
Abstract
Background
Whilst there are studies that have systematically reviewed the psychometric properties of quality of life measures for children and young people with intellectual disabilities, these narrowly focus on disease or health conditions. The objective of this planned systematic review is therefore to collate, summarise, and critically appraise the psychometric properties of self-report health-related quality of life (HRQoL) and subjective wellbeing measures used by adolescents (aged 11–16) with an intellectual disability.
Methods
We designed and registered a study protocol for a systematic review of studies which explores the psychometric properties of self-report HRQoL and subjective wellbeing measures used by adolescents with intellectual disabilities. Electronic databases including PsycINFO, CINAHL, MEDLINE, and ERIC will be searched using predefined search terms to identify relevant studies. Quantitative and mixed-methods studies, and studies published in peer-reviewed journals or grey literature, will be included. Review papers, editorials, and case studies will be excluded. Eligible studies should identify self-report measures which assess HRQoL and subjective wellbeing among adolescents with intellectual disabilities. The methodological quality of the included studies will be assessed by applying the COSMIN Risk of Bias checklist. The quality of the evidence (i.e. the total body of evidence used for the overall ratings on each psychometric property of an instrument) will be evaluated in accordance with the modified GRADE guidelines.
Discussion
This systematic review will be among the first to systematically explore the psychometric properties of self-report HRQoL and subjective wellbeing measures used by adolescents with intellectual disabilities. By providing evidence-based knowledge about measures being used in HRQoL and subjective wellbeing research amongst this population, and more importantly how reliable and valid these measures are, the most suitable for use will be identified. Our findings will be of potential interest to clinicians, researchers, and service providers who need information about the methodological quality and the characteristics of measures to make informed decisions about the most reliable and valid tool for a specific purpose. The findings from this study will contribute to the knowledge surrounding available and appropriate measures to use for measuring HRQoL and subjective wellbeing of adolescents with intellectual disabilities, which are necessary to inform intervention development and future health policy.
Systematic review registration
The protocol has been registered at the International Prospective Register of Systematic Reviews (PROSPERO). The registration number is CRD42021231697.
Similar content being viewed by others

Background
Only recently has the study of health-related quality of life (HRQoL) gained scientific interest and has assumed paramount importance in the identification of health risks and populations’ health status [32]. A related concept is that of subjective wellbeing. Despite some commonalities, HRQoL and subjective wellbeing should be treated as separate concepts [61]. According to the [59] can be defined ‘as a multi-dimensional construct shaped by an individuals’ experiences, beliefs, expectations and perceptions of their position in life in the context of their physical, psychological, and social domains of health’ [53].
Wellbeing has long been considered key to the creation and maintenance of healthy and productive societies [17]. Wellbeing is multifaceted [13, 15, 21] and encompasses both objective (e.g. income, education, health) and subjective (e.g. interpersonal relationships, autonomy) aspects of a person’s life [5, 21, 50, 54]. This approach to measuring perceptions and life experiences has been characterised as subjective wellbeing. There is no universally agreed definition of subjective wellbeing, and the term is often used interchangeably with life satisfaction, happiness, and quality of life [50, 54]. Subjective wellbeing falls within the hedonic perspective and can be understood as ‘how people feel and function, both on a personal and social level, and how they evaluate their lives as a whole’ [14, 34].
Intellectual disability (ID) is characterised by significant limitations in both intellectual functioning and adaptive behaviour as expressed in conceptual, social, and practical skills. This disability originates during the developmental period, which is defined operationally as before the individual attains age 22 [47]. The severity of ID is classified into four types, based on an intelligence quotient (IQ) test, namely mild, moderate, severe, and profound ID [46].
Whilst there is a wide range of research examining adolescent’s HRQoL and subjective wellbeing, few of these studies include children and young people with ID [2, 11]. Current large-scale global studies of wellbeing such as the WHO Health Behaviour of School-aged Children (HBSC) and Children’s Worlds do not include children with ID. This is of particular concern given that children and adolescents with ID are more likely to experience diminished mental health, chronic conditions, reduced quality of life, lower socioeconomic status, and social exclusion in comparison with their nonintellectually disabled peers [6, 18]. Many HRQoL and wellbeing measures are usually administered by survey and are not accessible to youth with ID. This population may have difficulty understanding the format and complexity of questions and response scales used in questionnaires designed for same-age peers [4, 11], as intellectual impairment is often associated with difficulties in communication [52], working memory [30], and self-insight [27], all of which are required to respond effectively to questionnaires. In 2011, Scott and colleagues carried out a pilot study including adolescents (aged 11–17 years) with ID/special educational needs in the WHO HBSC questionnaire. Using the standard protocol, just over half of the adolescents were able to ‘complete’ the survey questionnaire; however, a high proportion of their responses proved to be uncodable [49].
Adolescents with ID have traditionally been assessed via proxy reports completed by parents, teachers, or carers as it is assumed that these young persons do not have the capacity to self-report on these domains. While some professionals assume that adolescents with ID do not have the ability to self-report on these domains and cannot reliably report their own HRQoL and subjective wellbeing [31, 52], many researchers and clinicians do take the views of adolescents with ID seriously but acknowledge that it is a challenge [63]. As a result, this leaves adolescents with ID excluded from communicating their HRQoL and subjective wellbeing needs and thus heavily dependent on accurate information of the informants [49]. Limitations exist surrounding the robustness of proxy reflection of non-observable internal states (i.e. feelings), particularly in relation to people whose language limitations mean that they have not been able to tell even close proxies what they think [19]. Every individual has a unique perception of his/her HRQoL and subjective wellbeing which is influenced by context, previous experiences, and personal values [42]. This personal perspective can only be obtained through individuals themselves. Therefore, adolescent’s views should, where possible, be sought directly rather than being inferred from proxy reports [62]. Furthermore, recent research has shown that adolescents and parents’ perceptions of HRQoL and subjective wellbeing can differ, and that adolescents can reliably report their HRQoL and subjective wellbeing, provided that the measure is adapted to be appropriate to their age and cognitive functioning [26, 41].
Authors repeatedly note the underrepresentation of young people with ID in health and wellbeing surveys [25, 50]. A report from the Children’s Worlds survey highlights the exclusion of marginalised children, including those in special educational needs settings, and suggests that there is a real need for ways to be found to ‘include these children in research on children’s lives and wellbeing’ ([45]:16). Research has demonstrated that many adolescents with ID do have the capacity to respond to self-report questionnaires [16, 20], and that adaptations such as pictorial representations and limited forced choice options can strengthen their validity [23]. Thus, there has been an emphasis on finding alternative and more accessible ways to enable this population to complete questionnaires independently, reliably, and confidentially [3, 4]. Increasing attention has been paid to the involvement of young people with ID in the design of wellbeing measures and capturing their views on what wellbeing means to them and what is important to their quality of life [25]. For example, Boström et al. [4] developed the Wellbeing in Special Education Questionnaire (WellSEQ) in cooperation with 113 students (aged 12–16) and teachers in special educational needs settings for children with cognitive disabilities [4]. Both students and teachers participated in the process of cooperative inquiry [22] designing and developing the research instruments in three workshops using different methods (brainstorming, sketching, paper-prototyping, focus group, direct observations, and existing system analysis) [3, 4]. The WellSEQ is specifically tailored to measure self-rated mental and ill health, peer relations, and school and family environment in adolescents with mild or moderate intellectual and developmental disability and is administered via an interactive touch-based application for tablet PCs [4]. The standard method for collecting reliable self-reports from persons with ID has consisted of structured interviews (e.g. [24]), but because this is a highly time-consuming procedure, there has been a shift of focus to design questionnaires specifically for this population. As a result, in the past decade, and in line with the trend of stimulating participatory research used with young people with ID, recent studies have attempted to develop and use self-report HRQoL and subjective wellbeing measures for this target group as opposed to typically used proxy measures.
Researchers have started to address the dearth of instruments suitable for measuring HRQoL and subjective wellbeing with adolescents in the ID population. Whilst there are studies (e.g. [8, 28, 40, 53]) that have systematically reviewed the psychometric properties of QoL measures for young people with ID, these narrowly focus on disease or health conditions [11]. Therefore, an up-to-date systematic review is warranted to summarise and appraise the psychometric properties of HRQoL and subjective wellbeing measures focused on adolescents with ID as they are useful in selecting a measure that is fit for purpose [33, 48]. This review will provide evidence-based knowledge regarding what measures are being used in HRQoL and subjective wellbeing research amongst this population and, more importantly, how reliable and valid these measures are. The most suitable HRQoL and subjective wellbeing measures for use amongst adolescents with ID will be identified, and recommendations will be gathered to determine their reliability (i.e. to identify what works). This is urgently needed as clinicians, researchers, and service providers require information about the methodological quality and the characteristics of measures to make informed decisions about the most reliable and valid tool for a specific purpose [29]. It is expected that this systematic review will assist in informing choice when selecting an instrument for the measurement of HRQoL and subjective wellbeing with this population. It will contribute to the knowledge surrounding available and appropriate measures to use for measuring the HRQoL and subjective wellbeing of adolescents with ID, which are necessary to inform intervention development and future health policy.
The aim of this systematic review is to collate, summarise, and critically appraise the psychometric properties of all self-report HRQoL and subjective wellbeing measures used with adolescents (aged 11–16) with ID. The proposed systematic review will answer the following questions:
-
1.
What self-report measures are being/have been used to assess HRQoL and subjective wellbeing of adolescents with ID?
-
2.
What is the methodological quality of these HRQoL and subjective wellbeing measures for use by adolescents with ID?
-
3.
What self-report measures are the most suitable for assessing HRQoL and subjective wellbeing of adolescents with ID?
Methods
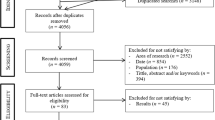
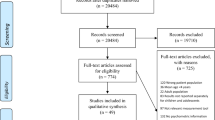
The present protocol has been written according to the PRISMA-P (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [35] (see PRISMA-P checklist is provided in Supplemental file 1). This protocol has been registered at the International Prospective Register of Systematic Reviews (PROSPERO) database (registration number: CRD42021231697).
Search strategy
The search strategy was developed after consultation with Ulster University’s Faculty of Life and Health Sciences senior librarian. The search strategy is broad to include all research articles that use a psychometric instrument to measure HRQoL and subjective wellbeing among adolescents with ID.
A systematic database search was performed using the Psychological Information Database (PsycINFO), Cumulative Index of Nursing and Allied Health Literature (CINAHL), Medical Literature Analysis Retrieval System Online (MEDLINE), and Education Resources Information Center (ERIC). Key terms pertaining to ID, HRQoL and subjective wellbeing, psychometric properties, measures, and adolescence will be used to search for studies for the review (see Supplemental file 2 for the search strategy and full search strings for each of the five key concepts in each database). Studies published from January 2000 to January 2020 and available in the English language will be considered.
Eligibility criteria
Studies will be selected according to the criteria outlined below.
Measures’ construct of interest
Eligible studies should report testing the psychometric properties of instruments designed for use with adolescents (aged 11–16) with ID to assess their HRQoL and subjective wellbeing. HRQoL includes physical health, psychological health, and social health. Subjective wellbeing includes life satisfaction, happiness, and quality of life. Studies designed for adults or older people with ID, and studies that do not assess HRQoL and subjective wellbeing domains, will be excluded.
Target population
The study population will include adolescents between the ages of 11 and 16 years as people younger than 11 are usually considered children, and studies that include people over 16 years may include samples with adults. If studies include adolescents with a broader or narrower age range than 11–16-year olds but encompass 11–16-year olds, they will also be included in our review. Participants must have an ID diagnosis, which is a disability characterised by significant limitations in both intellectual functioning and adaptive behaviour as expressed in conceptual, social, and practical skills [47]. Studies will be excluded if it is not clear whether participants have an ID (mild, moderate, severe, or profound) or where they have other conditions (i.e. autism, epilepsy, or physical disabilities) without specifically noting that they also have an ID.
Psychometric properties
To ensure standardisation across articles, the COSMIN taxonomy for psychometric properties will be adhered to [38, 39]. According to the taxonomy, psychometric properties cover three quality domains: reliability, validity, and responsiveness. The reliability domain comprises internal consistency, reliability, and measurement error. The validity domain comprises content validity, structural validity, hypotheses testing for construct validity, cross-cultural validity, and criterion validity. The responsiveness domain contains one measurement property, that is responsiveness. Where available, all three quality domains will be assessed in this review.
Study designs
Quantitative and mixed-methods studies, and studies published in peer-reviewed journals or grey literature, will be included. Reference lists of all included full texts will be hand searched to identify additional eligible instruments and studies. Websites of any charitable and non-governmental organisations will also be searched for additional reports and papers to identify potential instruments. Both searches for reference lists and websites will be conducted by one reviewer, and any additional identified instruments and studies will be checked by the other reviewer. Review papers, editorials, or case studies will be excluded.
Setting
There will be no restrictions by type of setting.
Language
We will include studies and instruments developed and published in English. Studies that have not been translated into English will be excluded.
Data Extraction
Data will be extracted as follows.
Literature search and study selection
The titles and abstracts of studies retrieved from the database searches and those from additional sources will be screened independently in Covidence by two review authors (SM and JD) to identify studies that meet the inclusion criteria outlined above. The full text of these potentially eligible studies will be retrieved and independently assessed for eligibility by two review authors. Any disagreement between them over the eligibility of studies will be resolved through discussion with a third review author (MM). The interrater agreement will be assessed by calculating weighted k [9] and interpreted as very good (0.81–1.00), good (0.61–0.80), moderate (0.41–0.60), fair (0.21–0.40), and poor (0.00–0.20) [1].
A standardised form will be used to extract data from included studies in the systematic review. Two independent reviewers will carry out data extraction to reduce bias and errors [51]. Data abstracted will include demographic characteristics, instruments, measurement domains, sample size, sample age, and psychometric properties assessed (see Table 1 in Appendix A for the data extraction form). Reviewers will resolve disagreements by discussion, and an arbitrator (MM) will adjudicate disagreements. We will contact study authors to resolve any uncertainties [7].
Study quality assessment and data synthesis
Evaluation of methodological quality of studies
Studies evaluating the measurement properties of an assessment require high methodological quality with a low-risk bias to guarantee that appropriate conclusions are drawn about the properties of the measure [57]. Thus, it is important to evaluate those methodological qualities [12]. Two review authors will assess the methodological quality by applying the COnsensus-based Standards for the selection of health status Measurement INstruments (COSMIN) Risk of Bias checklist [36, 37]. The COSMIN checklist contains ten boxes with standards for patient-reported outcome measure (PROM) development (box 1) and for nine measurement properties, including content validity (box 2), structural validity (box 3), internal consistency (box 4), cross-cultural validity/measurement invariance (box 5), reliability (box 6), measurement error (box 7), criterion validity (box 8), hypotheses testing for construct validity (box 9), and responsiveness (box 10) [36, 37]. Refer to Table 2 in Appendix B for the definitions of all psychometric properties defined by the COSMIN statement [38, 39]. Only psychometric properties that are assessed in each included study will be completed since not all psychometric properties are assessed in all articles. An overall judgement will be provided on the methodological quality of the studies. We will use a four-point rating system where each standard within a COSMIN box will be rated as 4 = ‘very good’, 3 = ‘adequate’, 2 = ‘doubtful,’ or 1 = ‘inadequate’ to assess the quality of a study on that specific measurement property [36, 37]. The overall rating of each study will be determined by taking the lowest rating of any standard in the box (i.e. ‘the worst score counts’ principle) [58]; however, this makes it difficult to differentiate between subtle psychometric qualities of assessments. Therefore, a revised scoring system will be applied and presented as a percentage: poor (0–25%), fair (25.1–50.0%), good (50.1–75%), and excellent (75.1–100%) [10]. As some COSMIN items only have an option to rate as good or excellent, the total score for each psychometric property will be calculated using the formula detailed below, to accurately capture the quality of psychometric properties [38, 39]:
Two review authors will rate the methodological quality independently, and any discrepancies will be resolved by consensus.
Evaluation of psychometric properties of instruments
The result of each single study on a psychometric property will be rated against the updated criteria for good measurement properties [56] on which consensus will be achieved by two review authors. Each result will be rated as either sufficient (above the quality criteria threshold: +), insufficient (below the quality criteria threshold: −), or indeterminate (less robust data that do not meet the quality criteria: ?) using the predefined criteria for good psychometric properties [36, 37] (see Table 2 in Appendix C).
The evidence will be summarised, and the quality of the evidence (i.e. the total body of evidence used for the overall ratings on each psychometric property of an instrument) will be graded as high, moderate, low, or very low using the modified Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach (see [43]). The quality assessment will be done by two reviewers independently, and that consensus among the reviewers is reached, if necessary, with the help of a third reviewer.
Selection of instruments
The selection of instruments and recommendation of suitable instruments for future use will be based on a combining overall rating results of each psychometric property (step 2) and the grading results (step 3) [43]. Each instrument will be classified into three recommendation categories [36, 37]: (A) instruments that have potential to be recommended as the most suitable instrument for the construct and population of interest; (B) instruments that may have the potential to be recommended, but further validation studies are needed (i.e. instruments categorized not in A or C); and (C) instruments that should not be recommended. Justifications will be given as to why an instrument is placed in a certain category, and direction will be given on future validation work, if applicable [43].
Discussion
To the best of our knowledge, this is the first systematic review exploring the psychometric properties of self-report HRQoL and subjective wellbeing measures used by adolescents with ID. By providing evidence-based knowledge about measures being used in health and wellbeing research amongst this population, and more importantly how reliable and valid these measures are, the most suitable for use will be identified. This is crucial as clinicians, researchers, and service providers need information about the methodological quality and the characteristics of measures to make informed decisions about the most reliable and valid tool for a specific purpose. The findings of this study will contribute to the knowledge surrounding available and appropriate measures to use for measuring the HRQoL and subjective wellbeing of adolescents with ID, which are necessary to inform intervention development and future health policy.
One limitation of the systematic review process is the exclusion of studies that are not available in the English language, which may mean that articles identifying HRQoL and subjective wellbeing measures used with adolescents with ID based in non-English-speaking countries and not available in the English language will be excluded. The interpretability and feasibility of measurement tools have also been shown to be important in understanding the overall quality of an instrument [60]. However, as this study utilises the COSMIN criteria which does not provide an assessment of these constructs, they will not be appraised and thus is another limitation of our systematic review.
Availability of data and materials
The studies included in the review will be available from the corresponding author upon request.
Abbreviations
- HRQoL:
-
Health-related quality of life
- ID:
-
Intellectual disability
- COSMIN:
-
COnsensus-based Standards for the selection of health status Measurement INstruments
- PsycINFO:
-
Psychological information
- CINAHL:
-
Cumulative Index of Nursing and Allied Health Literature
- MEDLINE:
-
Medical Literature Analysis Retrieval System Online
- ERIC:
-
Education Resources Information Center
- GRADE:
-
Grading of Recommendations, Assessment, Development and Evaluations
- PRISMA-P:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PROM:
-
Patient-reported outcome measure
References
Altman DG. Practical Statistics for Medical Research. 1st ed: Chapman and Hall/CRC; 1990. https://doi.org/10.1201/9780429258589.
Boström P, Broberg M. Protection and restriction: a mixed-methods study of self-reported well-being among youth with intellectual disabilities. J Appl Res Intellect Disabil. 2018;31(1):164–76. https://doi.org/10.1111/jar.12364.
Boström P, Eriksson E. Design for self-reporting psychological health in children with intellectual disabilities. In: I Proceedings of IDC 2015: The 14th International Conference on Interaction Design and Children (s. 279-282). [2771896] Association for Computing Machinery, Inc. Proceedings of IDC 2015: The 14th International Conference on Interaction Design and Children; 2015. https://doi.org/10.1145/2771839.2771896.
Boström P, Johnels AJ, Thorson M, Broberg M. Subjective mental health, peer relations, family, and school environment in adolescents with intellectual developmental 482 disorder: a first report of a new questionnaire administered on tablet PCs. J Ment Health Res Intellect Disabil. 2016;9(4):207–31. https://doi.org/10.1111/jir.12432.
Bowling A. Do older and younger people difer in their reported well-being? A National Survey of Adults in Britain, Family Practice. 2011;28:145–55. https://doi.org/10.1093/fampra/cmq082.
Buckley N, Glasson EJ, Chen W, Epstein A, Leonard H, Skoss R, et al. Prevalence estimates of mental health problems in children and adolescents with intellectual disability: a systematic review and meta-analysis. Aust N Z J Psychiatry. 2020;54(10):970–84. https://doi.org/10.1177/0004867420924101.
Busse JW, Ebrahim S, Connell G, Coomes EA, Bruno P, Malik K, et al. Systematic review and network meta-analysis of interventions for fibromyalgia: a protocol. Unknown J. 2013;2(18). https://doi.org/10.1186/2046-4053-2-18.
Carlon S, Shields N, Yong K, Gilmore R, Sakzewski L, Boyd R. A systematic review of the psychometric properties of quality-of-life measures for school aged children with cerebral palsy. BMC Pediatr. 2010;10:81. https://doi.org/10.1186/1471-2431-10-81.
Cohen J, Humphreys LH. Weighted kappa: nominal scale agreement provision for scaled disagreement or partial credit. Psychol Bull. 1968;70(4):213–20. https://doi.org/10.1037/h0026256.
Cordier R, Speyer R, Chen YW, Wilkes-Gillan S, Brown T, Bourke-Taylor H, et al. Evaluating the psychometric quality of social skills measures: a systematic review. PLoS One. 2015;10(7):e0132299. https://doi.org/10.1371/journal.pone.0132299.
Davidson G, Irvine R, Corman M, Kee F, Kelly B, Leavey G, et al. Measuring the Quality of Life of People with Disabilities and their Families: Scoping Study Final Report; 2017. Department for Communities. https://www.communities-ni.gov.uk/publications/measuring-quality-life-disabled-people-and-their-families-scoping-study-final-report
De Vet HC, Terwee CB, Mokkink LB, Knol DL. Systematic reviews of measurement properties. In: De Vet HCW, Terwee CB, Mokkink LB, Knol DL, editors. Measurement in Medicine: A practical Guide. New York: Cambridge University Press; 2011. p. 275–314. https://doi.org/10.1080/10543406.2013.737220.
Delle Fave A, Brdar I, Freire T, et al. The eudaimonic and hedonic components of happiness: qualitative and quantitative findings. Soc Indic Res. 2011;100(2):185–207. https://doi.org/10.1007/s11205-010-9632-5.
Diener E. The science of well-being: the collected works of Ed Diener: Springer Science + Business Media; 2009. https://doi.org/10.1007/978-90-481-2350-6.
Dodge R, Daly AP, Huyton J, Sanders LD. The challenge of defining wellbeing. Int J Wellbeing. 2012;2(3):222–35. https://doi.org/10.5502/ijw.v2i3.4.
Douma J, Dekker MC, Verhulst FC, Koot HM. Self-reports on mental health problems of youth with moderate to borderline intellectual disabilities. J Am Acad Child Adolesc Psychiatry. 2006;45(10):1224–31. https://doi.org/10.1097/01.chi.0000233158.21925.95.
Durand M. The OECD better life initiative: how’s life? and the measurement of well-being. Rev Income Wealth. 2015;61(1):4–17. https://doi.org/10.1111/roiw.12156.
Emerson E. Inequalities and inequities in the health of people with intellectual disabilities. In: Oxford Research Encyclopedia of Global Public Health; 2021. https://doi.org/10.1093/acrefore/9780190632366.013.326.
Emerson E, Felce D, Stancliffe RJ. Issues concerning self-report data and population-based data sets involving people with intellectual disabilities. Intellect Dev Disabil. 2013;51(5):333–48. https://doi.org/10.1352/1934-9556-51.5.333.
Emerson E, Robertson J, Wood J. Emotional and behavioural needs of children and adolescents with intellectual disabilities in an urban conurbation. J Intellect Disabil Res. 2005;49(1):16–24. https://doi.org/10.1111/j.1365-2788.2005.00658.x.
Forgeard MJC, Jayawickreme E, Kern M, Seligman MEP. Doing the right thing: measuring wellbeing for public policy. Int J Wellbeing. 2011;1(1):79–106. https://doi.org/10.5502/ijw.v1i1.15.
Frauenberger C, Good J, Keay-Bright W. Designing technology for children with special needs: bridging perspectives through participatory design. CoDesign. 2011;7(1):1–28. https://doi.org/10.1080/15710882.2011.587013.
Hartley SL, MacLean WE Jr. A review of the reliability and validity of Likert-type scales for people with intellectual disability. J Intellect Disabil Res. 2006;50(11):813–27. https://doi.org/10.1111/j.1365-2788.2006.00844.x.
Haynes A, Gilmore L, Shochet I, Campbell M, Roberts C. Factor analysis of the self-report version of the strengths and difficulties questionnaire in a sample of children with intellectual disability. Res Dev Disabil. 2013;34(2):847–54. https://doi.org/10.1016/j.ridd.2012.11.008.
Hicks S, Newton J, Haynes J, Evans J. Measuring children’s and young people’s well-being: Office for National Statistics and BRASS, Cardiff University; 2011.
Ingerski LM, Modi AC, Hood KK, Pai AL, Zeller M, Piazza-Waggoner C, et al. Health-related quality of life across pediatric chronic conditions. J Pediatr. 2010;156(4):639–44. https://doi.org/10.1016/j.jpeds.2009.11.008.
Jahoda A, Wilson A, Stalker K, Cairney A. Living with stigma and the self-perceptions of people with mild intellectual disabilities. J Soc Issues. 2010;66(3):521–34. https://doi.org/10.1111/j.1540-4560.2010.01660.x.
Jardine J, Glinianaia SV, McConachie H, Embleton ND, Rankin J. Self-reported quality of life of young children with conditions from early infancy: a systematic review. Pediatrics. 2014;134(4):1129–48. https://doi.org/10.1542/peds.2014-0352.
Kipfer S, Pihet S. Reliability, validity and relevance of needs assessment instruments for informal dementia caregivers: a psychometric systematic review. JBI Database System Rev Implement Rep. 2019;18(4):740–2. https://doi.org/10.11124/JBISRIR-2017-003976.
Lifshitz H, Shtein S, Weiss I, Vakil E. Meta-analysis of explicit memory studies in populations with intellectual disability. Eur J Spec Needs Educ. 2011;26(1):93–111. https://doi.org/10.1080/08856257.2011.543535.
Longo E, Badia M, Orgaz MB, Gómez-Vela M. Comparing parent and child reports of health-related quality of life and their relationship with leisure participation in children and adolescents with cerebral palsy. Res Dev Disabil. 2017;71(586):214–22. https://doi.org/10.1016/j.ridd.2017.09.020.
Marques A, Peralta M, Santos T, Martins J, Gaspar de Matos M. Self-rated health and health-related quality of life are related with adolescents’ healthy lifestyle. Public Health. 2019;170:89–94. https://doi.org/10.1016/j.puhe.2019.02.022.
Mason SJ, Catto J, Downing A, Bottomley SE, Glaser AW, Wright P. Evaluating patient-reported outcome measures (PROMs) for bladder cancer: a systematic review using the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) checklist. BJU Int. 2018;122(5):760–73. https://doi.org/10.1111/bju.14368.
Michaelson J, Mahony S, Schifferes J. Measuring wellbeing: a guide for practitioners. London: New Economics Foundation; 2012.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. https://doi.org/10.1186/2046-4053-4-1.
Mokkink LB, de Vet H, Prinsen C, Patrick DL, Alonso J, Bouter LM, et al. COSMIN Risk of Bias checklist for systematic reviews of patient-reported outcome measures. Qual Life Res Int J Qual Life Asp Treat Care Rehab. 2018a;27(5):1171–9. https://doi.org/10.1007/s11136-017-1765-4.
Mokkink LB, Prinsen CAC, Patrick DL, Alonso J, Bouter LM, de Vet HCW, et al. COSMIN methodology for systematic reviews of patient-reported outcome measures (PROMs)-user manual (version 1.0); 2018b. p. 1–78.
Mokkink LB, Terwee CB, Knol DL, Stratford PW, Alonso J, Patrick DL, et al. The COSMIN checklist for evaluating the methodological quality of studies on measurement properties: a clarification of its content. BMC Med Res Methodol. 2010a;10:22. https://doi.org/10.1186/1471-2288-10-22.
Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J Clin Epidemiol. 2010b;63(7):737–45. https://doi.org/10.1016/j.jclinepi.2010.02.006.
Morris C, Janssens A, Shilling V, Allard A, Fellows A, Tomlinson R, et al. Meaningful health outcomes for paediatric neurodisability: stakeholder prioritisation and appropriateness of patient reported outcome measures. Health Qual Life Outcomes. 2015;13(87). https://doi.org/10.1186/s12955-015-0284-7.
Morrow AM, Hayen A, Quine S, Scheinberg A, Craig JC. A comparison of doctors’, parents’ and children’s reports of health states and health-related quality of life in children with chronic conditions. Child Care Health Dev. 2011;38(2):186–95. https://doi.org/10.1111/j.1365-2214.2011.01240.x.
Noonan RJ, Boddy LM, Fairclough SJ, Knowles ZR. Write, draw, show, and tell: a child-centred dual methodology to explore perceptions of out-of-school physical activity. BMC Public Health. 2016;16(326):1–19. https://doi.org/10.1186/s12889-016-3005-1.
Prinsen C, Mokkink LB, Bouter LM, Alonso J, Patrick DL, de Vet H, et al. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual Life Res Int J Qual Life Asp Treat Care Rehab. 2018;27(5):1147–57. https://doi.org/10.1007/s11136-018-1798-3.
Prinsen CA, Vohra S, Rose MR, Boers M, Tugwell P, Clarke M, et al. How to select outcome measurement instruments for outcomes included in a “core outcome set” - a practical guideline. Trials. 2016;17(1). https://doi.org/10.1186/s13063-016-1555-2.
Rees, G. & Main, G. (2015). Children’s views on their lives and well-being in 15 countries: A report on the Children’s Worlds Survey, 2013-14. https://www.york.ac.uk/inst/spru/research/pdf/ChildrensWorlds.pdf. Accessed 15 Mar 2022
Schalock RL, Borthwick-Duffy SA, Bradley VJ, Buntinx WH, Coulter DL, Craig EM, et al. Intellectual disability: Definition, classification, and systems of supports. Washington, DC: American Association on Intellectual and Developmental Disabilities; 2010.
Schalock RL, Luckasson R, Tassé MJ. Twenty questions and answers regarding the 12th edition of the AAIDD manual: intellectual disability: definition, diagnosis, classification, and systems of supports: American Association on Intellectual and Developmental Disabilities; 2021. https://www.aaidd.org/docs/default-source/intellectualdisability/12th-ed-twenty-questions-faq.pdf?sfvrsn=a6403421_4. Accessed 15 Mar 2022
Scholtes VA, Terwee CB, Poolman RW. What makes a measurement instrument valid and reliable? Injury. 2011;42(3):236–40. https://doi.org/10.1016/j.injury.2010.11.042.
Scott J, Wishart J, Currie C. Including children with intellectual disabilities/special educational needs into national child health surveys: a pilot study. J Appl Res Intellect Disabil. 2011;24(5):437–646. https://doi.org/10.1111/j.1468-3148.2010.00621.x.
Selwyn J, Wood M. Measuring Well-Being: A Literature review: University of Bristol; 2015. https://research-information.bris.ac.uk/ws/portalfiles/portal/41278115/Measuring_Wellbeing_FINAL.pdf. Accessed 15 Mar 2022
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ (Clinical research ed). 2015;350:g7647. https://doi.org/10.1136/bmj.g7647.
Shevell M. Global developmental delay and mental retardation or intellectual disability: conceptualization, evaluation, and etiology. Pediatr Clin N Am. 2008;55(5):1071–xi. https://doi.org/10.1016/j.pcl.2008.07.010.
Solans M, Pane S, Estrada MD, Serra-Sutton V, Berra S, Herdman M, et al. Health-related quality of life measurement in children and adolescents: a systematic review of generic and disease-specific instruments. Value Health. 2008;11(4):742–64. https://doi.org/10.1111/j.1524-4733.2007.00293.x.
Statham J, Chase E. Childhood Wellbeing: A brief overview. Loughborough: Childhood Wellbeing Research Centre; 2010.
Streiner DL, Norman GR. Health Measurement Scales: A Practical Guide to Their Development and Use. 4th ed. New York: Oxford University Press; 2008. https://doi.org/10.1093/acprof:oso/9780199231881.001.0001.
Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42. https://doi.org/10.1016/j.jclinepi.2006.03.012.
Terwee CB, Jansma EP, Riphagen II, de Vet HC. Development of a methodological PubMed search filter for finding studies on measurement properties of measurement instruments. Qual Life Res Int J Qual Life Asp Treat Care Rehab. 2009;18(8):1115–23. https://doi.org/10.1007/s11136-009-9528-5.
Terwee CB, Mokkink LB, Knol DL, Ostelo RW, Bouter LM, de Vet HC. Rating the methodological quality in systematic reviews of studies on measurement properties: a scoring system for the COSMIN checklist. Qual Life Res Int J Qual Life Asp Treat Care Rehab. 2012;21(4):651–7. https://doi.org/10.1007/s11136-011-9960-1.
The World Health Organization Quality of Life Assessment (WHOQOL). Development and general psychometric properties. Soc Sci Med. 1998;46(12):1569–85. https://doi.org/10.1016/s0277-9536(98)00009-4.
Thornicroft G, Slade M. Are routine outcome measures feasible in mental health? Qual Health Care. 2000;9(2):84. https://doi.org/10.1136/qhc.9.2.84.
Upton D, Upton P. Quality of Life and Well-Being. In: Psychology of Wounds and Wound Care in Clinical Practice. Cham: Springer; 2015. https://doi.org/10.1007/978-3-319-09653-7.
Upton P, Lawford J, Eiser C. Parent–child agreement across child health-related quality of life instruments: a review of the literature. Qual Life Res. 2008;17(6):895-913. https://doi.org/10.1007/s11136-008-9350-5.
White-Koning M, Arnaud C, Bourdet-Loubère S, Bazex H, Colver A, Grandjean H. Subjective quality of life in children with intellectual impairment--how can it be assessed? Dev Med Child Neurol. 2005;47(4):281–5. https://doi.org/10.1017/s0012162205000526.
Acknowledgements
Not applicable
Funding
A Baily Thomas Charitable Fund (TRUST/VC/AC/SG/5662-8764) funded SM’s research assistance. The funders did not fund protocol development and are not responsible for the content of the review protocol.
Author information
Authors and Affiliations
Contributions
SM led the conceptualisation of the protocol with input from all authors. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval is not required for this systematic review as no tests, measurements, or experiments were performed on humans as part of this work.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:.
PRISMA-P 2015 Checklist.
Additional file 2.
Search Strategy.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Maguire, S., Davison, J., McLaughlin, M. et al. Protocol for a systematic review exploring the psychometric properties of self-report health-related quality of life and subjective wellbeing measures used by adolescents with intellectual disabilities. Syst Rev 11, 81 (2022). https://doi.org/10.1186/s13643-022-01957-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-022-01957-w