
Abstract
Purpose
The optimal time point for surgical resection of synchronous colorectal liver metastases (SCLMs) is still controversial. This meta-analysis evaluated the safety and long-term prognoses of simultaneous and staged resection of SCLM to provide a reference for clinical selection.
Methods
A systematic literature search for studies published by October 2022 was performed using PubMed, Web of Science, Embase, Scopus and Cochrane Library. The evaluated outcome parameters were total, gastrointestinal and hepatic complications, as well as perioperative mortality, intraoperative blood loss, total hospital stay, 5-year disease-free survival (DFS) and 5-year overall survival (OS).
Results
This meta-analysis included 22 nonrandomised and one randomised study comprising 4862 patients. The patients undergoing simultaneous resection of SCLM had similar total (OR = 0.88, 95% CI [0.66–1.19], P = 0.409), gastrointestinal (OR = 1.19, 95% CI [0.89–1.59], P = 0.241) and hepatic (OR = 1.04, 95% CI [0.83–1.31], P = 0.734) complications, as well as perioperative mortality (OR = 1.79, 95% CI [0.88–3.64], P = 0.108), 5-year DFS (HR = 1.26, 95% CI [0.96–1.66], P = 0.098) and 5-year OS (HR = 1.13, 95% CI [0.95–1.34], P = 0.164). Lower intraoperative blood loss (SMD = − 0.39, 95% CI [− 0.60 to − 0.18], P < 0.001) and shorter total hospital stay (WMD = − 5.43, 95% CI [− 7.29 to − 3.58], P < 0.001) were observed in the simultaneous-resection group versus the staged group.
Conclusions
Simultaneous resection is safe and effective for SCLM patients. The long-term prognosis is equivalent to that of the traditional staged resection. Correct selection of resectable SCLM patients for the simultaneous resection of the primary tumour and liver metastases can be the first choice. Owing to the potential heterogeneity, more RCTs should be included to verify our conclusions.
Similar content being viewed by others


Introduction
Colorectal cancer (CRC) is one of the most common malignant tumours worldwide [1]. According to the global cancer statistics in 2020 [2], the incidence and mortality of colorectal cancer ranked third and second, respectively. Because most mesenteric blood flows back to the portal vein, the liver is the most common metastatic site of colorectal cancer [3]. In fact, the liver is the only site with distant metastasis in approximately 20% of patients [4]. Approximately 15–25% of patients with CRC also present with synchronous liver metastases [5], a condition called synchronous colorectal liver metastases (SCLM). Patients with CRC who develop liver metastases are at a higher risk of death; the median overall survival (OS) of patients who cannot undergo surgery is 6–12 months [6]. Patients with SCLM can only be treated by resecting the metastases, representing the only hope for survival and cure [7, 8].
According to the time point of the surgery, resection of liver metastases can be classified into simultaneous resection (simultaneous resection of the primary tumour and liver metastases) and staged resection (resection of the primary tumour first, followed by resection of the metastases after 3–6 months) [9, 10]. Traditional views have advocated the staged strategy because previous findings have shown that simultaneous resection is highly traumatic and associated with higher perioperative complications and mortality rates than staged resection [11, 12]. The staged strategy also enables the identification of the small metastatic lesions in the liver or elsewhere that may be occult, in addition to the primary lesion. It is also possible to control the tumours via chemotherapy during the observation period after primary-tumour resection, which can provide a basis for selecting the subsequent chemotherapy regimen [13, 14]. A considerable number of studies have shown that in recent years, with the improvements in surgical operations and perioperative care, the mortality and perioperative complications after simultaneous resection have not been significantly different from those observed after staged resection [15, 16]. In addition, simultaneous resection prevents the loss of surgical opportunity that may result from tumour progression, as well as the physical and psychological trauma that a secondary surgery can cause to the patient [13, 17]. However, there is currently no consensus on the timing of the surgery for liver metastases derived from synchronous colorectal cancer. Therefore, this study compared the outcome parameters of the simultaneous surgery with those of the staged surgery, thereby providing a reference for the choice of the timing of surgery in SCLM.
Methods
PRISMA 2020 guidelines and AMSTAR guidelines were followed in conducting this meta-analysis [18]. The protocol has been registered on PROSPERO (CRD42021282727).
Search strategy
The databases of PubMed, Web of Science, Embase, Scopus and Cochrane Library were carefully screened for studies published by October 2022 by using the following keywords: “colorectal neoplasms,” “colorectal tumours,” “colorectal cancers,” “liver metastases,” “synchronous colorectal liver metastases,” “simultaneous resection,” “synchronous resection,” “staged resection,” and “delayed resection.” This search strategy was slightly adjusted to comply with the different database requirements and the references of the relevant articles were screened for additional relevant studies.
Inclusion and exclusion criteria
The inclusion criteria were defined based on the Population, Intervention, Comparison, Outcome and Study (PICOS) design principle as follows: (1) patients with SCLM (preoperatively or intraoperatively diagnosed with liver metastases; (2) both the primary colorectal tumour and liver metastases were resectable at the time of diagnosis; (3) the selected studies reported at least one outcome of interest; (5) when more than one report per study was available, the one with the best quality or published most recently was included in this analysis; (6) only randomised controlled trials (RCTs) and non-RCTs (nRCTs) published in English were included. Following were the exclusion criteria: (1) patients with extrahepatic metastases; (2) " liver first " resection (liver resection first, followed by primary-tumour resection); (3) studies lacking a control group or in which the control group was unreasonable; (4) a publication type which is not suitable (case reports, conference abstracts, meta-analyses, reviews and animals experiments); (5) reports not written in English; (6) low-quality studies; and (7) no original data could be obtained from the corresponding author.
Data extraction
Literature review, data extraction and quality assessment were independently performed by two reviewers (Shi-hao Wang and Lei Song). A full reading of the text resolved all inconsistencies between the two reviewers. The outcomes we focussed on were complications (including total as well as gastrointestinal and hepatic complications), perioperative characteristics (including perioperative mortality, intraoperative blood loss and total hospital stay) and long-term outcomes (including 5-year disease-free survival [DFS] and 5-year overall survival [OS]). The DFS and OS were calculated since the hepatectomy. Some outcome measures could not be obtained directly from the text and thus the following definitions were made: (1) gastrointestinal complications comprised anastomotic leakage, bleeding, ileus, colitis and abdominal and pelvic abscesses; (2) hepatic complications comprised perihepatic or subdiaphragmatic abscess, right-sided pleural effusion, bile leak and/or biloma and hepatic insufficiency or failure.
Quality evaluation
The Cochrane Risk of Bias Tool for Randomised Controlled Trials was used to evaluate the quality of the included RCT. nRCTs were evaluated using the Newcastle–Ottawa Quality Assessment Scale (NOS).
Statistical methods
The statistical analyses were carried out using the STATA software, version 14.0. Continuous variables were analysed using weighted/standardised mean differences (WMD/SMD) and 95% confidence intervals (CIs). Dichotomous variables were analysed using odds ratios (ORs) and 95% CIs. If mean values or standard deviations (SDs) were not provided in a report, we calculated the SDs from the median values and ranges using Wan et al.’s method [19]. If hazard ratios (HRs) and 95% CIs were not reported, the method published by Tierney et al. [20] was used to estimate the HR as the effect indicator to pool the survival statistics. Heterogeneity was measured using Cochran's Q test and the Chi-square test. The results were presented with the corresponding 95% CIs and statistical significance was set at P < 0.05. The random-effects model should be used as a default due to clinical heterogeneity among surgical trials [21]. If the studies were significantly heterogeneous (I2 > 50%), a sensitivity analysis was conducted using the leave-one-out approach to check the stability of the meta-analysis. In addition, subgroup analyses were performed on studies with NOS scores ≥ 7 and studies with more than 50 patients in the simultaneous group to assess consistency in data reporting. Finally, the studies were assessed for any publication bias using funnel plots and Begg's test.
Results
The basic characteristics about the included studies
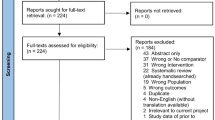
A total of 3597 publications were retrieved from the 5 databases and 23 of them were found eligible according to the specified inclusion and exclusion criteria (Fig. 1). In total, only 1 RCT [22] and 22 nRCTs [13, 14, 17, 23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41], comprising a total of 4862 patients (2056 and 2806 cases of simultaneous resection and staged resection, respectively) were included. All the nRCTs had a NOS score ≥ 6 and the RCT had a low bias risk, assessed using RevMan 5.3 (Fig. 2). The basic characteristics of the patients in the included studies are shown in Table 1.

Process of study selection

Methodological quality of the randomised controlled trial
The tumour characteristics in the included studies
We analysed the tumour characteristics, including whether neoadjuvant chemotherapy was administered, the sizes and number of metastases, unilobar or bilobar distribution and the number of metastases that required major resection (≥ 3 segments) or minor resection (< 3 segments), in the included studies. The rate of neoadjuvant chemotherapy was higher in the staged-resection group than in the simultaneous-resection group and the patients in the staged-resection group were more likely to undergo major resection of liver metastases than those in the simultaneous-resection group. These differences were all statistically significant. The remaining indicators, such as the sizes and number of metastases with unilobar or bilobar distribution, were not significantly different between the two groups. Table 2 shows the tumour characteristics in the included studies.
Complications
Total complications
A total of 17 articles described total complications; 479/1342 (35.69%) patients in the simultaneous-resection group and 667/1891 (35.27%) patients in the staged-resection group had total complications. Total complication rates between the two groups were not significantly different (OR = 0.88, 95% CI [0.66–1.19], P = 0.409; I2 = 61.3%; Fig. 3A).

Complications between two groups shown as a forest plot. A Total complications. B Gastrointestinal complications. C Hepatic complications
Gastrointestinal complications
Gastrointestinal complications were reported in 16 articles. In the simultaneous- and staged-resection groups, gastrointestinal complications occurred in 188/1358 (13.84%) and 186/1627 (11.43%) patients, respectively. There were no statistically significant differences between the two groups in terms of gastrointestinal complications (OR = 1.19, 95% CI [0.89–1.59], P = 0.208; I2 = 21.6%; Fig. 3B).
Hepatic complications
There were 17 publications describing hepatic complications, which occurred in 166/1398 (11.87%) patients in the simultaneous-resection group and 252/1806 (13.95%) patients in the staged-resection group. There was no statistically significant difference in hepatic complication rate between the two groups (OR = 1.04, 95% CI [0.83–1.31], P = 0.734; I2 = 0.0%; Fig. 3C).
Perioperative characteristics
Perioperative mortality
Perioperative mortality was reported in 10 publications. Based on the pooled outcome analysis, perioperative mortality was reported in 18/730 (2.47%) patients in the simultaneous-resection group and 20/1470 (1.36%) patients in the staged-resection group. Perioperative mortality did not significantly differ between the two groups (OR = 1.79, 95% CI [0.88–3.64], P = 0.108; I2 = 8.5%; Fig. 4A).

Forest plot of perioperative characteristics between two groups. A Perioperative mortality. B Intraoperative blood loss. C Total hospital stay
Intraoperative blood loss
A total of 10 publications reported intraoperative blood loss and the heterogeneity substantially decreased (from 91.4% to 69.1%) after excluding one publication [30] and thus 9 publications were included in the pooled analysis. The incidence of intraoperative blood loss in the simultaneous-resection group was significantly lower than that in the staged-resection group (SMD = –0.39, 95% CI [− 0.60 to − 0.18], P < 0.001; I2 = 69.1%; Fig. 4B).
Total hospital stay
Total hospital stay was reported in 14 articles and the heterogeneity substantially decreased (from 94.3% to 76.9%) after excluding one publication[40] and thus 13 publications were included in the pooled analysis. The average total hospital stay was five days shorter in the simultaneous resection than in the staged-resection group (WMD = –5.43, 95% CI [− 7.29 to − 3.58], P < 0.001; I2 = 76.9%; Fig. 4C).
Long-term prognosis
The 5-year DFS
A total of 4 publications reported the 5-year DFS, which was not significantly different between the simultaneous- and staged-resection groups (HR = 1.26, 95% CI [0.96–1.66], P = 0.098; I2 = 18.1%; Fig. 5A).

The forest plot compares long-term prognosis between two groups. A The 5-year DFS. B The 5-year OS
The 5-year OS
A total of 10 publications reported the 5-year OS, which was not significantly different between the simultaneous- and staged-resection groups (HR = 1.13, 95% CI [0.95–1.34], P = 0.164; I2 = 34.6%; Fig. 5B).
Each outcome is listed in Table 3.
Subgroup analysis
NOS score ≥ 7
Subgroup analysis of studies with NOS score ≥ 7 found that the intraoperative blood loss (SMD = − 0.50, P = 0.002) and total hospital stay (WMD = − 4.87, P < 0.001) were reduced in the simultaneous group, but there were no differences in total complications (OR = 0.82, P = 0.307), gastrointestinal complications (OR = 0.99, P = 0.973), hepatic complications (OR = 0.74, P = 0.207), perioperative mortality (OR = 2.29, P = 0.067), 5-year DFS (HR = 1.56, P = 0.234) and 5-year OS (HR = 1.11, P = 0.366).
More than 50 patients in the simultaneous group
Subgroup analysis was performed on the studies with more than 50 simultaneous group participants. The summary results showed that the intraoperative blood loss (WMD = − 239.90, P < 0.001) and the total hospital stay (WMD = − 1.17, P < 0.001) were reduced in the simultaneous group, but there were no differences in the total complications (OR = 1.05, P = 0.769), gastrointestinal complications (OR = 1.09, P = 0.673), hepatic complications (OR = 1.14, P = 0.315), perioperative mortality (OR = 1.00, P = 0.990), 5-year DFS (HR = 1.14, P = 0.412) and 5-year OS (HR = 1.16, P = 0.302). The results of all subgroup analyses are summarised in Additional file 1: Table S1.
Sensitivity analysis
Sensitivity analysis was carried out using the leave one-out approach. This analysis indicated that exclusion of any single study did not significantly affect the pooled results. The results of the meta-analysis were therefore concluded to be stable and reliable (Fig. 6).

Sensitivity analysis. A Total complications. B Intraoperative blood loss. C Total hospital stay
Publication bias
We assessed the funnel plot of the total complications for any publication bias. The funnel plot was found to be symmetrical, indicating a lack of publication bias (Fig. 7).

Funnel plot of the total postoperative complications (Begg's test, P = 0.149)
Discussion
It is estimated that 50% of patients with CRC develop liver metastases [42]. The current treatments for SCLM include surgical resection, radiofrequency ablation, cryosurgery, hepatic arterial infusion and systemic chemotherapy [43]. Although the combination of chemotherapy, molecular targeted therapy and radiotherapy prolongs the median survival time to 24 months [30], the 5-year OS rate of nonsurgically treated patients remains low [44]. Resection of liver metastases caused by colorectal cancer has been shown to be effective [45, 46]. However, it is still controversial whether simultaneous or staged resection is indicated for SCLM and no consensus regarding the surgery indications or timing has been reached yet [30, 38].
Several authors have reported that simultaneous resection is associated with poorer short-term outcomes than staged resection [47, 48]. However, several studies have also recently shown that simultaneous colorectal and liver surgery is feasible and safe [31, 32]. Growing evidence indicates that there is no significant difference in postoperative complication rate or perioperative mortality between simultaneous resection and staged resection of SCLMs [29, 34, 38]. Haas et al. [26] have analysed 228 patients with SCLM and observed a decreasing trend in the incidence of total postoperative complications when the liver metastases were removed via simultaneous resection instead of staged resection and there was no statistically significant difference between the two procedures in terms of perioperative mortality. Chua et al. [25] have reported that there is no significant difference between simultaneous and staged hepatectomy in terms of intraoperative blood loss, incidence of total postoperative complications, operative mortality, OS and length of hospital stay. Multiple scholars believe that simultaneous resection can impair the gastrointestinal function because the cumulative trauma of the two major surgeries in the intestine and liver causes the intestinal anastomoses to heal poorly and may even lead to anastomotic leakage [33]. Our pooled results showed no statistical difference between simultaneous resection and staged resection in terms of total, gastrointestinal and hepatic complications. Moreover, our results showed that simultaneous resection does not increase the complication rate, especially the rate of gastrointestinal complications or perioperative mortality.
The studies included in previous meta-analyses [15, 49] were all nRCTs and it is reassuring that our meta-analysis included the first RCT [22] to date on the surgery timing for SCLMs, thus adding credence to our conclusions. In this study, we analysed 85 patients ([39 and 46] in the simultaneous- and staged-resection groups, respectively) and found that the rates of colonic, hepatic and general complications and perioperative mortality were [28.2% and 13.0%], [15.4% and 17.4%], [12.8% and 23.9%] and [7.4% and 3.2%], respectively. The above outcomes were not statistically different between the two groups. Importantly, we found that the simultaneous-resection group showed significantly shorter total hospital stay and lower incidence of intraoperative blood loss than the staged-resection group, consistent with the results of previously published meta-analyses. In addition, simultaneous resection prevents the opportunity of surgical treatment from being missed due to tumour progression, eliminates the pain associated with a second open surgery and allows early surgical adjuvant chemotherapy [17, 35].
We also compared the 5-year DFS and OS rates of the two procedures to evaluate the long-term prognoses and there was no statistically significant difference between the two groups. The result was satisfactory from a clinical standpoint. Although synchronous metastases have been shown to have a negative prognostic value [50], they are not a contraindication to hepatectomy if a resection that can cure the cancer is possible [51, 52]. Thus, simultaneous resection is safe and feasible for patients with resectable SCLM who can tolerate the surgery and have no extrahepatic metastasis [10].
The advancements in imaging technologies in recent years have enabled on-time detection of early, isolated or small liver metastases [53]. With the continuous improvements in surgical technologies, anaesthetic approaches, and perinatal treatments, the safety of simultaneous hepatectomy to treat SCLM has been dramatically improved, which has increasingly been recognised by scholars [54, 55]. A few authors still argue that a 2–6-month waiting period between the resection of the primary tumour and liver resection is necessary for the presentation of any subclinical metastasis, thereby enabling complete tumour clearance [56]. According to a cascade hypothesis, metastases develop in discrete steps, first in the liver and then in the lungs [57]. Thus, it seems too risky to wait for several months after the resection of the primary tumour. It is worth noting that after analysing the tumour characteristics of the two groups in our analysis, we found differences between the two groups in terms of the method used for metastasis removal. The staged-resection group had more cases of major resection of liver metastasis than the simultaneous-resection group. This observation indicates that patients with complex liver tumours require major resection and are more likely to undergo staged resection than simultaneous resection and also emphasises the importance of patient selection [17]. Although such selection bias may be reasonable, it may reduce the credibility of the evidence.
Our subgroup analyses showed consistency in the results, based on our results and previous studies, the optimum treatment for simultaneous liver metastasis should be based on the symptoms and general conditions of the patient, tumour location and degree, and whether there are other potential systemic diseases [29]. Staged hepatectomy can be considered for patients with advanced colorectal cancer who cannot tolerate surgery or have extrahepatic metastasis [28]. It is still noteworthy that minimally invasive surgery, represented by laparoscopic surgery, has been the main direction established in terms of surgical development in the future [58, 59]; the application of laparoscopic surgery for resection in CRLM has increased recently. Multiple retrospective studies [60,61,62] have shown a laparoscopic approach for CRLM to be safe, feasible and oncologically efficient when compared with traditional laparotomy. Although the laparoscopic resection for CRLM has made significant progress in the past 20 years, it is still an operation with high difficulty. In the process of laparoscopic resection for CRLM, the indications should be strictly followed and the laparotomy should be converted in time if necessary. Therefore, laparoscopic resection for CRLM is a safe and feasible option in qualified medical units. CRLM-related prognostic biomarkers have attracted increasing attention as a means of predicting prognosis. In some studies [63, 64], the preoperative lymphocyte-to-monocyte ratio (LMR) correlates accurately with clinical outcomes in patients with CRLM undergoing hepatic resection. However, the included studies need more data to facilitate such an analysis.
There are several limitations in the present study. First, the majority of the included studies were nRCTs and only one RCT was included, which might affect the quality of the data. Second, the tumour characteristics in each group were not exactly the same. Third, the lack of individual data from each study does not allow in-depth analyses. Although we used the random-effect model instead of the fixed-effect model, we still cannot exclude any possibility of bias. Nevertheless, only one RCT study is still meaningful and provides a valuable reference for our summary results.
Conclusion
For the treatment of SCLM, simultaneous colectomy and hepatectomy are as safe as the staged approach. It does not increase the number of postoperative complications or perioperative mortality and can shorten the hospital stay and reduce the incidence of intraoperative bleeding. In terms of long-term prognosis, simultaneous resection is equivalent to staged resection. Therefore, simultaneous resection can be considered the first choice for the resection of the primary tumour and liver metastasis, provided that patients with resectable SCLM are carefully selected and the operation is performed by experienced staff.
Availability of data and materials
Data and materials will be available upon request.
References
Feng J, Yang M, Wei Q, Song F, Zhang Y, Wang X, et al. Novel evidence for oncogenic piRNA-823 as a promising prognostic biomarker and a potential therapeutic target in colorectal cancer. J Cell Mol Med. 2020;24(16):9028–40.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49.
Yang C, Zhang Y, Du W, Cheng H, Li C. Eukaryotic translation initiation factor 3 subunit G promotes human colorectal cancer. Am J Transl Res. 2019;11(2):612–23.
Chen JC, Hsieh YY, Lo HL, Li A, Chou CJ, Yang PM. In vitro and in silico mechanistic insights into miR-21–5p-mediated topoisomerase drug resistance in human colorectal cancer cells. Biomolecules. 2019;9(9):467.
Palkovics A, Vereczkei A, Fincsur A, Kiss I, Nemeth B, Takacs I, et al. Short- and long-term histological changes in liver parenchyma after different resection methods and their potential role in treatment of colorectal liver metastasis. Anticancer Res. 2020;40(3):1359–65.
Tanaka M, Kishi Y, Esaki M, Nara S, Miyake M, Hiraoka N, et al. Feasibility of routine application of gadoxetic acid-enhanced mri in combination with diffusion-weighted MRI for the preoperative evaluation of colorectal liver metastases. Ann Surg Oncol. 2016;23(12):3991–8.
Puijk RS, Ruarus AH, Vroomen L, van Tilborg A, Scheffer HJ, Nielsen K, et al. Colorectal liver metastases: surgery versus thermal ablation (COLLISION)—a phase III single-blind prospective randomized controlled trial. BMC Cancer. 2018;18(1):821.
Boileve A, Maillard A, Wagner M, Dromain C, Laurent C, Dupont Bierre E, et al. Treatment intensification with hepatic arterial infusion chemotherapy in patients with liver-only colorectal metastases still unresectable after systemic induction chemotherapy—a randomized phase II study—SULTAN UCGI 30/PRODIGE 53 (NCT03164655)—study protocol. BMC Cancer. 2020;20(1):74.
Serrano PE, Gafni A, Parpia S, Ruo L, Simunovic M, Meyers BM, et al. Simultaneous resection of colorectal cancer with synchronous liver metastases (RESECT), a pilot study. Int J Surg Protoc. 2018;8:1–6.
Fei F, Zhou Z, Shen Y, Su Z. Comparison of the effects and prognosis of concurrent and staged resections for the treatment of resectable colorectal cancer liver metastasis. Am J Transl Res. 2021;13(4):3634–41.
Fukami Y, Kaneoka Y, Maeda A, Takayama Y, Onoe S, Isogai M. Simultaneous resection for colorectal cancer and synchronous liver metastases. Surg Today. 2016;46(2):176–82.
Nanji S, Mackillop WJ, Wei X, Booth CM. Simultaneous resection of primary colorectal cancer and synchronous liver metastases: a population-based study. Can J Surg. 2017;60(2):122–8.
She WH, Chan AC, Poon RT, Cheung TT, Chok KS, Chan SC, et al. Defining an optimal surgical strategy for synchronous colorectal liver metastases: staged versus simultaneous resection? ANZ J Surg. 2015;85(11):829–33.
Yan TD, Chu F, Black D, King DW, Morris DL. Synchronous resection of colorectal primary cancer and liver metastases. World J Surg. 2007;31(7):1496–501.
Gavriilidis P, Sutcliffe RP, Hodson J, Marudanayagam R, Isaac J, Azoulay D, et al. Simultaneous versus delayed hepatectomy for synchronous colorectal liver metastases: a systematic review and meta-analysis. HPB (Oxford). 2018;20(1):11–9.
Yin Z, Liu C, Chen Y, Bai Y, Shang C, Yin R, et al. Timing of hepatectomy in resectable synchronous colorectal liver metastases (SCRLM): simultaneous or delayed? Hepatology. 2013;57(6):2346–57.
Martin RC 2nd, Augenstein V, Reuter NP, Scoggins CR, McMasters KM. Simultaneous versus staged resection for synchronous colorectal cancer liver metastases. J Am Coll Surg. 2009;208(5):842–50 (discussion 50–2).
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88: 105906.
Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135.
Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007;8:16.
Kalkum E, Klotz R, Seide S, Huttner FJ, Kowalewski KF, Nickel F, et al. Systematic reviews in surgery-recommendations from the Study Center of the German Society of Surgery. Langenbecks Arch Surg. 2021;406(6):1723–31.
Boudjema K, Locher C, Sabbagh C, Ortega-Deballon P, Heyd B, Bachellier P, et al. Simultaneous versus delayed resection for initially resectable synchronous colorectal cancer liver metastases: a prospective, open-label, randomized. Controlled Trial Ann Surg. 2021;273(1):49–56.
Abbott DE, Cantor SB, Hu CY, Aloia TA, You YN, Nguyen S, et al. Optimizing clinical and economic outcomes of surgical therapy for patients with colorectal cancer and synchronous liver metastases. J Am Coll Surg. 2012;215(2):262–70.
Capussotti L, Ferrero A, Vigano L, Ribero D, Lo Tesoriere R, Polastri R. Major liver resections synchronous with colorectal surgery. Ann Surg Oncol. 2007;14(1):195–201.
Chua HK, Sondenaa K, Tsiotos GG, Larson DR, Wolff BG, Nagorney DM. Concurrent vs. staged colectomy and hepatectomy for primary colorectal cancer with synchronous hepatic metastases. Dis Colon Rectum. 2004;47(8):1310–6.
de Haas RJ, Adam R, Wicherts DA, Azoulay D, Bismuth H, Vibert E, et al. Comparison of simultaneous or delayed liver surgery for limited synchronous colorectal metastases. Br J Surg. 2010;97(8):1279–89.
Kaibori M, Iwamoto S, Ishizaki M, Matsui K, Saito T, Yoshioka K, et al. Timing of resection for synchronous liver metastases from colorectal cancer. Dig Dis Sci. 2010;55(11):3262–70.
Kye BH, Lee SH, Jeong WK, Yu CS, Park IJ, Kim HR, et al. Which strategy is better for resectable synchronous liver metastasis from colorectal cancer, simultaneous surgery, or staged surgery? Multicenter retrospective analysis. Ann Surg Treat Res. 2019;97(4):184–93.
Le Souder EB, Azin A, Hirpara DH, Walker R, Cleary S, Quereshy F. Considering the cost of a simultaneous versus staged approach to resection of colorectal cancer with synchronous liver metastases in a publicly funded healthcare model. J Surg Oncol. 2018;117(7):1376–85.
Luo Y, Wang L, Chen C, Chen D, Huang M, Huang Y, et al. Simultaneous liver and colorectal resections are safe for synchronous colorectal liver metastases. J Gastrointest Surg. 2010;14(12):1974–80.
Martin R, Paty P, Fong Y, Grace A, Cohen A, DeMatteo R, et al. Simultaneous liver and colorectal resections are safe for synchronous colorectal liver metastasis. J Am Coll Surg. 2003;197(2):233–41 (discussion 41–2).
Moug SJ, Smith D, Leen E, Roxburgh C, Horgan PG. Evidence for a synchronous operative approach in the treatment of colorectal cancer with hepatic metastases: a case matched study. Eur J Surg Oncol. 2010;36(4):365–70.
Thelen A, Jonas S, Benckert C, Spinelli A, Lopez-Hanninen E, Rudolph B, et al. Simultaneous versus staged liver resection of synchronous liver metastases from colorectal cancer. Int J Colorectal Dis. 2007;22(10):1269–76.
Tsilimigras DI, Sahara K, Hyer JM, Diaz A, Moris D, Bagante F, et al. Trends and outcomes of simultaneous versus staged resection of synchronous colorectal cancer and colorectal liver metastases. Surgery. 2021;170(1):160–6.
Turrini O, Viret F, Guiramand J, Lelong B, Bege T, Delpero JR. Strategies for the treatment of synchronous liver metastasis. Eur J Surg Oncol. 2007;33(6):735–40.
Valdimarsson VT, Syk I, Lindell G, Sandstrom P, Isaksson B, Rizell M, et al. Outcomes of simultaneous resections and classical strategy for synchronous colorectal liver metastases in Sweden: a nationwide study with special reference to major liver resections. World J Surg. 2020;44(7):2409–17.
Vassiliou I, Arkadopoulos N, Theodosopoulos T, Fragulidis G, Marinis A, Kondi-Paphiti A, et al. Surgical approaches of resectable synchronous colorectal liver metastases: timing considerations. World J Gastroenterol. 2007;13(9):1431–4.
Weber JC, Bachellier P, Oussoultzoglou E, Jaeck D. Simultaneous resection of colorectal primary tumour and synchronous liver metastases. Br J Surg. 2003;90(8):956–62.
Karam E, Bucur P, Gil C, Sindayigaya R, Tabchouri N, Barbier L, et al. Simultaneous or staged resection for synchronous liver metastasis and primary rectal cancer: a propensity score matching analysis. BMC Gastroenterol. 2022;22(1):201.
Thongkan T, Wiboonkhwan N-A, Pitakteerabundit T, Wanitsuwan W, Boonpipattanapong T. Simultaneous hepatectomy as a safe approach for synchronous colorectal liver metastasis. J Health Sci Med Res. 2020;39:115.
Wu Y, Mao A, Wang H, Fang G, Zhou J, He X, et al. Association of simultaneous vs delayed resection of liver metastasis with complications and survival among adults with colorectal cancer. JAMA Netw Open. 2022;5(9): e2231956.
Tilgase A, Grine L, Blake I, Boroduskis M, Rasa A, Alberts P. Effect of oncolytic ECHO-7 virus strain Rigvir on uveal melanoma cell lines. BMC Res Notes. 2020;13(1):222.
Hazhirkarzar B, Khoshpouri P, Shaghaghi M, Ghasabeh MA, Pawlik TM, Kamel IR. Current state of the art imaging approaches for colorectal liver metastasis. Hepatobiliary Surg Nutr. 2020;9(1):35–48.
Loosen SH, Heise D, Dejong CH, Roy S, Tacke F, Trautwein C, et al. Circulating Levels of osteopontin predict patients’ outcome after resection of colorectal liver metastases. J Clin Med. 2018;7(11):390.
Park J, Lee SD, Han SS, Kim SH, Park SJ, Oh JH, et al. Repeat hepatectomy for recurred colorectal liver metastasis: is it justified? Ann Surg Treat Res. 2019;97(1):7–14.
Lv Y, Ji ML, Feng QY, Zhu DX, Lin SB, Mao YH, et al. Combined test of third lumbar skeletal muscle index and prognostic nutrition index improve prognosis prediction power in resected colorectal cancer liver metastasis. Aging (Albany NY). 2019;11(22):10301–15.
Wang LJ, Wang HW, Jin KM, Li J, Xing BC. Comparison of sequential, delayed and simultaneous resection strategies for synchronous colorectal liver metastases. BMC Surg. 2020;20(1):16.
Snyder RA, Hao S, Irish W, Zervos EE, Tuttle-Newhall JE, Parikh AA. Thirty-day morbidity after simultaneous resection of colorectal cancer and colorectal liver metastasis: American College of Surgeons NSQIP Analysis. J Am Coll Surg. 2020;230(4):617-27e9.
Slesser AA, Simillis C, Goldin R, Brown G, Mudan S, Tekkis PP. A meta-analysis comparing simultaneous versus delayed resections in patients with synchronous colorectal liver metastases. Surg Oncol. 2013;22(1):36–47.
Tang J, Zhang C, Huang Y, Wang L, Xu Z, Zhang D, et al. CircRNA circ_0124554 blocked the ubiquitination of AKT promoting the skip lymphovascular invasion on hepatic metastasis in colorectal cancer. Cell Death Dis. 2021;12(3):270.
Molla NW, Hassanain MM, Fadel Z, Boucher LM, Madkhali A, Altahan RM, et al. Effect of non-alcoholic liver disease on recurrence rate and liver regeneration after liver resection for colorectal liver metastases. Curr Oncol. 2017;24(3):e233–43.
Desjardin M, Bonhomme B, Le Bail B, Evrard S, Brouste V, Desolneux G, et al. Hepatotoxicities induced by neoadjuvant chemotherapy in colorectal cancer liver metastases: distinguishing the true from the false. Clin Med Insights Oncol. 2019;13:1179554918825450.
Nishikado A, Kawata R, Haginomori SI, Terada T, Higashino M, Kurisu Y, et al. A clinicopathological study of parotid carcinoma: 18-year review of 171 patients at a single institution. Int J Clin Oncol. 2018;23(4):615–24.
Chen X, Yan S, Zhao H, Zhang Y, Huang Z, Zhao J, et al. The safety and feasibility of a single incision in simultaneous resection for patients with colorectal cancer liver metastases. Ann Transl Med. 2019;7(20):547.
Wu Y, Guo T, Xu Z, Liu F, Cai S, Wang L, et al. Risk scoring system for recurrence after simultaneous resection of colorectal cancer liver metastasis. Ann Transl Med. 2021;9(12):966.
Jenkins LT, Millikan KW, Bines SD, Staren ED, Doolas A. Hepatic resection for metastatic colorectal cancer. Am Surg. 1997;63(7):605–10.
Tsukamoto S, Kinugasa Y, Yamaguchi T, Shiomi A. Survival after resection of liver and lung colorectal metastases in the era of modern multidisciplinary therapy. Int J Colorectal Dis. 2014;29(1):81–7.
Sheen AJ, Jamdar S, Siriwardena AK. Laparoscopic hepatectomy for colorectal liver metastases: the current state of the art. Front Oncol. 2019;9:442.
Xu X, Guo Y, Chen G, Li C, Wang H, Dong G. Laparoscopic resections of colorectal cancer and synchronous liver metastases: a case controlled study. Minim Invasive Ther Allied Technol. 2018;27(4):209–16.
Wakabayashi G, Cherqui D, Geller DA, Buell JF, Kaneko H, Han HS, et al. Recommendations for laparoscopic liver resection: a report from the second international consensus conference held in Morioka. Ann Surg. 2015;261(4):619–29.
Xie SM, Xiong JJ, Liu XT, Chen HY, Iglesia-Garcia D, Altaf K, et al. Laparoscopic versus open liver resection for colorectal liver metastases: a comprehensive systematic review and meta-analysis. Sci Rep. 2017;7(1):1012.
Zhong JH, Peng NF, Gu JH, Zheng MH, Li LQ. Is laparoscopic hepatectomy superior to open hepatectomy for hepatocellular carcinoma? World J Hepatol. 2017;9(4):167–70.
Facciorusso A, Del Prete V, Crucinio N, Serviddio G, Vendemiale G, Muscatiello N. Lymphocyte-to-monocyte ratio predicts survival after radiofrequency ablation for colorectal liver metastases. World J Gastroenterol. 2016;22(16):4211–8.
Neofytou K, Smyth EC, Giakoustidis A, Khan AZ, Williams R, Cunningham D, et al. The preoperative lymphocyte-to-monocyte ratio is prognostic of clinical outcomes for patients with liver-only colorectal metastases in the neoadjuvant setting. Ann Surg Oncol. 2015;22(13):4353–62.
Funding
None.
Author information
Authors and Affiliations
Contributions
SW and ZL: research design; SW, LS: literature review; SW and JT: data extraction, quality evaluation and statistical analysis; SW and LS: manuscript preparation; WS and ZL: revision; All authors contributed to the article and approved the submitted version. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
The results of all subgroup analyses.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, Sh., Song, L., Tang, Jy. et al. Safety and long-term prognosis of simultaneous versus staged resection in synchronous colorectal cancer with liver metastasis: a systematic review and meta-analysis. Eur J Med Res 27, 297 (2022). https://doi.org/10.1186/s40001-022-00937-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-022-00937-z