
Abstract
Background
Sarcomas are a rare and heterogeneous group of tumors originating from mesenchymal or connective tissue. They represent less than 1% of all adult cancers. The etiology and epidemiology of sarcomas remain understudied and poorly understood. The main objective of our study was to systematically assess the association between various occupational exposures and risk of sarcomas.
Methods
We performed a systematic literature search using the PubMed, Scopus, EMBASE and Cochrane databases to identify relevant cohort and case–control studies. A meta-analysis method was applied on the incidence and mortality outcomes where the estimate with 95% confidence interval (CI) was obtained.
Results
We included a total of 50 publications in our systematic review and 35 in meta-analysis. For exposures to phenoxy herbicides and chlorophenols, the pooled odds ratio (OR) for sarcoma was 1.85 (95% CI: 1.22, 2.82), based on 16 studies with 2254 participants, while the pooled standardized mortality ratio was 40.93 (95% CI 2.19, 765.90), based on 4 cohort studies with 59,289 participants. For exposure to vinyl chloride monomers the pooled risk ratios for angiosarcoma of the liver and other STS were 19.23 (95% CI 2.03, 182.46) and 2.23 (95 CI 1.55, 3.22) respectively based on 3 cohort studies with 12,816 participants. Exposure to dioxins was associated with an increased STS mortality; the pooled standardized mortality ratio was 2.56 (95% CI 1.60, 4.10) based on 4 cohort studies with 30,797 participants. Finally, woodworking occupation was associated with an increased risk of STS with the pooled OR of 2.16 (95% CI 1.39, 3.36).
Conclusions
Our findings suggest a positive association between higher exposure to dioxins and increased mortality from STS, between cumulative exposure to vinyl chloride monomers and increased mortality from angiosarcoma of the liver and STS, and between woodworking occupation and STS incidence. These findings were all statistically significant.
Similar content being viewed by others


Background
Sarcomas constitute a rare and heterogeneous group of tumors with over 70 different subtypes, originating from connective and mesenchymal tissue. They represent less than 1% of all adult cancers [1]. Due to the complexity and rarity of sarcomas, their etiology and epidemiology remain poorly understood [2].
Exposures to pesticides are amongst one of the most extensively studied exposures in epidemiological studies. Considerable attention has been focused on potential health effects of agricultural and non-agricultural exposures to phenoxy herbicides and chlorophenols as excess incidence and mortality for some specific cancers, including soft tissue sarcomas (STS), has been observed in exposed workers. The association between these compounds and STS was first reported in the Swedish observational study by Hardell et al. in 1977 [3]. The association was then supported by other Swedish case–control studies conducted in the 1970s and 1980s. A meta-analysis of four Swedish case–control studies confirmed significantly increased risks of STS from exposures to these compounds. Odds ratio (OR) 2.7 (95% confidence Interval (CI) 1.9, 4.7) and OR 3.3 (95% CI 1.8, 6.1) were obtained for phenoxyacetic acids and chlorophenols respectively [4]. However, multiple subsequent case–control and cohort studies in several countries have demonstrated conflicting results.
Since 1969, some of the herbicides including 2,4,5-trichlorophenoxyacetic acid (2,4,5-T) were banned in Europe and the United States (US) due to contamination by 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) [5]. The latest update from the International Agency for Research on Cancer (IARC) published in 1987 concluded that there was a limited evidence for carcinogenicity to humans from chlorophenoxy herbicides (Group 2B) and inadequate evidence for carcinogenicity to animals from 2,4-dichlorophenoxyacetic acid (2,4-D) and 2,4,5-T [5]. Another herbicide—Agent Orange, a mixture of 2.4.5-T and 2,4-D—was studied in Vietnam War veterans as it was widely used as a defoliant during the Vietnam War [6]. The US National Academies of Sciences, Engineering and Medicine linked exposure to Agent Orange to certain cancer precursors and cancers, including soft-tissue sarcoma, in its most recent report titled Veterans and Agent Orange: Update 11 (2018) [7].
STS is one of the few specific tumors linked to dioxins. TCDD, which is considered as the most potent dioxin, is classified as a group 1 carcinogen by the IARC. This is based on sufficient evidence in experimental animals and limited evidence in humans [8]. While the human epidemiological evidence showed an excess of all cancer mortality in four highly exposed industrial cohorts to dioxins [9,10,11,12], the association of exposure to dioxins and sarcomas was inconsistent.
Vinyl chloride monomer (VCM) is another compound studied in relation to angiosarcoma of the liver (ASL) and other soft-tissue sarcomas. The first reports on cases of ASL among workers occupationally exposed to VCM appeared in 1974 [13,14,15,16]. The IARC classifies VCM as a group 1 carcinogen, with sufficient evidence of carcinogenicity in humans [17].
Various occupational exposures have been studied to examine sarcoma incidence and mortality with inconsistent results. We aimed to include new epidemiological evidence in our systematic review and meta-analysis. The objective of this study is to explore the incidence and mortality of sarcomas in adult population with various occupational exposures.
Methods
Search strategy
We conducted a systematic literature search using the PubMed, Scopus, Embase, and Cochrane databases, as well as using backward citation tracking, to search for all reports of cohort or case–control studies that provided data on the risk of sarcoma in relation to occupational factors published up to May 2021. The literature review and meta-analysis was carried out and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) recommendations [18] (Supplementary table 8). The systematic review protocol and search strategy were registered online (PROSPERO May 7, 2020: CRD420201809).
The literature search was developed by two medical research librarians (GA and DG). In order to identify relevant studies, we used terms that combined various occupational exposure types with outcomes of interest—incidence and mortality of sarcomas. The full search strategy is available in supplementary table 1.
Study selection
After removal of duplicates, two authors (DE and AV) independently identified studies eligible for inclusion based on an initial screen of reference titles and abstracts. The inclusion and exclusion criteria for this review are provided in Table 1. Studies found to be relevant to the topic of interest were shortlisted. The shortlisted publications were retrieved for an independent full-text article review and were assessed for the eligibility criteria by the same authors. The articles that met all inclusion criteria were included for final systematic review. Any discrepancies during the search process were resolved by the lead investigator (AG). We used EndNote for management of references.
Data extraction and quality assessment
Two authors (DE and AV) independently extracted data using a standardized form. The publications that met the inclusion criteria were abstracted onto tables, separately for cohort and case–control studies. The data included author, year of publication, country, time period covered, exposure duration, exposure type, description of study and reference groups, outcome of interest, and risk estimates for relevant outcomes. The effect estimates that were abstracted were odds ratio (OR), risk ratio (RR), standardized incidence ratio (SIR) or standardized mortality ratio (SMR) estimates, and their 95% confidence intervals. Studies that did not report the later were excluded, and no crude numbers were abstracted to compute effect estimates. For cohort studies, risk estimates took the form of standardized mortality or risk ratios. For case–control studies, risk estimates were presented as odds ratios. The quality of case–control and cohort studies was assessed using the Newcastle–Ottawa Scale [19]. Cofounders in the studies were included as part of our risk of bias assessment. When cofounders were not adjusted for in the study the outcome risk of bias was judged as high.
Data synthesis and statistical analysis
We used Microsoft Excel for data abstraction. The primary meta-analyses were conducted to assess the association between various occupational exposures and sarcoma incidence and mortality. Pooled effect estimates of ORs, RRs, SIRs or SMRs, and 95% CI were calculated using a random-effects model. Forest plots were generated, displaying the individual study effects and the pooled estimate effect. Heterogeneity between individual studies was assessed by the chi-square test (by the Q statistic) and I2 statistic, which represents the amount of variability in the meta-analysis attributed to study heterogeneity [20]. An I2 of < 25% was considered as low-level heterogeneity and 25 to 50% as moderate level. P ≤ 0.10 and/or I2 > 50% indicated significant heterogeneity [21]. All analyses were conducted in SAS v9.4 (Cary, NC).
Results
Study characteristics
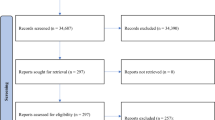
Our literature search identified an initial 3961 publications of which 92 duplicate articles were removed. We excluded 3329 articles based on title and abstract screening. We retrieved the 546 remaining articles for detailed full article screening for specific inclusion and exclusion criteria as well as for overlapping data. For duplicate reports, we selected the studies with larger sample size and longer follow-up time. A total of 50 studies met full eligibility criteria to be included in qualitative data synthesis and 35 studies were included in meta-analysis (Fig. 1). Fifteen studies were not included in the meta-analysis because the described exposures or occupations were not studied in any other study.

PRISMA flow diagram
Exposure to phenoxy herbicides and chlorophenols
We included 17 case–control [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38] and 10 cohort studies [38,39,40,41,42,43,44,45,46,47] that provided data on occupational exposures to phenoxy herbicides and chlorophenols. We presented the characteristics of individual studies in Tables 2 and 3 and the findings of these studies in supplementary tables 2 and 3.
The earlier study conducted in 1979 by Hardell et al. in Northern Sweden demonstrated a six-fold increased risk of STS with exposure to phenoxy herbicides [22]. A southern Swedish case-referent study [23] with a large number of histologically proven cases (n = 110) confirmed the earlier findings of an increase of the same magnitude in the risk for STS after exposure to phenoxy herbicides and chlorophenols. The third Swedish study [31] also concluded that occupations which may imply exposure to phenoxy herbicides and chlorophenols, such as gardeners and railroad and wood workers, had an increased risk of STS.
Studies from New Zealand [25] and Australia [34] failed to confirm the Swedish findings. This study in New Zealand was conducted on a similar scale as the Swedish studies with regard to the number of STS cases. However, the study design differed from the Swedish studies by the control group consisting of other cancers. In a large population-based study conducted in six Canadian provinces with diverse agricultural practices Pahwa et al. also came to conclusion that STS was not associated with exposure to phenoxy herbicides [37]. The study limitations were low response rate and potential for exposure recall-bias. In a population-based study from Northern Italy, Vineis et al. found an increased risk of STS in female rice weeders, but not in male [48]. In another study from Italy, which was hospital-based, Franceschi et al. found no significant association of STS risk with exposure to herbicides [33]. Both Italian studies were limited by low statistical power and possible recall-bias. Two population-based studies undertaken in Kansas (Hoar et al., 1986) and Western Washington (Woods et al., 1987), states with high use of herbicides, found no association between agricultural herbicide use and the occurrence of STS [26, 30].
In contrast, the results of the largest US population-based study (Hoppin et al., 1998) that included 295 male STS cases from eight population-based cancer registries supported the hypothesis of an association of sarcoma with exposure of chlorophenols in cutting oils and wood preservation [36]. The findings of two-nested case controlled studies (Kogevinas et al., 1995) within a large international cohort including 21,183 workers, with substantial exposure to herbicides in production workers and sprayers also reported excess risk of STS [35].
As for Agent Orange, in a hospital-based study, Kang et al. concluded that there was no significant association of STS and previous military service in Vietnam [27]. However, the authors noted that the absence of positive association might be due to insufficient observation time. Another study from the same group of researchers compared a total of 217 STS cases to 599 controls for Vietnam Service [28]. The study revealed that Vietnam veterans in general did not have an increased risk of STS when compared to those men who had never been in Vietnam. However, an increased risk of STS was observed in the subgroups of veterans, such as combat veterans, combat veterans with MOSC (military occupational specialty category), and those who served within military region III, the area where Agent Orange spray was reported to be excessive.
In a cohort study of workers in manufacture of phenoxy herbicides in Denmark, findings of Lynge et al. supported the earlier Swedish observations of an excess risk of STS following exposure to herbicides [49]. In contrast, in the Swedish study with 15% estimated risk of exposure to phenoxy herbicides in agricultural or forestry workers with large numbers of STS cases (n = 331), Wiklund et al. reported no increased risk of STS [39]. The findings from two other cohort studies of Swedish licensed pesticide applicators [40] and Swedish female farmers [43], presented by the same group of authors, were consistent with the hypothesis that exposure to these compounds does not increase risk of STS. These studies were limited by lack of information on exact exposure to herbicides and consisted of cohorts with assumed occupational exposure to phenoxy acids. Data from ongoing large prospective cohort study of farmers and pesticide applicators in North Carolina and Iowa called the Agricultural Health Study also did not show increased risk of STS [50]. Similarly, Fleming et al. found no cases of STS in a large retrospective cohort study of 33,658 pesticide applicators from Florida [46].
Increased mortality from STS was on the border of statistical significance among workers at a plant in Alabama manufacturing agricultural and other chemicals, based on small numbers (n = 3) [42]. Similarly, in the study of rice growers in Northern Italy Gambini et al. were unable to come to any firm conclusion as there was only one case of death from STS with SMR as high as 1808.5 due to the very low expectation in this category [44].
In a large international cohort of chemical workers from ten courtiers in manufacturing agricultural and other chemicals, set up by the IARC, Saracci et al. found a six-fold excess of STS in the cohort as a whole and a nine-fold excess among sprayers 10–19 years from first exposure [41].
Exposure to dioxins
We included 4 cohort studies that provided data on occupational exposures to dioxins [51,52,53,54]. The studies evaluating non-occupational exposures and industrial accidents were not included. We presented the characteristics of the individual studies in Table 4 and the findings of these studies in supplementary table 4.
The largest study was a historical cohort of 21,863 male and female workers from 12 countries coordinated by the IARC and followed for 70 years [51]. In this study, Kogevinas et al. observed twofold excess mortality for STS among workers exposed to herbicides contaminated with dioxins, subjects with a long duration of exposure, and persons first employed before 1965. The validity of this study may have been influenced by a possibility of exposure misclassification and inaccurate STS diagnosis on death certificates. Steenland et al. found excess mortality in the highest exposed chemical workers at 12 US plants [52]. Bodner et al. reported a greater than expected rate for STS in another US cohort of chemical production workers exposed to substantial levels of dioxin [53]. Collins et al. also observed an increased mortality rate from STS with dioxin exposure in the latest update from the largest single plant cohort study of workers at the Dow Chemical Company in Michigan with a follow-up period of 62 years [54]. Limitations of this study were the potential for misclassification of sarcoma diagnosis and the small number of sarcoma cases.
Exposure to vinyl chloride monomers
We included 5 cohort studies [55,56,57,58,59] observing the relationship to mortality from ASL. Three of these studies also evaluated the association between VCM and other STS. Two multicenter epidemiologic studies combined populations of exposed workers included in previous investigations and extended the follow-up. We presented the characteristics of the individual studies in Table 5 and the results of these studies in supplementary table 5.
The European multicenter study (Ward et al., 2001) [56] was an extended follow-up of a cohort organized by Simonato et al. [60] and included the population previously studied in the UK [61, 62], Sweden [63], and Norway [64]. The results were generally consistent with the original findings in which the excess from liver cancer was related to time since first exposure, duration of employment and estimated quantitative exposures. A strong relation was observed between cumulative exposure to VCM and occurrence of liver cancer. The relationship was even more evident when only ASL was analyzed.
Mundt et al. aimed to evaluate exposure–response relationships for mortality from ASL and hepatocellular carcinoma (HCC) in the North American cohort mortality data for men engaged in the manufacture of VC or PVC resin at any of 35 factories in the US [58]. The association between VCM and ASL reported in this cohort 44 years ago persisted in the updated study and was strongest among most highly exposed workers. These findings were consistent with those reported in the European study (Ward et al., 2001). The median latency for ASL deaths was 36 years.
Collins et al. reported 15 cases of ASL in the most recent update of the Dow chemical company diseases registry for ASL [65]. Thirteen ASL cases were at a single plant with high VCM exposure before 1974, which could indicate that exposures were higher at this location than the other locations. Fedeli et al. reported 9 deaths from ASL in a cohort of 1658 workers involved in VCM production and polymerization in northeastern Italy [59]. Latency among ASL cases was 32 years and the risk continued to increase through the highest levels of cumulative exposure. Wong et al. found increased mortality from HCC but no death caused by ASL in the retrospective cohort study from Taiwan [57]. This could be due to much lower levels of VCM exposure in Taiwanese workers compared to North American and Western European workers.
Other occupation exposures
We included 6 cohort studies [66,67,68,69,70,71] and 12 case–control studies [31, 33, 37, 72,73,74,75,76,77,78,79] that provided data on various other occupational exposures and sarcoma incidence and mortality. We presented the characteristics of the individual studies in Tables 6 and 7and the results of these studies in supplementary tables 6 and 7.
Zahm et al. demonstrated an association between woodworking occupations and increasing risk of STS in a population-based case–control study in Kansas[74]. Hoar et al. found increased risk of STS with exposure to insecticides used on animals but not on crops [72]. Similarly, Pahwa et al. observed a statistically significant increased risk of STS with exposure to insecticides—aldrin and diazinon in Canadian population-based case–control study [77]. STS risk was higher among the farmers with longer duration of exposure, farmers who themselves mixed or applied insecticides to animals and failed to use any protective equipment.
In a large historical cohort of Danish paper mill workers, Rix et al. found an increased risk of STS female workers with a high risk among paper sorters employed in manual sorting and packing [69]. Another cohort form the same authors found an excess risk of STS in Danish sulfite pulp workers [70].
In a large case–control study from six Canadian provinces, Hossain et al. found an increased risk for STS associated with an exposure to radium, longest-held job as a machinist, short-term job as chicken farm worker, pulp and paper industry worker, and apartment complex worker [79].
A large population-based study from the US reported by Hoppin et al. demonstrated excess risk of different sarcoma subtypes from various occupational exposures [75]. In this study, self-reported herbicide use and exposure to chlorophenols and cutting oil was associated with malignant fibrohistiocytic sarcoma and leiomyosarcoma, wood-related exposures with leiomyosarcoma, and meatpacking with dermatofibrosarcoma protuberans. In another large population-based case–control study from the US, Briggs et al. showed that exposure to wood dust was associated with increased risk of STS in African American men but not in white men [76]. Race-specific occupational risk factors evident only among African American men may represent racial disparities in levels of exposures to carcinogens.
In a case–control study from Sweden, Wingren et al. demonstrated that gardeners, railroad workers, unspecified chemical workers, workers in contact with wood, and construction workers with exposure to asbestos and pressure impregnating agents had an increased risk of STS [31]. In a case–control study from Northern Italy, Franceschi et al. came to the conclusion that workers with exposure to chemical agents, benzene, or other solvents had higher risk of developing STS [33]. Excess mortality in bone and soft tissue sarcomas was detected in a large cohort of US and Russian “Mayak” nuclear facility workers exposed to plutonium [71]. In a series of case-referent studies from the New Zealand, Pearce et al. observed that the risk for STS was elevated in meat workers [73]. In the study conducted in England and Wales, Balarajan et al. found no increased risk of STS among farmers and allied workers. However, when each occupational subgroup was analyzed separately, the excess risk found was limited to farmers, farm managers, and market gardeners [80]. In the largest international case–control study, conducted in nine European countries, Merletti et al. found increased risk of bone sarcoma in woodworkers (particularly carpenters), blacksmiths, toolmakers and machine-tool operators, workers employed in manufacture of equipment and machinery industry, construction workers, and workers who ever used pesticide [78].
Results of meta-analysis
Exposure to phenoxy herbicides and chlorophenols
We conducted a meta-analysis of 16 case–control studies, involving 2254 sarcoma cases and 24,148 con1trols (Fig. 2). The pooled OR was 1.85 (95% CI 1.22, 2.82), P = 0.008, indicating significant positive association between exposure to phenoxy herbicides and chlorophenols and incidence of sarcoma. There was significant heterogeneity across the individual studies I2 = 79.0%, P ≤ 0.001.

Forest plot of odds ratio (OR) for exposure to phenoxy herbicides and chlorophenols and sarcoma incidence
Four cohort studies involving 11 sarcoma cases and 59,289 participants assessed the association between exposure to phenoxy herbicides and chlorophenols and sarcoma mortality (Fig. 3). The pooled SMR was 40.93 (95% CI 2.19, 765.90), P = 0.013, indicating a statistically significant positive association. However, there was significant heterogeneity across the individual studies I2 = 93.7%, P ≤ 0.001.

Forest plot of standardized mortality ratio (SMR) for exposure to phenoxy herbicides and chlorophenols and sarcoma mortality (cohort studies)
Based on meta-analysis of 3 cohort studies, involving 379,864 participants and 343 sarcoma cases, assessing exposure to phenoxy herbicides and chlorophenols and sarcoma incidence, the pooled RR was 0.90 (95% CI 0.81, 1.00), P = 0.0489, indicating no association (Fig. 4). There was no evidence of heterogeneity across the included studies, I2 0.0%, P = 1.00. Two studies included in this meta-analysis, Wiklund et al. [39]and Wiklund et al. [40], that showed no association between exposure to phenoxy herbicides and chlorophenols and STS were much larger in size and tended to drive the results of meta-analysis. One explanation for the lack of any excess of sarcoma in these studies might be that both studies were register-based studies consisted of cohorts of agricultural and forestry workers and pesticide applicators with assumed occupational exposures to phenoxy acids and lacked individualized exposure data.

Forest plot of risk ratio (RR) for exposure to phenoxy herbicides and chlorophenols and sarcoma incidence (cohort studies)
Based on 2 cohort studies, involving 103,078 participants and 31 cases of sarcoma, the pooled SIR was 0.63 (95%CI 0.44, 0.89), P = 0.010, indicating no association between exposure to phenoxy herbicides sarcoma incidence (Fig. 5). There was no evidence of heterogeneity across the included studies, I2 0.0%, P ≤ 0.001.

Forest plot of standardized incidence ratio (SIR) for exposure to phenoxy herbicides and chlorophenols and sarcoma incidence (cohort studies)
Exposure to dioxins
A meta-analysis of 4 cohort studies involving 30,797 participants evaluated the association between exposure to dioxins and STS mortality (Fig. 6). There were 14 deaths due to STS in these studies. The pooled SMR was 2.56 (95% CI 1.60, 4.10), P ≤ 0.001, indicating a statistically significant positive association between exposure to dioxins and STS mortality. There was no evidence of heterogeneity across the included studies, I2 0.0%.

Forest plot of standardized mortality ratio (SMR) for occupational exposure to dioxins and soft tissue sarcoma (STS) mortality (cohort studies)
Exposure to vinyl chloride monomers
We conducted a meta-analysis of 3 cohort studies, including 12,816 participants. There were 110 deaths from STS in these studies. The RR of ASL was increased in all studies included in meta-analysis. The pooled RR was 19.23 (95% CI 2.03, 182.46, P = 0.010), indicating a statistically significant positive association between exposure to VCM and ASL mortality (Fig. 7). There was significant heterogeneity across the individual studies I2 = 94.4%, P ≤ 0.001.

Forest plot of risk ratio (RR) for exposure to vinyl chloride monomer (VCM) and mortality of angiosarcoma of the liver (ASL)
Excess death due to connective and soft tissue cancer was observed and was strongest amongst highly exposed workers in tree cohort studies including 12,816 participants (Fig. 8). There were 20 deaths due to connective and soft tissue cancer in these studies. The pooled SMR was 2.23 (95 CI 1.55, 3.22), P < 0.001, indicating statistically significant positive association between VCM exposure and STS. The study results were adequately similar, as I2 = 0.0%.

Forest plot of standardized mortality ration (SMR) for exposure to vinyl chloride monomer (VCM) and mortality of other soft tissue sarcomas
Other occupational exposures
With regard to other occupational exposures, population-based studies reported increased sarcoma incidence with exposure to insecticides used on animals, benzene, radium, cutting oil, and wood dust, in female paper sorters, gardeners, railroad workers, farmers, farm managers, long-term jobs as a machinist, short-term jobs as chicken farm workers, temporary jobs at apartment complexes, pulp and paper industry workers, meatpacking and woodworking occupations, and sulfite mill and nuclear facility workers.
Meta-analysis of 4 case–control studies with 8593 participants assessed the association between STS incidence and occupational exposure to woodworking and wood dust (Fig. 9). The pooled OR was 2.16 (95% CI 1.39, 3.36), P < 0.001, indicating a statistically significant positive association. There was no significant heterogeneity across the studies, I2 = 0.0%.

Forest plot of odds ratio (OR) for occupational exposure to woodworking and soft tissue sarcoma (STS) incidence
Discussion
Our systematic review and meta-analysis included a comprehensive review of the PubMed, Scopus, EMBASE, and Cochrane databases, allowing for a considerable amount of data collection. This is the largest study to date that evaluates the association between various occupational exposures and sarcoma incidence and mortality. Our study has multiple strengths. We have included studies from various geographical areas from several countries that add to the generalizability of our results. A broad mix of studies was analyzed, including different populations and a wide variety of occupational exposures. The total amount of participants was large and different study designs were included. Many studies confirmed their sarcoma diagnosis with review of histology, and long time for follow-up was preferred. The majority of included studies were rated between moderate and high quality of evidence (supplementary table 9).
However, there were several limitations noted both in case–control and cohort studies that contributed to the inconsistency of outcomes across the studies. We believe this inconsistency is most likely due to limitations faced with study design based on questionnaires that are prone to recall bias, among other biases including measurement bias from lack of accurate exposure levels among the different studies. These limitations were specifically noted in regard to exposures to phenoxy herbicides and chlorophenols. A number of studies have been limited by inadequate exposure information and difficulties in determining type, duration, and level of exposure in different jobs and different countries. The studies, in general, also lacked information on specific individual exposure level, on the proportion of exposed workers, or extent of exposure [39, 40, 43]. The occupational exposure level in the majority of studies was determined based on job title and exposure questionnaires [50]. In some studies, information on occupation was obtained from death certificates, enabling exposure misclassification bias [51]. Such misclassification of exposure may lead to either underestimation or overestimation of the relative risk, if not a systematic bias [81, 82]. In other studies, exposure information was collected from the study participants directly or from the next-of-kin, possibly allowing for recall bias [25, 34, 37]. Other reasons of inconsistency between the results of studies from different countries could be attributed to differences in type of herbicides used, level of dioxin contaminants, and climatic differences resulting in variability in agricultural practices [25, 30]. There is a possibility that in studies with positive results, the study population was exposed to higher cumulative levels of compounds or dioxin contaminants that were part of the commercial preparations [22]. Exposure risk evaluation for specific agents can be assessed only partially as workers often had simultaneous exposures to several different pesticides, engine fuels and exhausts, organic and inorganic dusts, UV radiation, heat, noise, vibration, mycotoxins, zoonotic viruses, and other biological agents [83, 84]. It would not be possible in the studies to identify a group of workers solely exposed to one specific agent.
Other possible reasons for a lack of consistency between the results may be differences between the study populations with respect to other uncontrolled confounding factors such as environmental conditions, lifestyle, and inherited factors. Main confounding factors considered in these studies were age and sex. Many studies excluded female workers due to small numbers and rarity of involvement in highly exposed occupations. Therefore, subgroup analysis based on gender was not performed due to population selection bias.
A number of cohort studies reported a limited statistical power and wide confidence interval, owing to the small number of sarcoma cases and low response rate [44, 54]. In some studies, the relative risk may have been underestimated because of the shorter follow-up period [27, 28]. The median latency period for the chemical induction of solid malignant tumors is generally considered to be in the range of 15–30 years [85, 86].
Another challenge across many studies was reliable and complete ascertainment of the cancers of main interest. Survival rates for sarcoma could be relatively high [87], meaning that cases will not necessarily be picked up from death certificates. Moreover, deaths from sarcoma have been often coded as cancers of the anatomical site at which they occur rather than as sarcoma specifically [88]. Sarcomas often present diagnostic difficulties that contribute to more misclassification bias [1]. The possibly of missing sarcoma cases due to incompleteness of cancer registration in many countries especially during early years of follow-up also could have influence on study outcomes. In several studies, death certificates were used to identify sarcoma cases, which add risk for misclassification of sarcoma and underestimation of sarcoma cases [51, 54].
With regard to VCM exposure, the included studies differed in design, size, length of follow-up, and covered time periods. Almost all studies concluded that the risk of malignant liver neoplasms, particularly ASL, was increased by exposure to VCM. However, the actual mechanisms of action of inducing ASL by VCM are unclear. The studies reported the highest incidence of ASL in workers of VCM production and polymerization. Some of the later observations report a dramatic decline in ASL cases from the late 1970s as a result of much stricter regulations implemented in North America and Western European countries to reduce VCM exposure. Most studies were unable to provide direct measurement of exposure to VCM and quantitative VCM exposure measure or analysis of liver cancer subtypes. The European multicenter study was the only study that provided a quantitative estimate of VCM exposure based on calendar-period-specific exposure, job, and plant. Some studies also noted difficulties in assessment of VCM as a cause of ASL or other STS because of lack of histological or other definitive clinical information to discriminate HCC from ASL. In most studies, the cause of death was obtained from death certificates that often incorrectly stated specific cause from liver cancer death and could have underestimated the number of cases of ASL and thus enabling misclassification bias. Only some studies provided SMR or SIR for ASL due to the rarity of the disease in the general population.
The results of our meta-analysis indicate that higher exposure to dioxins was associated with STS. However, the results were based on small number of STS due to rarity of sarcomas. Overall, included studies were good quality, with a large number of participants, long follow-up, and no significant heterogeneity across the included studies, which strengthen the validity of our findings.
Various other agricultural or non-agricultural exposures have been found to be associated with an increased risk of bone or soft-tissue sarcomas. However, due to limited number of studies, we were unable to conduct quantitative analysis for these occupations or exposures.
Conclusion
Overall, our findings from the meta-analysis suggest a statistically significant positive association between higher exposure to dioxins and increased mortality from STS, between cumulative exposure to VCM and increased mortality from ASL and other sarcomas in organs other than the liver, and between woodworking occupation and exposure to wood dust and sarcoma incidence. Notwithstanding the high heterogeneity of the studies, workers exposed to phenoxy herbicides and chlorophenols may experience an increased incidence of sarcoma based on meta-analysis of case–control studies. Meta-analysis of cohort studies for exposure to chlorophenols and phenoxy herbicides, however, produced conflicting results.
Conducting new large case–control studies using better characterizations of exposure and extending follow-up of previously assembled cohort studies would be effective ways at reducing uncertainties and could provide more evidence on other risk factors reported in our study.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Abbreviations
- ASL:
-
Angiosarcoma of the liver
- CI:
-
Confidence interval
- HCC:
-
Hepatocellular carcinoma
- IARC:
-
International Agency for Research on Cancer
- OR:
-
Odds ratio
- RR:
-
Risk ratio
- STS:
-
Soft-tissue sarcoma
- SIR:
-
Standardized incidence ratio
- SMR:
-
Standardized mortality ratio
- VCM:
-
Vinyl chloride monomer
- 2,4,5-T:
-
2,4,5-Trichlorophenoxyacetic acid
- TCDD:
-
2,3,7,8-Tetrachlorodibenzo-p-dioxin
References
Florou V, Nascimento AG, Gulia A, de Lima LG, Jr. . Global health perspective in sarcomas and other rare cancers. Am Soc Clin Oncol Educ Book. 2018;38:916–24.
Burningham Z, Hashibe M, Spector L, Schiffman JD. The epidemiology of sarcoma. Clin Sarcoma Res. 2012;2(1):14.
Hardell L. Soft tissue sarcomas and exposure to phenoxyacetic acids and cancer. Lakartidningen. 1977;1977(74):2753–4.
Hardell L, Eriksson M, Degerman A. Metaanalysis of 4 Swedish case-control studies on exposure to pesticides as risk-factor for soft-tissue sarcoma including the relation to tumor-localization and histopathological type. Int J Oncol. 1995;6(4):847–51.
Humans IWGotEoCRt, Organization WH: Overall evaluations of carcinogenicity: an updating of IARC monographs volumes 1 to 42, vol. 7: World Health Organization; 1987.
Stellman JM, Stellman SD. Agent Orange during the Vietnam War: the lingering issue of its civilian and military health impact. In.: American Public Health Association; 2018.
Hertz-Picciotto I, Berliner N, Bernstein WB, Carvan III MJ, Chakravarti A, Dolinoy DC, Fox MA, Kelsey KT, Kile ML, Olshan AF: Veterans and Agent Orange: Update 11 (2018)(2018). 2018.
IARC: IARC Monogr Eval Carcinog Risk Hum, Vol. 69, Polychlorinated dibenzo-para-dioxins and polychlorinated dibenzofurans. 1997.
Fingerhut MA, Halperin WE, Marlow DA, Piacitelli LA, Honchar PA, Sweeney MH, Greife AL, Dill PA, Steenland K, Suruda AJ. Cancer mortality in workers exposed to 2,3,7,8-tetrachlorodibenzo-p-dioxin. N Engl J Med. 1991;324(4):212–8.
Becher H, Flesch-Janys D, Kauppinen T, Kogevinas M, Steindorf K, Manz A, Wahrendorf J. Cancer mortality in German male workers exposed to phenoxy herbicides and dioxins. Cancer Causes Control. 1996;7(3):312–21.
Hooiveld M, Heederik DJ, Kogevinas M, Boffetta P, Needham LL, Patterson DG Jr, Bueno-de-Mesquita HB. Second follow-up of a Dutch cohort occupationally exposed to phenoxy herbicides, chlorophenols, and contaminants. Am J Epidemiol. 1998;147(9):891–901.
Ott MG, Zober A. Cause specific mortality and cancer incidence among employees exposed to 2,3,7,8-TCDD after a 1953 reactor accident. Occup Environ Med. 1996;53(9):606–12.
Creech JL Jr, Johnson MN. Angiosarcoma of liver in the manufacture of polyvinyl chloride. J Occup Med. 1974;16(3):150–1.
Tabershaw IR, Gaffey WR. Mortality study of workers in the manufacture of vinyl chloride and its polymers. J Occup Med. 1974;16(8):509–18.
Block JB. Angiosarcoma of the liver following vinyl chloride exposure. JAMA. 1974;229(1):53–4.
Falk H, Heath C Jr, Carter C, Wagoner J, Waxweiler R, Stringer W. Mortality among vinyl-chloride workers. The Lancet. 1974;304(7883):784.
Cancer IAfRo, Cancer IAfRo: Overall evaluations of carcinogenicity: an updating of IARC monographs volumes 1 to 42: IARC Lyon, France:; 1987.
Moher D, Liberati A, Tetzlaff J, Altman DG: Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009, 6(7):e1000097.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5.
Gagnier JJ, Morgenstern H, Altman DG, Berlin J, Chang S, McCulloch P, Sun X, Moher D. Consensus-based recommendations for investigating clinical heterogeneity in systematic reviews. BMC Med Res Methodol. 2013;13:106.
Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–58.
Hardell L, Sandstrom A. Case-control study: soft-tissue sarcomas and exposure to phenoxyacetic acids or chlorophenols. Br J Cancer. 1979;39(6):711–7.
Eriksson M, Hardell L, Berg NO, Möller T, Axelson O. Soft-tissue sarcomas and exposure to chemical substances: a case-referent study. Br J Ind Med. 1981;38(1):27–33.
Greenwald P, Kovasznay B, Collins DN, Therriault G. Sarcomas of soft tissues after Vietnam service. J Natl Cancer Inst. 1984;73(5):1107–9.
Smith AH, Pearce NE, Fisher DO, Giles HJ, Teague CA, Howard JK. Soft tissue sarcoma and exposure to phenoxyherbicides and chlorophenols in New Zealand. J Natl Cancer Inst. 1984;73(5):1111–7.
Hoar SK, Blair A, Holmes FF, Boysen CD, Robel RJ, Hoover R, Fraumeni JF: Agricultural herbicide use and risk of lymphoma and soft-tissue sarcoma. JAMA 1986, 256(9):1141–1147.
Kang HK, Weatherbee L, Breslin PP, Lee Y, Shepard BM. Soft tissue sarcomas and military service in Vietnam: a case comparison group analysis of hospital patients. J Occup Med. 1986;28(12):1215–8.
Kang H, Enzinger FM, Breslin P, Feil M, Lee Y, Shepard B. Soft tissue sarcoma and military service in Vietnam: a case-control study. J Natl Cancer Inst. 1987;79(4):693–9.
Vineis P, Terracini B, Ciccone G, Cignetti A, Colombo E, Donna A, Maffi L, Pisa R, Ricci P, Zanini E et al: Phenoxy herbicides and soft-tissue sarcomas in female rice weeders. A population-based case-referent study. Scand J Work Environ Health 1987, 13(1):9–17.
Woods JS, Polissar L, Severson RK, Heuser LS, Kulander BG. Soft tissue sarcoma and non-Hodgkin’s lymphoma in relation to phenoxyherbicide and chlorinated phenol exposure in western Washington. J Natl Cancer Inst. 1987;78(5):899–910.
Wingren G, Fredrikson M, Brage HN, Nordenskjold B, Axelson O. Soft tissue sarcoma and occupational exposures. Cancer. 1990;66(4):806–11.
Eriksson M, Hardell L, Adami HO. Exposure to dioxins as a risk factor for soft tissue sarcoma: a population-based case-control study. J Natl Cancer Inst. 1990;82(6):486–90.
Franceschi S, Serraino D. Risk factors for adult soft tissue sarcoma in northern Italy. Ann Oncol. 1992;3(Suppl 2):S85-88.
Smith JG, Christophers AJ. Phenoxy herbicides and chlorophenols: a case control study on soft tissue sarcoma and malignant lymphoma. Br J Cancer. 1992;65(3):442–8.
Kogevinas M, Kauppinen T, Winkelmann R, Becher H, Bertazzi PA, Bueno-De-mesquita HB, Coggon D, Green L, Johnson E, Littorin M, et al. Soft tissue sarcoma and non-Hodgkin’s lymphoma in workers exposed to phenoxy herbicides, chlorophenols, and dioxins: two nested case-control studies. Epidemiology. 1995;6(4):396–402.
Hoppin JA, Tolbert PE, Herrick RF, Freedman DS, Ragsdale BD, Horvat KR, Brann EA. Occupational chlorophenol exposure and soft tissue sarcoma risk among men aged 30–60 years. Am J Epidemiol. 1998;148(7):693–703.
Pahwa P, Karunanayake CP, Dosman JA, Spinelli JJ, McLaughlin JR. Soft-tissue sarcoma and pesticides exposure in men: results of a Canadian case-control study. J Occup Environ Med. 2011;53(11):1279–86.
Coggon D, Ntani G, Harris EC, Jayakody N, Palmer KT. Soft tissue sarcoma, non-Hodgkin’s lymphoma and chronic lymphocytic leukaemia in workers exposed to phenoxy herbicides: extended follow-up of a UK cohort. Occup Environ Med. 2015;72(6):435–41.
Wiklund K, Holm LE. Soft tissue sarcoma risk in Swedish agricultural and forestry workers. J Natl Cancer Inst. 1986;76(2):229–34.
Wiklund K, Dich J, Holm LE. Soft tissue sarcoma risk in Swedish licensed pesticide applicators. J Occup Med. 1988;30(10):801–4.
Saracci R, Kogevinas M, Bertazzi PA, Bueno de Mesquita BH, Coggon D, Green LM, Kauppinen T, L'Abbe KA, Littorin M, Lynge E et al: Cancer mortality in workers exposed to chlorophenoxy herbicides and chlorophenols. Lancet 1991, 338(8774):1027–1032.
Sathiakumar N, Delzell E, Austin H, Cole P. A follow-up study of agricultural chemical production workers. Am J Ind Med. 1992;21(3):321–30.
Wiklund K, Dich J. Cancer risks among female farmers in Sweden. Cancer Causes Control. 1994;5(5):449–57.
Gambini GF, Mantovani C, Pira E, Piolatto PG, Negri E. Cancer mortality among rice growers in Novara province Northern Italy. Am J Ind Med. 1997;31(4):435–41.
Lynge E: Cancer incidence in Danish phenoxy herbicide workers, 1947–1993. Environ Health Perspect 1998, 106 Suppl 2(Suppl 2):683–688.
Fleming LE, Bean JA, Rudolph M, Hamilton K. Cancer incidence in a cohort of licensed pesticide applicators in Florida. J Occup Environ Med. 1999;41(4):279–88.
Koutros S, Alavanja MCR, Lubin JH, Sandler DP, Hoppin JA, Lynch CF, Knott C, Blair A, Freeman LEB. An update of cancer incidence in the agricultural health study. J Occup Environ Med. 2010;52(11):1098–105.
Vineis P, Faggiano F, Tedeschi M, Ciccone G. Incidence rates of lymphomas and soft-tissue sarcomas and environmental measurements of phenoxy herbicides. J Natl Cancer Inst. 1991;83(5):362–3.
Lynge E. A follow-up study of cancer incidence among workers in manufacture of phenoxy herbicides in Denmark. Br J Cancer. 1985;52(2):259–70.
Alavanja MC, Sandler DP, Lynch CF, Knott C, Lubin JH, Tarone R, Thomas K, Dosemeci M, Barker J, Hoppin JA et al: Cancer incidence in the agricultural health study. Scand J Work Environ Health 2005, 31 Suppl 1:39–45; discussion 35–37.
Kogevinas M, Becher H, Benn T, Bertazzi PA, Boffetta P, Bueno-de-Mesquita HB, Coggon D, Colin D, Flesch-Janys D, Fingerhut M et al: Cancer mortality in workers exposed to phenoxy herbicides, chlorophenols, and dioxins. An expanded and updated international cohort study. Am J Epidemiol 1997, 145(12):1061–1075.
Steenland K, Piacitelli L, Deddens J, Fingerhut M, Chang LI. Cancer, heart disease, and diabetes in workers exposed to 2,3,7,8-tetrachlorodibenzo-p-dioxin. J Natl Cancer Inst. 1999;91(9):779–86.
Bodner KM, Collins JJ, Bloemen LJ, Carson ML. Cancer risk for chemical workers exposed to 2,3,7,8-tetrachlorodibenzo-p-dioxin. Occup Environ Med. 2003;60(9):672–5.
Collins JJ, Bodner K, Aylward LL, Wilken M, Bodnar CM. Mortality rates among trichlorophenol workers with exposure to 2,3,7,8-tetrachlorodibenzo-p-dioxin. Am J Epidemiol. 2009;170(4):501–6.
Smulevich VB, Fedotova IV, Filatova VS. Increasing evidence of the rise of cancer in workers exposed to vinylchloride. Br J Ind Med. 1988;45(2):93–7.
Ward E, Boffetta P, Andersen A, Colin D, Comba P, Deddens JA, De Santis M, Engholm G, Hagmar L, Langard S, et al. Update of the follow-up of mortality and cancer incidence among European workers employed in the vinyl chloride industry. Epidemiology. 2001;12(6):710–8.
Wong RH, Chen PC, Du CL, Wang JD, Cheng TJ. An increased standardised mortality ratio for liver cancer among polyvinyl chloride workers in Taiwan. Occup Environ Med. 2002;59(6):405–9.
Mundt KA, Dell LD, Crawford L, Gallagher AE. Quantitative estimated exposure to vinyl chloride and risk of angiosarcoma of the liver and hepatocellular cancer in the US industry-wide vinyl chloride cohort: mortality update through 2013. Occup Environ Med. 2017;74(10):709–16.
Fedeli U, Girardi P, Gardiman G, Zara D, Scoizzato L, Ballarin MN, Baccini M, Pirastu R, Comba P, Mastrangelo G. Mortality from liver angiosarcoma, hepatocellular carcinoma, and cirrhosis among vinyl chloride workers. Am J Ind Med. 2019;62(1):14–20.
Simonato L, L'Abbe KA, Andersen A, Belli S, Comba P, Engholm G, Ferro G, Hagmar L, Langard S, Lundberg I, et al. A collaborative study of cancer incidence and mortality among vinyl chloride workers. Scand J Work Environ Health. 1991;17(3):159–69.
Jones RD, Smith DM, Thomas PG. A mortality study of vinyl chloride monomer workers employed in the United Kingdom in 1940–1974. Scand J Work Environ Health. 1988;14(3):153–60.
Fox AJ, Collier PF. Mortality experience of workers exposed to vinyl chloride monomer in the manufacture of polyvinyl chloride in Great Britain. Br J Ind Med. 1977;34(1):1–10.
Byren D, Engholm G, Englund A, Westerholm P. Mortality and cancer morbidity in a group of swedish VCM and PCV production workers. Environ Health Perspect. 1977;17:167–70.
Langard S, Rosenberg J, Andersen A, Heldaas SS. Incidence of cancer among workers exposed to vinyl chloride in polyvinyl chloride manufacture. Occup Environ Med. 2000;57(1):65–8.
Collins JJ, Jammer B, Sladeczek FM, Bodnar CM, Salomon SS. Surveillance for angiosarcoma of the liver among vinyl chloride workers. J Occup Environ Med. 2014;56(11):1207–9.
Polednak AP, Stehney AF, Rowland RE: Mortality among women first employed before 1930 in the U.S. Radium dial-painting industry: A group ascertained from employment lists. Am J Epidemiol 1978, 107(3):179–195.
Teta MJ, Ott MG. A mortality study of a research, engineering, and metal fabrication facility in Western New York state. Am J Epidemiol. 1988;127(3):540–51.
Wiggs LD, Johnson ER, Cox-De Vore CA, Voelz GL. Mortality through 1990 among white male workers at the Los Alamos National Laboratory: considering exposures to plutonium and external ionizing radiation. Health Phys. 1994;67(6):577–88.
Rix BA, Villadsen E, Engholm G, Lynge E. Hodgkin’s disease, pharyngeal cancer, and soft tissue sarcomas in Danish paper mill workers. J Occup Environ Med. 1998;40(1):55–62.
Rix BA, Villadsen E, Lynge E. Cancer incidence of sulfite pulp workers in Denmark. Scand J Work Environ Health. 1997;23(6):458–61.
Koshurnikova NA, Gilbert ES, Sokolnikov M, Khokhryakov VF, Miller S, Preston DL, Romanov SA, Shilnikova NS, Suslova KG, Vostrotin VV. Bone cancers in Mayak workers. Radiat Res. 2000;154(3):237–45.
Hoar Zahm S, Blair A, Holmes FF, Boysen CD, Robel RJ: A case-referent study of soft-tissue sarcoma and Hodgkin’s disease. Farming and insecticide use. Scand J Work Environ Health 1988, 14(4):224–230.
Pearce N, Smith AH, Reif JS. Increased risks of soft tissue sarcoma, malignant lymphoma, and acute myeloid leukemia in abattoir workers. Am J Ind Med. 1988;14(1):63–72.
Zahm SH, Blair A, Holmes FF, Boysen CD, Robel RJ. A case-control study of soft-tissue sarcoma. Am J Epidemiol. 1989;130(4):665–74.
Hoppin JA, Tolbert PE, Flanders WD, Zhang RH, Daniels DS, Ragsdale BD, Brann EA. Occupational risk factors for sarcoma subtypes. Epidemiology. 1999;10(3):300–6.
Briggs NC, Levine RS, Hall HI, Cosby O, Brann EA, Hennekens CH. Occupational risk factors for selected cancers among African American and White men in the United States. Am J Public Health. 2003;93(10):1748–52.
Pahwa P, McDuffie HH, Dosman JA, Robson D, McLaughlin JR, Spinelli JJ, Fincham S. Exposure to animals and selected risk factors among Canadian farm residents with Hodgkin’s disease, multiple myeloma, or soft tissue sarcoma. J Occup Environ Med. 2003;45(8):857–68.
Merletti F, Richiardi L, Bertoni F, Ahrens W, Buemi A, Costa-Santos C, Eriksson M, Guénel P, Kaerlev L, Jöckel KH, et al. Occupational factors and risk of adult bone sarcomas: a multicentric case-control study in Europe. Int J Cancer. 2006;118(3):721–7.
Hossain A, McDuffie HH, Bickis MG, Pahwa P. Case-control study on occupational risk factors for soft-tissue sarcoma. J Occup Environ Med. 2007;49(12):1386–93.
Balarajan R, Acheson ED. Soft tissue sarcomas in agriculture and forestry workers. J Epidemiol Community Health. 1984;38(2):113–6.
Blair A, Stewart P, Lubin JH, Forastiere F. Methodological issues regarding confounding and exposure misclassification in epidemiological studies of occupational exposures. Am J Ind Med. 2007;50(3):199–207.
Stayner LT, Smith RJ. Methodologic issues in using epidemiologic studies of occupational cohorts for cancer risk assessment. Epidemiol Prev. 1992;14(53):32–9.
Blair A, Zahm SH, Pearce NE, Heineman EF, Fraumeni JF Jr. Clues to cancer etiology from studies of farmers. Scand J Work Environ Health. 1992;18(4):209–15.
Blair A, Freeman LB. Epidemiologic studies in agricultural populations: observations and future directions. J Agromedicine. 2009;14(2):125–31.
Hardell L: Epidemiological studies on soft-tissue sarcoma and maligrant lymphoma and their relation to phenoxy acid or chlorophenol exposure: University of Umea, Sweden. -- Thesis (Ph. D)--University of Linkoping, Sweden. -- Includes bibliographical references; 1981.
Fingerhut MA, Halperin WE, Honchar PA, Smith AB, Groth DH, Russell WO. An evaluation of reports of dioxin exposure and soft tissue sarcoma pathology among chemical workers in the United States. Scand J Work Environ Health. 1984;10(5):299–303.
Nandra R, Hwang N, Matharu GS, Reddy K, Grimer R. One-year mortality in patients with bone and soft tissue sarcomas as an indicator of delay in presentation. Ann R Coll Surg Engl. 2015;97(6):425–33.
Hess LM, Zhu YE, Sugihara T, Fang Y, Collins N, Nicol S. Challenges of using ICD-9-CM and ICD-10-CM codes for soft-tissue sarcoma in databases for health services research. Perspect Health Inf Manag. 2019;16(Spring):1a.
Acknowledgements
Wenyan Ji, Department of Biostatistics of the Roswell Park Comprehensive Cancer Center, helped with statistical analysis.
Gayle Ablove and Danielle Glynn, Dr. Edwin A. Mirand Library of the Roswell Park Comprehensive Cancer Center, performed the database searches.
Funding
The authors declare that they have received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
Conception and design of the work: DE and AG; acquisition, data extraction, analysis, and interpretation: DE and AV; drafting the work: DE and AV; revising the work critically for important intellectual content: DE, AV, AG, and KA; statistical analysis: KA. All authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Supplementary tables.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Edwards, D., Voronina, A., Attwood, K. et al. Association between occupational exposures and sarcoma incidence and mortality: systematic review and meta-analysis. Syst Rev 10, 231 (2021). https://doi.org/10.1186/s13643-021-01769-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-021-01769-4