
Abstract
Background
The COVID-19 pandemic has caused a large mortality and morbidity burden globally. For individuals, a strong immune response is the most effective means to block SARS-CoV-2 infection. To inform clinical case management of COVID-19, development of improved vaccines, and public health policy, a better understanding of antibody response dynamics and duration following SARS-CoV-2 infection and after vaccination is imperatively needed.
Methods
We systematically analyzed antibody response rates in naturally infected COVID-19 patients and vaccinated individuals. Specifically, we searched all published and pre-published literature between 1 December 2019 and 31 July 2023 using MeSH terms and “all field” terms comprising “COVID-19” or “SARS-CoV-2,” and “antibody response” or “immunity response” or “humoral immune.” We included experimental and observational studies that provided antibody positivity rates following natural COVID-19 infection or vaccination. A total of 44 studies reporting antibody positivity rate changes over time were included.
Results
The meta-analysis showed that within the first week after COVID-19 symptom onset/diagnosis or vaccination, antibody response rates in vaccinated individuals were lower than those in infected patients (p < 0.01), but no significant difference was observed from the second week to the sixth month. IgG, IgA, and IgM positivity rates increased during the first 3 weeks; thereafter, IgG positivity rates were maintained at a relatively high level, while the IgM seroconversion rate dropped.
Conclusions
Antibody production following vaccination might not occur as quickly or strongly as after natural infection, and the IgM antibody response was less persistent than the IgG response.
Similar content being viewed by others


Introduction
Coronavirus disease 2019 (COVID-19), which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has exacted a massive global burden in terms of mortality and morbidity. As of 5 September 2023, there have been more than 695 million confirmed cases and nearly seven million deaths worldwide [1]. SARS-COV-2-infected individuals often suffer respiratory infections and may develop severe pneumonia, which can subsequently lead to multiple organ failure and death [2]. Although some antiviral medicines have been approved for the treatment of COVID-19 [3, 4], the natural immune response plays a vital role in patient recovery and in prevention of symptomatic disease [5].
SARS-CoV-2 is a member of the coronavirus family of viruses, which are transmitted mainly through respiratory droplets [6]. The mechanisms of SARS-CoV-2 infection and immunity depend on its simple biological structure, which consists of the hereditary material RNA with a nucleocapsid (N) protein, surrounded by an envelope [7]. The virus’s important structural proteins include the spike (S), envelope (E), and membrane (M) proteins [7, 8]. The S protein has two functional subunits, S1 and S2 [8]. SARS-CoV-2 utilizes the receptor-binding domain (RBD) on the S1 protein to bind to the angiotensin-converting enzyme 2 (ACE2) in infected individuals’ bodies, allowing it to enter host cells [7, 9, 10].
The term “immune response” refers to the body’s defenses against foreign components or mutated self-components. A significant aspect of human immunity involves the antibody response, referring to the secretion of antibodies that can bind to specific pathogen antigens, thereby preventing those pathogens from entering host cells [5]. Five different types of immunoglobulins—IgG, IgA, IgM, IgE, and IgD—work in different parts of the body, serving as antibodies. If a protein on a given pathogen can trigger an antibody response, that protein is considered immunogenic. For SARS-CoV-2, the RBD is highly immunogenic [11], and the S protein and N protein are also main immunogens [8, 12]. Antibodies are categorized as neutralizing or non-neutralizing depending on whether they can inhibit pathogen infectivity [13]. Neutralizing antibodies directly prevent infection by blocking interactions between pathogens and host-cell receptors [13]. With respect to SARS-CoV-2 infection, neutralizing activity has been reported in the immune system’s anti-RBD and anti-S responses [14].
Individual positivity for and levels of antibodies serve as good indicators for doctors and researchers who wish to study SARS-CoV-2 immunity, assess patient prognoses, and evaluate vaccine effectiveness. In most patients, SARS-CoV-2 triggers a detectable antibody response in the early phase of infection [15]. However, the protective capacity of the generated antibodies is not yet fully understood. Furthermore, some studies show that a proportion of SARS-CoV-2-positive individuals may be seronegative for antibodies [16,17,18].
Vaccination is one of the most effective public health tools for combatting COVID-19 and other infectious diseases [19]. As of 30 March 2023, a total of 183 COVID-19 vaccines had either been approved for use or were under clinical development [20], and additional vaccine candidates were in preclinical development [21]. Vaccination works by triggering the body’s immune response, and antibody response rates are good indicators to evaluate vaccine efficacy. For COVID-19, some studies have shown that the triggered antibody response lasts at least 3 months following vaccination [22]. However, other studies have indicated that the seroconversion rates for special immunoglobulins descend after a period, suggesting that vaccination-induced immunity is transient [5, 23].
A comprehensive understanding of the differences between artificial immunity and natural immunity would greatly contribute to the development of future vaccine products and vaccination programs. However, to date, few systematic reviews have been published to summarize existing knowledge of both vaccination-induced antibody responses and natural antibody responses for SARS-CoV-2. To fill this gap, we conducted a systematic review and meta-analysis to assess seroconversion rates over time under the natural antibody response (for both symptomatic and asymptomatic patients) and under the vaccination-induced antibody response.
Methods
Selection criteria
A pre-established protocol for this review is shown in Appendix File S2. We included experimental and observational studies that provide antibody positivity rates after natural COVID-19 infection or vaccination. Individuals in eligible studies were either qRT-PCR-diagnosed COVID-19 patients (including both symptomatic and asymptomatic cases) or vaccine recipients without documented past COVID-19 infection, were adults (aged 18 years or older), and had undergone serum antibody testing (for the neutralizing antibody, IgG, IgM, IgA, or total antibody) with at least 21 days’ follow-up. The main outcome was the seroconversion rate after a specific number of days following symptom onset/diagnosis, or after vaccination. The seroconversion rate was defined as the proportion of COVID-19 antibody seropositive participants to the total number of people tested. This study does not limit the types of antibodies detected, and studies reporting results for any specific antibody (the neutralizing antibody, IgG, IgM, IgA) or total antibody were considered for inclusion. Detection methods and timing of assessment were not restricted as well.
The exclusion criteria were the following: (1) We excluded reviews, comments, letters, patents, editorials, case reports, animal studies, conference abstracts, and studies of ten or fewer subjects. (2) We excluded articles focused on comparison of antibody testing techniques. (3) We excluded research conducted exclusively on special populations (i.e., studies in which all subjects either suffered the same comorbid disease such as HIV or diabetes, were healthcare workers, or were convalescent plasma donors) because the antibody response in these subjects may differ from the response in the general population. (4) We excluded studies to avoid population overlap of study subjects.
Search strategy
We systematically searched PubMed, Web of Science, Embase, MEDLINE, medRxiv, and bioRxiv to identify all published and pre-publication studies with specified search terms between 1 December 2019 and 31 July 2023. Search terms included MeSH terms and “all field” terms comprising “COVID-19” or “SARS-CoV-2” and “antibody response” or “immunity response” or “humoral immune” (the detailed search terms for each database are shown in Appendix File S1). The reference lists of identified studies were also searched manually. The search was restricted to English language publications.
Study selection
Two reviewers (QZ and LJ) independently screened each study’s title and abstract and examined full texts to assess article eligibility. Disagreement was resolved through discussion with a senior author (SC). This review has not been registered previously.
Data extraction
The data extraction form used in this review was adapted from Cochrane’s data collecting form [24] and was shown in Appendix File S3. For the selected studies, we mainly collected the following information: author, publication year, region, sample size, sample mean or median age, gender composition, comorbidities, antibody testing method, antibody type, subject infection or vaccination status (including vaccine type and dose number), and median number of days to follow-up. To obtain the main outcome, we collected the number of seropositive participants, the total number of people tested, and the specific number of days following symptom onset/diagnosis, or after vaccination. Days following symptom onset/diagnosis/vaccination were divided into the following ranges: 0–7 days, 8–14 days, 15–21 days, 22 days–1 month, 1–2 months, 2–3 months, 3–6 months, and over 6 months. If the follow-up times reported in the article did not match these categories, we would try to obtain the original data and reclassify the serum results.
Quality assessment
Since most of the included studies were observational or non-randomized experimental studies, the MINORS score (methodological index for non-randomized studies) was utilized, with an ideal score of 16 for non-comparative studies and 24 for comparative studies [25]. In this review, for non-comparative studies, a score of ≤ 10 would be considered poor quality, 11–14 as moderate quality, and 15–16 as good quality. For comparative studies, we considered a high-quality study to have ≥ 23 points and a low-quality study to have ≤ 16 points. As for the randomized studies, Risk of Bias 1 (ROB 1) tool was used to assess quality through the RevMan software version 5.3 [26].
Heterogeneity
Between-study heterogeneity was assessed by the Q test, and the I2 statistic was calculated, with values of ≤ 50%, 50–75%, and > 75% indicating low, moderate, and high heterogeneity, respectively [27].
Data analysis
Since the main purpose of the study is to explore the changes and differences in serum positivity rates, we used proportional meta-analysis as the statistical method for data analysis. Proportional meta-analysis is a statistical technique used to analyze and combine the results from multiple studies that report proportions or rates of a particular event or characteristic, like incidence or prevalence of disease [28, 29]. In this study, the proportion of interest is COVID-19 antibody serum positivity rate, which is defined as the number of seropositive participants divided by the total number of people tested. Studies were combined in meta-analyses using the random effect model because of substantial heterogeneity among studies [30]. For each analysis, we considered p values < 0.01 to be statistically significant (two-tailed). All analyses were performed using R software version 4.1.2 [31].
Subgroup and sensitivity analysis
To compare the antibody response between SARS-CoV-2-infected individuals and vaccinees, a subgroup analysis was performed. We also conducted a subgroup analysis by antibody type (IgG, IgA, IgM, or neutralizing antibody) to further assess sources of heterogeneity.
To evaluate the robustness of our findings, a sensitivity analysis was performed by systematically excluding each study one at a time.
Publication bias
In the assessment of publication bias, we employed funnel plots to visually inspect the asymmetry in the distribution of effect sizes. Furthermore, Egger’s regression test was conducted to quantitatively assess the presence of publication bias [32].
Results
Characteristics of the studies
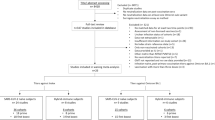
Of 15,656 studies from PubMed, 25,135 studies from Web of Science, 2469 studies from Ovid (containing Embase and MEDLINE), and 14,550 studies from bioRxiv and medRxiv, 418 studies were assessed for eligibility. After exclusion of articles according to different criteria, 44 studies were included in the final meta-analysis (Fig. 1). There are 40 observational studies in total, including 3 retrospective studies and 37 prospective studies (29 longitudinal studies, 2 cross-sectional studies, and 6 cohort studies). There are 4 experimental studies including 3 non-randomized studies and 1 randomized controlled trial.

PRISMA flow chart of the selection procedure [33]
Among these 44 included studies, 12 studies comprising a total of 43,664 subjects investigated antibody responses after vaccination with various types of COVID-19 vaccine (BNT162b2 [34,35,36,37], CoronaVac [23, 36, 38,39,40], ChAdOx1 [35,36,37], BBIBP-CorV [39, 41, 42], and mRNA-1237 [37]). Thirty-two studies comprising 9983 patients reported on antibody responses after infection. Median follow-up time was longer than 1 month for most studies, and the most common detection method were chemiluminescent immunoassay (50.0%) or enzyme-linked (43.2%). Basic information about the included studies is shown in Table 1 and the detailed demographic information is presented in Table S1.
IgG response rates by vaccination and infection
This subgroup analysis was performed to compare the antibody response between SARS-CoV-2-infected individuals and vaccinees. Twenty-eight studies comprising 10,878 subjects reported on the IgG antibody response in the first week following vaccination or COVID-19 symptom onset/diagnosis. The difference in antibody response between the vaccination group and the infection group was statistically significant (p < 0.01). In 7 studies of vaccinated subjects, 348 out of 6765 vaccinees showed a detectable IgG antibody response, and the pooled response rate was 0.14 (95% confidence interval [CI]: 0.00–0.32) with high heterogeneity (I2 = 98%). In 21 studies of naturally infected individuals, 1388 out of 4113 patients showed a detectable IgG antibody response, and the pooled response was 0.46 (95% CI: 0.34–0.57) with high heterogeneity (I2 = 100%). More details are given in Fig. 2. The results of this meta-analysis did not exhibit any statistically significant changes when systematically excluding each study one at a time and thus further reinforces the validity of our findings (Fig. S15).

Forest plot of pooled IgG response rates during days 0–7 across vaccination and infection groups. Events: number of participants with detectable IgG antibody levels. Blue dashed line: pooled rate for vaccination group; red dashed line: pooled rate for infection group. The proportion of IgG-positive subjects is higher in the infection group than in the vaccination group (p < 0.01)
We further conducted subgroup analyses by time intervals of 0–7 days, 8–14 days, 15–21 days, 22 days–1 month, 1–2 months, 2–3 months, 3–6 months, and over 6 months. The stratified results are summarized in Fig. 3 (detailed forest plots for each subgroup by the time interval can be found in Figs. S1–S7 in the Appendix). Among the vaccination group, the pooled antibody response rates for the eight time intervals were 0.14, 0.44, 0.70, 0.78, 0.92, 0.88, 0.93, and 0.22, respectively; among the infection group, the pooled rates for the eight time intervals were 0.46, 0.64, 0.86, 0.94, 0.94, 0.92, 0.81, and 0.79, respectively. For both the infection and vaccination groups, the pooled IgG response rates were relatively low during the first week but increased later. The difference between the infection group and vaccination group was significant during the first week (p < 0.01), but any between-group differences were not significant from the second week to the sixth month (all p values > 0.01). However, after 6 months, the pooled IgG response rate of the vaccination group declined dramatically, and the difference between the infection group and the vaccination group was once again significant (p < 0.01). Comparing both the variables “Events” (number of individuals with positive serum) and “Total” (number of individuals tested), sizes of the between group differences were estimated and 95% confidence intervals were calculated using R package “metafor” [76], as shown in Fig. 4.

Pooled IgG antibody response rates across the vaccination group and infection group. ***: p < 0.01; NS: not significant

Between-group differences of the pooled IgG antibody response rates. ***: p < 0.01; NS: not significant
Antibody response rates by antibody type
We then performed a subgroup analysis by antibody type (IgG, IgA, IgM, neutralizing antibody, and total antibody). Thirty studies comprising 16,138 subjects assessed antibody response rates 0–7 days following symptom onset or vaccination. No significant subgroup difference was identified for any antibody type (p = 0.97). For IgG, 1727 out of 10,878 subjects in 28 studies had detectable antibody levels, with a pooled response of 0.37 (95% CI: 0.26–0.48) and high heterogeneity (I2 = 100%). For IgM, 1304 out of 4299 subjects in 21 studies had detectable antibody levels, with a pooled response of 0.32 (95% CI: 0.23–0.41) and high heterogeneity (I2 = 98%). For IgA, 156 out of 617 subjects had detectable antibody levels, with a pooled response of 0.35 (95% CI: 0.19–0.52) and high heterogeneity (I2 = 98%). Finally, in the five studies that measured neutralizing antibody responses, 46 out of 143 subjects had detectable antibody levels, with a pooled response of 0.33 (95% CI: 0.06–0.60) and high heterogeneity (I2 = 97%). More detailed results can be found in the forest plot in Fig. 5. After excluding each study individually, the results of the meta-analysis remained stable, indicating the robustness and reliability of our study (Fig. S16).

Forest plot of pooled antibody response rates 0–7 days following infection or vaccination by antibody type. Events: number of participants with detectable antibody levels. The differences in proportion of positive subjects by antibody type are non-significant (p = 0.97)
For the antibody positivity rates at 8–14 days, 15–21 days, 22 days–1 month, 1–2 months, 2–3 months, 3–6 months, and after 6 months, the corresponding forest plots are provided in Figs. S8–S14 in the Appendix. The overall results are shown in Fig. 6. The pooled antibody response rates for IgG, IgM, IgA, neutralizing antibody, and total antibody increased from 0.37, 0.32, 0.35, 0.33, and 0.36, to 0.87, 0.63, 0.73, 0.83, and 0.92, respectively, during the first month. In the first week, between-group differences with respect to pooled antibody response rates were insignificant for all antibody types (p = 0.97). However, for follow-up during the second week and later, the between-group differences were significant (all p values < 0.01). The positivity rate for IgM dropped rapidly starting in the third month, with results of a hypothesis test indicating that this rate was significantly different from the positivity rate for IgG from this point onward (all p values < 0.01).

Pooled antibody response rates by antibody type. ***: p < 0.01; NS: not significant
Publication bias
The results of Egger’s regression test indicate that there is no significant evidence for the existence of publication bias (all p values > 0.01, Fig. S17).
Discussion
This meta-analysis considered data from 44 studies of antibody response following COVID-19 vaccination or natural infection with SARS-CoV-2 (including both symptomatic and asymptomatic infection). To our knowledge, it is the first meta-analysis to assess antibody response rate changes over time when comparing vaccination-induced immunity and natural immunity, as well as different antibody types.
Our primary findings show that for both the vaccination group and the infection group, the pooled IgG antibody response rate increased continuously for the first month. In the first week, the pooled response rate was significantly higher for naturally infected patients than for vaccinees (p < 0.01), indicating that COVID-19 vaccination triggers a slower and more gentle IgG antibody response than natural infection. This suggests that existing vaccines have room for improvement respecting the speed with which they provide antibody protection. However, starting from the second week following symptom onset/diagnosis/vaccination, any differences between the infection group and the vaccination group considering IgG positivity rate were not significant (all p values > 0.01). This suggests that vaccination may match the effectiveness of natural infection in inducing antibody production after a short period, which would increase confidence in existing COVID-19 vaccines. However, after more than 6 months, the vaccination group’s IgG response rate declined sharply, suggesting the need for a booster dose.
For the analysis by antibody type, between-group differences were not significant during the first week following vaccination or infection (p = 0.97). The pooled responses for each antibody type were all relatively small during the first 7 days, and antibody positivity rates generally increased over the first month. Röltgen and Boyd drew a similar conclusion in a previous review [5]. Relatively high positivity rates for IgG and IgA appear to have been maintained after the first month, compared those observed for IgM. Moreover, after the second month, IgM positivity rates were significantly different from those for other antibody types, with the IgG response appearing to be stronger and more persistent. This is consistent with previous knowledge that IgM usually provides early-stage protection while IgG provides long-term immune memory [77, 78]. Additional sensitivity analyses conducted by excluding each study one at a time yielded similar results and supported our main findings.
These findings have several important implications for vaccine development. If the immune response to SARS-CoV-2 could be maintained at sufficiently high levels for a period of time, it would effectively block infection for that period, which could have significant benefits for suppressing COVID-19 transmission. Improving the speed and level of antibody response produced by vaccines could substantially improve the population antibody protection level. One potential means to accomplish this would be developing new vaccine adjuvants designed to extend the duration of the IgG antibody response. Our findings also have important implications for serological surveys, which can shed light on population immunity levels. For example, a positive IgM test may suggest early period of infection/post-vaccination, while a negative IgM test plus a positive IgG test may indicate that the antibody response has been sustained in vivo for a time.
A notable consideration is the cybersecurity of the research regarding the dynamics of antibody response following SARS-CoV-2 vaccination or infection. With the increasing reliance on digital healthcare systems for data collection and storage, it has become crucial to address potential cybersecurity issues. The COVID-19 pandemic has expedited the utilization of digital platforms for healthcare data management, encompassing the collection and analysis of antibody response data, the implementation of biological data mining and machine learning techniques [79], and the utilization of artificial intelligence (AI) [80]. However, the integration of digital systems also introduces potential vulnerabilities and cybersecurity risks. Several studies have proposed strategies to safeguard data, such as employing blockchain technology in public health, which can foster secure practices in the realm of SARS-CoV-2 antibody response research [81, 82].
Our study has several limitations. First, the number of included studies of vaccinated individuals was limited, and only several types of vaccines were included among all the World Health Organization-approved vaccines (Ad26.COV2.S was missing from the study). Thus, our results should be generalized with caution. Second, the antibody responses of individuals who have been naturally infected with COVID-19 could potentially be affected by any therapies to which they were exposed. Due to the lack of treatment information in most studies, we were unable to consider the impact of therapy on immunity outcomes. Subgroup analysis by patient hospitalization status might reveal the impact of treatment on antibody response rates if therapy information were accessible. Third, we observed high heterogeneity values. Subgroup and sensitivity analyses confirmed the robustness of the results; however, they did not unveil the sources of this high heterogeneity. Possible sources of heterogeneity include large variations in sample size, demographic differences, and antibody detection methods employed in the studies, among others. More analyses could be conducted to further explore sources of heterogeneity. Finally, while the seroconversion rate is a vital indicator for assessing antibody response, the strength of the antibody response (i.e., antibody amount) is another important dimension. Evaluating this aspect of the antibody response is a potential direction for future study.
Conclusion
Vaccination may trigger a slower and gentler early antibody response against SARS-CoV-2 than natural infection, but seroconversion rates in vaccinees generally catch up after 1 week. IgG response is stronger and more persistent than the IgM response for both naturally infected and vaccinated individuals. These findings will provide useful insights on COVID-19 antibody responses and can help inform future vaccine development.
Availability of data and materials
The data will be made available from the corresponding authors upon reasonable request.
References
Worldometer: COVID live-corona statistics. https://www.worldometers.info/coronavirus/. Accessed Sept 2023.
Zachariah P, Johnson CL, Halabi KC, et al. Epidemiology, clinical features, and disease severity in patients with coronavirus disease 2019 (COVID-19) in a children’s hospital in New York City, New York. JAMA Pediatr. 2020;174(10):e202430. https://doi.org/10.1001/jamapediatrics.2020.2430.
FDA authorizes first oral antiviral for treatment of COVID-19. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-first-oral-antiviral-treatment-covid-19. Accessed Apr 2022.
AghamirzaMoghimAliabadi H, Eivazzadeh-Keihan R, BeigParikhani A, et al. COVID-19: a systematic review and update on prevention, diagnosis, and treatment. MedComm. 2022;3(1):e115.
Röltgen K, Boyd SD. Antibody and B cell responses to SARS-CoV-2 infection and vaccination. Cell Host Microbe. 2021;29(7):1063–75.
Wu D, Wu T, Liu Q, Yang Z. The SARS-CoV-2 outbreak: what we know. Int J Infect Dis. 2020;94:44–8.
Ezzikouri S, Nourlil J, Benjelloun S, Kohara M, Tsukiyama-Kohara K. Coronavirus disease 2019 — historical context, virology, pathogenesis, immunotherapy, and vaccine development. Hum Vaccin Immunother. 2020;16(12):2992–3000.
Wang MY, Zhao R, Gao LJ, Gao XF, Wang DP, Cao JM. SARS-CoV-2: structure, biology, and structure-based therapeutics development. Front Cell Infect Microbiol. 2020;10:587269.
Gorbalenya AE, Baker SC, Baric RS, Coronaviridae Study Group of the International Committee on Taxonomy of Viruses, et al. The species severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol. 2020;5(4):536–44.
Jackson CB, Farzan M, Chen B, Choe H. Mechanisms of SARS-CoV-2 entry into cells. Nat Rev Mol Cell Biol. 2022;23(1):3–20.
Premkumar L, Segovia-Chumbez B, Jadi R, et al. The receptor-binding domain of the viral spike protein is an immunodominant and highly specific target of antibodies in SARS-CoV-2 patients. Sci Immunol. 2020;5(48):eabc8413.
Galipeau Y, Greig M, Liu G, Driedger M, Langlois MA. Humoral responses and serological assays in SARS-CoV-2 infections. Front Immunol. 2020;11:610688.
Hangartner L, Zinkernagel RM, Hengartner H. Antiviral antibody responses: the two extremes of a wide spectrum. Nat Rev Immunol. 2006;6(3):231–43.
Chi X, Yan R, Zhang J, et al. A neutralizing human antibody binds to the N-terminal domain of the spike protein of SARS-CoV-2. Science. 2020;369(6504):650–5.
Altawalah H. Antibody responses to natural SARS-CoV-2 infection or after COVID-19 vaccination. Vaccines. 2021;9(8):910.
Wang J, Chen C, Li Q, Cai P, Wang Z, Wang L. COVID-19 confirmed patients with negative antibodies results. BMC Infect Dis. 2020;20(1):1–4.
Long QX, Tang XJ, Shi QL, et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat Med. 2020;26(8):1200–4.
Ibarrondo FJ, Fulcher JA, Goodman-Meza D, et al. Rapid decay of anti-SARS-CoV-2 antibodies in persons with mild COVID-19. N Engl J Med. 2020;383(11):1085–7.
Jones D, Helmreich S. A history of herd immunity. Lancet. 2020;396(10254):810–1.
WHO COVID-19 vaccine tracker and landscape. https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines. Accessed Sept 2023.
Yuan P, Ai P, Liu Y, et al. Safety, tolerability, and immunogenicity of COVID-19 vaccines: a systematic review and meta-analysis. MedRxiv. 2020. https://doi.org/10.1101/2020.11.03.20224998.
Vargas L, Valdivieso N, Tempio F, et al. Serological study of CoronaVac vaccine and booster doses in Chile: immunogenicity and persistence of anti-SARS-CoV-2 spike antibodies. BMC Med. 2022;20(1):1–3.
Bueno SM, Abarca K, González PA, et al. Safety and immunogenicity of an inactivated severe acute respiratory syndrome coronavirus 2 vaccine in a subgroup of healthy adults in Chile. Clin Infect Dis. 2022;75(1):e792-804.
Effective Practice and Organisation of Care (EPOC). Data collection form. EPOC resources for review authors. Oslo: Norwegian Knowledge Centre for the Health Services; 2013.
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (MINORS): development and validation of a new instrument. ANZ J Surg. 2003;73(9):712–6.
Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. https://doi.org/10.1136/bmj.d5928.
Van Houwelingen HC, Arends LR, Stijnen T. Advanced methods in meta-analysis: multivariate approach and meta-regression. Stat Med. 2002;21(4):589–624.
Barendregt JJ, Doi SA, Lee YY, Norman RE, Vos T. Meta-analysis of prevalence. J Epidemiol Community Health. 2013;67(11):974–8.
Barker TH, Migliavaca CB, Stein C, et al. Conducting proportional meta-analysis in different types of systematic reviews: a guide for synthesisers of evidence. BMC Med Res Methodol. 2021;21:189.
Tufanaru C, Munn Z, Stephenson M, Aromataris E. Fixed or random effects meta-analysis? Common methodological issues in systematic reviews of effectiveness. Int J Evid Based Healthc. 2015;13(3):196–207.
R Core Team. R: a language and environment for statistical computing. Vienna: R Foundation for Statistical Computing. https://www.r-project.org/. Accessed Feb 2022.
Jin ZC, Zhou XH, He J. Statistical methods for dealing with publication bias in meta-analysis. Stat Med. 2015;34(2):343–60.
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-34.
Kaneko S, Kurosaki M, Sugiyama T, et al. The dynamics of quantitative SARS-CoV-2 antispike IgG response to BNT162b2 vaccination. J Med Virol. 2021;93(12):6813–7.
Wei J, Stoesser N, Matthews PC, et al. Antibody responses to SARS-CoV-2 vaccines in 45,965 adults from the general population of the United Kingdom. Nat Microbiol. 2021;6(9):1140–9.
Barin B, Kasap U, Selçuk F, Volkan E, Uluçkan Ö. Comparison of SARS-CoV-2 anti-spike receptor binding domain IgG antibody responses after CoronaVac, BNT162b2, ChAdOx1 COVID-19 vaccines, and a single booster dose: a prospective, longitudinal population-based study. Lancet Microbe. 2022;3(4):e274-83.
Jäger M, Dichtl S, Bellmann-Weiler R, et al. Serum neutralization against SARS-CoV-2 variants is heterogenic and depends on vaccination regimen. J Infect Dis. 2023;227(4):528–32.
Liang XM, Xu QY, Jia ZJ, et al. A third dose of an inactivated vaccine dramatically increased the levels and decay times of anti-SARS-CoV-2 antibodies, but disappointingly declined again: a prospective, longitudinal, cohort study at 18 serial time points over 368 days. Front Immunol. 2022;1997:876037.
Hua Q, Zhang H, Yao P, et al. Immunogenicity and immune-persistence of the CoronaVac or Covilo inactivated COVID-19 vaccine: a 6-month population-based cohort study. Front Immunol. 2022;13:939311.
Tao Y, Ma M, Hu F, et al. A longitudinal study of humoral immune responses induced by a 3-dose inactivated COVID-19 vaccine in an observational, prospective cohort. BMC Immunol. 2022;23(1):1.
Cheng ZJ, Huang H, Zheng P, et al. Humoral immune response of BBIBP COVID-19 vaccination before and after the booster immunization. Allergy. 2022;77:2404–14.
Wang X, Deng Y, Zhao L, et al. Safety, immunogenicity, and immune persistence of two inactivated COVID-19 vaccines replacement vaccination in China: an observational cohort study. Vaccine. 2022;40(39):5701–8.
Padoan A, Sciacovelli L, Basso D, et al. IgA-Ab response to spike glycoprotein of SARS-CoV-2 in patients with COVID-19: a longitudinal study. Clin Chim Acta. 2020;1(507):164–6.
Mao N, Zhu Z, Zhu S, et al. Antibody response to COVID-19 virus — Heilongjiang Province and Gansu Province, China, 2020. China CDC Weekly. 2020;2(34):645.
Ren L, Fan G, Wu W, et al. Antibody responses and clinical outcomes in adults hospitalized with severe coronavirus disease 2019 (COVID-19): a post hoc analysis of LOTUS China trial. Clin Infect Dis. 2021;72(10):e545-51.
Jiang C, Wang Y, Hu M, et al. Antibody seroconversion in asymptomatic and symptomatic patients infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Clin Transl Immunol. 2020;9(9):e1182.
Liu C, Yu X, Gao C, et al. Characterization of antibody responses to SARS-CoV-2 in convalescent COVID-19 patients. J Med Virol. 2021;93(4):2227–33.
Solbach W, Schiffner J, Backhaus I, et al. Antibody profiling of COVID-19 patients in an urban low-incidence region in northern Germany. Front Public Health. 2020;8:570543.
Kowitdamrong E, Puthanakit T, Jantarabenjakul W, et al. Antibody responses to SARS-CoV-2 in patients with differing severities of coronavirus disease 2019. PLoS ONE. 2020;15(10):e0240502.
Maine GN, Lao KM, Krishnan SM, et al. Longitudinal characterization of the IgM and IgG humoral response in symptomatic COVID-19 patients using the Abbott Architect. J Clin Virol. 2020;133:104663.
Zhao J, Yuan Q, Wang H, et al. Antibody responses to SARS-CoV-2 in patients with novel coronavirus disease 2019. Clin Infect Dis. 2020;71(16):2027–34.
Li K, Huang B, Wu M, et al. Dynamic changes in anti-SARS-CoV-2 antibodies during SARS-CoV-2 infection and recovery from COVID-19. Nat Commun. 2020;11(1):1.
Sterlin D, Mathian A, Miyara M, et al. IgA dominates the early neutralizing antibody response to SARS-CoV-2. Sci Transl Med. 2021;13(577):eabd2223.
Imai K, Kitagawa Y, Tabata S, et al. Antibody response patterns in COVID-19 patients with different levels of disease severity in Japan. J Med Virol. 2021;93(5):3211–8.
Wu J, Liang B, Chen C, et al. SARS-CoV-2 infection induces sustained humoral immune responses in convalescent patients following symptomatic COVID-19. Nat Commun. 2021;12(1):1–9.
Patil HP, Rane PS, Shrivastava S, et al. Antibody (IgA, IgG, and IgG subtype) responses to SARS-CoV-2 in severe and nonsevere COVID-19 patients. Viral Immunol. 2021;34(3):201–9.
Carnicelli A, Fiori B, Ricci R, et al. Characteristic of IgA and IgG antibody response to SARS-CoV-2 infection in an Italian referral COVID-19 hospital. Intern Emerg Med. 2022;17(1):53–64.
Liu L, Chen HG, Li Y, et al. Temporal profiles of antibody responses, cytokines, and survival of COVID-19 patients: a retrospective cohort. Engineering. 2021;7(7):958–65.
Yadav AK, Ghosh S, Kotwal A, et al. Seroconversion among COVID-19 patients admitted in a dedicated COVID hospital: a longitudinal prospective study of 1000 patients. Med J Armed Forces India. 2021;1(77):S379-84.
Brynjolfsson SF, Sigurgrimsdottir H, Einarsdottir ED, et al. Detailed multiplex analysis of SARS-CoV-2 specific antibodies in COVID-19 disease. Front Immunol. 2021;12:695230.
Xiang T, Liang B, Fang Y, et al. Declining levels of neutralizing antibodies against SARS-CoV-2 in convalescent COVID-19 patients one year post symptom onset. Front Immunol. 2021;12:2327.
Luo H, Camilleri D, Garitaonandia I, et al. Kinetics of anti-SARS-CoV-2 IgG antibody levels and potential influential factors in subjects with COVID-19: a 11-month follow-up study. Diagn Microbiol Infect Dis. 2021;101(4):115537.
Alshami A, Al Attas R, Anan H, et al. Durability of antibody responses to SARS-CoV-2 infection and its relationship to disease severity assessed using a commercially available assay. Front Microbiol. 2021;12:770727.
Akter A, Ahmed T, Tauheed I, et al. Disease characteristics and serological responses in patients with differing severity of COVID-19 infection: a longitudinal cohort study in Dhaka, Bangladesh. PLoS Negl Trop Dis. 2022;16(1):e0010102.
Bastug A, Bodur H, Seker UO, et al. Neutralizing antibody response and associated factors in coronavirus-19 disease (COVID-19) up to one month. Turkish J Biochem. 2022;47(1):9–18.
Park S, Chang SH, Lee JH, et al. Serological evaluation of patients with coronavirus disease-2019 in Daegu, South Korea. PLoS ONE. 2022;17(1):e0262820.
Yang Y, Yang M, Peng Y, et al. Longitudinal analysis of antibody dynamics in COVID-19 convalescents reveals neutralizing responses up to 16 months after infection. Nat Microbiol. 2022;7(3):423–33.
Chen F, Zhong Y, Li J, Luo J. Dynamic changes of SARS-CoV-2 specific IgM and IgG among population vaccinated with COVID-19 vaccine. Epidemiol Infect. 2022;150:1–17.
Chansaenroj J, Yorsaeng R, Puenpa J, et al. Long-term persistence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike protein-specific and neutralizing antibodies in recovered COVID-19 patients. PLoS ONE. 2022;17(4):e0267102.
Kaduskar O, Gurav YK, Deshpande K, et al. Understanding the dynamics of IgM & IgG antibodies in COVID-19-positive patients. Indian J Med Res. 2022;155(5&6):565–9.
Xu R, Zhao B, Lan L, et al. A one-year follow-up study on dynamic changes of leukocyte subsets and virus-specific antibodies of patients with COVID-19 in Sichuan, China. Int J Med Sci. 2022;19(7):1122.
Ghasemi D, Araeynejad F, Maghsoud O, et al. The trend of IgG and IgM antibodies during 6-month period after the disease episode in COVID-19 patients. Iran J Sci Technol Trans A Sci. 2022;46(6):1555–62.
Yuan Y, Xu J, Ma B, et al. Characteristics of humoral and cellular responses to coronavirus disease 2019 (COVID-19) inactivated vaccine in central China: a prospective, multicenter, longitudinal study. Front Immunol. 2023;14:1107866.
Bang MS, Kim CM, Cho NH, et al. Evaluation of humoral immune response in relation to COVID-19 severity over 1 year post-infection: critical cases higher humoral immune response than mild cases. Front Immunol. 2023;14:1203803.
Carvalho Á, Henriques AR, Queirós P, et al. Persistence of IgG COVID-19 antibodies: a longitudinal analysis. Front Public Health. 2023;10:1069898.
Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010;36(3):1–48.
Li G, Chen X, Xu A. Profile of specific antibodies to the SARS-associated coronavirus. N Engl J Med. 2003;349(5):508–9.
Hsueh PR, Huang LM, Chen PJ, Kao CL, Yang PC. Chronological evolution of IgM, IgA, IgG and neutralisation antibodies after infection with SARS-associated coronavirus. Clin Microbiol Infect. 2004;10(12):1062–6.
Albahri AS, Hamid RA, Alwan JK, et al. Role of biological data mining and machine learning techniques in detecting and diagnosing the novel coronavirus (COVID-19): a systematic review. J Med Syst. 2020;44:1.
Albahri AS, Duhaim AM, Fadhel MA, et al. A systematic review of trustworthy and explainable artificial intelligence in healthcare: assessment of quality, bias risk, and data fusion. Inform Fusion. 2023;96:156–91.
Sadeq N, Hamzeh Z, Nassreddine G, ElHassan T. The impact of blockchain technique on trustworthy healthcare sector. Mesopotamian J CyberSec. 2023;2023:105–15.
Mijwil M, Aljanabi M, Ali AH. ChatGPT: exploring the role of cybersecurity in the protection of medical information. Mesopotamian J Cybersec. 2023;2023:18–21.
Acknowledgements
We would like to express our sincere gratitude to the authors of the included studies who provided further information.
Funding
Open Access funding enabled and organized by Projekt DEAL. This work was supported by grants from Chinese Academy of Medical Sciences & Peking Union Medical College (2024-CFT-QT-034) and EU Horizon Europe (HORIZON-MSCA-2021-SE-01, Project: 101086139 — PoPMeD-SuSDeV).
Author information
Authors and Affiliations
Contributions
TB, CW, SC, QZ, and LJ conceived and designed the study. QZ, LJ, and SC did literature review, collected data, and drafted the manuscript. QC, CB, PG, TB, CW, TO, and JY critically revised the article. All authors approved the final version.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, Q., Jiao, L., Chen, Q. et al. COVID-19 antibody responses in individuals with natural immunity and with vaccination-induced immunity: a systematic review and meta-analysis. Syst Rev 13, 189 (2024). https://doi.org/10.1186/s13643-024-02597-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-024-02597-y