
Abstract
Background
A considerable number of qualitative studies have been published in recent years on the issues that the quantitative studies have limitations on. This study aimed at performing a meta-synthesis on qualitative studies on Road Traffic Injuries (RTIs) with a scoping review approach.
Methods
This meta-synthesis study was conducted as a scoping review in 2019. The Arkesy and O’Malley framework was applied which has six steps of identifying the research question, identifying the relevant studies, selecting the studies, charting the data, data analysis and reporting the results, and consultation exercise. The required data were gathered by searching the relevant keywords in databases of PubMed, web of knowledge, Scopus, Cochrane Library, Science Direct, Google scholar, Sid, IranMedex. Extracted data were analyzed by the Content-Analysis method.
Results
Finally, 30 studies were included. Extracted data summarized in five main themes and 17 sub-themes. The main themes were: consequences (individual, family, social, financial), the needs of survivors (social support and healthcare), risk factors (general risk factors, risk factors for motorcyclists, risk factors for children and adolescents), barriers of prevention (general barriers, pre-hospital barriers, emergency, and hospital barriers), and prevention solutions (increasing safety, rules and regulations, education, increasing equipment, scientific solutions) of RTIs.
Conclusion
This study combined the methods of the scoping review and the meta-synthesis to mapping all qualitative studies on the RTIs, with this approach, this study provides extensive and practical information for policy-makers, managers, practitioners, and researchers in the field of RTIs. Also, by applying this approach, the gaps in the existing knowledge and areas in need of further research are identified.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Road Traffic Injuries (RTIs) are the main cause of morbidity and mortality in the world nowadays [1]. The biggest proportion of hospital emergency department admissions is comprised of those affected by the RTIs and these admissions result in an enormous amount of direct and indirect costs for both people and the government. So it consumes a considerable share of the country’s annual budget [2]. It is estimated that globally 1.35 million people lose their lives due to RTIs every year and 50 million people get injured [3]. Moreover, it is estimated that these numbers will increase by 65% in the future 20 years [4]. The estimations also show that for each death due to the RTIs, there are 16 cases of hospitalizations and 400 cases of outpatient visits or transient activity limitations [5].
Quantitative studies have been published on various aspects of the RTIs. Although the quantitative studies were brilliant in this area and have helped the prevention of the RTIs, they are faced with some limitations in some aspects. So the researchers used the qualitative methods besides the quantitative ones [6]. The qualitative studies have been the focus of researchers in the field of health sciences in recent years [7, 8]. Despite the successes of the quantitative researches in measurement, analysis, and use of knowledge, they have some limitations in measuring the subjects such as perception, attitude, experience, and feelings of the people. Thus the use of qualitative studies has been grown in fields such as social sciences and health service management [9].
Considering the characteristics of the qualitative studies, in recent years a significant number of these studies have been performed on some aspects of the RTIs that the quantitative studies were faced with serious limitations on those aspects [10, 11]. Summarization of the findings of these qualitative studies may produce some useful information for macro-level policymaking on the RTIs. Thus this study is performed with the aim of meta-synthesis of the qualitative studies on RTIs with the scoping review approach.
Methods
This was a meta-synthesis study performed as a scoping review in 2019 with the aim of the analysis of published qualitative studies on RTIs. The framework by Arkesy and O’Malley was used which is the first methodological framework to manage the scoping review studies. The framework is published in 2005 and includes six steps: identification of the research question, identification of the relevant studies, selection of the studies, data charting, data analysis and reporting the results, and consultation exercise [12].
-
Step one: Identification of the research question
The research question was what are the characteristics and results of the qualitative studies on RTIs. The question is specifically divided into the following:
-
What are the main approaches of the qualitative studies on RTIs?
-
What are the main methods of data collection in qualitative studies on RTIs?
-
What are the most important aspects of RTIs studied in qualitative studies and what are the results?
Inclusion and exclusion criteria: All qualitative studies on the RTIs from January 2000 to March 2019 were eligible to include in the analysis. The language was limited to English and Persian. Those studies on injuries of accidents other than road traffic accidents (such as sailing, aviation, railway), those studies that assessed the RTIs and other injuries at the same time, short communications, and conference abstracts were excluded.
-
Step two: Identification of the relevant studies
The required data were gathered by searching the keywords of road traffic injury, road traffic accidents, road traffic crashes, motorcycle accident, motorcycle crash, motorcycle injury, motor vehicle injury, motor vehicle crash, motor vehicle accident, qualitative, interview, phenomenology, focus group discussion, grounded theory at the databases of PubMed, web of knowledge, Scopus, Cochrane Library, Science Direct, Google scholar, Sid, IranMedex (Additional file 1: complete search strategy for PubMed databases). To assure the maximum coverage of the study identified these actions were made: some key journals were hand searched, after removing the irrelevant records the remaining papers were reference checked, they were also citation checked by using the Google Scholar citation, some experts were contacted, and the gray literature was searched through the European Association for Grey Literature Exploitation (EAGLE), the Health Care Management Information Consortium (HMIC), and the System for information on Grey Literature in Europe (SIGLE).
-
Step three: Study selection/screening
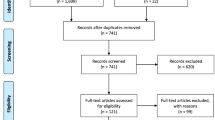
All works of the selection and screening of the papers were performed independently by two members of the research team. Cases of inconsistency between the two were resolved by discussion. Over 80% agreement was the cut of the agreement for the selection and screening of articles between the two researchers. Firstly, the titles of all papers were assessed and those irrelevant to the study purpose were removed. Then the abstracts and full-texts were assessed for eligibility according to inclusion and exclusion criteria. EndNote X5 software was used to handle these works and also to identify the duplications. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram [13] was used to report the findings (Fig. 1).

PRISMA chart, screening process of qualitative studies on Road Traffic Injuries (RTIs) published between2000 to 2019
Reporting quality assessment
After screening, the reporting quality of the studies was assessed by two researchers using the Critical Appraisal Skills Program (CASP) checklist. The checklist includes 10 items. The first two items are screening questions. The appraisal of the study would continue only if the answer to at least one of these two questions was yes. For the next eight questions the three options of Yes, Can’t tell, No were marked for which the scores of three, two, one were assigned respectively [14]. So the maximum score of each paper was 24 and the minimum was eight. The inconsistencies were resolved by discussion.
-
Step four: Categorization of the data
To extract the data, the data extraction form was developed in MS Word 2010. Data for three papers were extracted as a pilot. Then the form was revised. The intended data included: author(s), year, country, study purpose, participants, the approach of the study, data collection method, study findings (themes and sub-themes).
-
Step five: Conclusion, summarization, and reporting the results
The gathered data were analyzed by the content analysis method. Content-Analysis is a widespread method for the analysis of qualitative data through the identification, analysis, and reporting of the patterns (themes) within a text [15,16,17,18]. Coding the text was performed by two researchers independently. Steps of the analysis were: getting familiarized with data, identifying primary areas, putting the paper in the areas, reviewing the papers of each area to complete the findings, assuring the reliability of the work by comparing the results by the two coders.
-
Step six: Providing practical recommendations
After extracting and reporting the study results, based on the study findings and the opinions of the research team, practical recommendations were made in terms of research methodology and also for the policymakers and managers.
Results
Of the 4623 retrieved records, 1825 were duplicates. At the title and abstract screening, 2752 records were removed. The full-text review also resulted in the removal of 16 papers so finally, 30 papers were included in the synthesis (Fig. 1).
The characteristics of the included studies are shown in Table 1. They are conducted in 12 countries most of which (nine countries) are low-and-middle-income countries (LMICs). The total number of the participants of the included studies was 906 people. The interview was used in 25 studies, FGD in eight studies, and the nominal group in one study (four studies had used more than one method) as a data collection method. The approach of the study was not mentioned in 12 studies. Seven studies have used content analysis, six phenomenologies, and five grounded theory.
Extracted data were summarized into five main themes and 17 sub-themes by the content-analysis (Fig. 2).

Mapping the extracted results from qualitative studies on Road Traffic Injuries (RTIs) published between2000 to 2019
Consequences
The consequences of the RTIs were divided into four categories of individual, family, social, and financial consequences.
Individual consequences
One main individual consequence of the RTIs was the physical so that even if the individual survives at the accident, he/she will suffer from morbidity. Long-term pains, movement problems, and sleep problems were major examples of physical problems. Beyond the mortality and the morbidity, some mental problems also occur as a result of the RTIs such as feeling ashamed, being an encumbrance, and fear of the future.
Family consequences
Further to the individual consequences, the RTIs also have consequences on families. The major problems in this category were problems of caring for the injured people (skills, costs, the stamina of caring), change in roles of the family members such as the breadwinner role of the mother of children due to injury of the father), and cut or reduction of family income.
Social consequences
One main social consequence of the RTIs that was highly mentioned was the limitations of the social relations of the injured people. Moreover, the accidents due to the low safety of the vehicles and roads can result in distrust of the people in government actions.
Financial consequences
One of the most obvious consequences of RTIs is financial consequences. It includes damages to the vehicle, damages to road facilities, treatment and care costs of the injured people, costs of losing the productivity of the people in the society, paying the blood money, and other costs.
Needs of survivors
Every RTIs due to the mentioned consequences creates some needs in the injured individual and his/her family. One of these needs is the social needs of the injured people which include social support by the government, charities, family, and friends in terms of financial, mental, spiritual, and legal supports. Another need after an RTI is the need for healthcare which includes emergency care right after the accident, specialist and quality care at the hospital, rehabilitation care, and mental care.
Risk factors
The other main theme was the risk factors of the RTIs which had three sub-themes of general risk factors (five items), risk factors for motorcyclists (five items), risk factors for children and adolescents (four items). Table 2 shows the risk factors of the RTIs.
Barriers to prevention
The barriers to the prevention of the RTIs were in three categories of general barriers (five main and 13 sub-main), pre-hospital barriers (three main and 10 sub-main), emergency, and hospital barriers (two main and five sub-main). Table 3 shows the themes and sub-themes of the barriers to the prevention of the RTIs.
Solutions of prevention
Solutions for prevention of the RTIs and reduction of their consequences were categorized in five dimensions including increasing safety (three items), rules and regulations (four items), education (two items), increasing equipment (five items), and scientific solutions (two items). Table 4 shows these solutions.
Results of the quality appraisal of the included qualitative studies showed that the average quality score of them was 21.6 in the 8–24 range. One issue that did not receive sufficient attention in the studies was the ethical issues (Additional file 2).
Discussion
Of the 4623 retrieved papers, finally, 30 included in the study. The synthesis of the qualitative data resulted in five main themes and 17 sub-themes. The themes were consequences of the RTIs (individual, family, social, financial), needs (social support, healthcare), risk factors of the RTIs (five general risk factors, five risk factors of motorcyclists, four risk factors of children and adolescents), barriers of prevention of the RTIs (five general barriers, three pre-hospital barriers, two hospitals, and emergency barriers), and solutions of prevention of the RTIs (three items on increasing safety, four items on regulation, two items on education, five items on increasing equipment, and two items of scientific solutions).
Consequences of the RTIs
The RTIs not only cause physical and financial problems, but also cause some mental problems due to losing family members, feeling guilty, feeling ashamed, being an encumbrance, and fear of the future. The physical problems usually get better by healthcare or the person becomes adapted to the problems. But the mental problems such as long-term depressions bring more suffering for the person and have more severe consequences [49]. A meta-analysis by Wanli Lin and colleagues (2018) showed that the prevalence of Post-Traumatic Stress Disorder (PTSD) among 6804 victims of the RTIs was 22.2% [50]. Another meta-analysis by Dai et al. (2018) on 1532 children and adolescents injured in RTIs showed the prevalence of PTSD as 19.9% [51]. The study by Asuquo et al. in Nigeria (2017) showed that 63% of the victims of the RTIs became depressed [52]. Some other studies also indicated the high prevalence of mental problems among injured people in the RTIs [53,54,55,56,57]. Thus the mental problems of these people should be considered to provide appropriate care.
Another consequence of RTIs is financial issues. The high social and economic costs of the RTIs have challenged the policymakers of the countries [38, 58]. The economic costs of the RTIs include all costs of the RTIs and costs due to the RTIs [59]. It is estimated that the global costs of the RTIs be US $ 518 billion of which the US $ 65 billion is at the LMICs. It is also estimated that the costs of the RTIs at the low-income, middle-income, and high-income countries to be 1, 1.5, and 2% of the Gross Domestic Product (GDP) of that country, respectively [4]. According to the study by Eyni et al. (2014) which applied the willingness to pay (WTP) method found that the costs of the RTIs equal to 6.46% of the GDP of Iran [60]. A glance at the literature shows that several methods have been used to estimate the costs of the RTIs in recent years such as life insurance approach, court award, compensation method, implicit public sector valuation, gross output, Human Capital (HC), Willingness To Pay (WTP) [58, 61,62,63,64,65]. The systematic review by Azami-aghdash et al. (2018) showed that the HC method is more frequently used for this purpose [66].
Needs of survivors
One of the main needs of the victims of the RTIs is the need for social support because they cause the victims to be socially isolated [67, 68]. Numerous studies have shown that good social support to the survivors of the RTIs helps them to get better quickly and to overcome mental problems [69,70,71,72]. Family, friends, and some peer groups in the society can provide good social support for these people [73, 74]. The important point to consider in this regard is that to get the most possible impact, the support should be according to the conditions of the injured one and his/her injury.
Risk factors
One of the most important categories of the risk factors identified in this study is the risk factors of the motorcyclists. According to the National Highway Traffic Safety Administration (NHTSA), the risk of death of the motorcyclists is 34 times more than other vehicles. This number is eight times for severe injuries [75]. Most of the studies in this review also indicated a higher risk of injury to the motorcyclists [76,77,78,79,80]. It seems that the prevalence of using motorcycles has been grown so fast that the culture of its proper use has been lagged. So that people are not familiar with the culture of right and safe use of motorcycles [81]. Another reason for the higher rate of injuries of the motorcyclists might be its lower safety equipment compared to other vehicles [82, 83]. Moreover, compared to the other vehicles, most of the users of the motorcycles are the youth and peoples at this age due to the nature of the age and the more tendencies for excitement are at the higher risk of accident [84]. So, safer design of the motorcycles and more preventive laws along with the more measures to promote helmet seem necessary. Six risk factors were identified for the motorcyclists in this study. Quantitative studies have identified numerous risk factors for the motorcyclists [85,86,87,88,89]. Since in this study the risk factors are identified from qualitative studies, merging the findings of the qualitative and quantitative studies may provide a broader view on the issue.
As it is mentioned, the risk factors identified from qualitative papers in this study were general risk factors, specifically for motorcyclists and children and adolescents. Yet quantitative studies have identified specific risk factors for other groups of people such as the elderly, pedestrians, and bike riders. The literature shows that these groups are also vulnerable to RTIs [90,91,92,93,94,95,96] and should be investigated by qualitative studies.
Barriers to prevention
The study by Khorasani Zavareh et al. (2009) showed that there are several barriers to the prevention of the RTIs in Iran. The main theme of the study was the lack of a systemic approach to the prevention of the RTIs and the sub-themes were human resources, transportation systems, and organizational coordination [97]. A report by Hyder et al. (2013) assessed the barriers to prevention of the RTIs including knowledge, attitude, participation, management, capacity building, and infrastructure in five dimensions of government, health sector, society, academics, and private sector [98]. Alinia and colleagues (2015) studied the barriers of providing pre-hospital EMS care for the RTI victims and found 13 barriers in 4 main areas of barriers related to people, barriers related to the structure of the metropolises, barriers related to professions, and managerial barriers [35]. This study found few barriers in hospital and hospital emergency departments which might be mainly due to a limited number of studies in this regard. But other studies have shown that the hospital emergency medical care has a significant role in reducing the mortality and morbidity due to the RTIs [99, 100]. Thus it is suggested that more qualitative studies be conducted on the barriers to providing quality care for the RTI victims at the hospital emergency departments.
Solutions of prevention
The existence of a leading organization with sufficient authority and tools is one of the most important solutions for the prevention of the RTIs. Several organizations are involved in RTIs and their prevention, of which the main ones are the ministry of transportation, ministry of industry, ministry of health, traffic Police, forensic medicine organization, Central insurance organization, ministry of Justice, ministry of interior, the red crescent organization, and the EMS. At the countries that are successful in reducing the burden of the RTIs, usually, there is a leading organization that has the stewardship of the activities around the RTIs [101, 102]. For example, in Canada, the federal and provincial governments are the pioneer of road safety. The federal government has a commanding role in the transportation system and participates in the transportation system development by data collection and research. The police have the administrative role and develop safety plans with the help of the Judiciary [103]. The study by Soori et al. (2009) proposed the Traffic Police or the president as the steward leader in the prevention of the RTIs in Iran [104].
Another important solution that was emphasized in several studies is establishing an on-time and effective registration and reporting system. The experiences of the countries indicate that the health sector can play an effective role in designing and implementing the recording and reporting system of the RTIs [105,106,107,108]. In India, for example, the project named “Road Traffic Injury Surveillance Project” The project implemented in 2007 by the Indian Council of Medical Research Association (ICMRA), World Health Organization (WHO), ministry of health and family welfare after the many problems of the health sector data system. The main purpose of the project was to establish a care system in 25 major hospitals of India which then achieved considerable successes [109]. The system then merged with the Integrated Disease Surveillance Project (IDSP) by the government [110]. The other example is the case of Pakistan in which the health system of the country developed and implemented the RTIs’ care system in 2006. The goal of the system was to estimate the burden of the RTIs, to study the RTIs’ victims admitted to the hospital, and to provide solutions for reducing the RTIs. As a result of implementing this system, the attention to the RTIs was increased and the outputs of the system showed that the real number of the victims of the RTIs is higher than the statistics by the police [111]. The point to keep in mind is the cooperation of the health sector with other sectors and organizations in designing and implementing such systems. Since the RTIs are multilateral and many organizations are involved in it, the data of the RTIs should be integrated from all involved organizations.
Study limitation
Although with the best of our knowledge this is the first study of scoping review and meta-synthesis on qualitative studies on the RTIs, it has some limitations. The main limitation of this study was limiting the search of the literature to English and Persian languages because there might be some good studies in other languages that are not included in the synthesis. Subjective interpretation of the findings is another limitation of this study. Petticrew et al. (2013) noted that the results of meta-synthesis should be more interpreted by policy-makers and users [112]. But in the present study, this was not possible.
Conclusion
This study combined the methods of the scoping review and the meta-synthesis to mapping all qualitative studies on the RTIs to summarize the vast literature into five main themes and 17 sub-themes. The main themes found in this study were: consequences of the RTIs, needs, risk factors, barriers of prevention, and solutions for the prevention of the RTIs. With this approach, this study provides extensive and practical information for policy-makers, managers, practitioners, and researchers in the field of RTIs. Also, by applying this approach, the gaps in the existing knowledge and areas in need of further research are identified. However, this method is a new method and more studies are needed to become more mature with this method.
Future research
Based on the results of this study, the following topics are recommended for future qualitative studies:
-
➢ Psychological and social effects of traffic accidents.
-
➢ Policy-making, management, and organizational tasks of RTIs prevention.
-
➢ Qualitative studies to investigate RTIs prevention issues in high-risk and vulnerable groups (elderly, children, disabled people, etc.).
-
➢ Qualitative studies to further investigate the provision of high-quality health care services to traffic accident victims
-
➢ Carrying out qualitative studies on experiences, high-risk behaviors, and prevention of traffic accidents with the participation of drivers of public and heavy vehicles
-
➢ A qualitative study with policy-makers and senior managers on macro-level issues of traffic accident prevention (policies, rules, and regulations, culture, etc.).
-
➢ Application of qualitative studies in designing, implementing, and evaluating RTIs prevention interventions and policies.
Availability of data and materials
Supplementary files are available in the journal website.
Abbreviations
- RTIs:
-
Road Traffic Injuries
- EAGLE:
-
European Association for Grey Literature Exploitation
- HMIC:
-
Health Care Management Information Consortium
- SIGLE:
-
System for Information on Grey Literature in Europe
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- CASP:
-
Critical Appraisal Skills Program
- LMICs:
-
Low-and-middle income countries
- PTSD:
-
Post-Traumatic Stress Disorder
- GDP:
-
Gross Domestic Product
- HC:
-
Human Capital
- WTP:
-
Willingness To Pay
- NHTSA:
-
National Highway Traffic Safety Administration
- WHO:
-
World Health Organization
- IDSP:
-
Integrated Disease Surveillance Project
References
Azami-Aghdash S, Sadeghi-Bazargani H, Shabaninejad H, Abolghasem Gorji H. Injury epidemiology in Iran: a systematic review. J Inj Violence Res 2017;9(1):27–40.
Khorasani Zavareh D, Bohm K, Khankeh H, Talebian MT, Mohammadi R, Bigdeli M, et al. Why should being visible on the road? A challenge to prevent road traffic injuries among pedestrians in Iran. J Inj Violence Res. 2015;7(2):93–4. https://doi.org/10.5249/jivr.v7i2.490 Epub 2014 Mar 11.
Global status report on road safety 2018. Geneva: World Health Organization; 2018. Licence: CC BYNC-SA 3.0 IGO.
Peden M, Scurfield R, Sleet D, Hyder AA, Mathers C, Jarawan E, et al. World report on road traffic injury prevention. Geneva: World Health Organization; 2004.
Roy N, Murlidhar V, Chowdhury R, Patil SB, Supe PA, Vaishnav PD, et al. Where there are no emergency medical services-prehospital care for the injured in Mumbai, India. Prehosp Disaster Med. 2010;25(2):145–51.
Gooberman-Hill R, Fox R. What can qualitative approaches bring to trauma outcome research? Injury. 2011;42:321–3.
Al-Busaidi ZQ. Qualitative research and its uses in health care. Sultan Qaboos Univ Med J. 2008;8(1):11–9.
The PME. Qualitative research: understanding Patients’ needs and experiences. PLoS Med. 2007;4(8):e258.
Turato ER. Métodos qualitativos e quantitativos na área da saúde: definições, diferenças e seus objetos de pesquisa. Rev Saude Publica. 2005;39:507–14.
Azami-Aghdash S, Gorji HA, Shabaninejad H, Sadeghi-Bazargani H. Policy analysis of road traffic injury prevention in Iran. Electron Physician. 2017;9(1):3630–8.
Salter E, Stallard P. Young people's experience of emergency medical services as road traffic accident victims: a pilot qualitative study. J Child Health Care. 2004;8(4):301–11.
Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Intl J Soc Res Methodol. 2005;8:19–32.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Critical Appraisal Skills Programme. https://casp-uk.net/. Accessed Aug 2019.
Campos CJ. Content analysis: a qualitative data analysis tool in health care. Rev Bras Enferm. 2004;57(5):611–4.
Liamputtong P. Qualitative data analysis: conceptual and practical considerations. Health Promot J Austr. 2009;20(2):133–9.
Seers K. Qualitative data analysis. Evid Based Nurs. 2012;15(1):100352.
Smith J, Firth J. Qualitative data analysis: the framework approach. Nurse Res. 2011;18(2):52–62.
Doohan I, Saveman BI. Impact on life after a major bus crash--a qualitative study of survivors’ experiences. Scand J Caring Sci. 2014;28(1):155–63.
Pashaei Sabet F, Norouzi Tabrizi K, Khankeh H, Saadat S, Abedi H, Bastami A. Experiences of encountering physical trauma caused by traffic accidents: a qualitative study. Health Emergencies Disasters Q. 2016;1(4):187–92.
Yadav SK, Shrestha S. A study on posttraumatic experience of road traffic accident afflicted maxillofacial trauma patient at tertiary hospital. J Nat Sci, Biol Med. 2017;8(1):40–5.
Franzen C, Bjornstig U, Jansson L. Injured in traffic: experiences of care and rehabilitation. Accid Emerg Nurs. 2006;14(2):104–10.
Pashaei Sabet F, Norouzi Tabrizi K, Khankeh H, Fallahi KM. Rehabilitation needs of patients with physical disabilities due to traffic accidents for returning to the community: a qualitative study. Iran J Rehabil Res Nurs. 2014;1(1):74–87.
Ghorashi Z, Kazemi M, Sayyadi AR, Nikbakht NA. Experience of motorcycle accident victims: a qualitative study. J Rafsanjan Univ Med Scie. 2012;11(2):115–27.
Batool Z, Carsten O, Jopson A. Road safety issues in Pakistan: a case study of Lahore. Transp Plan Technol. 2012;35(1):31–48.
Christie N, Ward H, Kimberlee R, Towner E, Sleney J. Understanding high traffic injury risks for children in low socioeconomic areas: a qualitative study of parents’ views. Inj Prev. 2007;13(6):394–7.
Sanusi AA, Emmelin M. Commercial motorcycle drivers’ perceptions of risk and road safety in urban Nigeria: an explorative study. Int J Inj Control Saf Promot. 2015;22(4):328–39.
Tetali S, Lakshmi JK, Gupta S, Gururaj G, Wadhwaniya S, Hyder AA. Qualitative study to explore stakeholder perceptions related to road safety in Hyderabad, India. Injury. 2013;44(Suppl 4):S17–23.
Hashemiparast M, Montazeri A, Garmaroudi G, Nedjat S, Sadeghi R, Negarandeh R. Social reasons for young pedestrian’s risky road crossing behaviors: a qualitative study. Hayat. 2017;23(1):74–85.
Shams M, Shojaeezadeh D, Rashidian A, Majdzadeh S, Montazeri A. Taxi drivers’ views about risky driving behaviors in Tehran: a qualitative study. Payesh. 2010;9(4):391–401.
Zamani-Alavijeh F, Niknami S, Bazargan M, Mohamadi E, Montazeri A, Ghofranipour F, et al. Risk-taking behaviors among motorcyclists in middle east countries: a case of islamic republic of Iran. Traffic Inj Prev. 2010;11(1):25–34.
Khorasani-Zavareh D, Khankeh HR, Mohammadi R, Laflamme L, Bikmoradi A, Haglund BJ. Post-crash management of road traffic injury victims in Iran. Stakeholders’ views on current barriers and potential facilitators. BMC Emerg Med. 2009;9:8.
Haghparast-Bidgoli H, Khankeh H, Johansson E, Yarmohammadian MH, Hasselberg M. Exploring the provision of hospital trauma care for road traffic injury victims in Iran: a qualitative approach. J Inj Violence Res. 2013;5(1):28–37.
Haghparast-Bidgoli H, Hasselberg M, Khankeh H, Khorasani-Zavareh D, Johansson E. Barriers and facilitators to provide effective pre-hospital trauma care for road traffic injury victims in Iran: a grounded theory approach. BMC Emerg Med. 2010;10:20.
Alinia S, Khankeh H, Maddah SS, Negarandeh R. Barriers of pre-Hospital Services in Road Traffic Injuries in Tehran: the viewpoint of service providers. Int J Community Based Nurs Midwifery. 2015;3(4):272–82.
Razzaghi A, Pourrajabi A, Daneshi S. Obstacles and problems related to elderly pedestrians: a qualitative study. J Saf Promot Inj Prev. 2017;5(2):73–8.
Hashemiparast M, Negarandeh R, Montazeri A. How young pedestrians do explain their risky road crossing behaviors? A qualitative study in Iran. Health Promot Perspect. 2017;7(3):140–4.
Perez-Nunez R, Pelcastre-Villafuerte B, Hijar M, Avila-Burgos L, Celis A. A qualitative approach to the intangible cost of road traffic injuries. Int J Inj Control Saf Promot. 2012;19(1):69–79.
Noori Hekmat S, Dehnavie R, Jafari Sirizi M, Sharifi T. Health care financing for the victims of traffic accidents in Iran; Challenges and solutions. J Health Dev. 2015;4(3):219–34.
Bazeli J, Aryankhesal A, Khorasani-Zavareh D. Exploring the perception of aid organizations’ staff about factors affecting management of mass casualty traffic incidents in Iran: a grounded theory study. Electron Physician. 2017;9(7):4773–9.
Huicho L, Adam T, Rosales E, Paca-Palao A, Lopez L, Luna D, et al. Evaluation of interventions on road traffic injuries in Peru: a qualitative approach. BMC Public Health. 2012;12:71.
Ramos P, Diez E, Perez K, Rodriguez-Martos A, Brugal MT, Villalbi JR. Young people's perceptions of traffic injury risks, prevention and enforcement measures: a qualitative study. Accid Anal Prev. 2008;40(4):1313–9.
Soori H, Ainy E, Bazargan-Hejazi S. Opportunities, threats and barriers to enacting mandatory child car restraint laws in Iran. Int J Inj Control Saf Promot. 2015;22(4):314–9.
Trevino-Siller S, Hijar M, Mora G. Prioritisation of road traffic injury interventions: results of a participative research with stakeholders in Mexico. Int J Inj Control Saf Promot. 2011;18(3):219–25.
Ainy E, Soori H, Mahfozphoor S, Movahedinejad AA. Presenting a practical model for governmental political mapping on road traffic injuries in Iran in 2008: a qualitative study. JRSM Short Rep. 2011;2(10):79.
Salari H, Motevalian SA, Arab M, Esfandiari A, Akbari SA. Exploring measures to control road traffic injuries in Iran: key informants points of view. Iran J Public Health. 2017;46(5):671–6.
Patel A, Vissoci JRN, Hocker M, Molina E, Gil NM, Staton C. Qualitative evaluation of trauma delays in road traffic injury patients in Maringa, Brazil. BMC Health Serv Res. 2017;17(1):804.
Teye-Kwadjo E. Risk factors for road transport–related injury among pedestrians in rural Ghana: implications for road safety education. Health Educ J. 2017;76(7):880–90.
Wang CH, Tsay SL, Bond AE. Post-traumatic stress disorder, depression, anxiety and quality of life in patients with traffic-related injuries. J Adv Nurs. 2005;52(1):22–30.
Lin W, Gong L, Xia M, Dai W. Prevalence of posttraumatic stress disorder among road traffic accident survivors: A PRISMA-compliant meta-analysis. Medicine. 2018;97(3):e9693–e.
Dai W, Liu A, Kaminga AC, Deng J, Lai Z, Wen SW. Prevalence of Posttraumatic Stress Disorder among Children and Adolescents following Road Traffic Accidents: A Meta-Analysis. Can J Psychiatry. 2018;63(12):798–808.
Asuquo JE, Edet BE, Abang IE, Essien EA, Osakwe OG, Aigbomain EJ, et al. Depression and posttraumatic stress disorder among road traffic accident victims managed in a tertiary hospital in southern Nigeria. Niger J Clin Pract. 2017;20(2):170–5.
Brand S, Otte D, Petri M, Decker S, Stubig T, Krettek C, et al. Incidence of posttraumatic stress disorder after traffic accidents in Germany. Int J Emerg Mental Health. 2014;16(1):233–6.
Heron-Delaney M, Kenardy J, Charlton E, Matsuoka Y. A systematic review of predictors of posttraumatic stress disorder (PTSD) for adult road traffic crash survivors. Injury. 2013;44(11):1413–22.
Mairean C. Driving cognitions, rumination, and posttraumatic stress disorder in road traffic accidents survivors. Clin Psychol Psychother. 2019;26(1):47–54.
Seidler A, Hegewald J, Seidler AL, Schubert M, Wagner M, Droge P, et al. Association between aircraft, road and railway traffic noise and depression in a large case-control study based on secondary data. Environ Res. 2017;152:263–71.
Wu F, Meng WY, Hao CZ, Zhu LL, Chen DQ, Lin LY, et al. Analysis of posttraumatic stress disorder in children with road traffic injury in Wenzhou, China. Traffic Inj Prev. 2016;17(2):159–63.
Olukoga A. Cost analysis of road traffic crashes in South Africa. Inj Control Saf Promot. 2004;11(1):59–62.
Elvik R, Amundsen AH. Improving road safety in Sweden. Main Report 490. Oslo: Institute of Transport Economics; 2000.
Ainy E, Soori H, Ganjali M, Le H, Baghfalaki T. Estimating cost of road traffic injuries in Iran using willingness to pay (WTP) method. PloS one. 2014;9(12):e112721.
Ainy E, Soori H. Review on road traffic injuries cost calculation methods. J Saf Prom Inj Prev. 2014;1(4):236–44.
Elvik R. Analysis of official economic valuations of traffic accident fatalities in 20 motorized countries. Accid Anal Prev. 1995;27(2):237–47.
Garcia-Altes A, Perez K. The economic cost of road traffic crashes in an urban setting. Inj Prev. 2007;13(1):65–8.
Parkinson F, Kent SJ, Aldous C, Oosthuizen G, Clarke D. The hospital cost of road traffic accidents at a south African regional trauma Centre: a micro-costing study. Injury. 2014;45(1):342–5.
Reddy GM, Negandhi H, Singh D, Singh AJ. Extent and determinants of cost of road traffic injuries in an Indian city. Indian J Med Sci. 2009;63(12):549–56.
Saber Azami-Aghdash S, Homayoun Sadeghi-Bazarghani H, Mahdiyeh Heydari M, Ramin Rezapour R, Naser DN. Economic burden of road traffic injuries in Iran: a mini-systematic review. J Clin Res Gov. 2016;5(2):1–6.
Adellund Holt K, Jensen PT, Gilsa Hansen D, Elklit A, Mogensen O. Rehabilitation of women with gynaecological cancer: the association between adult attachment, post-traumatic stress disorder and depression. Psycho-oncology. 2016;25(6):691–8.
Másilková M. Health and social consequences of road traffic accidents. Kontakt. 2017;19(1):e43–e7.
Schumm JA, Briggs-Phillips M, Hobfoll SE. Cumulative interpersonal traumas and social support as risk and resiliency factors in predicting PTSD and depression among inner-city women. J Trauma Stress. 2006;19(6):825–36.
Chossegros L, Hours M, Charnay P, Bernard M, Fort E, Boisson D, et al. Predictive factors of chronic post-traumatic stress disorder 6 months after a road traffic accident. Accid Anal Prev. 2011;43(1):471–7.
Holeva V, Tarrier N, Wells A. Prevalence and predictors of acute stress disorder and PTSD following road traffic accidents: thought control strategies and social support. Behav Ther. 2001;32(1):65–83.
Nijs J, Inghelbrecht E, Daenen L, Hachimi-Idrissi S, Hens L, Willems B, et al. Long-term functioning following whiplash injury: the role of social support and personality traits. Clin Rheumatol. 2011;30(7):927–35.
Valizadeh S, Dadkhah B, Mohammadi E, Hassankhani H. The perception of trauma patients from social support in adjustment to lower-limb amputation: a qualitative study. Indian J Palliat Care. 2014;20(3):229–38.
Prang K-H, Berecki-Gisolf J, Newnam S. Recovery from musculoskeletal injury: the role of social support following a transport accident. Health Qual Life Outcomes. 2015;13(1):97.
Administration NHTS. Traffic Safety Facts 2007: Motorcycles. Washington DC: National Highway Traffic Safety Administration; 2007.
Brazinova A, Majdan M. Road traffic mortality in the Slovak Republic in 1996-2014. Traffic Inj Prev. 2016;18:1–7.
Nepal S, Gupta S, Wong EG, Gurung S, Swaroop M, Kushner AL, et al. Burden of road traffic injuries in Nepal: results of a countrywide population-based survey. Lancet. 2015;27(385):60802–9.
Celine T, Antony J. A study on injuries sustained in road traffic accidents at a tertiary care level. Int J Env Health Eng. 2014;3:23.
Madubueze CC, Chukwu CO, Omoke NI, Oyakhilome OP, Ozo C. Road traffic injuries as seen in a Nigerian teaching hospital. Int Orthop. 2011;35(5):743–6.
Yongchaitrakul T, Juntakarn C, Prasartritha T. Socioeconomic inequality and road traffic accidents in Thailand: comparing cases treated in government hospitals inside and outside of Bangkok. Southeast Asian J Trop Med Public Health. 2012;43(3):785–94.
Shahla A, Charesaz S. Injuries resulting from motorcycle- induced trauma during two years in Shahid Motahari Clinical Center of URMIA. IJFM. 2006;12(2):79–83.
Williams VH, McLaughlin SB. A survey of motorcyclists: data for research design and instrumentation; 2013.
Haworth NL, Rowden PJ, Wishart DE, Buckley L, Greig K, Watson BC. Motorcycle rider safety project summary report; 2012.
Araghi E, Vahedian M. Study on Suceptible and damages from motorcycle accidents in Mashhad in 2005. Ofoghe-E-Danesh. 2007;13(1):34–9.
Lin MR, Kraus JF. A review of risk factors and patterns of motorcycle injuries. Accid Anal Prev. 2009;41(4):710–22.
Wu D, Hours M, Martin JL. Risk factors for motorcycle loss-of-control crashes. Traffic Inj Prev. 2018;19(4):433–9.
Naqvi HM, Tiwari G. Factors contributing to motorcycle fatal crashes on National Highways in India. Transportation Res Procedia. 2017;25:2084–97.
Sadeghi-Bazargani H, Samadirad B, Hosseinpour-Feizi H. Epidemiology of traffic fatalities among motorcycle users in East Azerbaijan, Iran. BioMed Res Int. 2018;2018:10.
Abedi L, Sadeghi-Bazargani H. Epidemiological patterns and risk factors of motorcycle injuries in Iran and eastern Mediterranean region countries: a systematic review. Int J Inj Control Saf Promot. 2017;24(2):263–70.
Azami-Aghdash S, Aghaei MH, Sadeghi-Bazarghani H. Epidemiology of road traffic injuries among elderly people; a systematic review and meta-analysis. Bull Emerg Trauma. 2018;6(4):279–91.
Santos AMRd, Rodrigues RAP, Diniz MA. Trauma by traffic accident in elderly people: risk factors and consequences. Texto & Contexto-Enfermagem. 2017;26(2):e4220015.
Hasani J, Khorshidi A, Erfanpoor S, Nazparvar B, Hashemi NS. Comparison of risk factors for pedestrian fatality in urban and suburban traffic accidents. Arch Trauma Res. 2018;7(2):39–44.
Stoker P, Garfinkel-Castro A, Khayesi M, Odero W, Mwangi MN, Peden M, et al. Pedestrian safety and the built environment: a review of the risk factors. J Plan Lit. 2015;30(4):377–92.
Lin Z-B, Ji Y-H, Xiao Q-Y, Luo L-B, Li L-P, Choi B. Risk factors of bicycle traffic injury among middle school students in chaoshan rural areas of china. Int J Equity Health. 2017;16(1):28.
Tin Tin S, Woodward A, Ameratunga S. Incidence, risk, and protective factors of bicycle crashes: findings from a prospective cohort study in New Zealand. Prev Med. 2013;57(3):152–61.
Embree TE, Romanow NTR, Djerboua MS, Morgunov NJ, Bourdeaux JJ, Hagel BE. Risk factors for bicycling injuries in children and adolescents: a systematic review. Pediatrics. 2016;138(5):e20160282.
Khorasani-Zavareh D, Mohammadi R, Khankeh HR, Laflamme L, Bikmoradi A, Haglund BJ. The requirements and challenges in preventing of road traffic injury in Iran. A qualitative study. BMC Public Health. 2009;9(486):1471–2458.
Hyder AA, Puvanachandra P, Allen KA. Road traffic injury and trauma care: Innovations for policy (Road Trip). WISH Road Traffic Injury Report. 2013:[52]. Available from: https://www.imperial.ac.uk/media/imperial-college/institute-of-global-health-innovation/public/27425_WISH_Road_Injuries_Report_web.pdf. [cited 2015Apr 15].
Organization WH. Strengthening care for the injured: success stories and lessons learned from around the world. 2010.
Organization WH. Guidelines for essential trauma care. 2004.
Stevenson M, Thompson J. On the road to prevention: road injury and health promotion. Health Promot J Austr. 2014;25(1):4–7.
Al Turki YA. How can Saudi Arabia use the decade of action for road safety to catalyse road traffic injury prevention policy and interventions? Int J Inj Control Saf Promot. 2014;21(4):397–402.
Johnson M, Howard E. Road Safety Vision 2010 Mid-Term Review. Canadian Traffic Safety Institute. Prepared for the Canadian Council of Motor Transport Administrators. 2007.
Soori H, Movahedinejad A, Mahfozphoor S, Movahedi M, Rezazadeh Azari M, Hatamabadi H, et al. A practical model of political mapping in road traffic injury in Iran in 2008. Hakim. 2009;12(3):1–9.
Ma S, Li Q, Zhou M, Duan L, Bishai D. Road traffic injury in China: a review of national data sources. Traffic Inj Prev. 2012;13(sup1):57–63.
Ward E, McCartney T, Arscott-Mills S, Gordon N, Grant A, McDonald AH, et al. The Jamaica injury surveillance system: a profile of the intentional and unintentional injuries in Jamaican hospitals. West Indian Med J. 2010;59(1):7–13.
Rojas Medina Y, Espitia-Hardeman V, Dellinger AM, Loayza M, Leiva R, Cisneros G. A road traffic injury surveillance system using combined data sources in Peru. Rev Panam Salud Publica. 2011;29(3):191–7.
Hatamabadi HR, Vafaee R, Haddadi M, Abdalvand A, Soori H. Necessity of an integrated road traffic injuries surveillance system: a community-based study. Traffic Inj Prev. 2011;12(4):358–62.
Gururaj G, Sateesh V L, Rayan AB, Roy AC, Amarnath, Ashok J, et al. Bengaluru Injury surveillance collaborators group. National Institute of Mental Health and Neuro Sciences, Publication No. 68, Bengaluru 2008; Availablefrom: http://www.nimhans.kar.nic.in/epidemiology/bisp/sr1.pdf. [Last cited on 2012 May 22].
Integrated Disease Surveillance Project. Medical Officers Manual. May 2005. Government of India, Directorate General of Health Services, Ministry of Health and Family Welfare. Available from: http://www.nvbdcpchd.gov.in/reporting%20 formats/MoUManual.pdf. [Last cited on 2012 May 23].
Razzak JA, Shamim MS, Mehmood A, Hussain SA, Ali MS, Jooma R. A successful model of road traffic injury surveillance in a developing country: process and lessons learnt. BMC Public Health. 2012;12(357):1471–2458.
Petticrew M, Rehfuess E, Noyes J, Higgins JP, Mayhew A, Pantoja T, et al. Synthesizing evidence on complex interventions: how meta-analytical, qualitative, and mixed-method approaches can contribute. J Clin Epidemiol. 2013;66(11):1230–43.
Acknowledgments
I would like to express my very great appreciation to my best friend Naser derakhshani for his valuable help during the selection and screening of the papers, assessing the reporting quality of the studies and Coding. His willingness to give his time so generously has been very much appreciated”.
Consent to participate
Not applicable.
Funding
This study was supported by the Research Center for Evidence-Based Medicine (RCEBM), Tabriz University of Medical Sciences. Grant no IR.TBZMED.VCR.REC.1397.455. However, the University played no roles in study design, data collection, analysis, writing or submitting to a publication.
Author information
Authors and Affiliations
Contributions
SA.A designed the project, collected data, analyzed the data, drafted the first version of the manuscript and revised the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
The study was approved by the Ethics Committees of the Institute of Tabriz University of Medical Sciences (IR.TBZMED.VCR.REC.1397.455).
Consent for publication
Not applicable.
Competing interests
The authors declare that there is no conflict of interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Complete search strategy in PubMed databases for identifying the qualitative studies on Road Traffic Injuries (RTIs) published between2000 to 2019.
Additional file 2.
Results of the quality appraisal of qualitative studies on Road Traffic Injuries (RTIs) published between2000 to 2019.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Azami-Aghdash, S. Meta-synthesis of qualitative evidence in road traffic injury prevention: a scoping review of qualitative studies (2000 to 2019). Arch Public Health 78, 110 (2020). https://doi.org/10.1186/s13690-020-00493-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13690-020-00493-0