
Abstract
Background
Connecting end-users to research evidence has the power to improve patient knowledge and inform health decision-making. Differences in the culture and language of the end users may shape the effectiveness of knowledge mobilization (KMb). This scoping review set out to understand current approaches and methods when creating or adapting KMb products for culturally and linguistically diverse (CALD) audiences.
Methods
We searched 3 databases (Ovid Medline, CINAHL via EBSCOhost, PsychINFO) from 2011 until August 2023. We included any literature about KMb product creation or adaptation processes serving CALD communities. A primary reviewer screened all identified publications and a second reviewer screened publications excluded by the primary. Data were extracted using a standardized form by one reviewer and verified by a second reviewer. Studies were categorized by type of adaptations (‘surface’ and/or ‘deep’ structure) and mapped based on type of stakeholder engagement used in the research approach (i2S model), and end-user involvement (content, design, evaluation and dissemination) in KMb product creation or adaptation.
Results
Ten thousand two hundred ninety-nine unique titles and abstracts were reviewed, 670 full-text studies were retrieved and reviewed, and 78 studies were included in final data extraction and mapping. Twenty-four studies (31%) created or adapted exclusively text-based KMb products such as leaflets and pamphlets and 49 (63%) produced digital products such as videos (n = 16, 33%), mobile applications (n = 14, 29%), and eHealth websites (n = 7, 14%). Twenty-five studies (32%) reported following a framework or theory for their creation or adaptation efforts. Twenty-eight studies (36%) engaged stakeholders in the research approach. Nearly all (96%) involved end-users in creating or adapting the KMb products through involvement in content development (n = 64), design features (n = 52), evaluation (n = 44) and dissemination (n = 20). Thirty-two (41%) studies included reflections from the research teams on the processes for creating or adapting KMb products for CALD communities.
Conclusion
Included studies cited a variety of methods to create or adapt KMb products for CALD communities. Successful uptake of created or adapted KMb products was often the result of collaboration and involvement with end-users for more applicable, accessible and meaningful products. Further research developing guidance and best practices is needed to support the creation or adaptation of KMb products with CALD communities.
Registration
Protocol submitted to Open Science Framework on August 16, 2022 (https://osf.io/9jcw4/).
Similar content being viewed by others

Text box 1. Contributions to the literature |
|---|
• Adaptations found as a part of this scoping review show a wide range of processes used and reveal gaps in what current approaches suggest to be effective. |
• Although many of the studies we reviewed claimed to culturally adapt health-related information, they were excluded since they only performed linguistic level translations. |
• Theoretical frameworks or evidence-based best practices need to be developed to guide cultural adaptation of health-related information for all levels of consumers (e.g., parents, adolescents, etc.). |
Background
Knowledge mobilization (KMb) (an umbrella term encapsulating knowledge translation, knowledge transfer, and knowledge exchange) [1] involves synthesis, dissemination, transfer and exchange to ensure evidence is accessible, understandable and useful to knowledge users [2, 3]. KMb encompasses a variety of activities, including dissemination of research evidence to increase knowledge users’ access to research, as well as efforts to build and maintain relationships with knowledge users to support the uptake of information [4, 5]. Knowledge creation, in the form of KMb products, is one activity that supports the uptake and use of evidence to inform decision making [6].
Within healthcare, KMb products (which present evidence in clear, concise and user-friendly formats) can help patients and families by informing their health-related behaviours and healthcare decisions to improve health outcomes and reduce health system costs [7]. Successful uptake of evidence is contingent on relevance of the KMb products for the target end-user [2]. However, recognized barriers or determinants of effective KMb are differences in culture and language among the end-users of the evidence [8].
While KMb efforts have advanced substantially in the field of health promotion over the last decade, predominant cultures often comprise the accessible pool of engaged end-users [9, 10]. Subsequently, KMb products frequently entail English communication, and mainstream images not conveying relevance to minority cultures. Similarly, most health related KMb products assume end-users possess a certain level of health literacy and are relatively familiar with their healthcare system, which may not represent the experiences of many newcomer cultural groups. Public health agencies (e.g. Health Canada) sometimes provide linguistic translations of healthcare information for common languages; however, exclusive linguistic translation does not guarantee accessibility and relevance of healthcare information for the target communities. Instead, nuanced visuals, relevant terms, and overall cultural sensitivity have proved more desirable for end-users [11].
Resnicow and colleagues [12] have proposed that cultural adaptation consists of two dimensions: surface structure and deep structure. Aspects of culture that are easily observable to external onlookers like language, clothing, and ethnicity would fall under surface structure, while historical and psychological influences on health decisions would fall under deep structure. Though admittedly gray in nature, the delineation of surface and deep aspects provides potential broad categories of cultural adaptation. In terms of the application of cultural sensitivity, efforts to create or adapt KMb products could include surface structures of language and appearance of end-users, as well as deep structures of historical barriers and psychological stressors for end-users [13]. Resnicow and colleagues suggest that both surface and deep structures of cultural knowledge are essential for well-rounded cultural adaptations and encourage the involvement of end-users to understand the nuanced aspects.
Types and extent of stakeholder engagement can also vary in KMb product creation and adaptation [9, 14, 15]. Bammer [16] proposed a modified version of the International Association for Public Participation (IAP2) stakeholder engagement model, where researchers are positioned as support for the directions chosen by stakeholders and end-users (e.g. those who use the resources), rather than decision-makers and researchers themselves. The positioning of end-users as experts in their own information needs and preferences mirrors other public participation approaches often employed by heath researchers (e.g. Participatory Action Research (PAR) [17], Community-Based Participatory Research (CBPR) [18], etc.). Both cultural adaptation and stakeholder and end-user engagement appear to be core pillars in KMb product creation.
While there are several processes (e.g. translation and cultural brokerage, ecological validity model) of cultural adaptation that have been previously applied to adapt health intervention programs [19], and patient reported outcome scales [20], no guidance currently exists on how best to create or adapt KMb products that reach diverse end-user needs. As an initial step towards understanding best practices for effective KMb product creation or adaptation, within healthcare, this scoping review (ScR) aimed to map what approaches researchers have used to create or adapt culturally relevant health related KMb products. The following questions guided this ScR:
-
1.
What approaches and methods have researchers used when creating or adapting health related KMb products for culturally and linguistically diverse (CALD) end-users?
-
2.
What are the key considerations when creating or adapting KMb products for CALD end-users?
Understanding what methods have previously been used, resources required, as well as key considerations for how best to create or adapt KMb products will support health researchers and healthcare organizations in creating or adapting effective resources for CALD communities.
Methods
Review methods
This ScR followed the methodological framework proposed by Arksey and O’Malley [21], enhanced by Levac et al. [22] Specifically, we followed these five steps: (1) identifying the research question(s); (2) identifying the relevant studies; (3) study selection; (4) charting the data; (5) and reporting the results. Reporting of the review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) – 2018 Extension for Scoping Review. (Additional file 1) [23] A protocol was developed a priori and registered in Open Science Framework on August 16, 2022, and any protocol deviations have been reported there.
Search strategy
In collaboration with a research librarian and content experts, we developed and refined a comprehensive search strategy. The strategy combined subject headings and keywords for terms related to KMb, knowledge exchange, knowledge mobilization, cross-culture, culturally appropriate, CALD communities, and adaptation of health information and implementation science. On August 12, 2021 we searched Ovid Medline (1946-), CINAHL via EBSCOhost (1937-), PsycINFO (2002-), as well as ProQuest Dissertations & Theses Global to identify grey literature. Search results were exported to EndNote V.X7 (Clarivate Analytics) and duplicates removed before the file was provided to reviewers for screening in Microsoft Excel. The search was limited to English language, peer-reviewed studies published in academic journals from 2011 to August 2021 (given KMb was introduced and reported within health research literature around 2011). A search update was run in July 2023.
Study selection
All published study design types and secondary evidence syntheses were included if they contained a patient, public or consumer population and created or adapted a KMb product for CALD end-users. We defined a KMb product as any health research-based product that supported decision-making to provide explicit recommendations, and/or meet knowledge needs. We excluded any studies that only performed purely linguistic translations of a KMb product or the validation of translated measurement tools/questionnaires. Health interventions without standalone KMb products for end-user decision-making were also excluded. One reviewer screened titles and abstracts of each study as “include/unsure” or “exclude” based on a priori inclusion criteria (Additional file 2). A second independent reviewer verified all studies excluded by the first reviewer. Both reviewers performed a pilot screen where they independently screened 10% of the studies to assess consistency. Two independent reviewers reviewed the full-text of each included study from the primary screening. When agreement on a citation or full-text could not be reached between two reviewers, a third senior reviewer was consulted for resolution.
Data extraction
The following details were extracted from each study: publication characteristics, study design, population, KMb product description, methods of creation or adaptation, stakeholder (defined within as “individuals, organizations or communities that have a direct interest in the process and outcomes of a project, research or policy endeavor”) [24] engagement processes, KMb product evaluation processes, and reflections from researchers. Data were collected using a standardized form by one reviewer and verified by a second reviewer. Any discrepancies were resolved through a third-party decision.
Data analysis
We performed a narrative synthesis, guided by a qualitative content analysis approach [25] to summarize the quantity, content, and coverage of the evidence including summary statistics on studies examining the different ways of creating or adapting culturally relevant KMb products. Processes for creation or adaptation were mapped into five categories (Product creation, Literature search, Stakeholder engagement, Resources utilized, Evaluation) representing different methods reported throughout the literature.
Cultural adaptations were categorized into two broad groups, surface and deep structure [12, 26]. Surface structure involved coordinating materials and messages to observable characteristics of the target end-user (i.e., imagery, sounds, backgrounds, clothing, etc.). Deep structure involved contextualizing the social, historical, environmental, and psychological features of the proposed end-user group.
Bammer’s iS2 version [16] of the IAP2 Spectrum of Public Participation was used to classify levels of stakeholder (including end-user) engagement in the research approach/design across each study [27, 28]. The i2S is a spectrum of engagement across five stages: 1) Inform (e.g. informing stakeholders of health information and research processes), 2) Consult (e.g. researchers obtain feedback on research [i.e. recruitment processes, community engagement, tool topic], 3) Involve (e.g. researchers work directly with stakeholders to ensure their concerns or needs are considered in the research), 4) Collaborate (e.g. researchers develop equal partnerships for undertaking the research [i.e. co-designing a research study]), 5) Support (e.g. researchers support stakeholder in designing and implementing desirable research and dissemination methods) [16]. In moving from ‘inform’ to ‘support’ stakeholders have increasing influence on the research. We acknowledge that the term stakeholder may inadvertently feed into a colonialist mentality by perpetuating colonization and re-traumatization. A published model was used to define stakeholder engagement at various levels for this project and thus this term is used throughout the manuscript.
Additionally, end-user engagement in the creation or adaptation of the KMb product was mapped, based on their input into processes related to content, design, evaluation and dissemination.
Results
Search results
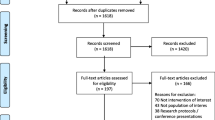
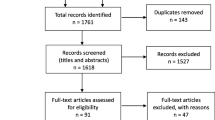
The search strategy (Additional file 3) captured 10, 299 studies after removing duplicates. Of these, the full-text of 670 were reviewed and 78 met eligibility criteria and were included in the review. The PRISMA flow diagram (Fig. 1) provides a detailed outline of the screening and selection process.

PRISMA Flow Diagram
Study characteristics
Table 1 provides a summary of the included studies’ characteristics with detailed characteristics in Additional file 4. The majority of studies were from USA (50%, n = 39) and Canada (10%, n = 7), with three (4%) studies each from Australia and United Kingdom and two (3%) studies each from Netherlands, Portugal and Tanzania. Most of the studies used qualitative methods (78%, n = 61) followed by mixed methods (14%, n = 11) and quantitative methods (8%, n = 6). Forty-nine (63%) reported the age of participants, most (n = 45, 92%) focused on adult populations and four (8%) on adolescents.
End-user groups varied across the included studies, with Latinx Spanish speakers (21%, n = 16) as the most frequently reported cultural communities served. Seventeen (22%) studies undertook cultural adaptations into more than one language. Health topics of the KMb products included: cancer (15%, n = 12), mental health conditions (6%, n = 5), COVID topics (6%, n = 5), diabetes (5%, n = 4), organ donation (5%, n = 4), and dementia (5%, n = 4).
Forty-nine (63%) created digital KMb products, twenty-four (31%) created non-digital products and five (6%) created both a digital and non-digital version of the same KMb product. Digital KMb products (63%, n = 49) included Internet-based tools such as videos/animations/infographics (45%, n = 22), eHealth websites (14%, n = 7), mobile-based tools such as health applications (29%, n = 14), tailored text messaging campaigns (14%, n = 7), and patient decision aids (6%, n = 3). Non-digital formats included booklets/leaflets/pamphlets (79%, n = 19) and patient decision aids (21%, n = 5).
Creation or adaptation processes
Creation or adaptation processes are mapped out in Table 2, and further details for each of the processes are outlined in Additional file 5. Each included study followed a unique process for creating or adapting a KMb product for CALD communities. Fifty-four (69%) reported the processes of creating a new KMb product, while twenty-four studies (31%) outlined their process for adapting a pre-existing KMb product for a specific end-user group. Thirty-eight studies (49%) reported a preparatory information gathering process, where literature reviews (68%, n = 26), systematic/scoping reviews (16%, n = 6), and conversations with community agencies or experts (8%, n = 3), provided background to direct creation of the KMb product.
Stakeholder engagement in research
Twenty eight studies (36%) engaged stakeholders at varying levels in the approach to the research project, or stakeholders gave input on the research methods and study design. Most commonly, stakeholders were engaged at the level of Involve (n = 17, 61%), followed by Consult (n = 14, 50%), Collaborate (n = 10, 36%), and Inform (n = 2, 7%). Three studies (11%) engaged stakeholders at the highest level of engagement, Support. All three studies worked in partnership with American Indian or Indigenous communities, in which community-based research methods were used.
End-user engagement in KMb product creation or adaptation
Seventy-five studies (96%) involved end-users specifically in the creation or adaptation of the KMb product. End-users were involved in providing input on content (n = 64, 85%) and design (n = 52, 69%) features. Input was gathered through a mix of focus group sessions (n = 24), one-on-one interviews (n = 31), surveys (n = 7), workshops (n = 7) and via community advisory groups (n = 36). Over half the studies (n = 44, 59%) reported involving end-users in the evaluation of the KMb product. This included seeking feedback from end-users via surveys (n = 14, 32%), focus groups (n = 5, 11%) as well as formal evaluation studies (n = 9, 20%). Of these, 40 (91%) studies reported the results of their evaluation. Assessments included usability testing, acceptability, cultural appropriateness, esthetics, and knowledge gained through use of the KMb product. However, none of the studies included a structured assessment of end-user engagement and involvement when adapting or creating the KMb product. Twenty studies (27%) reported that end-users were involved in the dissemination of the created or adapted KMb resource. Thirteen studies (65%) reported end-users provided suggestions on where and how to disseminate, and in 11 studies (55%) end-users helped with dissemination of the KMb resource.
Resources utilized
Most studies (n = 74, 95%) reported the various human resources they utilized during their creation or adaptation process. The involvement of healthcare providers was the most prevalent (n = 35, 47%), followed by translation support (n = 27, 36%), research or content experts (n = 25, 34%) and creative or visual designers (n = 22, 30%). Two studies used specialists to moderate their process, one study [32] had a participatory design expert to assist with guiding exercises and another study [57] used an experienced moderator to lead their discussion sessions.
Approach and type of cultural adaptation
Details regarding the type of cultural adaptations used and involvement of end-users is presented in Table 3. Six studies (8%) cited using a CBPR [18] approach, and twenty-five studies (32%) reported using a framework, theory or model to guide their creation or adaptation efforts. All studies utilized surface structure cultural adaptations and most (85%, n = 66) included deep structure adaptations in their creation or adaptation processes. To achieve deep structure contextualization authors most commonly consulted specific end-user populations (e.g. clinical populations [14%, n = 9], community members [30%, n = 20]) through focus groups (11%, n = 7), and assessed various cultural contexts (18%, n = 12).
Researcher reflections
Thirty-two (41%) studies included reflections from the research team on the processes for creating or adapting KMb products (See Additional File 6). Notably, researchers emphasized the importance of forming stakeholder relationships before and involving end-users throughout the research process [32], that communication between multiple stakeholder groups can be time-consuming [58], that initial positive reception to adapted products does not guarantee adherence to behavior change [88], but that the process of adapting KMb products can be rewarding for researchers (e.g. meeting end-users needs) [78].
Discussion
This ScR provides an outline of documented processes used to create or adapt KMb products for CALD communities, highlights gaps in that literature, and provides direction for future research. As a means of addressing the needs of populations often underserved by health systems, researchers and organizations have begun specifically creating or adapting their KMb products for CALD communities. To the best of our knowledge, this is the first review to synthesize and examine literature on processes and considerations for creating or adapting KMb products. There appears to be a range of methods employed to address KMb creation for CALD groups. These methods range from original co-created KMb products with participatory frameworks (e.g. Wild et al., [10]; Telenta et al., [14]) to cultural adaptations of pre-existing KMb products [81].
Through this ScR, we identified 78 studies that reported a variety of methods for creating or adapting KMb products for CALD communities. Across the various cultural communities, modes of information delivery, and approaches/processes cited, many studies demonstrated deep structure cultural adaptation [12]. While the majority involved end-users in the creation or adaptation of the KMb resource, only 28 studies engaged stakeholders in the research approach (as per i2S model) [16].
Along with study characteristics and creation processes, we extracted information about the depth of creation or adaptation based on Resnicow’s [12] explanation of surface and deep structures of cultural sensitivity. It has been reported that gaining deep structure cultural knowledge can be a time-consuming process, largely inaccessible to outsiders to the cultural community [151]. Although it was not possible to extract information about the cultural background of included studies team members, it is likely that researchers may not identify with the end-user population of study. Researchers who are outsiders to the end-user community lack the necessary information for deep structure cultural sensitivity on their own. However, engaging with community members directly can provide insider perspectives for culturally sensitive practices.
Each phase of the i2S framework represents increasing involvement of stakeholders in research processes [16]; with the ultimate stage of Support representing research decisions led by end-users. The few studies that utilized this level of the i2S framework in this review potentially indicate the challenges and commitment required for this process. Studies that exemplified the Support phase of the i2S utilized end-user committees that were involved from early conversations about research priorities to eventual dissemination of findings. However, while it is important to note that stakeholder engagement may vary depending on project aims and resources, ongoing stakeholder engagement at the Involve, Collaborate, or Support level is essential to gain insights for deep structure cultural aspects and relevant KMb [26]. The majority of studies included in this review engaged in some form of deep structure cultural adaptation, likely due in part to some form of end-user engagement and involvement [16] reported in included studies.
This emphasis on inductive knowledge obtainment and delivery mirrors processes outlined in CBPR [152] and PAR [17] approaches. In both CBPR and PAR, the end-user from the community of study is positioned as a collaborator: someone who has autonomy in the research process as well as insider information for the community of study [17, 18, 152]. CBPR has been used as a guiding approach in health intervention literature, and may provide similar guidance for KMb product creation and adaptation [153]. Additionally, frameworks used for adapting health interventions, such as the Ecological Validity Model [20], may also offer a systematic approach to cultural adaptations of KMb products. Regardless of the framework used, researchers who choose to create or adapt KMb products for CALD communities may be well-supported by seeking deep structure cultural understandings through supportive, inductive stakeholder engagement and through involving end-users in the development of KMb resources.
A gap in the literature was around researchers’ reflections of the processes used, as well as the specific methods of KMb product evaluation. Many involved a wide range of people and skill sets, which is also potentially time consuming and costly. While many studies reported they evaluated the created or adapted KMb product for usability, few mentioned the specific tools used to assess uptake and impact. It is unknown whether some of the initial positive receptions to the adapted products reported resulted in increased knowledge or influenced behavior change or decision-making (pending the purpose of the tool). Evaluation tools should assess not only the cultural appropriateness of the developed or adapted KMb product, but also the effectiveness of the products in terms of achieving their intended purpose (e.g. increased health literacy, influenced decision making). Further, no studies reported evaluating the engagement process with their end-users. Additionally, many did not report on the practicality or feasibility of the processes used (time, resources, engagement), nor whether the product met end-users’ needs and expectations. Those that did, reflected that incorporation and balancing of opinions and feedback from different stakeholders (researchers, clinicians, end-users, community members) was difficult and time-consuming. Further, fostering collaborations between researchers and community members was resource intensive, yet many reported that establishing these partnerships was key to ensure materials were comprehensive, accessible, and appropriate for the end-users.
Future research should aim to understand the practicalities and nuances of engaging end-users and evaluating the processes to support others in this field. Furthermore, greater transparency by researchers in their adaptation processes would aid in solidifying best practice considerations for culturally adapting KMb products. Ultimately, the most successful methods used by researchers to create or adapt KMb products for CALD communities could be collated and used to form a framework for future work. Additionally, drawing on culturally targeted or tailored approaches proposed by Kreuter et al., [121] could help identify factors such as familial roles, communication patterns, belief systems, social structures and other behavioral and social characteristics within the end-user community that should be considered during tool development or adaption. A framework that integrates peripheral, evidential, linguistic, and social cultural dimensions, could then be evaluated with end-users from various cultural communities to assess its usefulness in this field [121]. However, given how nuanced and tailored KMb should be in meeting the needs of the end-user, perhaps careful planning considering meaningful engagement and being intentional about the best methods to use is key.
Limitations
This review only included publications in English, yet other cultural creation or adaptation methods studies may be present in languages other than English. The process of defining a KMb product was iterative and largely guided by consensus discussion. The overlap between KMb products and intervention materials was difficult to navigate, particularly when studies did not thoroughly describe their intervention materials.
Consultation
By examining the methods others have used for their creation and adaptation work, a better understanding around the key considerations when creating or adapting KMb products for culturally and linguistically diverse communities can be achieved.
A methods working group stemming from this work has been developed to drive the creation of key considerations for how to linguistically and culturally create or adapt KMb products. The methods working group is made up of researchers, cultural knowledge brokers and community members who have firsthand experience and knowledge around how to engage with diverse communities as well as co-design KMb products. By critically evaluating current adaptation practices, we intend to establish a core set of methods and considerations for creating or adapting healthcare decision-making tools for CALD communities. A driving questions behind those discussions will be: is it possible to create a KMb product that meets the needs of multiple diverse communities, or does that go against the foundational tenets of KMb (contextualization, target end-user)?
Conclusion
This review provides information on the various processes, resources needed and levels of stakeholder engagement and end-user involvement used to create or adapt KMb products for CALD communities. While methods and processes, as well as theory or frameworks underpinning the work, varied across projects, it is clear that an important amount of time and resources is required. Significant gaps in the literature still remain surrounding how best to create or adapt culturally relevant KMb products and how to evaluate their impact, what level of engagement is needed, as well as understanding the practicalities of culturally adapting KMb products. Until an appropriate framework exists that integrates both cultural and linguistic dimensions, researchers would be well-supported by emphasizing cultural sensitivity and meaningful end-user engagement in their approaches.
The findings of this review and examples of cultural adaptation could be used to support the creation of best practice guidelines for researchers working in this field. Understanding and developing considerations for best practices will assist researchers and organizations in effectively reaching a wider population with health promotion and KMb initiatives.
Availability of data and materials
No datasets were generated or analysed during the current study.
Abbreviations
- CALD:
-
Culturally and linguistically diverse
- CBPR:
-
Community-based participatory research
- IAP2:
-
International Association for Public Participation
- KMb:
-
Knowledge mobilization
- PAR:
-
Participatory Action Research
- ScR:
-
Scoping review
References
Ward V. Why, Whose, What and How? A framework for knowledge mobilisers. Evidence & Policy: J Res, Debate Pract. 2017;13:477–97.
Straus SE, Tetroe J, Graham I. Defining knowledge translation. CMAJ. 2009;181(3–4):165–8.
Turin TC, Chowdhury N, Vaska M, et al. Knowledge mobilisation in bridging community-practice–academia-policy through meaningful engagement: systematic integrative review protocol focusing on studies conducted on health and wellness among immigrant communities. BMJ Open. 2020;10:e036081. https://doi.org/10.1136/bmjopen-2019-03608.1.
Davies HTO, Powell AE, Nutley SM. Mobilising knowledge to improve UK health care: learning from other countries and other sectors – a multi-method mapping study. Health Services and Delivery Research. 2015;3(27). National Institute for Health Research Service Delivery and Organisation. https://doi.org/10.3310/hsdr03270.
Grimshaw JM, Eccles MP, Lavis JN, et al. Knowledge translation of research findings. Implementation Sci. 2012;7:50. https://doi.org/10.1186/1748-5908-7-50.
Straus SE, Tetroe JM, Graham ID. Knowledge translation is the use of knowledge in health care decision making. J Clin Epidemiol. 2011;64(1):6–10. https://doi.org/10.1016/j.jclinepi.2009.08.016.
Albrecht L, Scott SD, Hartling L. Knowledge translation tools for parents on child health topics: a scoping review. BMC Health Serv Res. 2017;17(1):1–12.
Harrison R, Walton M, Chitkara U, Manias E, Chauhan A, Latanik M, et al. Beyond translation: engaging with culturally and linguistically diverse consumers. Health Expect. 2020;23(1):159–68.
O’Brien J, Fossey E, Palmer VJ. A scoping review of the use of co-design methods with culturally and linguistically diverse communities to improve or adapt mental health services. Health Soc Care Community. 2021;29(1):1–17.
Wild A, Kunstler B, Goodwin D, Onyala S, Zhang L, Kufi M, et al. Communicating COVID-19 health information to culturally and linguistically diverse communities: insights from a participatory research collaboration. Public Health Res Pract. 2021;31(1):e3112105.
Elliott SA, Wright KS, Scott SD, Hartling L. Perspectives from French and Filipino parents on the adaptation of child health knowledge translation tools: qualitative exploration. JMIR Form Res. 2022;6(3):e33156.
Resnicow K, Baranowski T, Ahluwalia JS, Braithwaite RL. Cultural sensitivity in public health: defined and demystified. Ethn Dis. 1999;9(1):10–21.
Durlak JA, DuPre EP. Implementation matters: a review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am J Community Psychol. 2008;41(3):327–50.
Telenta J, Jones SC, Francis KL, Polonsky MJ, Beard J, Renzaho AMN. Australian lessons for developing and testing a culturally inclusive health promotion campaign. Health Promot Int. 2020;35(2):217–31.
Thomson MS, Chaze F, George U, Guruge S. Improving immigrant populations’ access to mental health services in Canada: a review of barriers and recommendations. J Immigr Minor Health. 2015;17(6):1895–905.
Bammer G. Stakeholder engagement primer: 4. Options for engagement Integration and Implementation Insights. 2021. Available from: https://i2insights.org/2021/11/04/options-for-engagement/.
Baum F, MacDougall C, Smith D. Participatory action research. J Epidemiol Community Health. 2006;60(10):854.
Wallerstein NB, Duran B. Using community-based participatory research to address health disparities. Health Promot Pract. 2006;7(3):312–23.
Gonzàlez Castro F, Garfinkle J. Critical issues in the development of culturally relevant substance abuse treatments for specific minority groups. Alcohol Clin Exp Res. 2003;27(8):1381–8.
Bernal G, Bonilla J, Bellido C. Ecological validity and cultural sensitivity for outcome research: issues for the cultural adaptation and development of psychosocial treatments with Hispanics. J Abnorm Child Psychol. 1995;23(1):67–82.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73.
Deverka PA, Lavallee DC, Desai PJ, Esmail LC, Ramsey SD, Veenstra DL, et al. Stakeholder participation in comparative effectiveness research: defining a framework for effective engagement. J Comp Eff Res. 2012;1(2):181–94.
Erlingsson C, Brysiewicz P. A hands-on guide to doing content analysis. Afr J Emerg Med. 2017;7(3):93–9.
Wilson BD, Miller RL. Examining strategies for culturally grounded HIV prevention: a review. AIDS Educ Prev. 2003;15(2):184–202.
International Association for Public Participation. Public participation spectrum 2004 [updated Retrieved October 2021 from. Available from: https://iap2canada.ca/Resources/Documents/0702-Foundations-Spectrum-MW-rev2%20(1).pdf.]
McNeill M, Noyek S, Engeda E, Fayed N. Assessing the engagement of children and families in selecting patient-reported outcomes (PROs) and developing their measures: a systematic review. Qual Life Res. 2021;30(4):983–95.
Abascal Miguel L, Lopez E, Sanders K, Skinner NA, Johnston J, Vosburg KB . . . Diamond-Smith N. Evaluating the impact of a linguistically and culturally tailored social media ad campaign on COVID-19 vaccine uptake among indigenous populations in Guatemala: a pre/post design intervention study. BMJ Open. 2022;12(12):e066365. https://doi.org/10.1136/bmjopen-2022-066365.
Abbass-Dick J, Brolly M, Huizinga J, Newport A, Xie F, George S, et al. Designing an eHealth Breastfeeding Resource With Indigenous Families Using a Participatory Design. J Transcult Nurs. 2018;29(5):480–8.
Alexandrou C, Müssener U, Thomas K, Henriksson H, Löf M. Adapting a Parental Support App to Promote Healthy Diet and Physical Activity Behaviors (MINISTOP) for a Multi-Ethnic Setting: A Qualitative Study on the Needs and Preferences of Parents and Nurses within Swedish Child Health Care. Nutrients. 2021;13(7):2190. https://doi.org/10.3390/nu13072190.
Ali PA, Salway S, Such E, Dearden A, Willox M. Enhancing health literacy through co-design: development of culturally appropriate materials on genetic risk and customary consanguineous marriage. Prim Health Care Res Dev. 2019;20.
Arnold CM, Aragon D, Shephard J, Van Sell SL. The coming of the blessing: A successful cross-cultural collaborative effort for American Indian/Alaska Native families. Special Issue: Issues related to the health of American Indians and Alaska Natives. 2011;34(3):196–201.
Avila S, Franco I, Bregio C, Haydon A, Macayan JPM, Rooney MK . . . Ortega P. Spanish Adaptation and Evaluation of Clinical Discussion Guides: Communicating the External Beam Radiotherapy Experience (CEBRE) en Espanol. Int J Radiat Oncol Biol Phys. 2023;116(1):166–75. https://doi.org/10.1016/j.ijrobp.2023.01.031.
Baptista S, Heleno B, Pinto M, Guimaraes B, China D, Ramos JP . . . Martins C. Translation and cultural adaptation of a prostate cancer screening decision aid: a qualitative study in Portugal. BMJ Open. 2020;10(3):e034384. https://doi.org/10.1136/bmjopen-2019-034384.
Best AL. Speaking to the spirit: Examining the effectiveness of spiritually-framed breast cancer screening messages among African American women. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2013;74(6-B(E)). Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=psyc10&NEWS=N&AN=2013-99240-159.
Bilbrey AC, Humber MB, Plowey ED, Garcia I, Chennapragada L, Desai K . . . Gallagher-Thompson D. The Impact of Latino Values and Cultural Beliefs on Brain Donation: Results of a Pilot Study to Develop Culturally Appropriate Materials and Methods to Increase Rates of Brain Donation in this Under-Studied Patient Group. Clin Gerontol. 2018;41(3):237–48. https://doi.org/10.1080/07317115.2017.1373178.
Blazey M, Marinac C, Whiteley J, Peterson S, Burns White K, Jacques C . . . Wright J. Designing a Dyad-Based Digital Health Intervention to Reduce Sedentary Time in Black Breast Cancer Survivors and Their First-degree Relatives: Human-Centered Design Study. JMIR Form Res. 2023;7:e43592. https://doi.org/10.2196/43592.
Cabassa LJ, Molina GB, Baron M. Depression fotonovela: development of a depression literacy tool for Latinos with limited English proficiency. Health Promot Pract. 2012;13(6):747–54. https://doi.org/10.1177/1524839910367578.
Caplan S, Lovera AS, Comas EV, Attilus J. A mobile app to prevent depression among low-income primary care patients in the Dominican Republic: Sociocultural adaptations. J Transcult Nurs. 2020;31(4):413–24. https://doi.org/10.1177/1043659620912315.
Celentano I, Winer RL, Jang SH, et al. Development of a theory-based HPV vaccine promotion comic book for East African adolescents in the US. BMC Public Health. 2021;21(1):1137. Published 2021 Jun 14. https://doi.org/10.1186/s12889-021-11005-2.
Chang HC, Ho M-H, Traynor V, Tang L-Y, Liu MF, Chien H-W . . . Montayre J. Mandarin version of dementia and driving decision aid (DDDA): Development and stakeholder evaluation in Taiwan. Int J Older People Nurs. 2021;16(3):1–11. https://doi.org/10.1111/opn.12370.
Crouse JJ, LaMonica HM, Song YJC, Boulton KA, Rohleder C, DeMayo MM, et al. Designing an App for Parents and Caregivers to Promote Cognitive and Socioemotional Development and Well-being Among Children Aged 0 to 5 Years in Diverse Cultural Settings: Scientific Framework. JMIR Pediatr Parent. 2023;6:e38921.
Cunningham-Erves J, Brandt HM, Sanderson M, Clarkson K, Lee O, Schlundt D . . . Davis J. Development of a Theory-Based, Culturally Appropriate Message Library for Use in Interventions to Promote COVID-19 Vaccination Among African Americans: Formative Research. JMIR Form Res. 2022;6(7):e38781. https://doi.org/10.2196/38781.
Drago MJ, Guillén U, Schiaratura M, Batza J, Zygmunt A, Mowes A . . . Kirpalani H. Constructing a Culturally Informed Spanish Decision-Aid to Counsel Latino Parents Facing Imminent Extreme Premature Delivery. Matern Child Health J. 2018;22(7):950–7. https://doi.org/10.1007/s10995-018-2471-8.
Drenkard C, Fuentes-Silva Y, Parente Costa Seguro L, Torres dos Reis-Neto E, Ibanez S, Elera-Fitzcarrald C, et al. Let’s talk about Lupus. Overview of an innovative, high-reach, online program to fill the education gaps of Latin Americans living with Lupus. J Clin Rheumatol. 2022;28(2):e368–74.
Du Plessis LM, Job N, Coetzee A, Fischer S, Chikoko MP, Adam M, Love P. Development and Field-Testing of Proposed Food-Based Dietary Guideline Messages and Images amongst Consumers in Tanzania. Nutrients. 2022;14(13):2705-N.PAG. https://doi.org/10.3390/nu14132705.
Glennie M, Dowden M, Grose M, Scolyer M, Superina A, Gardner K. Engaging Remote Aboriginal Communities in COVID-19 Public Health Messaging via Crowdsourcing. Front Public Health. 2022;10:866134. https://doi.org/10.3389/fpubh.2022.866134.
Gordon EJ, Feinglass J, Carney P, Ramirez D, Olivero M, O’Connor K . . . Caicedo JC. An interactive, bilingual, culturally targeted website about living kidney donation and transplantation for hispanics: development and formative evaluation. JMIR Res Protoc. 2015;4(2):e42. https://doi.org/10.2196/resprot.3838.
Grasaas E, Fegran L, Helseth S, Stinson J, Martinez S, Lalloo C, Haraldstad K. iCanCope With Pain: Cultural Adaptation and Usability Testing of a Self-Management App for Adolescents With Persistent Pain in Norway. JMIR Res Protoc. 2019;8(6):e12940. https://doi.org/10.2196/12940.
Grinker RR, Kang-Yi CD, Ahmann C, Beidas RS, Lagman A, Mandell DS. Cultural Adaptation and Translation of Outreach Materials on Autism Spectrum Disorder. J Autism Dev Disord. 2015;45(8):2329–36. https://doi.org/10.1007/s10803-015-2397-6.
Guttman N, Gesser-Edelsburg A, Aycheh S. Communicating health rights to disadvantaged populations: challenges in developing a culture-centered approach for Ethiopian immigrants in Israel. Health Commun. 2013;28(6):546–56.
Hainsworth E, McGrowder E, McHugh J, Bancroft E, Mahabir S, Webber W . . . Cruickshank S. How can we recruit more men of African or African-Caribbean ancestry into our research? Co-creating a video to raise awareness of prostate cancer risk and the PROFILE study. Res Involv Engagem. 2022;8(1):14. https://doi.org/10.1186/s40900-022-00347-9.
Hall CE, Hall AB, Mallya J, Courtright P, Kok G. Developing comic strips promoting diabetic retinopathy screening in Kilimanjaro, Tanzania, using Intervention Mapping. Eye (London, England). 2022;36(Suppl 1):25–32. https://doi.org/10.1038/s41433-022-02003-8.
Hamdiui N, Bouman MPA, Stein ML, Crutzen R, Keskin D, Afrian A . . . Timen A. The development of a culturally sensitive educational video: How to facilitate informed decisions on cervical cancer screening among Turkish- and Moroccan-Dutch women. Health expectations : an international journal of Public Participation in Health Care and Health Policy. 2022;25(5):2377–85. https://doi.org/10.1111/hex.13545.
Harvey I, O’Brien M. Addressing health disparities through patient education: the development of culturally-tailored health education materials at Puentes de Salud. J Community Health Nurs. 2011;28(4):181–9. https://doi.org/10.1080/07370016.2011.614827.
Hashim MJ, Mustafa H, Al Abdouli AO, Abdulla Al RA, AlQahtani SM, Almajed SA, et al. Health education materials for Arab patients: content and design preferences. Med Princ Pract. 2013;22(4):411–4. https://doi.org/10.1159/000346276.
Hempler NF, Nicic S, Ewers B, Willaing I. Dietary education must fit into everyday life: a qualitative study of people with a Pakistani background and type 2 diabetes. Patient Prefer Adherence. 2015;9:347.
Hodge FS, Itty TL, Cadogan MP, Martinez F. “Weaving balance into life”: Development and cultural adaptation of a cancer symptom management toolkit for Southwest American Indians. J Cancer Surviv. 2012;6(2):182–8. https://doi.org/10.1007/s11764-011-0209-3.
Hong YA, Shen K, Lu HK, et al. A Social Media-Based Intervention for Chinese American Caregivers of Persons With Dementia: Protocol Development. JMIR Aging. 2022;5(3):e40171. Published 2022 Sep 29. https://doi.org/10.2196/40171.
Jameel A, Penny L, Arabena K. Closing the miscommunication gap: A user guide to developing picture-based communication tools for Aboriginal and Torres Strait Islander peoples in emergency departments. Emerg Med Australas: EMA. 2023. https://doi.org/10.1111/1742-6723.14274.
Jiang N, Nguyen N, Siman N, Cleland CM, Nguyen T, Doan HT . . . Shelley DR. Adaptation and Assessment of a Text Messaging Smoking Cessation Intervention in Vietnam: Pilot Randomized Controlled Trial. JMIR Mhealth Uhealth. 2021;9(10):e27478. https://doi.org/10.2196/27478.
Jiang N, Rogers ES, Cupertino P, Zhao X, Cartujano-Barrera F, Lyu JC . . . Sherman SE. Development of a WeChat-based Mobile Messaging Smoking Cessation Intervention for Chinese Immigrant Smokers: Qualitative Interview Study. JMIR Form Res. 2022;6(6):e36091. https://doi.org/10.2196/36091.
Kandasamy S, Ariyarajah A, Limbachia J, An D, Lopez L, Manoharan B . . . Anand SS. South Asian Youth as Vaccine Agents of Change (SAY-VAC): evaluation of a public health programme to mobilise and empower South Asian youth to foster COVID-19 vaccine-related evidence-based dialogue in the Greater Toronto and Hamilton Area, Canada. BMJ Open. 2022;12(9):e061619. https://doi.org/10.1136/bmjopen-2022-061619.
Kayler LK, Breckenridge B, Thomas C, Brinser-Day S, Sierra E, Cadzow RB, et al. Using Community-Based Participatory Research to Create Animated Videos to Attenuate Disparities in Access to Kidney Transplant Information. Progress in transplantation (Aliso Viejo, Calif). 2023;33(1):5–14.
Kerr J, Ayangeakaa S, Combs R, Harris L, Sears J, Northington T . . . Krigger K. Community-informed development of a campaign to increase HIV pre-exposure prophylaxis (PrEP) awareness among African-American young adults. J Racial Ethn Health Disparities. 2021;8(4):901–11. https://doi.org/10.1007/s40615-020-00848-x.
Ko LK, Reuland D, Jolles M, Clay R, Pignone M. Cultural and linguistic adaptation of a multimedia colorectal cancer screening decision aid for Spanish-speaking Latinos. J Health Commun. 2014;19(2):192–209. https://doi.org/10.1080/10810730.2013.811325.
Lee HY, Lee MH, Sharratt M, Lee S, Blaes A. Development of a Mobile Health Intervention to Promote Papanicolaou Tests and Human Papillomavirus Vaccination in an Underserved Immigrant Population: A Culturally Targeted and Individually Tailored Text Messaging Approach. JMIR Mhealth Uhealth. 2019;7(6):e13256. Published 2019 Jun 6. https://doi.org/10.2196/13256.
Leiter RE, Varas MTB, Miralda K, Muneton-Castano Y, Furtado G, Revette A . . . Enzinger AC. Adaptation of a Multimedia Chemotherapy Educational Intervention for Latinos: Letting Patient Narratives Speak for Themselves. Journal of Cancer Education : the official journal of the American Association for Cancer Education. 2023. https://doi.org/10.1007/s13187-023-02270-3.
LeLaurin JH, Sypniewski C, Wing K, Freytes IM, Findley K, Uphold CR. Development, Usability Testing, and Promotion of the English- and Spanish-language RESCUE Stroke Caregiver Websites. Am J Health Educ. 2022;53(3):174–85. https://doi.org/10.1080/19325037.2022.2048747.
Lemon D, Swan-Castine J, Connor E, van Dooren F, Pauli J, Boffa J . . . Pedruzzi RA. Vision, future, cycle and effect: A community life course approach to prevent prenatal alcohol exposure in central Australia. Health promotion journal of Australia : official journal of Australian Association of Health Promotion Professionals. 2022;33(3):788–96. https://doi.org/10.1002/hpja.547.
Li W-W, Leung C. Development and pilot test of a culturally sensitive CD-ROM for hypertensive, older Chinese immigrants. Computers, informatics, nursing : CIN. 2012;30(4):190–5. https://doi.org/10.1097/NCN.0b013e3182388921.
Liu X, Ghisi GLM, Meng S, et al. Establishing a process to translate and adapt health education materials for natives and immigrants: The case of Mandarin adaptations of cardiac rehabilitation education. Heart Lung. 2021;50(6):794–817. https://doi.org/10.1016/j.hrtlng.2021.06.002.
Maertens JA, Jimenez-Zambrano AM, Albright K, Dempsey AF. Using Community Engagement to Develop a Web-Based Intervention for Latinos about the HPV Vaccine. J Health Commun. 2017;22(4):285–93. https://doi.org/10.1080/10810730.2016.1275890.
Malamsha MP, Sauli E, Luhanga ET. Development and Validation of a Mobile Game for Culturally Sensitive Child Sexual Abuse Prevention Education in Tanzania: Mixed Methods Study. JMIR Serious Games. 2021;9(4):e30350. Published 2021 Nov 8. https://doi.org/10.2196/30350.
Martinez SN. Beyond basic bips: Efficacy of parent training using enhanced pamphlets. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2023;84(6-B). Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=psyc21&NEWS=N&AN=2023-38657-068.
Materia FT. Understanding factors that influence mobile health implementation using evidence-driven approaches. Dissertation Abstracts International: Section B: The Sciences and Engineering. 2022;83(3-B). Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=psyc21&NEWS=N&AN=2021-94600-291.
Mathieson F, Mihaere K, Collings S, Dowell A, Stanley J. Maori cultural adaptation of a brief mental health intervention in primary care. J Prim Health Care. 2012;4(3):231–8.
Mauka W, Mbotwa C, Moen K, Lichtwarck HO, Haaland I, Kazaura M . . . Mmbaga EJ. Development of a Mobile Health Application for HIV Prevention Among At-Risk Populations in Urban Settings in East Africa: A Participatory Design Approach. JMIR Form Res. 2021;5(10):e23204. https://doi.org/10.2196/23204.
McFarlane SJ, Morgan SE, Occa A, Peng W. An evaluation of clinical trial multimedia to support Hispanic cancer patients’ informational and decision-making needs. J Cancer Educ. 2021;36(1):110–7. https://doi.org/10.1007/s13187-019-01606-2.
Meherali S, Hartling L, Scott SD. Cultural Adaptation of Digital Knowledge Translation Tools for Acute Otitis Media in Low- to Middle-Income Countries: Mixed Methods Usability Study. JMIR Form Res. 2021;5(1):e13908.
Montague J, Haith-Cooper M. A study to assess the feasibility of using a novel digital animation to increase physical activity levels in asylum seeking communities. Health Soc Care Community. 2022;30(5):1960–8. https://doi.org/10.1111/hsc.13575.
Norris AE, Thalasinos RD, Hecht ML. Multicultural Adaptation of Mighty Girls for Widespread Dissemination: Pilot Study, App Development and Usability Testing, and Gauging Parent Support With Focus Groups. JMIR Form Res. 2021;5(6):e24937. https://doi.org/10.2196/24937.
Pathak LE, Aguilera A, Williams JJ, Lyles CR, Hernandez-Ramos R, Miramontes J . . . Figueroa CA. Developing messaging content for a physical activity smartphone app tailored to low-income patients: User-centered design and crowdsourcing approach. JMIR mHealth and uHealth. 2021;9(5). https://doi.org/10.2196/21177.
Payan DD, Maggard-Gibbons M, Florez KR, Mejia N, Hemmelgarn M, Kanouse D . . . Lara M. Taking care of yourself and your risk for breast cancer (CUIDARSE): A randomized controlled trial of a health communication intervention for Latinas. Health Educ Behav. 2020;47(4):569–80. https://doi.org/10.1177/1090198120920529.
Povey J, Sweet M, Nagel T, Lowell A, Shand F, Vigona J, Dingwall KM. Determining Priorities in the Aboriginal and Islander Mental Health Initiative for Youth App Second Phase Participatory Design Project: Qualitative Study and Narrative Literature Review. JMIR Form Res. 2022;6(2):e28342. https://doi.org/10.2196/28342.
Quintana R, Fernandez S, Guggia L, Fay M, Camacho C, Gomez G . . . Pons-Estel BA. Social networks as education strategies for indigenous patients with rheumatoid arthritis during COVID-19 pandemic. Are they useful? Clin Rheumatol. 2022;41(11):3313–8. https://doi.org/10.1007/s10067-022-06273-1.
Rami H, Hussien H, Rabie M, Sabry W, Missiry ME, Ghamry RE. Evaluating the effectiveness of a culturally adapted behavioral family psycho-educational program for Egyptian patients with schizophrenia. Transcult Psychiatry. 2018;55(5):601–22.
Santos LMd, de Oliveira Lima VL, Silva CSGe, Silva JDd, Passos SdSS, de Santana Carvalho ES. CONSTRUCTION AND VALIDATION OF THE CONTENT OF THE CHILDREN’S BOOKLET “IT’S TIME TO GET MY VEIN: WHAT DO I DO?” Revista Mineira de Enfermagem. 2021;25:1–12. https://doi.org/10.5935/1415-2762-20210018.
Sharpe PA, Brandt HM, McCree DH, Owl-Myers E, Taylor B, Mullins G. Development of culturally tailored educational brochures on HPV and pap tests for American Indian women. J Transcult Nurs. 2013;24(3):282–90.
Songtaweesin WN, LeGrand S, Bandara S, Piccone C, Wongharn P, Moonwong J . . . Tangmunkongvorakul A. Adaptation of a Theory-Based Social Networking and Gamified App-Based Intervention to Improve Pre-Exposure Prophylaxis Adherence Among Young Men Who Have Sex With Men in Bangkok, Thailand: Qualitative Study. J Med Internet Res. 2021;23(11):e23852. https://doi.org/10.2196/23852.
Stanley LR, Kelly KJ, Swaim RC, Jackman D. Cultural Adaptation of the Be under Your Own Influence Media Campaign for Middle-School American Indian Youth. J Health Commun. 2018;23(12):1017–25. https://doi.org/10.1080/10810730.2018.1536730.
Teles S, Napolskij MS, Paul C, Ferreira A, Seeher K. Training and support for caregivers of people with dementia: The process of culturally adapting the World Health Organization iSupport programme to Portugal. Dementia: The International Journal of Social Research and Practice. 2021;20(2):672–97. https://doi.org/10.1177/1471301220910333.
Tolentino M, Millerd S, Bali NZ, Ranido E, Takiguchi J, Balaz HooJ . . . Sentell T. Next Gen Hawai'i: Collaborative COVID-19 Social Media Initiative to Engage Native Hawaiian, Other Pacific Islander, and Filipino Youth. Hawaii J Health Soc Welf. 2022;81(7):201–8. Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med22&NEWS=N&AN=35821668
Umaefulam V, Fox T-L, Hazlewood G, Bansback N, Barber CEH, Barnabe C. Adaptation of a Shared Decision-Making Tool for Early Rheumatoid Arthritis Treatment Decisions with Indigenous Patients. The Patient. 2022;15(2):233–43. https://doi.org/10.1007/s40271-021-00546-8.
Valenzuela-Araujo D, Godage SK, Quintanilla K, Dominguez Cortez J, Polk S, DeCamp LR. Leaving Paper Behind: Improving Healthcare Navigation by Latino Immigrant Parents Through Video-Based Education. J Immigr Minor Health. 2021;23(2):329–36. https://doi.org/10.1007/s10903-020-00969-9.
van der Steen JT, Hertogh CMPM, de Graas T, Nakanishi M, Toscani F, Arcand M. Translation and cross-cultural adaptation of a family booklet on comfort care in dementia: sensitive topics revised before implementation. J Med Ethics. 2013;39(2):104–9. https://doi.org/10.1136/medethics-2012-100903.
Van Son CR. Developing Culturally Targeted Diabetes Educational Materials for Older Russian-Speaking Immigrants. Diabetes Educ. 2014;40(4):418-26. Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med11&NEWS=N&AN=24667951.
Versteegh LA, Chang AB, Chirgwin S, Tenorio FP, Wilson CA, McCallum GB. Multi-lingual “Asthma APP” improves health knowledge of asthma among Australian First Nations carers of children with asthma. Front Pediatr. 2022;10:925189. https://doi.org/10.3389/fped.2022.925189.
Wall SP, Castillo P, Shuchat-Shaw F, Norman E, Brown D, Martinez-Lopez N . . . Ravenell JE. Targeting versus tailoring educational videos for encouraging deceased organ donor registration in Black-owned barbershops. J Health Commun. 2022;27(1):37–48. https://doi.org/10.1080/10810730.2022.2035021.
Wright A, VanEvery R, Burnside H, Lopez KB, Kewageshig-Fyfe K, Jacobs B, et al. The Unexpected Benefits of a Decolonized Knowledge Translation Initiative for Indigenous Mother Participants. Qual Health Res. 2023;33(7):638–46.
Wu VS, Smith AB, Girgis A. Moving beyond translation: Development of WeCope, a self-management resource for Chinese-Australian immigrants affected by cancer. Eur J Cancer. 2022;31(1):1–16. https://doi.org/10.1111/ecc.13531.
Yeager KA, Bai J, Gogineni K, Meisel JL, Kweon J, Bruner DW, Waldrop-Valverde D. Pilot feasibility study of a video intervention to educate patients with breast cancer about clinical trials. J Cancer Educ. 2022;37(2):387–94. https://doi.org/10.1007/s13187-020-01826-x.
Zerafa N. Benefits of Co-Design with Consumers to Develop a No-Language Resource on Incontinence...Podium Presentations Joint 31st National Conference on Incontinence (NCOI) and the 4th Functional Urology Symposium (FUS) (NCOIFUS23) 14-17 June 2023. Adelaide Convention Centre, Adelaide SA. Australian & New Zealand Continence Journal. 2023;29(2):37.
Lefebvre RC. Social marketing and social change: Strategies and tools for improving health, well-being, and the environment. San Francisco, CA: John Wiley & Sons; 2013.
Morrison C, Dearden A. Beyond tokenistic participation: using representational artefacts to enable meaningful public participation in health service design. Health Policy. 2013;112(3):179–86.
European Centre for Disease Prevention and Control. Translation is not enough – Cultural adaptation of health communication materials. Stockholm: ECDC; 2016.
Entman RM. Framing: Towards clarification of a fractured paradigm. McQuail’s reader in mass communication theory. 1993;390:397.
Holt CL. Religiosity, spirituality, and the design of health communication message and interventions. Health communication message design: Theory and practice. 2012:153–64.
Bandura A, National Inst of Mental Health. Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, New Jersey: Prentice Hall; 1986.
Joseph RP, Keller C, Affuso O, Ainsworth BE. Designing Culturally Relevant Physical Activity Programs for African-American Women: A Framework for Intervention Development. J Racial Ethn Health Disparities. 2017;4(3):397–409.
Leventhal ADM, Leventhal EA. Illness cognition: Using common sense to understand adherence and affect cognition interactions. Cogn Ther Res. 1992;16:143–63.
Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211.
Singhal AR, E. Entertainment-Education: A Communication Strategy for Social Change. 1st ed. New Jersey: Lawrence Erlbaum Associates; 1999.
Hevner AR. A Three Cycle View of Design Science Research. Scand J Inf Syst. 2007;19(2):87–92.
Champion VLSC. The health belief model. In: Glanz K, Rimer BK, Lewis FM, editors. Health behavior and health education theory, research and practice. 3rd ed. San Francisco: Jossey-Bass; 2002. p. 45–66.
Montaño DEKD. Reasoned action, planned behavior, and the integrated behavioral model. In: Glanz K, Rimer BK, Lewis FM, editors. Health behavior and health education Theory, research and practice. 3rd ed. San Francisco: Jossey-Bass; 2002.
Collaboration IPDASI. IPDAS 2005: Criteria for judging the quality of patient decision aids: IPDAS; 2005. Available from: http://ipdas.ohri.ca/IPDAS_checklist.pdf.
Fishbein M, Ajzen I. Belief, attitude, intention and behavior: an introduction to theory and research. Contemp Sociol. 1977;6(2):244.
Rosenstock I. The Health Belief Model and Preventive Health Behavior. Health Educ Monographs. 1974;2(4):354–86.
Kreuter MW, Lukwago SN, Bucholtz RD, Clark EM, Sanders-Thompson V. Achieving cultural appropriateness in health promotion programs: targeted and tailored approaches. Health Educ Behav. 2003;30(2):133–46.
Kerrigan V, Lee AM, Ralph AP, Lawton PD. Stay Strong: aboriginal leaders deliver COVID-19 health messages. Health Promot J Austr. 2021;32(Suppl 1):203–4.
Finlay S, Wenitong M. Aboriginal community controlled health organisations are taking a leading role in COVID-19 health communication. Aust NZ J Public Health. 2020;44(4):251–2.
Gagne RBL, Wager W. Principles of instructional design. 4th ed. Orlando, FL: Harcourt Brace Jovanovich; 1992.
Wild D, Grove A, Martin M, Eremenco S, McElroy S, Verjee-Lorenz A, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value in health. 2005;8(2):94–104.
Weller SC. Cultural consensus theory: Applications and frequently asked questions. Field Methods. 2007;19(4):339–68.
Kelder SHHD, Perry CL. How individuals, environments, and health behaviors interact: social cognitive theory. In: Glanz KRB, Viswanath K, editors. Health behavior: theory, research, and practice. San Francisco: Jossey-Bass/Wiley; 2015.
Bartholomew Eldredge LK, MC, Ruiter RAC, Fernández ME, Kok G, & Parcel GS. Planning health promotion programs: an intervention mapping approach. 4th ed. San Francisco: Jossey-Bass; 2016.
Green L, Kreuter M. The precede–proceed model. In: Health promotion planning: an educational approach. 3rd ed. Mountain View (CA): Mayfield Publishing Company; 1999. p. 32–43.
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215.
Mayer REMR. Animation as an aid to multimedia learning. Educational Psychol Rev. 2002;14:87–99.
Dutta MJ. Communicating about culture and health: theorizing culture-centered and cultural snesitivity approaches. Commun Theory. 2007;17(3):304–28.
Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. 2021;374:n2061.
Viswanath K RS, Kontos E Mass media and population health: a macrosocial view. In: S G, editor. Macrosocial Determinants of Population Health. New York: Springer Publishing Co.; 2007. p. 275–94.
Aleem SCL, Ahmed F. Game development software engineering process life cycle: a systematic review. J Softw Eng Res Dev. 2016;4(1):1–30.
Plass JLHB, Kinzer CK. Foundations of game-based learning. Educational Psychologist. 2016;50(4):258–83.
Barrera M Jr, Castro FG, Strycker LA, Toobert DJ. Cultural adaptations of behavioral health interventions: a progress report. J Consult Clin Psychol. 2013;81(2):196.
King DK, Glasgow RE, Leeman-Castillo B. Reaiming RE-AIM: using the model to plan, implement, and evaluate the effects of environmental change approaches to enhancing population health. Am J Public Health. 2010;100(11):2076–84.
Mummah SA, Robinson TN, King AC, Gardner CD, Sutton S. IDEAS (Integrate, Design, Assess, and Share): a framework and toolkit of strategies for the development of more effective digital interventions to change health behavior. J Med Internet Res. 2016;18(12).
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4:50.
Schnall R, Rojas M, Bakken S, Brown W, Carballo-Dieguez A, Carry M, et al. A user-centered model for designing consumer mobile health (mHealth) applications (apps). J Biomed Inform. 2016;60:243–51.
Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42.
Rothman ABR, Wlaschin J, Salovey P. The strategic use of gain- and loss-framed messages to promote healthy behavior: how theory can inform practice. J Communication. 2006;56(1):202–20.
DiMatteo MRH-ZK, Martin LR. Improving patient adherence: a three-factor model to guide practice. Health Psychol Rev. 2012;6(1):74–91.
McGuire WJ. McGuire’s Classic Input-Output Framework for Constructing Persuasive Messages. In: Rice RE, Atkin CK, Eds., Public Communication Campaigns, 4th Edition. Thousand Oaks: SAGE Publications; 2013. p. 133–146. https://doi.org/10.4135/9781544308449.n9.
Israel BA, Coombe CM, Cheezum RR, Schulz AJ, McGranaghan RJ, Lichtenstein R, et al. Community-based participatory research: a capacity-building approach for policy advocacy aimed at eliminating health disparities. Am J Public Health. 2010;100(11):2094–102.
Bernal G, Jiménez-Chafey MI, Domenech Rodríguez MM. Cultural adaptation of treatments: A resource for considering culture in evidence-based practice. Prof Psychol Res Pract. 2009;40(4):361.
Jull J, Giles A, Boyer Y, Stacey D. Cultural adaptation of a shared decision making tool with Aboriginal women: a qualitative study. BMC Med Inform Decis Mak. 2015;15:1.
Singhal A, Cody, M. J., Rogers, E. M., & Sabido, M,. Entertainment-education and social change: History, research, and practice. . New Jersey Lawrence Erlbaum Associates.; 2004.
Jackson R, Masching R. Knowledge Translation in Indigenous Communities: A Review of the Literature. Canadi J Aborig Community Based HIV/AIDS Res. 2016;8:81–104.
Collins PH. Learning from the outsider within: The sociological significance of Black feminist thought. Soc Probl. 1986;33(6):s14–32.
Wallerstein N, Duran B. Community-based participatory research contributions to intervention research: the intersection of science and practice to improve health equity. Am J Public Health. 2010;100(S1):S40–6.
Salimi Y, Shahandeh K, Malekafzali H, Loori N, Kheiltash A, Jamshidi E, et al. Is community-based participatory research (CBPR) useful? A systematic review on papers in a decade. Int J Prev Med. 2012;3(6):386.
Acknowledgements
We would like to thank Erica Wright for expertise in developing the ScR search strategy. We would also like to thank Samantha Cyrkot, Kelsey Wright, Sharon Parappally-Joseph, and Alex Melton for their assistance with protocol development, screening and data extraction.
Funding
This work has been supported by funding from the Stollery Children’s Hospital Foundation through the Stollery Science Lab. Dr. Hartling and Dr. Scott are Distinguished Researchers with the Stollery Science Lab supported by the Stollery Children’s Hospital Foundation. Dr. Hartling is supported by a Canada Research Chair in Knowledge Synthesis and Translation. Dr. Scott is supported by a Canada Research Chair in Knowledge Translation in Child Health.
Author information
Authors and Affiliations
Contributions
SAE and LH developed the research question. SAE, LH, and SDS designed the study. LB coded the data, supervised by SAE. LB managed the project team and review processes. SE and LB drafted the manuscript. All authors edited the manuscript and provided feedback. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Elliott, S.A., Bialy, L., Scott, S.D. et al. Exploring methods for creating or adapting knowledge mobilization products for culturally and linguistically diverse audiences: a scoping review. Arch Public Health 82, 111 (2024). https://doi.org/10.1186/s13690-024-01334-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13690-024-01334-0