
Abstract
Introduction
Drug use is highly prevalent among female sex workers (FSWs). Some forms of drug use, such as injecting drug users (IDU), put them at greater risks for HIV and blood born disease (BBD). In this study, the pattern of drug use and its related factors among Iranian FSWs were investigated.
Materials and methods
This cross-sectional study was performed based on the data of the integrated bio-behavioral surveillance-III (IBBS-III) on FSWs in 8 cities of Iran using the respondent-driven sampling (RDS) method conducting in 2019–2020. Of the 1515 FSWs participating in the IBBS-III study, 1,480 answered questions about drug use. To calculate the prevalence of drug use lifetime and in the past month, weighted analysis was used. Univariate and multivariate logistic regression was used to investigate the factors related to drug use.
Results
The prevalence of lifetime drug use and the prevalence of current drug use (single and poly drug use) among FSWs were estimated to be 29.3% and 18.86%, respectively. According to multivariate regression analysis, the odds ratio (odds) of lifetime drug use showed a statistically significant association with lower education (AOR = 1.18; 95% CI: 1.07–1.3), being a direct sex worker (AOR = 1.77; 95% CI: 1.21–2.61), working in team houses or hangouts (AOR = 1.51; 95% CI: 1.10–2.06), a history of intentional abortion (AOR = 1.41; 95% CI: 1.07–1.87), condom use in the last sex (AOR = 1.61; 95% CI: 1.19–2.17), a history of imprisonment (AOR = 3.05; 95% CI: 2.25–4.14), HIV positive tests (AOR = 8.24; 95% CI: 1.66–40.9), alcohol use (AOR = 1.69; 95% CI: 1.29–2.29), and finding sexual clients in places such as parties, shopping malls, streets, and hotels, or by friends (AOR = 1.46; 95% CI: 1.01–2.12).
Conclusion
Given that drug use among FSWs is about 14 times higher than that of the Iranian general population, it is imperative that drug reduction programs be integrated into service packages. Specifically, prevention programs should be prioritized for occasional drug users within this population as they are at a greater risk of developing drug use issues compared to the general population.
Similar content being viewed by others


Text box 1. Contributions to the literature |
|---|
•It’s important to recognize that FSWs are a vulnerable population that faces a range of challenges and risks, and that addressing these challenges requires a comprehensive and multi-faceted approach that takes into account the complex interplay of physical, social, emotional, and economic factors that contribute to their vulnerability. |
•Addressing the structural and systemic factors that perpetuate the vulnerability of FSWs may require changes to laws and policies that criminalize sex work and contribute to the marginalization of this population. |
•Overall, addressing the challenges faced by FSWs requires a holistic and multi-faceted approach that takes into account the complex interplay of factors that contribute to their vulnerability. By addressing these factors, we can help to promote the health, well-being, and safety of this vulnerable population. |
Introduction
The high prevalence of drug use in FSWs has been reported in various international studies [1, 2]. FSWs may use drug as a mechanism to dull or numb themselves to future triggering encounters with clients. Most FSWs experience a wide range of physical, social, emotional, and economic situations which, individually or in combination, increase their vulnerability and put them at risk [3, 4]. Drug use among FSWs is a worldwide high-risk behavior in this group. Some FSWs may use it due to their dependence on drugs. Others may start taking it to meet the job and environmental challenges associated with sexual activities [5].
Studies show that deaths due to drug use occur faster among women than men, and in FSWs because of violence, deaths caused by drug use are increasing. One of the risk factors which has led to an increase in the diseases caused by drug use and alcohol use is unprotected sex [6]. Drug use and low or no condom use are high-risk behaviors which increase the prevalence of HIV in FSWs than the general population. Risks and harms of drug use are higher among FSWs, especially those with injecting drug users (IDU) and prisoners [5].
Estimates show that between 0.1% and 7.4% of the general population of women at reproductive ages in different regions are FSWs [7]. Also, about 57 to 90% of FSWs are involved in IDU, and between 46 and 96% of them are addicted to illegal drugs [8]. In Iran, drug use is also recognized as a common high-risk behavior among FSWs [9].
It is difficult to investigate drug use and FSWs because both activities are illegal and highly stigmatized. As a result, obtaining accurate information is difficult in this regard. Obtaining information about FSWs and drug use in this group increases our understanding of this group’s needs and helps to design appropriate interventions [10, 11]. Similar to other countries, there are different types of FSWs in Iran. The majority of FSWs in Iran engage in sexual activities in small groups and as an individual business but some are associated with homes and places known as "illegal brothels" where they can meet clients [3]. However, experts believe that FSWs located on the street are the most dangerous subgroups, especially those who have a profile of multiple high-risk behaviors, including drug use, and should be targeted by a prevention program [12]. Due to the importance of drug use in FSWs and its individual and social consequences, such as increasing the prevalence of HIV in them and subsequently in the society, and the inadequacy of national studies and limitations of previous studies, the present study was conducted to investigate the prevalence of drug use and its related factors among FSWs in surveillance system with IBBS-III of HIV / AIDS in Iran.
Materials and methods
Study design, setting and participants
This cross-sectional study was conducted using the data obtained through the integrated bio-behavioral surveillance-III (IBBS-III) survey among FSWs using respondent-driven sampling (RDS) in 2019–2020. The IBBS-III survey was conducted in eight large cities of Iran including Tehran, Tabriz, Shiraz, Mashhad, Kermanshah, Bandar Abbas, and Khorramabad.
Inclusion criteria included age 16 years or older, having sex (vaginal / anal) with more than one male client in the past year, living or working in the city, and giving initial consent to participate in the study. 1515 FSWs participated in the research.
Data collection
Recruitment started with 4–9 seeds representing different groups of FSWs and data were collected face-to-face interview in the RDS centers. All eight cities used the same questionnaire containing different sections: demographic characteristics; history of sexual with clients; alcohol consumption and drug abuse; and discrimination and history of detention.
Dependent variables
The dependent variables were the history of lifetime drug use as a binary variable (yes, no) and current drug use based on the frequency of drug use per person like no drug use, i.e. women who had not used any drug in the past six months, single drug use, i.e. women who used only one type of drug, and poly drug use, i.e. women who used more than one type of drugs. By drug, we mean Opium, heroin, Hashish, methamphetamine, Psychedelic drugs such as MDMA, Norgesic, Marijuana.Note that drug use in the last six months is considered as current use. Infrequent users were those who characterized their use as monthly or less; moderate users were those admitting to use on weekends or on no more than 2 days during any particular week; regular users used at least 3 days per week but no more than 5 days per week; daily users used nearly every day (6 or 7 days per week) [13].
Covariates
The variables studied in this research included the age, marital status (single, married, divorced, concubine,Footnote 1 widow, living with a partner), level of education (illiterate, elementary school, middle school, high school, diploma and academic), type of FSWs (direct (transactional sex as the main source of income), indirect (the main source of income is not transactional sex), age at the first vaginal or anal sex, age of first transactional sex, history of presence in team houses and hangouts to have sex with clients or find a client (yes, no), the main way of finding customers (team houses / hangouts, referrers (owners and pimps), virtual sex (via a mobile, internet and social networks) and others (parties, shopping malls, streets, parks, hotels and inns, and public transportation places, or friends)), history of anal sex (yes, no), history of group sex (yes, no), history of intentional abortion (yes, no), number of clients in the past month (1, 2–5, 6 clients and more), condom use in the last vaginal, anal or oral sex (yes, no), history of detention or imprisonment (yes, no), result of HIV serology tests (positive, negative) and lifetime alcohol use (yes, no).
Data entry and analysis
In this study, the data of all cities were merged after examining the possibility of errors in entering the data into the software and after cleaning. Finally, 1480 women who answered the questions related to drug use were analyzed. Descriptive analysis included weighted mean ± standard deviation (SD) or number (adjusted percentage) calculated based on RDS-II method and Bootstraps #1000. P-value in the contingency tables was assigned to the weighted frequencies calculated by RDS software not crude frequencies. The P-value obtained for qualitative and quantitative variables was based on Pearson's Chi-squared and t-test, respectively. We decided to consider lifetime use in a multivariate model, because we believe that any woman who is FSW and uses drugs at least once has the potential for risky behavior. To identify the factors associated with drug use, all the variables with a P < 0.05 at the univariable model were included in the multivariable analysis. Univariate and multivariate logistic regression was performed using non-weighted analysis based on the suggestion in the latest article. Stata software (version 14), RDS Analyze and R (version 4.1.2) were used to perform all analyzes. (For more information on the RDS software settings used about seeds, refer to [14]).
Results
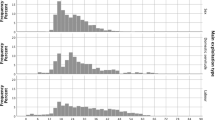
In this study, 1480 FSWs with a mean (standard deviation) (SD) age of 35.76 years (9.15) were evaluated. The prevalence of lifetime drug use and the prevalence of current drug use (single or poly drug use) among FSWs were estimated to be 29.3% and 18.86%, respectively. The mean (SD) age of onset of drug use in FSWs was 23.96 (7.69) years.
The results showed that the highest prevalence of lifetime drug use (33.27%) was in the age group of 41–50 years. Also, the prevalence of lifetime drug use was higher in concubine women. Single and poly drug use in widows and concubines were reported 12.85% and 17.24%, respectively. In this study, the prevalence of lifetime drug use in women living with a partner was reported 47.92%. Also, the prevalence of lifetime drug use in terms of the education levels was 37.18% in illiterate people. In terms of FSWs’ types, the prevalence of lifetime drug use was higher in women who was a direct sex worker (31.25%) (Table 1).
The results showed that the mean (SD) age of FSWs at the first sexual relation and the first transactional sex in individuals with lifetime drug use was 17.03 (4.25) and 26 (8.49) years, respectively, and the mean age of first transactional sex in FSWs showed a statistically significant difference for both outcomes. Also, the prevalence of lifetime drug use was reported in 39.06% of people who were in team houses and the prevalence of single and poly drug use in FSWs was 13.51% and 12.45%, respectively. The highest prevalence of single and poly drug use was reported 12.49% (in FSWs with 6 or more customers) and 14.10% (in FSWs with ones with 2–5 clients) respectively. The prevalence of drug use was higher in FSWs with a history of abortion, and imprisonment, with an HIV positive test, who had used a condom in their last sex, and who alcohol use and found customers in ways other than hangouts and pimps while they showed a significant association (Table 2). 273 (with a weighted percentage of 89%) of the FSWs who used drugs in the last month had a history of using drugs during their sexual activities in the last month. Among FSWs who have had lifetime drug use (with the weight percentage corresponding to the number), 35 (6.51%) of the FSWs are moderate users, 25 (4.14%) regular users, 236 (51.71%) daily users. The rest of the FSWs, 213(37.65%) are either infrequent drug users or did not answer the question.
Based on multivariate regression analysis, the odds of drug use in lifetime increase with decreasing education from the academic level compared to the lower levels (AOR = 1.18; 95% CI: 1.07–1.3), and who were direct sex workers (AOR = 1.77; 95% CI: 1.21–2.61). Work in team houses or hangouts showed a significant association with lifetime drug use (AOR = 1.51; 95% CI: 1.10–2.06). Also lifetime drug use showed a statistically significant association with a history of intentional abortion (AOR = 1.41; 95% CI: 1.07–1.87), condom use in the last sex (AOR = 1.61; 95% CI: 1.19–2.17), a history of imprisonment (AOR = 3.05; 95% CI: 2.25–4.14), an HIV sero- status positive (AOR = 8.24; 95% CI: 1.66–40.9), alcohol use (AOR = 1.69; 95% CI: 1.29–2.29), and finding a sex client in parties, shopping centers, streets, and hotels or by friends (AOR = 1.46; 95% CI: 1.01–2.12) (Table 3).
Discussion
The results of the present study showed that the prevalence of lifetime drug use and the prevalence of current drug use (single or poly drug use) among FSWs were estimated to be 29.3% and 18.86%, respectively. Also in multivariate logistic regression, education levels, types of FSWs (direct/ indirect sex worker), work in team houses / hangouts, a history of intentional abortion, condom use in the last sex, a history of arrest or prison, HIV positive tests, alcohol use and finding a customer through other ways than hangouts and pimps showed a significant association with lifetime drug use.
In the present study, the prevalence of lifetime drug use among FSWs was estimated to be 29.3% (95% CI: 29.4–33.65). This rate is much higher than the prevalence of drug use in the Iranian adult women, which has been reported to be about 1.2% [15, 16]. However, the prevalence of lifetime drug use in international studies is wide, ranging from 2.6% to 7.4% in China [12, 17], 25% in the region with a high prevalence of HIV in India, 34% in China-Myanmar border [18, 19], and more than 90% in Australia [8]. The results of the study by Roshanfekr et al. in Iran showed that the prevalence of non-IDU lifetime and in the last month drug use was 60.3% (95% CI: 51–84) and 47.2% (95% CI: 38–67) respectively [3] while the study of Shokouhi et al. in Iran reported the prevalence of drug use in the last month at 24.9% (95% CI: 16.1–36.4) [20]. In the study of Ahmadi et al. in Iran, the prevalence of IDU was reported to be more than 20% among FSWs [21]. The results of a meta-analysis on FSWs in Iran showed that the prevalence of IDU and non-IDU was 67.5% (95% CI: 2.09–10.73) and 56.94% (95% CI: 44.68–68.78), respectively [22]. The results of a BSS study in Iran showed that 24.9% of FSWs had reported drug use in the last month [22]. A high prevalence of lifetime drug use among FSWs was reported in Iran and in the provinces of Mazandaran (59%) [23], Fars (69.9%) [24] and Tehran (90.7%). The longer the period of FSWs, the higher the prevalence of drug use. For this reason, harm reduction programs of drug use among FSWs are recommended to be prioritized to improve their health status and reduce the prevalence of HIV/AIDS in the community.
The pattern of drug use also varies among FSWs. In the study by Tegang et al., 79% of FSWs was reported more than one type of drug use [25]. The results of other studies in Iran showed that having more clients, experiencing sexual violence or forced sex, instable housing or homelessness, and imprisonment were significantly associated with the likelihood of crystal methamphetamine use, single and poly drug use [20, 26]. Drug use may also lead to an increase in other high-risk sexual behaviors [27].
The results of the present study showed that there was no statistically significant association between the marital status and lifetime drug use among FSWs, which was consistent with the results of other studies [28, 29]. According to the study of Roshanfekr et al., the odds of using non-IDU among divorced FSWs was 2 times higher than that in single FSWs [3]. Temporary marriage can be an indicator of poor communication or family support, and low socioeconomic status among sex workers, which is associated with an increased risk of drug use [20].
The results of the present study showed that there was a significant association between low education levels and lifetime drug use, which was consistent with the results of other studies in Iran and China [12, 20, 21, 28]. However, there are inconsistent results which show that drug use is higher in people with higher education [29, 30]. Also, in previous studies, a significant association was observed between low levels of education as one of the important indicators of individuals’ socio-economic status and drug use [15]. Of course, people with lower education may report behavioral problems more than people with higher education [31].
The association between sexual activities in team homes and lifetime drug use was reported in this research. In the study of Shokouhi et al. in Iran, a higher frequency of drug use has been reported among FSWs with a larger number of sexual partners, which indicates that the impact of drug use is greater on high-risk behaviors [20].
The results of the present study and other ones showed that the prevalence of lifetime drug use was higher among HIV positive FSWs [20]. In the study by Lau et al., unprotected sex due to lack of condoms, making more money, and the demand for unprotected sex by clients were among the factors associated with using IDU or non-IDU and the increased incidence of HIV [32]. Access to HIV prevention, treatment, and care programs is difficult for many FSWs and people with IDU, especially in low- and middle-income countries. Poor coverage of services to this group as well as the lack of government support increase the disease prevalence in FSWs [33].
The association between a history of alcohol use and lifetime drug use among FSWs was reported in this study, which was consistent with the results of the study by Li et al. [34]. In the study by Medhi et al., the results showed that alcohol use was more common with drug use among FSWs, and a significant association was observed between alcohol use (at least once a week) and drug use among FSWs [18]. Low socioeconomic status, income, and education levels increase the susceptibility of FSWs to drug use [35]. Simultaneous alcohol and drug use is among the undesirable behaviors which require prevention programs to be changed.
The results of the study showed that the odds of history of intentional abortion was higher in lifetime drug use FSWs. The association between intentional abortion and drug use has been reported in other studies, which was consistent with the results of the present study [35, 36]. Relations with multiple sexual partners, less awareness of condom use, or less access to contraceptive methods lead to unwanted pregnancies and an increase in intentional abortion [37].
The results showed that the prevalence of lifetime drug use was higher in FSWs who found their clients through parties, shopping malls, streets, parks, hotels and inns, public transportation places, and friends. Clubs, cafes, team houses or hangouts are the main places for FSWs to find sexual partners, drug use and thus engage in risky behaviors [35].
There were several limitations in this RDS study, one of which was the nature of cross-sectional studies. In this type of study, we could only examine the existence or non-existence of the association between independent factors and the pattern of drug use and not its causality. Another limitation of this study was the non-random nature of the study samples. Random sampling is almost impossible in all hidden groups, but RDS sampling is its best alternative for hidden populations. One of the main limitations in the field of FSWs is that a consent letter for FSWs under 18 years of age must be obtained from the legal guardian of these people, while most of these people do not have a guardian or cannot be reached at all. This issue leads to this important group being ignored. A suggestion for future studies is to include a question in the questionnaire about how many years FSWs have been using drugs continuously.
Conclusion
Given that drug use among FSWs is about 14 times higher than that of the Iranian general population, it is imperative that drug reduction programs be integrated into service packages. Specifically, prevention programs should be prioritized for occasional drug users within this population as they are at a greater risk of developing drug use issues compared to the general population.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the corresponding author.
Notes
Concubine is a term that refers to marriage for a short period of time, not for the rest of their life, and does not include a legal contract between couples who are considered lifelong partners.
References
Lancaster KE, Go VF, Lungu T, Mmodzi P, Hosseinipour MC, Chadwick K, et al. Substance use and HIV infection awareness among HIV-infected female sex workers in Lilongwe. Malawi Int J Drug Policy. 2016;30:124–31.
Pérez-Figueroa R, Mittal I, Halpern M, Pérez-Mencia M, Donastorg Y, Taylor B, et al. Drug use, sexual risk, and structural vulnerability among female sex workers in two urban centers of the Dominican Republic: the EPIC study. Drug Alcohol Depend. 2020;212:108039.
Roshanfekr P, Khezri M, Karimi SE, Vameghi M, Ali D, Ahmadi S, et al. Lifetime and past-month substance use and injection among street-based female sex workers in Iran. Harm Reduct J. 2021;18:1–9.
Wechsberg WM, Wu L-T, Zule WA, Parry CD, Browne FA, Luseno WK, et al. Substance abuse, treatment needs and access among female sex workers and non-sex workers in Pretoria, South Africa. Subst Abuse Treat Prev Policy. 2009;4:1–11.
Strathdee SA, Hallett TB, Bobrova N, Rhodes T, Booth R, Abdool R, et al. HIV and risk environment for injecting drug users: the past, present, and future. Lancet. 2010;376(9737):268–84.
Mokdad AH, Forouzanfar MH, Daoud F, Mokdad AA, El Bcheraoui C, Moradi-Lakeh M, et al. Global burden of diseases, injuries, and risk factors for young people’s health during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2016;387(10036):2383–401.
Vandepitte J, Lyerla R, Dallabetta G, Crabbé F, Alary M, Buvé A. Estimates of the number of female sex workers in different regions of the world. Sexually Transmitted Infections. 2006;82(suppl 3):iii18–25.
Roxburgh A, Degenhardt L, Copeland J, Larance B. Drug dependence and associated risks among female street-based sex workers in the greater Sydney area. Australia Substance use & misuse. 2008;43(8–9):1202–17.
Karamouzian M, Shokoohi M, Kaplan RL, Noroozi A, Sharifi H, Baral SD, et al. Characterizing the relationship between incarceration and structural risks among female sex workers in Iran: findings of a nationwide biobehavioral surveillance survey. Ann Epidemiol. 2019;35:29–34.
Strathdee SA, West BS, Reed E, Moazan B, Azim T, Dolan K. Substance use and HIV among female sex workers and female prisoners: risk environments and implications for prevention, treatment, and policies. J Acquir Immune Defic Syndr (1999). 2015;69(0 1):S110.
Wiessing L, Ferri M, Běláčková V, Carrieri P, Friedman SR, Folch C, et al. Monitoring quality and coverage of harm reduction services for people who use drugs: a consensus study. Harm Reduct J. 2017;14:1–14.
Li J, Gong XD, Yue X, Jiang N. Dual Epidemics of Club Drug Use and Sexually Transmitted Infections among Chinese Female Sex Workers: New Challenges to STI Prevention. Biomed Res Int. 2017;2017:2093421. https://doi.org/10.1155/2017/2093421.
Harrison L. The validity of self-reported drug use in survey research: an overview and critique of research methods. NIDA Res Monogr. 1997;167:17-36. PMID: 9243555.
Izadi N, Gouya M-M, Akbarpour S, Zareie B, Moradi Y, Kazerooni PA, et al. HIV prevalence and associated factors among female sex workers in Iran: a bio-behavioral survey in 2020. AIDS Behav. 2023;27(3):909–18.
Amin-Esmaeili M, Rahimi-Movaghar A, Sharifi V, Hajebi A, Radgoodarzi R, Mojtabai R, et al. Epidemiology of illicit drug use disorders in Iran: prevalence, correlates, comorbidity and service utilization results from the Iranian Mental Health Survey. Addiction. 2016;111(10):1836–47.
Noorbala AA, Saljoughian A, Yazdi SAB, Faghihzadeh E, Farahzadi MH, Kamali K, et al. Evaluation of drug and alcohol abuse in people aged 15 years and older in Iran. Iran J Public Health. 2020;49(10):1940.
Tang Z, Zhang C, Li X, Liu Y, Su S, Zhou Y, et al. HIV risk among female sex workers with different patterns of drug use behaviors in Southwest China: a cross-sectional study. AIDS Care. 2015;27(3):293–300.
Medhi GK, Mahanta J, Kermode M, Paranjape RS, Adhikary R, Phukan SK, et al. Factors associated with history of drug use among female sex workers (FSW) in a high HIV prevalence state of India. BMC Public Health. 2012;12(1):1–8.
Hail-Jares K, Choi S, Duo L, Luo Z, Huang ZJ. Occupational and demographic factors associated with drug use among female sex workers at the China-Myanmar border. Drug Alcohol Depend. 2016;161:42–9.
Shokoohi M, Karamouzian M, Bauer GR, Sharifi H, Hooshyar SH, Mirzazadeh A. Drug use patterns and associated factors among female sex workers in Iran. Addict Behav. 2019;90:40–7.
Ahmadi K, Rezazade M, Nafarie M, Moazen B, Yarmohmmadi Vasel M, Assari S. Unprotected Sex with Injecting Drug Users among Iranian Female Sex Workers: Unhide HIV Risk Study. AIDS Res Treat. 2012;2012:651070. https://doi.org/10.1155/2012/651070.
Tavakoli F, Khezri M, Tam M, Bazrafshan A, Sharifi H, Shokoohi M. Injection and non-injection drug use among female sex workers in Iran: a systematic review and meta-analysis. Drug Alcohol Depend. 2021;221:108655.
Taghizadeh H, Taghizadeh F, Fathi M, Reihani P, Shirdel N, Rezaee SM. Drug Use and High-Risk Sexual Behaviors of Women at a Drop-In Center in Mazandaran Province, Iran, 2014. Iran J Psychiatry Behav Sci. 2015;9(2):e1047. https://doi.org/10.17795/ijpbs1047.
Kazerooni PA, Motazedian N, Motamedifar M, Sayadi M, Sabet M, Lari MA, et al. The prevalence of human immunodeficiency virus and sexually transmitted infections among female sex workers in Shiraz, South of Iran: by respondent-driven sampling. Int J STD AIDS. 2014;25(2):155–61.
Tegang S-P. Concurrent sexual and substance-use risk behaviours among female sex workers in Kenya’s Coast Province: findings from a behavioural monitoring survey. SAHARA: J Soc Aspects of HIV/AIDS Res Alliance. 2010;7(4):10–6.
Shokoohi M, Karamouzian M, Sharifi H, Rahimi-Movaghar A, Carrico AW, Hooshyar SH, et al. Crystal methamphetamine use and its correlates in women engaged in sex work in a developing country setting. Drug Alcohol Depend. 2018;185:260–5.
Woods-Jaeger BA, Jaeger JA, Donenberg GR, Wilson HW. The relationship between substance use and sexual health among African-American female adolescents with a history of seeking mental health services. Womens Health Issues. 2013;23(6):e365–71.
Li J, Jiang N, Yue X, Gong X. [Club drug use and its association with syphilis infection among female sex workers]. Zhonghua Liu Xing Bing Xue Za Zhi. 2014;35(11):1223-6.
Yu YJ, McCarty C, Wang B. Network and individual factors associated with drug use among female sex workers (FSWs) in Southern China: A mixed-method approach. Subst Use Misuse. 2018;53(11):1763–70.
Puradiredja DI, Coast E. Transactional sex risk across a typology of rural and urban female sex workers in Indonesia: a mixed methods study. PLoS ONE. 2012;7(12):e52858.
Brener ND, Billy JO, Grady WR. Assessment of factors affecting the validity of self-reported health-risk behavior among adolescents: evidence from the scientific literature. J Adolesc Health. 2003;33(6):436–57.
Lau JT, Gu J, Tsui HY, Chen H, Holroyd E, Wang R, et al. Prevalence and associated factors of condom use during commercial sex by female sex workers who were or were not injecting drug users in China. Sexual health. 2012;9(4):368–76.
Baral S, Beyrer C, Muessig K, Poteat T, Wirtz AL, Decker MR, Sherman SG, Kerrigan D. Burden of HIV among female sex workers in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Infect Dis. 2012;12(7):538-49. https://doi.org/10.1016/S1473-3099(12)70066-X.
Li Q, Li X, Stanton B. Alcohol use among female sex workers and male clients: an integrative review of global literature. Alcohol Alcohol. 2010;45(2):188–99.
Galea S, Nandi A, Vlahov D. The social epidemiology of substance use. Epidemiol Rev. 2004;26(1):36–52.
Benotsch EG, Somlai AM, Pinkerton SD, Kelly JA, Ostrovski D, Gore-Felton C, et al. Drug use and sexual risk behaviours among female Russian IDUs who exchange sex for money or drugs. Int J STD AIDS. 2004;15(5):343–7.
Luchters S, Geibel S, Syengo M, Lango D, King’Ola N, Temmerman M, et al. Use of AUDIT, and measures of drinking frequency and patterns to detect associations between alcohol and sexual behaviour in male sex workers in Kenya. BMC Public Health. 2011;11:1–8.
Acknowledgements
We are whole-heartedly grateful to all those participants and interviewers who collaborated with us in collecting the study data.
Funding
Vice-Chancellor funded this study for Research and Technology of Kurdistan University of Medical Sciences, Sanandaj, Iran.
Author information
Authors and Affiliations
Contributions
GM, MMG, BZ, and MAR conceived and designed the study. BZ, MAR and GM analyzed and interpreted the data and drafted the manuscript. BZ, MAR, GM, SA, FH, ER, YM, MMG, and AS were involved in the composition of the study tool, collect data, supervision of the research process, and critical revision and review of the manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee of Kurdistan University of Medical Sciences reviewed and approved this study (IR.MUK.REC.1398.132) and accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All women were given information about the study and asked for written informed consent to participate.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zareie, B., Rasouli, M.A., Gouya, M.M. et al. Drug use patterns and related factors among female sex workers in Iran in 2019–2020: results from Integrated Bio-Behavioral Surveillance-III (IBBS-III). Arch Public Health 81, 120 (2023). https://doi.org/10.1186/s13690-023-01143-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13690-023-01143-x