
Abstract
Background
Globally, infant mortality is a major public health concern and a sensitive indicator of countries' socio-economic and health status. Despite the substantial reduction of under-five mortality in sub-Saharan African countries specifically in East Africa, the infant mortality rate remains highest and too far below to achieve the WHO target. As to our search of the literature is concerned, there is a dearth of evidence on the incidence and predictors of infant mortality in East Africa. Therefore, this study investigated the incidence of infant mortality and its predictors in East Africa.
Methods
The present study has utilized 138,803 weighted samples from Demographic and Health Surveys (DHSs) of 12 East African countries. Considering the hierarchical nature of DHS data shared frailty parametric survival models were fitted and compared based on deviance (-2LLR), AIC, and BIC. Gompertz gamma shared frailty model was the best-fitted model for the data since it had the lowest deviance, AIC, and BIC values. Variables with a p-value < 0.2 in the bi-variable analysis were considered for the multivariable analysis. In the multivariable Gompertz gamma shared analysis, the Adjusted Hazard Ratio (AHR) with 95% Confidence Interval (CI) was reported to declare the significant predictors of infant mortality.
Results
The infant mortality rate in East Africa was 41.41 per 1000 live births. Mothers aged 25–34 years, wanted birth, health facility delivery, 1–3 ANC visit, being 2nd- 4th birth order, 5th and above, the birth interval of 24–48 months, and birth interval of 49 months and above were significantly associated with lower risk of infant mortality. Whereas women who didn’t have formal education, women who didn't participate in making health care decisions making, being male children, cesarean delivery, small size at birth, and large size at birth were significantly associated with a higher risk of infant mortality.
Conclusion
Despite the substantial progress in improving maternal and child health, this study showed that infant mortality is still a major public health concern in East Africa. Maternal age, place of delivery, maternal education, birth size, sex of the child, mode of delivery, women's autonomy, birth order, birth interval, and ANC visit were found to be significant predictors of infant mortality. Therefore, public health interventions enhancing health facility delivery, ANC visit, maternal education, birth spacing, and empowering women are crucial for reducing the incidence of infant mortality in East Africa.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Despite the remarkable reduction in infant mortality worldwide, 4.1 million children still died every year before their first birthday, accounting for 73% of under-5 mortality [1]. The global infant mortality rate decreased from 65 deaths per 1000 live births in 1990 to 29 deaths per 1000 live births in 2017 [2]. Infant mortality is one of the most important indicators of population health and has important implications for countries' economic development, social well-being, and access to medical care [3, 4].
Notwithstanding the substantial reduction in under-five mortality, infant mortality remains high and continues as a major public health challenge [1, 5,6,7]. The deaths are primarily concentrated in Sub-Saharan Africa specifically East Africa, which has the greatest infant mortality rate (92.2% per 1000 live births) when compared to developed countries (8 death per 1000 birth) [2, 8]. It is primarily caused by preventable factors that can be eradicated by providing necessities, and it is seen as a reflection of disparities in infrastructure, services, and socioeconomic development [9]. Almost 80% of infant deaths could have been avoided, and the majority (51.3%) could have been reduced if mothers had received proper care during their pregnancy and infants had received basic care [10].
Infant mortality is still a public health issue around the world, particularly in low-income countries [11], and is used as an important woman and child health indicator [12, 13]. However, despite progress made by many countries to achieve the Millennium Development Goals (MDG) 4 to reduce child mortality by two-thirds between the years 1990 and 2015 [14], half of the world’s nations are still behind their targets [15]. Millions of babies are estimated to die in the first year of life in East Africa but most die at home, remain uncounted, and are invisible to public health programs[16, 17]. Unlike developed countries, East Africa's reduction in infant mortality has shown slow progress, due to the continued huge burden of pneumonia, diarrhea, malaria, and vaccine-preventable diseases [18,19,20]. Previous literature documented that infant mortality was significantly associated with place of delivery [21], mode of delivery [22], Antenatal Care (ANC) visit during pregnancy [23], preceding birth interval [24], maternal education [25,26,27], media exposure [28], and place of residence [21, 29]. Besides, women's health care decision-making [30,31,32], household wealth status [33,34,35], distance to a health facility [12, 36], birth order [37], wanted pregnancy [38], childbirth size [39], multiple births [40] and sex of child [41] were found to be significant predictors of infant mortality.
Despite East African countries sharing the huge burden of global infant mortality, as to our search of the literature, there is limited evidence on the pooled incidence and predictors of infant mortality in East Africa. Therefore, this study aimed to investigate the predictors of infant mortality in East Africa based on the pooled DHS data in 12 East African countries. Given DHS data nature, studying the effect of community clustering on infant mortality has both research and policy implications. We can determine the risk factors of infant mortality, accounting for the correlated observations of live births in the same cluster. Having identified the literature gaps to capture the incidence and predictors of infant mortality, the present study investigated whether there are dependencies between study subjects within the same community, that is, to check if the children share similar frailty within the community.
Methods and materials
Study design and area
The Demographic and Health Surveys (DHSs) of the 12 East African countries were the data source for the present study. These were Burundi, Ethiopia, Comoros, Uganda, Rwanda, Tanzania, Mozambique, Madagascar, Zimbabwe, Kenya, Zambia, and Malawi. The DHS is a nationally representative survey that provides data for monitoring indicators of population dynamics, nutrition, and health. The permission to use the data was granted from the measure DHS program.
Study population and sampling
Newborns from birth to the first year of birth in 12 East African countries were the source of the population whereas those found in the selected Enumeration Areas (EAs) or clusters were the study population. A multi-stage cluster sampling technique was employed to recruit the samples using EAs and households as primary and secondary sampling units, respectively. In DHS, some of the regions or counties were oversampled and some were undersampled specifically in large counties or regions. Therefore, we have applied sample weighting for the computation of means, percentages, and regression as per the DHS recommendation to restore the representativeness of the data at the national and sub-national levels. for this study. The most recent births of the mother were considered for this study and the data were extracted from the Kids Record (KR) file. A total of 138,803 most recent live births were considered for analysis.
Study variables
Dependent variable
The time to death of the children before their first birthday was the dependent variable. Children who died in the first year of life were considered as having the event and coded as 1 whereas those who were not were considered censored and coded as 0. The information about child survival was obtained retrospectively by interviewing the mother. Age at death was recorded in months.
Explanatory variables
The explanatory variables were categorized into three themes. 1) Demographic variables; residence, marital status, maternal age, and country, 2) socio-economic variables; maternal education, husband education, wealth status, media exposure, and maternal occupation, and 3) maternal obstetric and child-related variables were child age, sex of the child, birth order, birth size, birth outcome, birth size, place of delivery, mode of delivery, women's health care decision making autonomy, unwanted pregnancy, number of ANC visits, preceding birth interval and distance to the health facility.
Statistical analysis
All the reported results were based on the weighted data and STATA version 17 and R version 3.5.1 software were used for analysis. The global Schoenfeld residuals test (both global and scaled) and graphical methods were used to check the proportional hazard assumption. When the p-value < 0.05, indicated the proportional hazard assumption was violated, this indicates the Cox-proportional model is not an appropriate model. Because the proportional hazard assumption was violated, the Cox-proportional model was ruled out. Unlike the Cox model, the parametric survival models assume a particular distribution whose parameters depend on the covariates. We compared the equality of the survival curve across population groups using a log-rank test with the null hypothesis of no difference between two or more survival distributions at any point in time.
Given the hierarchical nature of the DHS data, infants were nested within EAs. There might be the possibility of a clustering effect and therefore the fundamental assumption of the classical regression model i.e. equal variance and independence of observations. Parametric survival models were fitted. Then we checked whether there is clustering or not by fitting the frailty model (random effect survival model) and the theta value was significant in the null model, if its p-value is < 0.05, indicates that there is unobserved heterogeneity or shared frailty. Therefore, infants in one cluster were more related to each other than infants in other clusters. In addition, the LR-test assesses whether the shared frailty model was the best-fitted model compared to the classical model for the data. Frailty can't be directly estimated from the data, it is assumed to follow a distribution with mean = 1 and variance = 0. If the frailty is less than 1, the subjects are less likely to be frail, and if greater than 1, the subjects are more likely to be frail. In this study, frailty was modeled according to the number of EAs. Besides, the EDHS data structure has hierarchical nature and we have checked whether there is clustering or not by fitting the frailty model (random effect survival model) and the theta was significant in the null model (θ = 0.03, 95% CI: 0.01, 0.05), LR test of theta = 0: chibar2 (01) = 12.35, Prob > = chibar2 < 0.001). It suggests that there is unobserved heterogeneity or shared frailty. As a result, infants in one cluster were more closely related than those in other groups. Furthermore, because the LR-test was significant, the shared frailty model was the best-fitted model for the data. The Gompertz gamma shared frailty model was shown to be the best-fitting of five parametric models.
Nested parametric models in generalized gamma (Exponential, Weibull, lognormal) were compared based on deviance, and non-nested models (Gompertz and log-logistic) were compared using AIC. Deviance, AIC, and Cox-Snell residual graph. Based on the above-mentioned comparison parameters, the Gompertz gamma shared frailty model was found the best-fitted model for the data.
Variables with a p-value less than 0.20 in the uni-variable gamma shared frailty analysis were included in the multivariable analysis. We estimate the hazard ratio and 95% confidence interval. In the multivariable analysis, the Adjusted Hazard Ratio (AHR) with 95% Confidence Interval (CI) was used to declare significant predictors of infant mortality.
Ethical consideration
Permission for data access was obtained from the measure DHS program through an online request from http://www.dhsprogram.com. The data used for this study were publicly available with no personal identifier.
Results
Descriptive results of the study participants
A total of 138,803 most recent live births were included. About 66,070 (47.6%) of the children were born to mothers aged 25–34 years and more than three-quarters of the respondents (78.3%) were rural residents. About 33,229 (23.9%) and 23,298 (16.8%) of the children belonged to the poorest and richest households, respectively. Nearly one-fourth (24.1%) of the children were born to mothers who didn't have formal education, and the majority (64.9%) of the respondent had no media exposure. Regarding birth size, about 64,315 (46.3%) of them were average size at birth (Table 1).
Infant mortality rate
From the total of 138,803 most recent live births, the overall infant mortality in East Africa was 41.41 (95% CI: 41.41, 41.1) per 1000 live births, and it was varied across regions (Fig. 1).

The infant mortality rate in East African countries
Comparison of failure functions
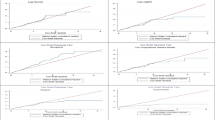
The Kaplan–Meier failure curve was used to compare the probability of mortality across categorical explanatory variables visually and log-rank test objectively. The overall Kaplan–Meier failure curve indicated that the probability of infant mortality increased over time (Fig. 2). There was a statistically significant difference in infant mortality across the residence, country, mode of delivery, birth order, ANC, birth outcome, place of delivery, preceding birth interval, health insurance coverage, distance to the health facility, wanted pregnancy, birth size, maternal education, husband education, respondent age, twin pregnancy, and wealth index (log-rank, p < 0.05) (Table 2).

The Kaplan–Meier failure curve of infant mortality in East Africa
Assessing proportional hazard assumption
Proportional hazard assumption was checked using the global Schoenfeld residuals test (global and scaled) for all possible predictors of infant mortality. The global Schoenfeld residual test and the p-value was < 0.05 (Table 3).
Predictors of infant mortality
In the multivariable Gompertz gamma shared frailty model; country, maternal age, maternal education status, wanted pregnancy, women health care decision-making autonomy, sex of a child, place of delivery, number of ANC visits, mode of delivery, twin birth, birth order, birth size and preceding birth interval were significant predictors of infant mortality. Child in Burundi, Madagascar, Malawi, Mozambique, Tanzania, Uganda, Zambia and Zimbabwe were 1.34 (AHR = 1.34, 95% CI: 1.15, 1.56), 1.20 (AHR = 1.20, 95% CI: 1.03, 1.41), 1.29 (AHR = 1.29, 95% CI: 1.11, 1.50), 1.68 (AHR = 1.68, 95% CI: 1.44, 1.96), 1.23 (AHR = 1.23, 95% CI: 1.04, 1.44), 1.18 (AHR = 1.18, 95% CI: 1.01, 1.37), 1.29 (AHR = 1.29, 95% CI: 1.09, 1.52) and 1.45 (AHR = 1.45, 95% CI: 1.21, 1.74) times higher hazard of death in the first year of life compared to child born in Rwanda respectively. The hazard of infant mortality among children born to mothers aged 25–34 years was decreased by 11% (AHR = 0.89, 95% CI: 0.83, 0.96) than a child born to a mother aged 15–24 years. Mothers who didn’t attend formal education had 1.23 times (AHR = 1.23, 95% CI: 1.13, 1.33) higher hazard of infant mortality than mothers who attained secondary education and higher. Wanted births had decreased the hazard of infant mortality by 32% (AHR = 0.68, 95% CI: 0.64, 0.72) compared to unwanted births. Births born to mothers who didn't participate in making their own health care decision were 1.12 times (AHR = 1.12, 95% CI: 1.04, 1.21) higher hazard of infant mortality compared to a child born to a mother who made their own health care decision. The hazard of infant mortality among male children was increased by 33% (AHR = 1.33, 95% CI: 1.27, 1.43) than female children. The hazard of infant mortality among health facility delivered and having 1–3 ANC visits were decreased by 10% (AHR = 0.90, 95% CI: 0.84, 0.97) and 41% (AHR = 0.59, 95% CI: 0.51, 0.67) than who delivered at home and who didn't have ANC visit during pregnancy, respectively. Cesarean deliveries were 1.13 times (AHR = 1.13, 95% CI: 1.01, 1.25) higher than vaginal deliveries. Multiple births had 4.18 times (AHR = 4.18, 95% CI: 3.84, 4.55) higher hazard of infant mortality than singletons. The hazard of infant mortality among children who were second or fourth birth and above four was lowered by 39% (AHR = 0.61, 95% CI: 0.55, 0.67), and 29% (AHR = 0.71, 95% CI: 0.63, 0.80) compared to first-order birth, respectively. Children who were small and large size at birth were 1.87 times (AHR = 1.87, 95% CI: 1.75, 1.99) and 1.08 times (AHR = 1.08, 95% CI: 1.01, 1.15) at higher hazard of infant mortality than average size child at birth respectively. The hazard of infant mortality among children born to mothers who had a preceding birth interval of 24–48 months and ≥ 49 months were decreased by 49% (SHR = 0.51, 95% CI: 0.47, 0.55) and 51% (AHR = 0.49, 95% CI: 0.45, 0.54) than a child born to mother who had less than 24 months, respectively (Table 4).
Discussion
The present study revealed infant mortality rate in East Africa was 41.41 (95% CI: 41.41, 41.1) per 1000 live births. It was higher than the WHO target [42], it might be due to sub-Saharan African countries specifically East Africa continuing to be the host spot areas of infectious disease, malnutrition, and poor health care access, which in turn directly or indirectly responsible for infant mortality and morbidity [43]. Besides, East Africa faces extreme poverty, poor education, low health knowledge, poor infrastructure, lifestyle, and environmental factors (i.e., limited access to resources such as clean water) that have been identified as primary factors contributing to the high incidence of infant mortality [44, 45].
Maternal age, maternal education status, wanted pregnancy, women health care decision-making autonomy, sex of a child, place of delivery, number of ANC visits, mode of delivery, twin birth, birth order, birth size, and preceding birth interval found to be significant predictors of infant mortality. Maternal education and participation in making health care decisions were found significantly associated with a lower risk of infant mortality. It was in line with studies in Nicaragua [25], Denmark [46], Bangladesh [47], and Pakistan [48]. The possible explanation might be due to maternal education plays a significant role in adopting healthy behaviors and habits that have a positive impact on their child's health and more capable of getting quality care for their children [49]. Women participating in making health care decision-making can make key decisions about their own and their children, such as compliance with vaccination schedules, provision of recommended nutrition, and having a good awareness of childhood illness, these could be responsible for the reduced risk of infant mortality among children born to mothers who have decision making autonomy [50]. In line with study findings reported in Low and middle-income countries (LMIC) [51] and South Asia [52], children born to mothers aged 25–34 years had a lower hazard of infant mortality than children born to mothers aged 15–24 years. The higher risk of infant mortality among births to adolescent mothers could be due to nutritional insufficiencies, because of mother-fetus and infants’ competition for nutrients, as adolescents still require additional energy for growth and development [26]. In addition, teenage pregnancy is a high-risk pregnancy and increases the risk of obstetric complications and adverse child outcomes [53,54,55,56,57]. moreover, studies affirmed that teenagers are less likely to use maternal health care services such as ANC, institutional delivery, PNC, and routine immunization which could increase the risk of infant mortality [58].
Being male increases the hazard of infant mortality to female children. This was supported by a study reported in Pakistan [48], this can be due to males being more vulnerable to morbidities such as low Apgar score, Intra-uterine Growth Restriction (IUGR), respiratory insufficiency, and prematurity than the female sex [59]. Besides, it might be because of a higher level of testosterone among males and this could affect pulmonary biomechanics and vascular development that could make males more vulnerable to respiratory and neurological diseases [60, 61]. In line with studies reported in Bangladesh [62], SSA [63], and India [48], health facility delivery and ANC visits were significantly correlated with decreased risk of infant mortality. It could be due to the reason that ANC visit is an entry point for the other maternal health services, and births from mothers who had no ANC visit are not aware of danger signs of pregnancy and underlying medical conditions that could lead to low birth weight, prematurity, congenital anomalies as compared to women who had ANC visit [64]. Cesarean delivery was significantly associated with an increased risk of infant mortality. It was consistent with studies reported in Nepal [65] and industrialized countries [66]. Though cesarean delivery is life-saving for the mother and the baby during emergency conditions, they are at risk of developing complications due to surgical procedures. Compared to babies born vaginally, babies born by cesarean are at risk for health complications they are more likely to have difficulty breathing on their own and are born preterm before the lungs have fully developed. Mothers who gave birth through cesarean section, mothers and babies are less likely to have skin-to-skin contact immediately after birth, and because of the drug for anesthesia the mother sedates make them not initiate breastfeeding immediately, and the newborn's mouth, esophagus, and airways can also make it more difficult for babies to begin and continue breastfeeding [67, 68].
Twin births and higher-order birth had an increased risk of infant mortality than single births, it was in line with study findings in the USA [69]. The possible explanation for the increased hazard of infant mortality among twins could be because twin births are more likely to experience obstructed labor, birth asphyxia, and competition for nutrition, which in turn increases the risk of respiratory infections and other related complications that can increase their risk of mortality during their first year of life [70, 71]. This also has a programmatic implication of giving special care to women with a twin pregnancy during ANC as well as intrapartum care. Regarding birth order, the birth order increases the financial burden of the family, and poverty affects infant survival through insufficient food intake, greater exposure to infections, and lack of access to vaccinations and basic health care [72].
As evidenced by previous study findings reported in Brazil [73], India [74], and developing countries [24], the birth interval was found a significant predictor of infant mortality in this study. This might be due to shorter birth interval that has been significantly correlated with maternal depletion, sibling competition, and infection transmission [75, 76]. Small size and large size babies at birth were significantly associated with excess risk of infant mortality than average size babies at birth. It was in line with studies in Pakistan [48] and Sweden [77], the possible explanation could be because low birth weight is a good indicator of the newborn's chances for survival, growth, long-term health, and psychosocial development and this could increase the risk of death in the infantile period [78, 79]. Besides, macrosomic infants are closely linked with under-lined medical conditions like DM and other lipodystrophies and are prone to birth trauma during delivery they are at risk of mortality than average size babies [80].
This study has several strengths. First, this study used weighted data to make it representative at national and regional levels, and it can be generalized to all live births in East Africa. Secondly, Gompertez gamma share frailty was fitted by considering the dependency nature of the DHS data to get reliable predictors of infant mortality. Furthermore, the study was based on a large sample size, this could increase the power of the study to get the true effect of the predictors. This finding should be interpreted in light of the following limitations. First, this study was based upon recall by mothers and it is prone to recall bias. Besides, variables such as underlined medical conditions such as congenital heart diseases, pneumonia, malaria, etc. were not included in this study since these variables were not collected in DHS.
Conclusions
The infant mortality rate remains a major public health problem in East Africa with significant variations across the countries. The infant mortality rate is considered the most important sensitive indicator of the socioeconomic and health status of a community and its description is very vital for the evaluation and planning of public health strategies. Place of delivery, ANC visit, twin births, sex of a child, maternal education, women's autonomy, wanted pregnancy, birth size, birth interval, mode of delivery, maternal age, and birth order were found to be significant predictors of infant mortality. Therefore, enhancing health facility delivery, ANC visit, birth spacing, empowering women, and promoting maternal education should be done to reduce the incidence of infant mortality in East Africa.
Availability of data and materials
Data is available online and you can access it from www.measuredhs.com.
Abbreviations
- AHR:
-
Adjusted Hazard Ratio
- AIC:
-
Akakie Information Criteria
- ANC:
-
Antenatal Care
- AHR:
-
Adjusted Hazard Ratio
- CI:
-
Confidence Interval
- DHS:
-
Demographic Health Survey
- DM:
-
Diabetic Mellitus
- LLR:
-
Log-likelihood Ratio
- PH:
-
Proportional Hazard
- SDGs:
-
Sustainable Development Goals
- SSA:
-
Sub-Saharan Africa
- WHO:
-
World Health Organization
References
UNICEF W. Levels and trends in child mortality: report 2011 Estimates developed by the UN Inter-agency Group for child mortality estimation. New York: United Nation’s Children Fund; 2011.
WHO. Global Health Observatory (GHO) data. 2017.
Reidpath DD, Allotey P. Infant mortality rate as an indicator of population health. J Epidemiol Community Health. 2003;57(5):344–6.
Pampel FC Jr, Pillai VK. Patterns and determinants of infant mortality in developed nations, 1950–1975. Demography. 1986;23(4):525–42.
Defo BK. Demographic, epidemiological, and health transitions: are they relevant to population health patterns in Africa? Glob Health Action. 2014;7(1):22443.
Sartorius BK, Sartorius K. Global infant mortality trends and attributable determinants–an ecological study using data from 192 countries for the period 1990–2011. Popul Health Metrics. 2014;12(1):29.
Rutstein SO. Factors associated with trends in infant and child mortality in developing countries during the 1990s. Bull World Health Organ. 2000;78:1256–70.
Ester PV, Torres A, Freire JM, Hernández V, Gil Á. Factors associated to infant mortality in Sub-Saharan Africa. J Public Health Afr. 2011;2(2):e27.
Deogaonkar M: Socio-economic inequality and its effect on healthcare delivery in India: inequality and healthcare. Electron J Sociol. 2004;11.
de Oliveira CM. do Bonfim CV, Guimarães MJB, Frias PG, Medeiros ZM: Infant mortality: temporal trend and contribution of death surveillance. Acta Paulista de Enfermagem. 2016;29(3):282–90.
Organization WH. The World health report: 1998: Life in the 21st century: a vision for all: executive summary. Geneva: World Health Organization; 1998.
Gruber J, Hendren N, Townsend RM. The great equalizer: Health care access and infant mortality in Thailand. Am Econ J Appl Econ. 2014;6(1):91–107.
Masuy-Stroobant G, Gourbin C. Infant health and mortality indicators. Eur J Population. 1995;11(1):63–84.
Rajaratnam JK, Marcus JR, Flaxman AD, Wang H, Levin-Rector A, Dwyer L, Costa M, Lopez AD, Murray CJ. Neonatal, postneonatal, childhood, and under-5 mortality for 187 countries, 1970–2010: a systematic analysis of progress towards Millennium Development Goal 4. Lancet. 2010;375(9730):1988–2008.
Tomashek KM, Qin C, Hsia J, Iyasu S, Barfield WD, Flowers LM. Infant mortality trends and differences between American Indian/Alaska Native infants and white infants in the United States, 1989–1991 and 1998–2000. Am J Public Health. 2006;96(12):2222–7.
Lawn JE, Kerber K, Enweronu-Laryea C, Cousens S. 3.6 million neonatal deaths—what is progressing and what is not? In: Seminars in perinatology: 2010: Elsevier; 2010: 371–386.
Kudamatsu M. Has democratization reduced infant mortality in sub-Saharan Africa? Evidence from micro data. J Eur Econ Assoc. 2012;10(6):1294–317.
Wang H, Bhutta ZA, Coates MM, Coggeshall M, Dandona L, Diallo K, Franca EB, Fraser M, Fullman N, Gething PW. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1725–74.
Bart KJ, Lin KF-YC. Vaccine-preventable disease and immunization in the developing world. Pediatr Clin North Am. 1990;37(3):735–56.
Christian P: Infant mortality. In: Nutrition and Health in Developing countries. edn.: Springer; 2008: 87–111.
Adetunji JA. Infant mortality in Nigeria: effects of place of birth, mother’s education and region of residence. J Biosoc Sci. 1994;26(4):469–77.
Högberg U, Holmgren P. Infant mortality of very preterm infants by mode of delivery, institutional policies and maternal diagnosis. Acta Obstet Gynecol Scand. 2007;86(6):693–700.
Dube L, Taha M, Asefa H. Determinants of infant mortality in community of Gilgel Gibe Field Research Center, Southwest Ethiopia: a matched case control study. BMC Public Health. 2013;13(1):401.
Rutstein SO. Effects of preceding birth intervals on neonatal, infant and under-five years mortality and nutritional status in developing countries: evidence from the demographic and health surveys. Int J Gynecol Obstet. 2005;89:S7–24.
Peña R, Wall S, Persson L-A. The effect of poverty, social inequity, and maternal education on infant mortality in Nicaragua, 1988–1993. Am J Public Health. 2000;90(1):64.
Desai S, Alva S. Maternal education and child health: Is there a strong causal relationship? Demography. 1998;35(1):71–81.
Hobcraft JN, McDonald JW, Rutstein SO. Socio-economic factors in infant and child mortality: a cross-national comparison. Popul Stud. 1984;38(2):193–223.
Aksit B, Aksit B. Sociocultural determinants of infant and child mortality in Turkey. Soc Sci Med. 1989;28(6):571–6.
Clarke LL, Coward RT. A multivariate assessment of the effects of residence on infant mortality. J Rural Health. 1991;7(3):246–65.
Adhikari R, Sawangdee Y. Influence of women’s autonomy on infant mortality in Nepal. Reprod Health. 2011;8(1):7.
Boehmer U, Williamson JB. The impact of women’s status on infant mortality rate: A cross-national analysis. Soc Indic Res. 1996;37(3):333–60.
Jain AK. Determinants of regional variations in infant mortality in rural India. Popul Stud. 1985;39(3):407–24.
Chung H, Muntaner C. Welfare state matters: a typological multilevel analysis of wealthy countries. Health Policy. 2007;80(2):328–39.
Pamuk ER, Fuchs R, Lutz W. Comparing relative effects of education and economic resources on infant mortality in developing countries. Popul Dev Rev. 2011;37(4):637–64.
Sahu D, Nair S, Singh L, Gulati B, Pandey A. Levels, trends & predictors of infant & child mortality among Scheduled Tribes in rural India. Indian J Med Res. 2015;141(5):709.
Frankenberg E. The effects of access to health care on infant mortality in Indonesia. Health Transit Rev. 1995;5(2):143–63.
Cabrera R. The influence of maternal age, birth order and socioeconomic status on infant mortality in Chile. Am J Public Health. 1980;70(2):174–7.
Singh A, Singh A, Mahapatra B. The consequences of unintended pregnancy for maternal and child health in rural India: evidence from prospective data. Matern Child Health J. 2013;17(3):493–500.
Scrimshaw SC. Infant mortality and behavior in the regulation of family size. Popul Develop Rev. 1978;4:383–403.
Uthman OA, Uthman MB, Yahaya I. A population-based study of effect of multiple birth on infant mortality in Nigeria. BMC Pregnancy Childbirth. 2008;8(1):41.
Bicego GT, Ahmad OB. Infant and child mortality. Citeseer; 1996.
Organization WH. Global Health Observatory (GHO) data: infant mortality. Situation and trends. 2016.
Chretien J-P, Anyamba A, Small J, Britch S, Sanchez JL, Halbach AC, Tucker C, Linthicum KJ. Global climate anomalies and potential infectious disease risks: 2014–2015. PLoS currents. 2015;7.
BeLue R, Okoror TA, Iwelunmor J, Taylor KD, Degboe AN, Agyemang C, Ogedegbe G. An overview of cardiovascular risk factor burden in sub-Saharan African countries: a socio-cultural perspective. Glob Health. 2009;5(1):10.
Kjellén M: Health and environment. Sida; 2001.
Olsen O, Madsen M. Effects of maternal education on infant mortality and stillbirths in Denmark. Scand J public health. 1999;27(2):128–36.
Lindenbaum S, Chakraborty M, Elias M. The influence of maternal education on infant and child mortality in Bangladesh. 1985.
Agha S. The determinants of infant mortality in Pakistan. Soc Sci Med. 2000;51(2):199–208.
Hobcraft J. Women’s education, child welfare and child survival: a review of the evidence. Health Transit Rev. 1993;3(2):159–75.
Stiyaningsih H, Wicaksono F. Impact of Women’s empowerment on infant mortality in Indonesia. Kesmas National Public Health J. 2017;11(4):185–91.
Finlay JE, Özaltin E, Canning D. The association of maternal age with infant mortality, child anthropometric failure, diarrhoea and anaemia for first births: evidence from 55 low-and middle-income countries. BMJ Open. 2011;1(2):e000226.
Raj A, McDougal L, Rusch ML. Effects of young maternal age and short interpregnancy interval on infant mortality in South Asia. Int J Gynaecol Obstet. 2014;124(1):86.
Mukhopadhyay P, Chaudhuri R, Paul B. Hospital-based perinatal outcomes and complications in teenage pregnancy in India. J Health Popul Nutr. 2010;28(5):494.
Chen X-K, Wen SW, Fleming N, Demissie K, Rhoads GG, Walker M. Teenage pregnancy and adverse birth outcomes: a large population based retrospective cohort study. Int J Epidemiol. 2007;36(2):368–73.
Paranjothy S, Broughton H, Adappa R, Fone D. Teenage pregnancy: who suffers? Arch Dis Child. 2009;94(3):239–45.
Kalaivani K. Prevalence & consequences of anaemia in pregnancy. Indian J Med Res. 2009;130(5):627–33.
Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, De Onis M, Ezzati M, Grantham-McGregor S, Katz J, Martorell R. Maternal and child undernutrition and overweight in low-income and middle-income countries. The lancet. 2013;382(9890):427–51.
Barber S. Does the quality of prenatal care matter in promoting skilled institutional delivery? A study in rural Mexico. Matern Child Health J. 2006;10(5):419–25.
Ergaz Z, Avgil M, Ornoy A. Intrauterine growth restriction—etiology and consequences: what do we know about the human situation and experimental animal models? Reprod Toxicol. 2005;20(3):301–22.
Orshal JM, Khalil RA. Gender, sex hormones, and vascular tone. Am J Physiol Regul Integr Comp Physiol. 2004;286(2):R233–49.
Zhao D, Zou L, Lei X, Zhang Y. Gender differences in infant mortality and neonatal morbidity in mixed-gender twins. Sci Rep. 2017;7(1):1–6.
Rahman KM, Sarkar P. Determinants of infant and child mortality in Bangladesh. Pak J Soc Sci. 2009;6(3):175–80.
Stanley WA, Huber LRB, Laditka SB, Racine EF. Association of type of birth attendant and place of delivery on infant mortality in sub-Saharan Africa. Afr Health Sci. 2016;16(1):1–9.
Pembe AB, Carlstedt A, Urassa DP, Lindmark G, Nyström L, Darj E. Quality of antenatal care in rural Tanzania: counselling on pregnancy danger signs. BMC Pregnancy Childbirth. 2010;10(1):35.
Lamichhane R, Zhao Y, Paudel S, Adewuyi EO. Factors associated with infant mortality in Nepal: a comparative analysis of Nepal demographic and health surveys (NDHS) 2006 and 2011. BMC Public Health. 2017;17(1):53.
Xie Rh, Gaudet L, Krewski D, Graham ID, Walker MC, Wen SW. Higher cesarean delivery rates are associated with higher infant mortality rates in industrialized countries. Birth. 2015;42(1):62–9.
Chaplin J, Kelly J, Kildea S. Maternal perceptions of breastfeeding difficulty after caesarean section with regional anaesthesia: A qualitative study. Women and Birth. 2016;29(2):144–52.
Gouchon S, Gregori D, Picotto A, Patrucco G, Nangeroni M, Di Giulio P. Skin-to-skin contact after cesarean delivery: an experimental study. Nurs Res. 2010;59(2):78–84.
Kleinman JC, Fowler MG, Kessel SS. Comparison of infant mortality among twins and singletons: United States 1960 and 1983. Am J Epidemiol. 1991;133(2):133–43.
Guo G, Grummer-Strawn LM. Child mortality among twins in less developed countries. Popul Stud. 1993;47(3):495–510.
Justesen A, Kunst A. Postneonatal and child mortality among twins in Southern and Eastern Africa. Int J Epidemiol. 2000;29(4):678–83.
Aber JL, Bennett NG, Conley DC, Li J. The effects of poverty on child health and development. Annu Rev Public Health. 1997;18(1):463–83.
Curtis SL, Diamond I, McDonald JW. Birth interval and family effects on postneonatal mortality in Brazil. Demography. 1993;30(1):33–43.
Whitworth A, Stephenson R. Birth spacing, sibling rivalry and child mortality in India. Soc Sci Med. 2002;55(12):2107–19.
Kozuki N, Lee AC, Silveira MF, Victora CG, Adair L, Humphrey J, Ntozini R, Black RE, Katz J. The associations of birth intervals with small-for-gestational-age, preterm, and neonatal and infant mortality: a meta-analysis. BMC Public Health. 2013;13(S3):S3.
Kozuki N, Walker N. Exploring the association between short/long preceding birth intervals and child mortality: using reference birth interval children of the same mother as comparison. BMC Public Health. 2013;13(S3):S6.
Sovio U, Dibden A, Koupil I. Social determinants of infant mortality in a historical Swedish cohort. Paediatr Perinat Epidemiol. 2012;26(5):408–20.
Lewit EM, Baker LS, Corman H, Shiono PH. The direct cost of low birth weight. Future Child. 1995;5(1):35–56.
Hack M, Klein NK, Taylor HG. Long-term developmental outcomes of low birth weight infants. Future Child. 1995;5(1):176–96.
Boulet SL, Salihu HM, Alexander GR. Mode of delivery and the survival of macrosomic infants in the United States, 1995–1999. Birth. 2006;33(4):278–83.
Acknowledgements
We greatly acknowledge MEASURE DHS for granting access to the East African DHS data sets.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
GAT, BLS, ABT, MGW and ZTT conceived the study. GAT, BLS, ABT, MGW and ZTT analyzed the data, drafted the manuscript, and reviewed the article. GAT, BLS, ABT, MGW and ZTT extensively reviewed the article. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study doesn’t involve the collection of information from subjects. Consent to participate is not applicable. Since the study is a secondary data analysis based on DHS data.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tesema, G.A., Seifu, B.L., Tessema, Z.T. et al. Incidence of infant mortality and its predictors in East Africa using Gompertz gamma shared frailty model. Arch Public Health 80, 195 (2022). https://doi.org/10.1186/s13690-022-00955-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13690-022-00955-7