed consent before enrollment.
For each FFPE sample, DNA was extracted using E.A.N., an FFPE DNA Kit (Omega Biotek) according to the manufacturer’s protocol. The DNA concentration was quantified using a Qubit 4.0 Fluorometer. The fragment length and degradation were assessed by a Qsep100 bioanalyzer (BIOptic). The DNA was stored at – 20 °C before use.
HPV genotyping by capture sequencing
Capture sequencing was performed as described previously [11]. Briefly, we designed a custom panel containing the whole-genome sequences of 15 types of hrHPV, and ordered a biotinylated RNA probe library from IDT (IDT, USA).
DNA (250 ng) from tumor samples was sheared to 250–350 bp by a Bioruptor Pico (Diagenode). After purification using Agencourt AMPure XP beads (Beckman), whole-genome libraries were constructed using a TargetSeq Enrichment Kit (iGeneTech). Hybridization was performed at 65 °C for 16 h. After capture and PCR amplification, the HPV libraries were analyzed using Qubit4.0 and Qsep100 bioanalyzers, and sequenced using the Illumina HiSeq2500 platform.
Data were submitted to our in-house pipeline VIPA [12] for HPV genotype and integration detection. This included the following: (i) quality control; (ii) reference preparation. A human reference genome (GRCh38.p12) was downloaded from UCSC (http://genome.ucsc.edu/), and HPV genome references was downloaded from the PaVE database (http://pave.niaid.nih.gov); (iii) alignment to the mixed human and 15 types of hrHPV references with BWA-MEM [13] to detect virus genomes; (iv) remapping of the clean reads to mixed human–virus references to identify breakpoints; (v) junction positions were annotated by ANNOVAR (V2017-07-17) [14] as integration breakpoints.
WES sample processing
Two micrograms of DNA from all tumor and adjacent normal samples was sent to BGI company (Wuhan, China) for library preparation and sequencing. The Agilent SureSelect Human All Exon V6 kit (Agilent Technologies, 60.33 Mb target region) was used for WES capture experiments according to the manufacturer’s recommendations. Specifically, a Bioruptor Pico shearing system was used for fragmentation to generate 200–300 bp fragments. Next, liquid-phase hybridization was performed to selectively enrich DNA fragments using biotin-labeled probes. After library quantification, PE100 data were generated using a BGI DNBSEQ platform.
WES alignment and variant calling
Trimmed paired-end reads were aligned to the UCSC hg38 reference genome using BWA-MEM. Picard tools and SAMtools [15] were employed to remove PCR duplicate reads and deal with alignment files. Bam files were locally realigned using Genome Analysis Toolkit (GATK) to improve accuracy [16]. Somatic mutations in tumor–control paired samples were detected by GATK Mutect2 [17] and annotated by ANNOVAR. The Mutation Annotation Format (MAF) of somatic variants was visualized by using the maftools [18] R package.
Significant CNV detection
Somatic copy number variation (CNV) was called with FACETS [19] using deduplicated mapping bam files for each paired sample. FACETS provides estimates of copy number based on comparing binned read depths to the reference genome. The CNVs were annotated using GISTIC2.0 [20] to generate focal-level CNVs for the cohort with G-Score and FDR Q values used to indicate the significance of the CNVs identified.
Statistical analysis
Statistical analyses were performed using Prism 9 (GraphPad) and SPSS Statistics v.26 (IBM). One-way ANOVA was used to assess the relationship between mean age and clinical characteristics. Molecular alterations were compared using Chi-squared Fisher’s exact test for categorical variables and Welch’s t test for continuous variables. P values < 0.05 were considered statistically significant.
Results
Patient characteristics
Of the 59 PCa patients included in this study, the mean age was 72.83 \(\pm\) 6.22 years. The baseline characteristics are shown in Table 1. The mean age of the patients showed no significant relationship with the tPSA value, fPSA/tPSA ratio, ISUP group, T stage, N stage, or M stage. There was no significant difference in the distribution of all clinical features between the higher age group and the lower age group, except for a higher fPSA/tPSA ratio detected in the age group over 70 years (P = 0.010).
HPV genotypes and clinical characteristics relative to HPV status
HPV genotyping results showed that 10 patients (16.9%) were HPV positive. HPV16 was the most frequent genotype detected in eight cases (13.6%). We found the presence of both single-type infection and coinfection, including single HPV16 (11.9%), double HPV16/98 (1.7%), single HPV18 (1.7%) and multiple HPV26/51/66 (1.7%) infections (Additional file 1: Figure S1A).
The median age of the patients showed no statistically significant difference between the HPV-positive and HPV-negative groups (Additional file 1: Figure S1B). As shown in Table 2, the distribution of the T stage between the two groups did differ. The highest prevalence of HPV was in the T1 stage (3/5, 60%), followed by the T4 stage (3/10, 30%), but no trend was observed for higher T stage corresponding to higher HPV infection rates. Additionally, the frequency distributions of age, ISUP group, N stage, and M stage between the positive and negative groups were not significant.
We performed pipeline VIPA and found no HPV DNA integration event in our data set.
Detection of somatic aberrations
WES was performed on 59 tumor–adjacent normal pairs. All samples had at least 60.12 Mb of target exome region covered with a median depth of 145.54\(\times\) (range: 18.31–268.47\(\times\)) for tumor samples and 107.17\(\times\) (range: 32.76–142.03\(\times\)) for adjacent normal samples (Additional file 4: Table S1). Collectively, the 59 samples contained 24,058 somatic mutations, including 4902 missense, 428 nonsense, 2254 silent, 315 splice-site, four nonstop mutations, 559 frameshift insertions and deletions (indels) and 406 in-frame indels. Eight hypermutant samples showed outlier mutation frequencies (>600 mutants per sample). The average mutation density was 6.76 mutations per Mb across all tumors, and 2.59 when the hypermutant tumors were excluded (Additional file 5: Table S2). At all targeted bases, we did not detect a significant difference in overall mutation rates by HPV status (HPV-positive 2.68/Mb, HPV-negative 2.58/Mb, P = 0.891) (Additional file 2: Figure S2).
Overall, the most common genomic alterations in PCa were mutations in SPOP (17%), followed by TTN (15%), OBSCN (14%), FOXA1 (12%), and SYNE1 (12%). The findings are summarized in Additional file 3: Figure S3. As illustrated in the waterfall map in Fig. 1A, the somatic mutation was altered in seven of ten HPV-positive PCa patients (70%). KMT2B and SYNE1 were the most frequently mutated genes. Figure 1B shows that the somatic mutation was altered in 30 of 49 HPV-negative PCa patients (61.22%). SPOP, FOXA1, TTN, and OBSCN were the four most frequently mutated genes, with the frequencies of 20.4%, 14.3%, 14.3%, and 12.2%, respectively. Only four of the top 20 mutated genes were shared by the two groups.

The landscape of somatic mutation profiles in PCa samples. Mutation information of each gene in each HPV-positive PCa sample (A) and HPV-negative PCa sample (B) is shown in the waterfall plot. Each column represents a tumor with the bar graph at the top depicting the number of alterations per sample. Each Oncoprint row shows alterations for each gene. The bar graph on the right of the panel shows the number and distribution of alterations per gene. Different colors with specific annotations at the bottom depict the various mutation types and clinical features. C A stacked bar plot shows the differences in the SMGs mutation of HPV-positive PCa versus HPV-negative PCa. OR: odds ratio for HPV (Positive/Negative)
Next, the mutation differences of genes were compared between these two groups. Using Cancer Gene Census (CGC), a curated list of 736 known cancer genes [21], we compared cancer genes in the most frequently mutated gene list (> 8% of samples) in our cohort. Genes that have been previously reported as significantly mutated genes (SMGs) of Asian PCa [10] were also compared. Among the 11 SMGs, HPV-positive patients showed higher alteration frequencies in SYNE1, KMT2C, and KMT2D. SPOP, FOXA1, ATM, and APC mutations were observed only in the HPV-negative group. Among the other five CGC genes, HPV-positive patients showed a higher alteration frequency for CSMD3 and FAT1, and MED12 mutation was observed only in the HPV-negative group, but these differences did not reach statistical significance (P \(>\) 0.05) (Fig. 1C).
CNV analysis
A total of 5719 CNVs were identified in the 59 PCa samples, including 2358 amplifications (526 in the positive group and 1832 in the negative group) and 3361 deletions (683 in the positive group and 2678 in the negative group). The CNVs per sample are depicted and compared in Fig. 2A. No differences were observed in either amplifications (P = 0.840) or in deletions (P = 0.824) between these two groups. The most frequent gains were in chromosomes 7p, 7q, and 8q and losses in chromosomes 8p and 16q, similar in the two groups (Fig. 2B). In total, we identified two amplification peaks and eight deletion peaks in the HPV-positive group, and 17 amplification peaks and 36 deletion peaks in the HPV-negative group (Fig. 2B and Additional file 6: Table S3). When comparing these recurrent peaks, we found one common amplification peak and three common deletion peaks between the two different HPV status groups (Fig. 2C, D). We found a clear difference in the CGC genes contained in each wide peak (Fig. 2B and Additional file 6: Table S3). No amplification of oncogenes was identified in the HPV-positive group, but two amplifications of oncogenes were identified in the HPV-negative group: FCGR2B (1q23.3, five cases) and CCND1 (11q13.3, five cases). Twenty-nine deletions of key tumor suppressor genes (TSGs) were identified in the HPV-positive group, including ARNT (1q21.2, two cases), JAK1 (1q21.2, two cases), and NOTCH2 (1q21.2, two cases); 22 deletions of TSGs were identified in the HPV-negative group, including CCNC (6q16.3, 22 cases), RB1 (13q21.1, 17 cases), RAD17 (5q35.3, 11 cases), MAP3K1 (5q13.2, 11 cases), and PIK3R1 (5q13.2, 11 cases). Interestingly, in one of the common deletion peaks 1q21.2, all 29 TSGs, including ARNT, JAK1, and NOTCH2, were only contained in the HPV-positive group peak (not in the HPV-negative group peak).

Distribution of CNVs in our cohort. A Comparison of CNVs between the HPV-positive group and HPV-negative group. P = 0.840 is determined by the Mann–Whitney U test in copy number amplifications and P = 0.824 in copy number deletions. B Focal-level somatic CNV events. Red and blue denoted amplification and deletion, respectively. Chromosomal locations of peaks of significantly recurring focal amplification and deletion are filtered by FDRs. Peaks are annotated with amplification of candidate oncogenes or deletion of TSGs by cytoband (1q23.3(FCGR2B), 11q13.3(CCND1), 1q21.2(ARNT/JAK1), 5q13.2(MAP3K1/PIK3R1), 5q35.3(RAD17/APC), 6q16.3(CCNC), 11q22.3(ZBTB16/SDHD), 12p13.2(ETV6), and 13q21.1(RB1)). Heatmap of the CNAs of 10 HPV-positive samples (top) and 49 HPV-negative samples (bottom) in units of log2 (tumor/adjacent non-tumor) along the chromosomes. C, D Venn diagrams showing comparisons of recurrent peaks between the HPV-positive group and HPV-negative group
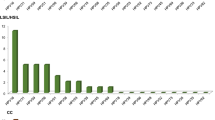
We then combined mutations and focal CNVs to define an enlarged list of putative HPV-related genes. We implemented the mafCompare function to identify differentially mutated CGC genes between the HPV-positive and HPV-negative groups, with the mutation load for each gene being compared by Fisher’s exact tests. Comparisons of these two groups revealed 55 differentially altered genes (P \(<\) 0.05) (Additional file 7: Table S4). By utilizing PRISM dataset (https://depmap.org/portal/prism/) [22], we attempted to identify potential drug targets among the 55 genes mentioned above. In the HPV-positive group, 13 targetable mutations and copy number aberrations were found, while in the HPV-positive group, one targetable copy number deletion was identified. These genes have been individually annotated in Additional file 7: Table S4. Figure 3 shows the comparison of 11 genes with ≥ three alterations (nonsynonymous mutation, copy number amplification or copy number deletion) among the 59 PCa samples. Among them, ERCC2, ATP1A1, DDR2, LMNA, and THRAP3 were significantly enriched only in the HPV-positive group. CCNC, RB1, and CYSLTR2 were significantly enriched only in the HPV-negative group.

Cohort comparison analysis. Differentially mutated genes between HPV-positive group and HPV-negative group are displayed as a bar plot. Orange and blue denote mutation and deletion, respectively. The adjacent table includes the number of samples in each group with the alterations in the highlighted gene. M, nonsynonymous mutation; A, amplification; D, deletion. P value indicates the significance threshold. *P < 0.05, **P < 0.01 was determined by Fisher’s exact test
Discussion
HPV infection is the most common sexually transmitted infection worldwide. Although the vast majority of infections disappear within 1 to 2 years, persistent hrHPV infection is responsible for virtually all cervical and anal cancers, 70% of vaginal and vulvar cancers, and a large percentage of penile cancers [23].
The majority of previous studies on assessment of HPV prevalence in PCa applied PCR methods that can only detect a limited number of HPV genotypes. Additional factors such as the multifocal feature of PCa and detection using biopsy specimens may contribute to poor specificity for HPV detection. Several studies examined hrHPV infection in PCa, and the frequency varied in a vast range from 2 to 75% [24]. In this study, we applied a hybrid capture-based NGS assay to FFPE samples, which enlarged the pool of HPV types to search for 15 types of hrHPV and effectively enabled us to determine HPV genotypes and integration status with high sensitivity. Moreover, capture sequencing can robustly detect multiple hrHPV infections [25]. In our study, HPV DNA was detected in 16.9% of patients with PCa, with HPV16 being the most frequent genotype and 20% of HPV-positive cases were multiple-type coinfections. These data indicate that the burden of HPV infection in men and the male genitourinary tract might serve as a reservoir of HPV transmission to women.
Many studies have focused on the Western population, whereas only a few have profiled molecular signatures in PCas in Asian. We performed WES to analyze genomic alterations in Chinese PCa patients and conducted comparative analysis of genomic differences between HPV-positive and HPV-negative groups. The mutational spectrum in HPV-negative PCa with enrichment for mutations in SPOP, FOXA1, and MED12 is very similar to that previously reported for PCa [26]. Of note, no SPOP, FOXA1, or MED12 mutations were observed in the HPV-positive PCa group. Preclinical studies have revealed that mutations in SPOP promote genetic instability in PCa and drive prostate tumorigenesis through coordinated regulation of PI3K/mTOR and AR signaling [27]. FOXA1 is essential for prostate organogenesis and functions as an oncoprotein that increases transcription of androgen receptor (AR) to drive metastatic progression [28]. Recent evidence suggests that patients with FOXA1 mutations have less favorable prognosis [10]. It has also been proposed that MED12 mutations in PCa may disrupt the androgen signaling pathway and CDK8-dependent transcriptional regulation of p53 [26].
In contrast, HPV-positive PCa showed distinct alterations with top mutations in KMT2B, CSMD3, ERCC2, and KMT2D. A recent study reported that KMT2B facilitates cervical cancer metastasis and angiogenesis by upregulating EGF expression. KMT2B, along with KMT2C and KMT2D, belongs to the lysine methyltransferase 2 (KMT2) family. The KMT2 family members are important regulators of gene transcription in cancer [29]. Given the increasing focus on abnormal epigenetic regulation in cancer, further investigation of involvement of the KMT2 family in HPV-positive PCa is needed. ERCC group genes are key factors in DNA transcription and the nucleotide excision repair pathway, which is an important DNA repair mechanism. It has been demonstrated that deficiency in the DNA repair gene ERCC2 has a central role in modulation of PCa susceptibility. ERCC2 polymorphism was observed to be related to increased risk in the Asian PCa population [30].
Next, we found comparable average CNVs between the HPV-positive and HPV-negative groups. The number of recurrent amplification or deletion peaks was much lower in the HPV-positive group, and each wide peak contained a completely different composition of candidate cancer genes. Among the 29 deletions of key TSGs identified in the HPV-positive group, JAK1 was previously found to promote sensitivity to docetaxel in PCa cells. Further drug–gene interaction analyses identified that combination therapy with JAK1 inhibitors and docetaxel may be useful in PCa treatment. Loss-of-function JAK1 mutations occur at high frequency in cancers with MSI and represent a potential pancancer adaptation of immune evasion [31]. NTRK1, another TSG deletion identified in the HPV-positive group, is recognized as a prognostic marker of primary PCa. Downregulation of NTRK1 is linked to poor prognosis in PCa, and NTRK1 expression correlates significantly with immune cell infiltration levels [32].
Our study presents novel somatic alterations in cancer-related genes in HPV-positive PCa, e.g., ATP1A1, DDR2, LMNA, THRAP3, CSF3R, and DICER1. To our knowledge, these mutations have not been previously described in PCa, and DICER1 mutation is of particular interest. DICER1 syndrome [33] is an autosomal dominant familial tumor predisposition disorder involving a heterozygous DICER1 germline mutation. Mutation of DICER1 results in the susceptibility to a variety of malignant tumors.
Precision oncology in PCa is rapidly evolving. In this study, we focused on the specific genetic events in HPV-positive and HPV-negative PCa likely contribute to the distinct biologic behavior. Today, the HPV vaccination program has been extended to prevent increasing incidence of HPV-related cancers, and HPV-positive PCa as a unique subpopulation might benefit from HPV vaccination. Besides, genomic testing is increasingly common, as biomarker-guided therapies are approved for specific individuals harboring genetic alterations in DNA repair genes such as BRCA [34, 35]. Here, we identified a series of potential therapeutic targets through tissue-based sequencing. HPV-positive PCas were characterized by mutations in KMT2C, KMT2D and ERCC2. Copy number deletions in NTRK1 and JAK1 were also discovered. These driver genes may serve as therapeutic targets for HPV-positive PCa. Mutations in SPOP, FOXA1, and MED12 were identified exclusively as driver genes in HPV-negative PCa as potential therapeutic targets. Additionally, these distinct genomic alterations identified in different HPV status subgroups, either individually or in combination as a panel, may serve as characteristic biomarkers for future liquid biopsies of HPV-positive or HPV-negative PCa [36]. These biomarkers could be utilized for early detection, treatment stratification, or recurrence monitoring. However, the therapeutic implications of these distinct gene aberrations in PCa require investigation and validation in future studies.
Limitations
One primary limitation of this study was the small sample size of 59 patients in our cohort. Second, this is a retrospective study and the proportion of HPV-positive patients is relatively low. Therefore, expanding the sample size and conducting a prospective randomized trial are required to provide stronger evidence.
Conclusion
Here, we provide HPV capture sequencing as a valuable approach for HPV-related PCa screening. The HPV-positive group had several genomic features that differed from the negative group in specific mutations and TSGs with CNV. These characteristics render HPV-positive PCa a unique subpopulation that might benefit from HPV vaccination and virus-targeted therapy. Furthermore, detecting HPV infection and mutation characteristics in PCa patients can guide personalized treatment, future studies of clinical implications of the observed mutations will be vital.
Availability of data and materials
All data generated or analyzed during the current study are available in the main text or the additional files. Sequencing data generated in this study are available through corresponding author Yan upon request.
Change history
26 June 2024
A Correction to this paper has been published: https://doi.org/10.1186/s40001-024-01935-z
Abbreviations
- PCa:
-
Prostate cancer
- TCGA:
-
The Cancer Genome Atlas
- HPV:
-
Human papillomavirus
- hrHPV:
-
High-risk HPV
- OR:
-
Odds ratio
- WES:
-
Whole-exome sequencing
- FFPE:
-
Formalin-fixed, paraffin-embedded
- CNV:
-
Copy number variation
- indels:
-
Insertions and deletions
- SMGs:
-
Significantly mutated genes
- TSG:
-
Tumor suppressor genes
- AR:
-
Androgen receptor
- PARP:
-
Poly-ADP ribose polymerase
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
Xia C, Dong X, Li H, Cao M, Sun D, He S, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chin Med J (Engl). 2022;135(5):584–90.
Moghoofei M, Keshavarz M, Ghorbani S, Babaei F, Nahand JS, Tavakoli A, et al. Association between human papillomavirus infection and prostate cancer: a global systematic review and meta-analysis. Asia Pac J Clin Oncol. 2019;15(5):e59–67.
Yin B, Liu W, Yu P, Liu C, Chen Y, Duan X, et al. Association between human papillomavirus and prostate cancer: a meta-analysis. Oncol Lett. 2017;14(2):1855–65.
Lawson JS, Glenn WK. Evidence for a causal role by human papillomaviruses in prostate cancer—a systematic review. Infect Agent Cancer. 2020;15:41.
Khatami A, Nahand JS, Kiani SJ, Khoshmirsafa M, Moghoofei M, Khanaliha K, et al. Human papilloma virus (HPV) and prostate cancer (PCa): the potential role of HPV gene expression and selected cellular MiRNAs in PCa development. Microb Pathog. 2022;166:105503.
Sadri Nahand J, Esghaei M, Hamidreza Monavari S, Moghoofei M, Jalal Kiani S, Mostafaei S, et al. The assessment of a possible link between HPV-mediated inflammation, apoptosis, and angiogenesis in Prostate cancer. Int Immunopharmacol. 2020;88:106913.
Porter VL, Marra MA. The drivers, mechanisms, and consequences of genome instability in HPV-driven cancers. Cancers (Basel). 2022;14(19):4623.
Cancer Genome Atlas Research. The molecular taxonomy of primary prostate cancer. Cell. 2015;163(4):1011–25.
Li J, Xu C, Lee HJ, Ren S, Zi X, Zhang Z, et al. A genomic and epigenomic atlas of prostate cancer in Asian populations. Nature. 2020;580(7801):93–9.
Tian R, Cui Z, He D, Tian X, Gao Q, Ma X, et al. Risk stratification of cervical lesions using capture sequencing and machine learning method based on HPV and human integrated genomic profiles. Carcinogenesis. 2019;40(10):1220–8.
Tian R, Wang Y, Li W, Cui Z, Pan T, Jin Z, et al. Genome-wide virus-integration analysis reveals a common insertional mechanism of HPV, HBV and EBV. Clin Transl Med. 2022;12(8):e971.
Vasimuddin M, Misra S, Li H, Aluru S. Efficient architecture-aware acceleration of BWA-MEM for multicore systems. In: 2019 IEEE international parallel and distributed processing symposium (IPDPS) 2019. p. 314–24.
Wang K, Li M, Hakonarson H. ANNOVAR: functional annotation of genetic variants from high-throughput sequencing data. Nucleic Acids Res. 2010;38(16):e164.
Li H, Handsaker B, Wysoker A, Fennell T, Ruan J, Homer N, et al. The sequence alignment/map format and SAMtools. Bioinformatics (Oxf, Engl). 2009;25(16):2078–9.
DePristo MA, Banks E, Poplin R, Garimella KV, Maguire JR, Hartl C, et al. A framework for variation discovery and genotyping using next-generation DNA sequencing data. Nat Genet. 2011;43(5):491–8.
Cibulskis K, Lawrence MS, Carter SL, Sivachenko A, Jaffe D, Sougnez C, et al. Sensitive detection of somatic point mutations in impure and heterogeneous cancer samples. Nat Biotechnol. 2013;31(3):213–9.
Mayakonda A, Lin D-C, Assenov Y, Plass C, Koeffler HP. Maftools: efficient and comprehensive analysis of somatic variants in cancer. Genome Res. 2018;28(11):1747–56.
Shen R, Seshan VE. FACETS: allele-specific copy number and clonal heterogeneity analysis tool for high-throughput DNA sequencing. Nucleic Acids Res. 2016;44(16):e131.
Mermel CH, Schumacher SE, Hill B, Meyerson ML, Beroukhim R, Getz G. GISTIC2.0 facilitates sensitive and confident localization of the targets of focal somatic copy-number alteration in human cancers. Genome Biol. 2011;12(4):R41.
Sondka Z, Bamford S, Cole CG, Ward SA, Dunham I, Forbes SA. The COSMIC Cancer Gene Census: describing genetic dysfunction across all human cancers. Nat Rev Cancer. 2018;18(11):696–705.
Steven MC, Rohith TN, Ryan DS, Jordan R, Mustafa K, Jordan GB, et al. Non-oncology drugs are a source of previously unappreciated anti-cancer activity. bioRxiv. 2019:730119.
de Martel C, Plummer M, Vignat J, Franceschi S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int J Cancer. 2017;141(4):664–70.
Lawson JS, Glenn WK. Multiple pathogens and prostate cancer. Infect Agent Cancer. 2022;17(1):23.
Zhang J, Tian X, Chen Y, Huang S, Cui Z, Tian R, et al. Feasibility and accuracy of menstrual blood testing for high-risk human papillomavirus detection with capture sequencing. JAMA Netw Open. 2021;4(12):e2140644.
Barbieri CE, Baca SC, Lawrence MS, Demichelis F, Blattner M, Theurillat J-P, et al. Exome sequencing identifies recurrent SPOP, FOXA1 and MED12 mutations in prostate cancer. Nat Genet. 2012;44(6):685–9.
Hjorth-Jensen K, Maya-Mendoza A, Dalgaard N, Sigurðsson JO, Bartek J, Iglesias-Gato D, et al. SPOP promotes transcriptional expression of DNA repair and replication factors to prevent replication stress and genomic instability. Nucleic Acids Res. 2018;46(18):9484–95.
Adams EJ, Karthaus WR, Hoover E, Liu D, Gruet A, Zhang Z, et al. FOXA1 mutations alter pioneering activity, differentiation and prostate cancer phenotypes. Nature. 2019;571(7765):408–12.
Zhai X, Brownell JE. Biochemical perspectives on targeting KMT2 methyltransferases in cancer. Trends Pharmacol Sci. 2021;42(8):688–99.
Liu Y, Hu Y, Zhang M, Jiang R, Liang C. Polymorphisms in ERCC2 and ERCC5 and risk of prostate cancer: a meta-analysis and systematic review. J Cancer. 2018;9(16):2786–94.
Albacker LA, Wu J, Smith P, Warmuth M, Stephens PJ, Zhu P, et al. Loss of function JAK1 mutations occur at high frequency in cancers with microsatellite instability and are suggestive of immune evasion. PLoS ONE. 2017;12(11):e0176181.
Bagherabadi A, Hooshmand A, Shekari N, Singh P, Zolghadri S, Stanek A, et al. Correlation of NTRK1 downregulation with low levels of tumor-infiltrating immune cells and poor prognosis of prostate cancer revealed by gene network analysis. Genes (Basel). 2022;13(5):840.
González IA, Stewart DR, Schultz KAP, Field AP, Hill DA, Dehner LP. DICER1 tumor predisposition syndrome: an evolving story initiated with the pleuropulmonary blastoma. Mod Pathol. 2022;35(1):4–22.
Mizuno K, Beltran H. Future directions for precision oncology in prostate cancer. Prostate. 2022;82(Suppl 1):S86–96.
Crocetto F, Barone B, Caputo VF, Fontana M, de Cobelli O, Ferro M. BRCA germline mutations in prostate cancer: the future is tailored. Diagnostics (Basel). 2021;11(5):908.
Crocetto F, Russo G, Di Zazzo E, Pisapia P, Mirto BF, Palmieri A, et al. Liquid biopsy in prostate cancer management-current challenges and future perspectives. Cancers (Basel). 2022;14(13):3272.
Acknowledgements
Not applicable.
Funding
This work was supported by the Initiation Research Fee for Special Talent Introduction of Dongzhimen Hospital Affiliated to Beijing University of Chinese Medicine (Grant no. 2014RC); the National Natural Science Foundation of China (Grant no. 32171465 and 82102392); General Program of Natural Science Foundation of Guangdong Province of China (Grant no. 2021A1515012438); Guangdong Basic and Applied Basic Research Foundation (Grant no. 2020A1515110170); the National Ten Thousand Plan-Young Top Talents of China (Grant no. 80000-41180002); Hubei Public Health Young Top Talent Training Program; Macao Polytechnic University (Grant no. RP/ESCSD-05/2021).
Author information
Authors and Affiliations
Contributions
Study concept and design: YY, ZH, XT; acquisition of data: YC, XuZ, TZ, TL, WL; analysis and interpretation of data: BL, CC, TZ, WY; drafting of the manuscript: BL, CC, XiZ; critical revision of the manuscript for important intellectual content: YC, XuZ; statistical analysis: BL, XiZ, TL, WL; obtaining funding: YY, ZH; administrative, technical, or material support: ZH, XT; revision: JZ, YW. Supervision: YY, ZH, XT. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Central Hospital of Wuhan in China (WHZXKYL2022-047) and conducted in accordance with the Declaration of Helsinki. All patients provided signed informed consent before enrollment.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article has been revised: the grant number has been updated.
Supplementary Information
Additional file 1: Figure S1.
The HPV infection status of cohort. (A) The distribution of HPV single and coinfections in PCa. (B) The correlation between age and HPV infection status. P = 0.893 was determined by Welch’s t-test.
Additional file 2: Figure S2.
The average mutation density between HPV-positive and HPV-negative PCa groups when the 8 hypermutant tumors were excluded. P = 0.891 was determined by Welch’s t-test.
Additional file 3: Figure S3.
Oncoplot depicting the most recurrent somatic mutations in PCa cohort.
Additional file 4: Table S1.
The summary of WES quality control.
Additional file 5: Table S2.
The summary of somatic SNV and InDel.
Additional file 6: Table S3.
CNV information in our cohort. Related to Fig. 3.
Additional file 7: Table S4.
The summary of differentially altered genes between HPV-positvie and HPV-negative groups.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lang, B., Cao, C., Zhao, X. et al. Genomic alterations related to HPV infection status in a cohort of Chinese prostate cancer patients. Eur J Med Res 28, 239 (2023). https://doi.org/10.1186/s40001-023-01207-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01207-2