
Abstract
Background
Leptospirosis, an important zoonotic bacterial disease, commonly affects resource-poor populations and results in significant morbidity and mortality worldwide. The value of antibiotics in leptospirosis remains unclear, as evidenced by the conflicting opinions published.
Methods
We conducted a search in the PubMed, Web of Science, and Cochrane Library databases for studies. These studies included clinical trials and retrospective studies that evaluated the efficacy or safety of antibiotics for leptospirosis treatment. The primary outcomes assessed were defervescence time, mortality rate, and hospital stays. Subgroup analyses were performed based on whether there were cases involving children and whether there were cases of severe jaundice. Safety was defined as the prevalence of adverse events associated with the use of antibiotics. p scores were utilized to rank the efficacy of the antibiotics.
Results
There are included 9 randomized controlled trials (RCTs), 1 control trial (CT), and 3 retrospective studies (RS) involving 920 patients and 8 antibiotics. Six antibiotics resulted in significantly shorter defervescence times compared to the control, namely cefotaxime (MD, − 1.88; 95% CI = − 2.60 to − 1.15), azithromycin (MD, − 1.74; 95% CI = − 2.52 to − 0.95), doxycycline (MD, − 1.53; 95% CI = − 2.05 to − 1.00), ceftriaxone (MD, − 1.22; 95% CI = − 1.89 to − 0.55), penicillin (MD, − 1.22; 95% CI = − 1.80 to − 0.64), and penicillin or ampicillin (MD, − 0.08; 95% CI = − 1.01 to − 0.59). The antibiotics were not effective in reducing the mortality and hospital stays. Common adverse reactions to antibiotics included Jarisch–Herxheimer reaction, rash, headache, and digestive reactions (nausea, vomiting, diarrhea, abdominal pain, and others).
Conclusions
Findings recommend that leptospirosis patients be treated with antibiotics, which significantly reduced the leptospirosis defervescence time. Cephalosporins, doxycycline, and penicillin are suggested, and azithromycin may be a suitable alternative for drug-resistant cases.
Systematic review registration
PROSPERO CRD42022354938.
Similar content being viewed by others


Background
Leptospirosis is an endemic zoonotic infection with significant implications for human health, particularly for agricultural workers and those who engage in outdoor activities in endemic areas. Leptospira species are divided into pathogenic and putrefactive spirochetes and comprise more than 250 pathogenic species [1, 2]. These are aerobic spirochetes measuring 6 to 20 μm in length and 0.1 μm in diameter [3]. Leptospirosis is contracted when leptospires enter the body through the skin or mucous membranes of the mouth and conjunctiva. Transmission is either direct, from host to host, or indirect, via soil, infected animal urine, or contaminated water [4]. Incidence rates are underestimated due to a lack of disease awareness and relatively inaccessible and insufficiently rapid diagnostics [5]. Leptospirosis has protean manifestations, often resembling the clinical presentations of other diseases [5]. The disease most commonly affects the kidney and liver [6, 7] and can progress to vasculitis and multi-organ invasion. Most infections are subclinical or mild, with symptoms such as fever, chills, headache, severe myalgia, conjunctival suffusion, anorexia, nausea, vomiting, and prostration usually characterizing acute infections. Leptospirosis usually presents as a non-specific acute febrile illness with similar signs and symptoms to dengue, influenza, and rickettsial infections [8]. Despite its mild initial presentation, delayed intervention leads to severe and possibly fatal Weil’s disease, characterized by hemorrhage, jaundice, renal failure [1], and even nervous system involvement [9]. The clinicopathological features include azotemia, hyperbilirubinemia, elevated liver enzyme levels, and thrombocytopenia [7].
Symptomless Leptospira infections are common in endemic areas and affect resource-poor populations in Malaysia, India, Sri Lanka, and Brazil, resulting in significant morbidity and mortality [4]. Leptospira are estimated to cause one million infections and approximately 58,900 deaths annually with a case–fatality ratio of 6.85%, yet progress on leptospirosis treatments has been minimal [2]. Livestock and wildlife infections also result in economic livestock industry losses [10]. The main antibiotics currently used to treat leptospirosis include penicillin, ceftriaxone, doxycycline, oxytetracycline, and macrolides (azithromycin or clarithromycin) [5, 11, 12]. Mild cases may not require antibiotics or can be treated with oral doxycycline. More serious cases require intensive care and intravenous penicillin or ceftriaxone [5, 12]. Individuals allergic to penicillin or ceftriaxone may use doxycycline or a macrolide (azithromycin or clarithromycin) [11]. However, despite the ubiquity of leptospirosis with an estimated one million annual global cases, the effectiveness of these antibiotics against leptospirosis is unclear, and treatment choices remain controversial [1, 13,14,15,16]. This study aims to discern the best antibiotic options to treat leptospirosis.
The lack of quantitative efficacy comparisons between different antibiotics due to technical limitations has compromised the scope of previous meta-analyses and review articles [13,14,15,16]. To address this limitation, we conducted a systematic analysis of data from randomized clinical trials (RCTs), clinical trials (CTs), and retrospective studies (RSs) using network meta-analysis (NMA) to assess the efficacy and safety of antibiotic treatment for leptospirosis. Our aim with this NMA was to compare and rank different antibiotics to evaluate the efficacy and safety of antibiotic therapy for leptospirosis.
Methods
We developed and followed a protocol for all steps of our systematic review and meta-analysis (PROSPERO CRD42022354938) and reported the study in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [17] (eTable 1).
Search strategies and inclusion criteria
We conducted a comprehensive search of the three databases PubMed, Web of Science, and Cochrane Library from the date of creation to December 26, 2023, and the search was completed on January 2, 2024. We conducted three separate searches to maximize data collection, using terms like “leptospirosis,” “antibiotic,” and “controlled trials” (eTable 2).
The eligible studies met the following criteria: (i) controlled or retrospective clinical trials; (ii) laboratory-confirmed leptospirosis diagnoses via microscopic agglutination test (MAT), enzyme-linked immunosorbent assay (ELISA), polymerase chain reaction (PCR), or histopathological evaluation in hospitalized patients; (iii) evaluation of drug efficacy or safety for leptospirosis treatment; and (iv) written in English. We excluded studies on the basis of the following criteria: (i) incomplete data; (ii) review, case report, or comment to editors (lacking primary data); (iii) repeated publication; and (iv) patients unable to complete the therapy.
Two reviewers assessed all included studies independently (JMM and SX). Any disagreements were addressed during discussions with a third reviewer (FB or AL) until a consensus was reached.
Data extraction and outcomes
After training, two individuals reviewed the abstracts independently and identified articles for detailed assessment. In case of disagreement, the two parties discussed and resolved the issue or referred it to a third researcher for a final decision. Then, they extracted data from each included study and entered the results into a database. Collected data include first author, year of publication, country, screening test used, sample size, antibiotic dose, defervescence time, hospital stays, deaths, and adverse effects. We defined effectiveness on the basis of defervescence time, mortality, and hospital stays (lower values indicate better drug efficacy).
Quality of evidence and risk of bias
We assessed the risk of bias for each included study using the methodology established by the Cochrane Collaboration [18]. This involved assessing the validity of data from the included studies and assigning a judgement of either “low risk,” “high risk,” or “unclear risk” to each entry in a “risk of bias table.” Entries assigned an “unclear risk” indicate either lack of information or uncertainty over the potential for bias (eTable 3). The extent to which a Cochrane review can draw conclusions regarding the effects of an intervention depends on the validity of the data obtained from the included studies.
Statistical analysis
We used the Netmeta package of R version 4.2.1 and Cytoscape 3.9.1 to perform this NMA.
Data transformation before analysis was primarily based on the method by Hozo et al. and Cai et al. [19, 20]. Our efficacy assessment employed NMA frequency analysis methods by using the Netmeta package to synthesize total effects, analyze heterogeneity, and calculate rankings. Network plots graphed were by NAM analysis results, Cytoscape graphing (Fig. 2). We selected a fixed-effect or random-effect model based on the heterogeneity to synthesize the study effect sizes. We used Q and I2 tests to evaluate the statistical heterogeneity among studies, with an I2 > 50% indicating statistically significant heterogeneity. We used odds ratios (ORs) and 95% confidence intervals (95% CIs) to report the effect size for mortality and mean deviations (MDs) and 95% CIs to report the effect size for assessing the defervescence time and hospital stays. Antibiotic effectiveness of different subgroups was finally plotted in Fig. 3.
Inconsistency is a critical indicator for assessing the quality of an NMA (which reflects the difference in the effect estimate between direct and indirect evidence). Hence, we applied the back-calculation method to assess the inconsistency of this NMA. This method is based on the Z test and determines the inconsistency by the p-value; if p < 0.05, it indicates the presence of inconsistency in the NMA [21] (Fig. 4). Next, we ranked the efficacy of drugs according to the NMA results. We used p scores to measure the extent of certainty that a treatment was better than others, averaged over all competing therapies [22]. Subsequently, we used the p score as a metric to assess the efficacy ranking. p scores ranged from 0 (worst) to 1 (best), with higher scores indicating better efficacy. Forest and funnel plots were generated to assess the overall effect size and identify any publication bias. We used Begg’s funnel plot and Egger’s test to detect potential publication bias, with p < 0.05 considered as statistically significant [23, 24].
Results
Study characteristics
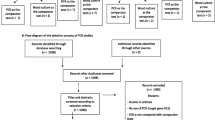
We obtained 1126 articles after searching the databases three times (609 papers from PubMed, 483 from Embase, and 29 from the Cochrane Library). The other 5 articles were identified through manual searches. We included 13 eligible articles [25,26,27,28,29,30,31,32,33,34,35,36,37] after excluding 493 duplicates and 620 ineligible articles. These included clinical trials were published between 1954 and 2012 and included 920 patients comparing the efficacy and safety of 8 antibiotics. Figure 1 illustrates the study selection process, and Table 1 presents the main characteristics of the included studies. The risk of bias assessment can be found in Supplemental Material 3.

Literature flowchart
Defervescence time
Effectiveness was demonstrated on the basis of the defervescence time [25, 26, 28,29,30,31,32, 34,35,36], mortality [29, 30, 32, 34, 35, 37], and hospital stays [32, 33, 35]. We assessed the effectiveness of eight treatment regimens by measuring their defervescence time (Fig. 2A). We found six interventions that improved the defervescence time including cefotaxime (MD, − 1.88; 95% CI, − 2.60 to − 1.15), azithromycin (MD, − 1.74; 95% CI, − 2.52 to − 0.95), doxycycline (MD, − 1.53; 95% CI, − 2.05 to − 1.00), ceftriaxone (MD, − 1.22; 95% CI, − 1.89 to − 0.55), penicillin (MD, − 1.22; 95% CI, − 1.80 to − 0.64), and penicillin or ampicillin (MD, − 0.08; 95% CI, − 1.01 to − 0.59) (Fig. 3A). By contrast, penicillin + chloramphenicol (MD, − 0.65; 95% CI, − 1.44 to 0.13) and chloramphenicol (MD, − 0.06; 95% CI, − 0.76 to 0.64) had no effect on the defervescence time. We also analyzed the defervescence time in subgroups according to whether there were cases involving children and whether there were cases of severe jaundice. Figure 2B, C shows the corresponding antibiotics, and Fig. 3A shows the antibiotic efficacies. Grouping patients with severe disease and jaundice resulted in a decrease in heterogeneity (I2 = 0%), compared to the previous value (I2 = 60.6%; Fig. 3A). This suggests that some of the heterogeneity may originate from seriously ill patients.

Network plots of available direct comparisons. Each node (solid circle) represents only one type of antibiotic delivery. The size of the nodes is proportional to the number of participants (sample size) involving the specific treatment intervention. The solid lines link treatments being directly compared (the thickness is proportional to the number of trials)

Treatment network meta-analysis and ranking. Other vs. control, “other” refers to antibiotics, “control” contains placebo, no antibiotics, ascorbic acid, and no treatment; Tau2/tau, quantifying heterogeneity; I2, quantifying inconsistency; MD, mean deviation; OR, odds ratio. A Comparisons of defervescence time for antibiotics and control. The subgroups are cases in children, patients without jaundice or severe disease, and patients with jaundice or severe disease. Cases in children include case studies of children. B Comparisons of mortality for antibiotics and controls. C Comparisons of hospital stays for antibiotics and controls
Mortality and hospital stays
Mortality and hospital stays were measured in association with four and three antibiotics, respectively (Fig. 2E, F). We observed similar mortality and hospital stays for all antibiotic and control groups (Fig. 3A), which no heterogeneity was found between the two measures.
Incidence of adverse reactions
Five studies [28, 30, 35,36,37] reported adverse reactions after antibiotic treatment for leptospirosis, including three antibiotics (penicillin, doxycycline, and azithromycin). Adverse reactions were mainly Jarisch–Herxheimer reactions for penicillin (2.6%), rashes, headaches, and digestive reactions (nausea, vomiting, diarrhea, abdominal pain, etc.). The rash incidences were 1.1% for penicillin, 0.7% for doxycycline, and 2.0% for azithromycin. We observed the highest incidence of adverse reactions in the digestive system, with a 15.2% of doxycycline users and 6.6% of azithromycin users experiencing vomiting (Table 2).
Ranking
We conducted pairwise comparisons of drugs to establish a ranking of their contribution to defervescence time, mortality, and hospital stays. As shown in Fig. 3, the p score decreased in order of efficacy, as in cefotaxime (0.93) > azithromycin (0.86) > doxycycline (0.75) > ceftriaxone (0.58) > penicillin (0.58) > penicillin or ampicillin (0.36). We observed similar mortality and hospital stays with controls and, therefore, do not describe these indicators.
Inconsistency and publication bias
The results of the evaluation of the inconsistency of the defervescence time across all comparisons are presented in Fig. 4. The analysis revealed statistically significant differences between the four groups in children: chloramphenicol vs. control (p < 0.01), chloramphenicol vs. penicillin (p < 0.01), penicillin + chloramphenicol vs. control (p < 0.01), and penicillin + chloramphenicol vs. penicillin (p < 0.01). These groups differed in their comparative analysis of direct evidence vs. indirect evidence (eFigure 1).

Pairwise comparisons of defervescence time, mortality, and hospital stays for antibiotics and control. Estimated treatment effect (MD) derived from direct and indirect evidence (95% confidence interval); p-value, test for disagreement (direct versus indirect); *p < 0.05
We found no evidence of publication bias in the defervescence time, as indicated by Begg’s funnel plot and Egger’s test results (p = 0.65). However, due to the limited number of studies, we could not apply Egger’s test to the other two indicators (mortality and hospital stays). See eFigure 2 for further details.
Discussion
Broad-spectrum antibiotics to cover bacteria are usually required while a definite diagnosis of leptospirosis is pending [34]. However, no exact guidelines on the type of antibiotic that should be prescribed exist, and the effectiveness of this approach has yet to be demonstrated. Improper use of antibiotics may lead to the emergence of resistant strains, adverse side effects, and increased medical costs [8]. Thus, this meta-study evaluating the effectiveness of antibiotics for Leptospira was needed. We aimed to identify the best antibiotic option to treat leptospirosis through a comprehensive meta-analysis, searching the literature in English using various related terms.
Despite the worldwide distribution of leptospirosis, only a small number of RCTs evaluating treatments have been performed [27,28,29,30, 32,33,34,35]. Unfortunately, the existing findings are conflicting, with some studies concluding that antibiotic treatment for spirochetes is beneficial [25, 27,28,29, 31, 34,35,36,37], while others have indicated that it is not effective [26, 30, 32, 33]. Some studies have recommended penicillin as the standard antibacterial drug for the treatment of moderate to severe leptospirosis [25, 29], but others found poor efficacy for patients with advanced severe leptospirosis [30, 32, 33]. Cefotaxime and ceftriaxone are third-generation cephalosporins with potential efficacy against leptospirosis. They can effectively inhibit the growth of Leptospira and shorten the duration of leptospirosis [34, 35]. Cephalosporins are preferred over penicillin because they are simpler to administer (ceftriaxone once a day given either intravenously or intramuscularly vs. penicillin four times per day given only intravenously) and more readily available. Also, in many cases of penicillin allergy, it is possible to safely administer a cephalosporin [38, 39]. Another favored antibiotic is doxycycline, which shortens the duration of the disease and has favorable effects on fever, malaise, headache, and myalgia [28, 36]. Doxycycline, which has been recommended and used widely for the prophylaxis and treatment of leptospirosis of mild severity [38, 40, 41], is also active against Rickettsia organisms. Azithromycin, although expensive, may be a good alternative for the treatment of leptospirosis, especially when drug resistance is suspected [36]. Clinical studies suggest that oxytetracycline may have good efficacy in the treatment of leptospirosis and that chloramphenicol has no efficacy [26, 27]. The tissue localization stages of leptospirosis have been identified and organ damage has been observed, but antibiotics may be of little value in regulating the disease process [30]. We found that the studies reporting limited significance for antibiotic treatment of leptospirosis were conducted in patients with severe, jaundiced, and acute renal failure leptospirosis, and we cannot exclude that our results were affected by this selection of patients [26, 30, 32, 33].
Fever is one of the most common symptoms of leptospirosis, and we evaluated the time to fever reduction with antibiotics. Six types of medications (cefotaxime, azithromycin, doxycycline, ceftriaxone, penicillin, and penicillin or ampicillin group) significantly reduced the defervescence time. However, the antibiotics were not effective in reducing the mortality and hospital stay lengths. We speculate that the smaller number of included studies and larger number of included severe leptospirosis cases have an impact on the evaluation of mortality and hospital stay lengths. The main adverse reactions after antibiotic use included Jarisch–Herxheimer reactions, rash, headache, and digestive reactions (nausea, vomiting, diarrhea, and abdominal pain). We found that most of the included articles discussed severe or jaundiced leptospirosis, so we performed a subgroup study on the defervescence time for these patients. Antibiotics were ineffective for treating severe or jaundiced leptospirosis, with the exception of the penicillin or ampicillin group, which showed some efficacy. Severe or advanced disease reflects the second stage of leptospirosis, which is largely considered an immune-mediated event [42, 43]. The use of antibiotic potency at this stage is controversial. The limited number of studies included in our analysis prevents us from drawing definitive conclusions regarding the efficacy of antibiotics in severe/late leptospirosis.
Evaluating antibiotic therapies for leptospirosis is difficult due to the wide range of severity and complications associated with the disease. Mild clinical symptoms may not require antibiotic treatment and may resolve on their own [44]. However, as the disease can potentially evolve to a more severe stage, with life-threatening complications, we recommend that the patient be treated with antibiotics in time after diagnosis. Although antibiotics have no meaningful impact on the lethality of the infection, they can accelerate the defervescence, thereby alleviating the patient’s discomfort and buying time for treatment. Therefore, we recommend the use of cephalosporins, doxycycline, or penicillin for the treatment of leptospirosis. Azithromycin is a potential drug-resistance alternative.
The management of antibiotic therapy for leptospirosis is fraught with problems: (i) the lack of experimental and clinical data, as well as the lack of understanding of the pathophysiology of the disease, has hindered progress in the field of antibiotic treatment of leptospirosis. (ii) The leptospirosis diagnoses are commonly delayed, and some experts recommend that medication should be administered as soon as leptospirosis is suspected [44, 45]. (iii) The use of antibiotics in severe or advanced leptospirosis is controversial, and the terms “severe” and “late” have been used interchangeably with differing definitions. This is probably due to the notion that protracted clinical disease is de facto severe or prone to progressing to severe complications [44,45,46] and has implications for treatment. Prompt diagnoses and initiation of appropriate therapy are important for managing leptospirosis.
The sources of infection included in this paper were from Australia, Malaya, Malaysia, Panama, the Philippines, the West Indies, Brazil, and Thailand. Most of these places are tropical developing countries with a high incidence of leptospirosis. High temperatures, stagnant water, and poor sanitation all contribute to the high incidence of leptospirosis in the tropics. There are more Leptospira serotypes in the tropics and there is no literature on the relationship of these serotypes to treatment and drug resistance. Clinical trials of antibiotic treatment for leptospirosis are few and old, and it is difficult to discern differences in antibiotic treatment and resistance in different regions from the available data. It is hoped that more studies will supplement these deficiencies at a later stage.
This study has limitations. First, while we only included clinical control trials, some of these were not randomized control trials, which may lead to variable results. We did a bias analysis and did not find any bias in the results due to non-RCT data. Second, we did not have access to high-quality data on all drugs and mortality, which may affect efficacy and safety to some extent. Third, there is insufficient RCT data to produce results on the duration of drug treatment, dosage, etc. Lastly, we did find evidence of inconsistency in the results from our indirect comparison analysis. These findings should be interpreted with caution as the low number of pairwise comparisons suggests that there may be significant differences in drug efficacy from a clinical perspective.
Conclusions
Although antibiotics have no meaningful impact on the mortality and hospital stays of the leptospirosis infection, they can accelerate the defervescence, thereby alleviating the patient’s discomfort and buying time for treatment. Cephalosporins, doxycycline, penicillin, and azithromycin are recommended for leptospirosis.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- RCTs:
-
Randomized clinical trials
- CTs:
-
Clinical trials
- RSs:
-
Retrospective studies
- NMA:
-
Network meta-analysis
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analysis
- MAT:
-
Microscopic agglutination test
- ELISA:
-
Enzyme-linked immunosorbent assay
- PCR:
-
Polymerase chain reaction
- ORs:
-
Odds ratios
- CIs:
-
Confidence intervals
- MDs:
-
Mean deviations
References
Pinto GV, Senthilkumar K, Rai P, Kabekkodu SP, Karunasagar I, Kumar BK. Current methods for the diagnosis of leptospirosis: issues and challenges. J Microbiol Methods. 2022;195:106438.
Costa F, Hagan JE, Calcagno J, Kane M, Torgerson P, Martinez-Silveira MS, et al. Global morbidity and mortality of leptospirosis: a systematic review. PLoS Negl Trop Dis. 2015;9:e0003898.
Evangelista KV, Coburn J. Leptospira as an emerging pathogen: a review of its biology, pathogenesis and host immune responses. Future Microbiol. 2010;5:1413–25.
Soo ZMP, Khan NA, Siddiqui R. Leptospirosis: increasing importance in developing countries. Acta Trop. 2020;201:105183.
Bharti AR, Nally JE, Ricaldi JN, Matthias MA, Diaz MM, Lovett MA, et al. Leptospirosis: a zoonotic disease of global importance. Lancet Infect Dis. 2003;3:757–71.
Gohil J, Gowda A, George T, Easwer HV, George A, Nair P. Pituitary apoplexy and panhypopituitarism following acute leptospirosis. Pituitary. 2021;24:854–8.
Eric Klaasen HL, Adler B. Recent advances in canine leptospirosis: focus on vaccine development. Vet Med (Auckl). 2015;6:245–60.
Levett PN. Leptospirosis. Clin Microbiol Rev. 2001;14:296e326.
Tomacruz ID, Sandejas JC, Berba R, Sacdalan DR. Behavioural change: a rare presentation of leptospirosis. BMJ Case Rep. 2019;12:e230619.
Rocha BR, Martins G, Lilenbaum W. An historical view of the experimental leptospiral infection in ruminants. Comp Immunol Microbiol Infect Dis. 2020;73:101532.
Rajapakse S. Leptospirosis: clinical aspects. Clin Med (Lond). 2022;22:14–7.
Grennan D. Leptospirosis. JAMA. 2019;321:812.
Guzmán Pérez M, Blanch Sancho JJ, Segura Luque JC, Mateos Rodriguez F, Martínez Alfaro E, Solís García Del Pozo J. Current evidence on the antimicrobial treatment and chemoprophylaxis of human leptospirosis: a meta-analysis. Pathogens. 2021;10:1125.
Brett-Major DM, Coldren R. Antibiotics for leptospirosis. Cochrane Database Syst Rev. 2012;2:CD008264.
Guidugli F, Castro AA, Atallah AN. Antibiotics for treating leptospirosis. Cochrane Database Syst Rev. 2000;2:CD001306.
Naing C, Reid SA, Aung K. Comparing antibiotic treatment for leptospirosis using network meta-analysis: a tutorial. BMC Infect Dis. 2017;17:29.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5:13.
Cai S, Zhou J, Pan J. Estimating the sample mean and standard deviation from order statistics and sample size in meta-analysis. Stat Methods Med Res. 2021;30:2701–19.
Dias S, Welton NJ, Caldwell DM, Ades AE. Checking consistency in mixed treatment comparison meta-analysis. Stat Med. 2010;29:932–44.
Rücker G, Schwarzer G. Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med Res Methodol. 2015;15:1–9.
Ji Z, Jian M, Chen T, Luo L, Li L, Dai X, et al. Immunogenicity and safety of the M72/AS01E candidate vaccine against tuberculosis: a meta-analysis. Front Immunol. 2019;10:2089.
Ji Z, Jian M, Yue P, Cao W, Xu X, Zhang Y, et al. Prevalence of Borrelia burgdorferi in Ixodidae tick around Asia: a systematic review and meta-analysis. Pathogens. 2022;11:143.
Doherty RL. A clinical study of leptospirosis in North Queensland. Australas Ann Med. 1955;4:53–63.
Fairburn AC, Semple SJ. Chloramphenicol and penicillin in the treatment of leptospirosis among British troops in Malaya. Lancet. 1956;270:13–6.
Russell RW. Treatment of leptospirosis with oxytetracycline. Lancet. 1958;2:1143–5.
McClain JB, Ballou WR, Harrison SM, Steinweg DL. Doxycycline therapy for leptospirosis. Ann Intern Med. 1984;100:696–8.
Watt G, Padre LP, Tuazon ML, Calubaquib C, Santiago E, Ranoa CP, et al. Placebo-controlled trial of intravenous penicillin for severe and late leptospirosis. Lancet. 1988;1:433–5.
Edwards CN, Nicholson GD, Hassell TA, Everard CO, Callender J. Penicillin therapy in icteric leptospirosis. Am J Trop Med Hyg. 1988;39:388–90.
Marotto PC, Marotto MS, Santos DL, Souza TN, Seguro AC. Outcome of leptospirosis in children. Am J Trop Med Hyg. 1997;56:307–10.
Daher EF, Nogueira CB. Evaluation of penicillin therapy in patients with leptospirosis and acute renal failure. Rev Inst Med Trop Sao Paulo. 2000;42:327–32.
Costa E, Lopes AA, Sacramento E, Costa YA, Matos ED, Lopes MB, et al. Penicillin at the late stage of leptospirosis: a randomized controlled trial. Rev Inst Med Trop Sao Paulo. 2003;45:141–5.
Panaphut T, Domrongkitchaiporn S, Vibhagool A, Thinkamrop B. Ceftriaxone compared with sodium penicillin G for treatment of severe leptospirosis. Clin Infect Dis. 2003;36:1507–13.
Suputtamongkol Y, Niwattayakul K, Suttinont C, Losuwanaluk K, Limpaiboon R, Chierakul W, et al. An open, randomized, controlled trial of penicillin, doxycycline, and cefotaxime for patients with severe leptospirosis. Clin Infect Dis. 2004;39:1417–24.
Phimda K, Hoontrakul S, Suttinont C, Chareonwat S, Losuwanaluk K, Chueasuwanchai S, et al. Doxycycline versus azithromycin for treatment of leptospirosis and scrub typhus. Antimicrob Agents Chemother. 2007;51:3259–63.
Daher EF, Silva GB Jr, de Abreu KL, Mota RM, Batista DV, Rocha NA, et al. Leptospirosis-associated acute kidney injury: penicillin at the late stage is still controversial. J Clin Pharm Ther. 2012;37:420–5.
Pappas G, Cascio A. Optimal treatment of leptospirosis: queries and projections. Int J Antimicrob Agents. 2006;28:491–6.
Vinetz JM. A mountain out of a molehill: do we treat acute leptospirosis, and if so, with what? Clin Infect Dis. 2003;36:1514–5.
Sehgal SC, Sugunan AP, Murhekar MV, Sharma S, Vijayachari P. Randomized controlled trial of doxycycline prophylaxis against leptospirosis in an endemic area. Int J Antimicrob Agents. 2000;13:249–55.
Takafuji ET, Kirkpatrick JW, Miller RN, Karwacki JJ, Kelley PW, Gray MR, et al. An efficacy trial of doxycycline chemoprophylaxis against leptospirosis. N Engl J Med. 1984;310:497–500.
Rodrigo C, de LakshithaSilva N, Goonaratne R, Samarasekara K, Wijesinghe I, Parththipan B, et al. High dose corticosteroids in severe leptospirosis: a systematic review. Trans R Soc Trop Med Hyg. 2014;108:743–50.
Cagliero J, Villanueva SYAM, Matsui M. Leptospirosis pathophysiology: into the storm of cytokines. Front Cell Infect Microbiol. 2018;8:204.
Faucher JF, Hoen B, Estavoyer JM. The management of leptospirosis. Expert Opin Pharmacother. 2004;5:819–27.
Yang CW. Leptospirosis in Taiwan–an underestimated infectious disease. Chang Gung Med J. 2007;30:109–15.
Daher Ede F, de Abreu KL, da Silva Junior GB. Leptospirosis-associated acute kidney injury. J Bras Nefrol. 2010;32:400–7.
Funding
This work was supported by Natural Foundation of Yunnan Province grants 2019FE001-(002) and 2017FE467-(001) and National Natural Science Foundation of China grants 32060180, 81860644, 81560596, and 31560051.
Author information
Authors and Affiliations
Contributions
Bao and Liu had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. AHL, FKB, and ZHJ initiated the project and were responsible for the design of the protocol. ZHJ, MMJ, XS, YYP, YD, WJM, LZ, JRY, JQS, XW, LG, WJM, JK, BXL, JJC, MXL, YXF, LP, and YD performed the literature review, collected the data, and assessed the quality of the studies. MMJ, XS, YYP, WJM, LZ, JRY, BXL, JJC, MXL, and YXF analyzed the data. MMJ, XS, YYP, WJM, LZ, and JRY interpreted the data. ZHJ and MMJ wrote the initial draft of the manuscript. FKB, AHL, and ZHJ were responsible for the critical revision of the manuscript. All authors approved the final version submitted for publication.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This work does not involve any participants and as such ethical approval was not sought.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ji, Z., Jian, M., Su, X. et al. Efficacy and safety of antibiotics for treatment of leptospirosis: a systematic review and network meta-analysis. Syst Rev 13, 108 (2024). https://doi.org/10.1186/s13643-024-02519-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-024-02519-y