
Abstract
Background
Diabetes is a major public health issue and there is a need to develop low-cost, novel interventions to prevent or reduce disease progression. Growing evidence shows that supplementation with carnosine, or its rate-limiting precursor β-alanine, can ameliorate aspects of the metabolic dysregulation that occurs in diabetes. There is, however, a need to develop a better understanding of the magnitude of effect and the factors associated with positive outcomes. The purpose of this systematic review and meta-analysis is to evaluate the effect of carnosine or β-alanine supplementation on markers of glycaemic control and insulin resistance in humans and animals.
Methods
We will perform a systematic search for randomised and non-randomised controlled trials. Studies will be retrieved by searching electronic databases, clinical trial registers, author review, and cross-referencing. Primary outcomes include changes in (i) fasting glucose, (ii) glycated haemoglobin, and (iii) 2-h glucose following a glucose tolerance test. A set of additional outcomes includes other markers of glycaemic control and insulin resistance. Risk of bias (RoB) will be assessed using the Cochrane RoB 2.0 tool (human studies) and the Systematic Review Centre for Laboratory Animal Experimentation (SYRCLE) RoB tool (animal studies). Confidence in the cumulative evidence will be assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. All meta-analyses will be conducted within a Bayesian framework, providing a flexible modelling approach to account for uncertainty in model parameters and underlying structures within the data.
Discussion
By including all available human and animal data, we will provide the most comprehensive overview on the topic to date. The results will have implications for those working in prediabetes, diabetes, and metabolic health in general and may lead to the development of new treatment approaches.
Dissemination
Study results will be presented at a professional conference and published in a peer-reviewed journal.
Systematic review registration
Similar content being viewed by others
Background
Diabetes is a major public health problem. Recent estimates show that 4.8 million people in the UK are living with diabetes, which is expected to rise to 5.3 million by 2025 [1]. Type 2 diabetes accounts for over 90% of these cases, with the remaining made up of type 1 diabetes, gestational diabetes, and rarer types of diabetes (e.g. maturity onset diabetes of the young). A hallmark of type 2 diabetes is poor glycaemic control and insulin resistance [2], which can present earlier in life as impaired fasting glucose or impaired glucose tolerance (also known as prediabetes). For individuals aged 45 years, there is a 74% lifetime risk of progression from prediabetes to type 2 diabetes [3]. While lifestyle modifications are central to risk reduction, they can be challenging to implement, and long-term adherence limits their effectiveness. It is therefore important to develop low-cost, novel interventions to improve glycaemic control and help prevent or delay disease progression.
The multifunctional compound carnosine has emerged as a candidate for clinical use. Carnosine, a member of the histidine-containing dipeptide (HCD) family, exists naturally in high concentrations in mammalian skeletal muscle and in smaller amounts in other excitable tissues [4,5,6,7]. Contents in skeletal muscle can be increased by supplementing with carnosine or its rate-limiting precursor β-alanine [8]. Work from our Research Group shows that treatment with carnosine decreases highly toxic lipid peroxidation products in skeletal muscle cells (unpublished data), leading to an increase in insulin-stimulated glucose uptake under glucolipotoxic conditions [9]. Further evidence supports the role of carnosine in non-enzymatic detoxification of reactive aldehydes [10, 11], an effect that β-alanine supplementation potentiates in vivo [12, 13]. Through these actions, carnosine may be able to ameliorate aspects of the metabolic dysregulation that occurs in diabetes and its related conditions.
There is growing evidence from rodent studies that carnosine supplementation can prevent or delay the development of type 2 diabetes [14, 15]. Initial human trials also show promise [16, 17], but the factors associated with positive outcomes are unclear. A recent meta-analysis of human studies sought to address this knowledge gap, concluding that supplementation with histidine-containing dipeptides improves waist circumference, fasting glucose, and glycated haemoglobin (HbA1c) [18]. The review, however, had several methodological shortcomings (for details, see [19]), which included combining effects from studies using multi-ingredient supplements with those supplementing carnosine or β-alanine in isolation. This approach cannot determine whether the beneficial effects are due to carnosine or β-alanine alone. It is also important to consider relevant outcomes from animal models that can provide mechanistic insight and help inform future human research studies. There is a clear need to develop a better understanding of the magnitude of effect, as well as the factors associated with supplementation for improving outcomes. Therefore, the purpose of this systematic review and meta-analysis is to evaluate the effect of carnosine or β-alanine supplementation on markers of glycaemic control and insulin resistance in humans and animals.
Methods
This protocol follows the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) [20] and is registered on PROSPERO (registration number CRD42020191588).
Eligibility criteria
Studies will be selected according to the eligibility criteria outlined in Table 1. There will be no restrictions on the timing or duration of supplementation and no restrictions on the type of setting. English and non-English language sources will be included with the latter translated into English using freely available online translators (e.g. Google or Bing). Any studies that cannot be adequately translated will be excluded from the review and a list of the titles provided as an appendix.
Information sources
We will search the following electronic databases for potentially eligible studies: PubMed, Scopus, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), Cumulative Index to Nursing and Allied Health Literature (CINAHL), and ProQuest. The electronic database search will be supplemented by searching for trial protocols listed on trial registers: Clinical Trials (www.ClinicalTrials.gov), EU Clinical Trials Register (www.clinicaltrialsregister.eu), International Standard Randomised Controlled Trial Number (ISRCTN) (www.isrctn.com/mrct), and Animal Study Registry (www.animalstudyregistry.org). To ensure full coverage of the literature, we will search the reference lists and perform citation tracking of included studies and relevant reviews identified through the search. Review authors will also search their own personal files to identify any potentially relevant material.
Search strategy
Search strategies will be developed using key text words and Medical Subject Headings (MeSH) related to the population, intervention, and outcomes (Table 1). A preliminary search strategy for PubMed can be viewed in the supporting information. The search strategy will be peer-reviewed by an academic librarian, not otherwise associated with the project, using the Peer Review of Electronic Search Strategies (PRESS) approach [23]. This search strategy will then be adapted for other databases. Searches will be performed from the earliest record in each database up to the present day and repeated prior to submission of the final review to retrieve any articles published during the interim period.
Initial searches, data extraction, and assessment of risk of bias steps will be completed independently by two reviewers. Full-text screening will be completed independently by three reviewers. Any disagreements will be resolved via consensus-based discussion, and remaining disagreements for searches, data extraction, and risk of bias will be referred to a third reviewer who will provide a recommendation.
Study records
Titles and abstracts of articles from the initial searches will be imported into a systematic review management platform (Covidence, Veritas Health Innovation Ltd., Melbourne; Australia), duplicates removed, and remaining articles screened for potential eligibility. We will obtain full texts for all articles that appear to meet the inclusion criteria or where there is any uncertainty. Each reviewer will use the reference manager functions to highlight eligibility criteria and add comments on each article, which allows decisions to be cross-referenced in the event of a disagreement. Reviewers will not be blinded to the journal titles or the study authors.
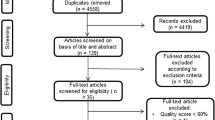
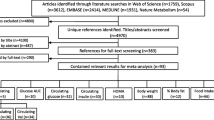
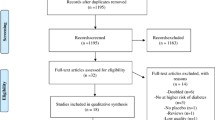
Multiple reports of the same study will be handled by including the published article that provides the most relevant outcome data, assuming similar methods and sample sizes. We will seek additional information from study authors where necessary to resolve issues regarding eligibility (maximum of three e-mail attempts). A PRISMA flow diagram that depicts the search process will be included (see supporting information for a template), as well as supporting information that includes a reference list of all full-text studies excluded, including reasons for exclusion.
Data will be extracted using a standardised spreadsheet based on the Cochrane data collection form for intervention reviews [24]. To ensure consistency between reviewers, we will conduct calibration exercises before starting data extraction.
Data items
We will extract data for (i) study characteristics (location, setting, study design, size, duration, funding sources, and study aim), (ii) human participant characteristics (age, height, sex, body mass, body mass index, body fat %, type and duration of condition, activity and exercise levels, and dietary information), (iii) animal characteristics (age, body mass, source, species, strain, sex, developmental stage, genetic modification status, genotype, type and duration of condition, method used to induce disease, and housing conditions), (iv) intervention characteristics (name, type of control used, dosage, frequency, duration, route of administration), and (v) outcome characteristics for glycaemic control and insulin resistance (type of measure, sample sizes, baseline, interim, and post-intervention measures of central tendency and dispersion, adherence to the intervention, dropouts, number and nature of side effects, and assessment of blinding to the intervention). We will also extract information relevant to measures of risk of bias and quality assessment. Where necessary, measures of central tendency and dispersion will be extracted from figures in the articles using WebPlotDigitizer version 3.10 (https://apps.automeris.io/wpd/). If parameters cannot be adequately calculated, we will contact study authors for additional data (maximum of three e-mail attempts).
Outcomes and prioritisation
The three primary outcomes will be changes in fasting glucose (FG) (includes plasma, serum, and blood glucose values), glycated haemoglobin (HbA1c), and 2-h glucose following a glucose tolerance test (GTT). These outcomes represent the three clinical markers used in the diagnosis of type 1 diabetes, type 2 diabetes, prediabetes, and gestational diabetes [21, 22]. Additional outcomes include changes in other markers of glycaemic control and insulin resistance (for a full list see supporting information).
Risk of bias in individual studies
Risk of bias in individual human studies will be assessed using the Cochrane risk of bias 2.0 tool (RoB 2.0) for assessing risk of bias in randomised trials [25] and in individual animal studies using the Systematic Review Centre for Laboratory Animal Experimentation (SYRCLE) tool [26]. Reviewers will assess each study item as either “high risk”, “low risk”, “some concerns” (RoB 2.0), or “unclear risk” (SYRCLE) of bias. All disagreements and referrals will be recorded.
Data synthesis
Data will be presented in summary tables to describe the study population and intervention. We will conduct meta-analyses using appropriate models to account and explore for variation within and between studies. All meta-analyses will be conducted within a Bayesian framework, providing a flexible modelling approach to account for uncertainty in model parameters and underlying structures within the data. Additionally, Bayesian models will enable results to be interpreted more intuitively through reporting subjective probabilities rather than null hypothesis tests or frequentist confidence intervals [27]. Each of the primary and additional outcomes will be extracted and analysed as continuous measures. For primary outcomes, the effect of each study will be estimated by calculating the pre-post raw scale mean difference between intervention and control. Modelling outcomes on the same absolute scale as the original measurement will provide more interpretable findings. Effect size estimates for additional outcomes will be standardised using reported standard deviations to account for differences in measurement scales. Standard threshold values of 0.2, 0.5, and 0.8 will be used to describe effect size estimates as small, medium, and large, respectively [28]. Values between 0 and 0.2 will be described as trivial. Three-level Bayesian hierarchical models will be used to pool effect sizes and model average effect, variance within studies, variance between studies, and covariance of multiple outcomes reported in the same study (e.g. single outcome variable reported at intermediate testing points). Informative priors will be used to estimate within-study variances and account for unknown correlations between pre and post values of the different outcomes. Non-informative priors will be used for all other model parameters. Inconsistency in models will be described by comparing variances across the three levels. Inferences from all analyses will be performed on posterior samples generated by Hamiltonian Markov chain Monte Carlo and through the use of credible intervals and calculated probabilities. Analyses will be performed using the R wrapper package brms interfaced with Stan to perform sampling [29].
Sensitivity analyses will be performed to examine the robustness of the outcomes by excluding studies at high risk of bias. Animal and human studies will be aggregated if sufficient data are available and meta-regressions indicate no substantive difference in the median pooled effect size estimate. Meta-regressions where possible will be used to explore the effect of type of supplementation (carnosine or β-alanine), duration of supplementation, and the disease type. Meta-regressions using categorical variables will be performed where there are at least four data points for each factor level.
Meta-biases
Outcome reporting bias
Where possible, we will screen clinical trial registers to compare outcomes reported in the protocol with each published report. Where there is no preregistration or protocol, we will compare the outcomes reported in the methods and results section of each published report.
Small study bias (includes publication and study quality bias)
We will visually inspect funnel plots and assess using a multi-level extension of Egger’s regression test [30].
Confidence in cumulative evidence
The quality of evidence for each outcome will be assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach [31], which assesses quality across five domains: risk of bias, inconsistency (heterogeneity), indirectness, imprecision, and publication bias. Quality will be graded as “high”, “moderate”, “low”, or “very low” (Table 2). Outcomes from randomised controlled trials begin as “high” quality evidence and can be downgraded for issues in each domain. Outcomes can also be upgraded when there is evidence of a large magnitude of effect, presence of a dose-response gradient, and all plausible confounders of other biases increase the confidence in the estimated effect [33]. The approach and procedures will be the same as for study selection and data extraction.
Discussion
This systematic review and meta-analysis will synthesise evidence to determine the effect of carnosine or β-alanine supplementation on markers of glycaemic control and insulin resistance. By including all available human and animal data, we will provide the most comprehensive overview on the topic to date. Further, the proposed meta-analysis will explore the factors associated with positive outcomes and highlight promising avenues of future research. The results will have implications for those working in prediabetes, diabetes, and metabolic health in general and may lead to the development of new treatment approaches.
Dissemination
The study results will be presented at a professional conference and published in a peer-reviewed journal.
Availability of data and materials
Not applicable.
Abbreviations
- BMI:
-
Body mass index
- FG:
-
Fasting glucose
- GRADE:
-
Grading of Recommendations Assessment, Development and Evaluation
- GTT:
-
Glucose tolerance test
- HbA1c :
-
Glycated haemoglobin A1c
- HCD:
-
Histidine-containing dipeptide
- MeSH:
-
Medical Subject Headings
- PRESS:
-
Peer Review of Electronic Search Strategies
- PRISMA:
-
Preferred Reporting Items for Systematic Review and Meta-Analysis
- RCTs:
-
Randomised controlled trials
- SYRCLE:
-
Systematic Review Centre for Laboratory Animal Experimentation
- WHO:
-
World Health Organization
References
Diabetes UK. Number of people with diabetes reaches 4.8 million. Diabetes UK. Available from: https://www.diabetes.org.uk/about_us/news/diabetes-prevalence-2019. [cited 2020 Sep 4].
Kahn SE. The relative contributions of insulin resistance and beta-cell dysfunction to the pathophysiology of type 2 diabetes. Diabetologia. 2003;46(1):3–19.
Ligthart S, van Herpt TTW, Leening MJG, Kavousi M, Hofman A, Stricker BHC, et al. Lifetime risk of developing impaired glucose metabolism and eventual progression from prediabetes to type 2 diabetes: a prospective cohort study. Lancet Diabetes Endocrinol. 2016;4(1):44–51.
Matthews JJ, Artioli GG, Turner MD, Sale C. The physiological roles of carnosine and β-alanine in exercising human skeletal muscle. Medicine & Science in Sports & Exercise. 2019;51(10):2098–108.
Crush KG. Carnosine and related substances in animal tissues. Comp Biochem Physiol. 1970;34(1):3–30.
Kohen R, Yamamoto Y, Cundy KC, Ames BN. Antioxidant activity of carnosine, homocarnosine, and anserine present in muscle and brain. Proc Natl Acad Sci. 1988;85(9):3175–9.
Peters V, Klessens CQF, Baelde HJ, Singler B, Veraar KAM, Zutinic A, et al. Intrinsic carnosine metabolism in the human kidney. Amino Acids. 2015. https://doi.org/10.1007/s00726-015-2045-7.
Harris RC, Tallon MJ, Dunnett M, Boobis L, Coakley J, Kim HJ, et al. The absorption of orally supplied β-alanine and its effect on muscle carnosine synthesis in human vastus lateralis. Amino Acids. 2006;30:279–89.
Cripps MJ, Hanna K, Lavilla C, Sayers SR, Caton PW, Sims C, et al. Carnosine scavenging of glucolipotoxic free radicals enhances insulin secretion and glucose uptake. Sci Rep. 2017;7:1–7.
Aldini G, Carini M, Beretta G, Bradamante S, Facino RM. Carnosine is a quencher of 4-hydroxy-nonenal: through what mechanism of reaction? Biochem Biophys Res Commun. 2002;298(5):699–706.
Baba SP, Hoetker JD, Merchant M, Klein JB, Cai J, Barski OA, et al. Role of aldose reductase in the metabolism and detoxification of carnosine-acrolein conjugates. J Biol Chem. 2013;288(39):28163–79.
Carvalho VH, Oliveira AHS, de Oliveira LF, da Silva RP, Di Mascio P, Gualano B, et al. Exercise and β-alanine supplementation on carnosine-acrolein adduct in skeletal muscle. Redox Biol. 2018;18:222–8.
Hoetker D, Chung W, Zhang D, Zhao J, Schmidtke VK, Riggs DW, et al. Exercise alters and β-alanine combined with exercise augments histidyl dipeptide levels and scavenges lipid peroxidation products in human skeletal muscle. J Appl Physiol. 2018;125:1767–78.
Albrecht T, Schilperoort M, Zhang S, Braun JD, Qiu J, Rodriguez A, et al. Carnosine Attenuates the development of both type 2 diabetes and diabetic nephropathy in BTBR ob / ob mice. Sci Rep. 2017;7:44492.
Sauerhöfer S, Yuan G, Braun GS, Deinzer M, Neumaier M, Gretz N, et al. L-carnosine, a substrate of carnosinase-1, influences glucose metabolism. Diabetes. 2007;56(10):2425–32.
De Courten B, Jakubova M, De Courten MPJ, Kukurova IJ, Vallova S, Krumpolec P, et al. Effects of carnosine supplementation on glucose metabolism: pilot clinical trial. Obesity. 2016;24(5):1027–34.
Houjeghani S, Kheirouri S, Faraji E, Jafarabadi MA. L-Carnosine supplementation attenuated fasting glucose, triglycerides, advanced glycation end products, and tumor necrosis factor–α levels in patients with type 2 diabetes: a double-blind placebo-controlled randomized clinical trial. Nutr Res. 2018;49:96–106.
Menon K, Marquina C, Liew D, Mousa A, de Courten B. Histidine-containing dipeptides reduce central obesity and improve glycaemic outcomes: a systematic review and meta-analysis of randomized controlled trials. Obes Rev. 2020;21(3):e12975.
Matthews JJ, Sale C. Comments upon ‘Histidine-containing dipeptides reduce central obesity and improve glycaemic outcomes: a systematic review and meta-analysis of randomized controlled trials’. Obes Rev. 2020;21(7):e13036.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1.
World Health Organization. Definition and diagnosis of diabetes mellitus and intermediate hyperglycaemia: report of a WHO/IDF consultation. Geneva: World Health Organization; 2006. Available from: https://www.who.int/diabetes/publications/Definition%20and%20diagnosis%20of%20diabetes_new.pdf. [cited 2019 May 25].
World Health Organization. Use of glycated haemoglobin (HbA1c) in the diagnosis of diabetes mellitus: abbreviated report of a WHO consultation. Geneva: World Health Organization; 2011. Available from: https://www.who.int/diabetes/publications/report-hba1c_2011.pdf. [cited 2019 May 25].
McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40–6.
The Cochreane Collaboration. Data collection form (for RCTs) [Internet]. Cochrane Training. Available from: https://training.cochrane.org/data-collection-form-rcts. [cited 2020 Oct 4].
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
Hooijmans CR, Rovers MM, de Vries RBM, Leenaars M, Ritskes-Hoitinga M, Langendam MW. SYRCLE’s risk of bias tool for animal studies. BMC Med Res Methodol. 2014;14:43.
Kruschke JK, Liddell TM. The Bayesian New Statistics: Hypothesis testing, estimation, meta-analysis, and power analysis from a Bayesian perspective. Psychon Bull Rev. 2018;25(1):178–206.
Cohen J. The effect size index: d. Statistical power analysis for the behavioral sciences, vol. 2; 1988. p. 284–8.
Bürkner P-C. Others. brms: an R package for Bayesian multilevel models using Stan. J Stat Softw. 2017;80(1):1–28.
Fernández-Castilla B, Declercq L, Jamshidi L, Beretvas SN, Onghena P, Van den Noortgate W. Detecting selection bias in meta-analyses with multiple outcomes: a simulation study. J Exp Educ. 2019;3:1–20.
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–94.
Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401–6.
Guyatt GH, Oxman AD, Sultan S, Glasziou P, Akl EA, Alonso-Coello P, et al. GRADE guidelines: 9. Rating up the quality of evidence. J Clin Epidemiol. 2011;64(12):1311–6.
Funding
This article is not sponsored and is not receiving funding.
ED has been supported financially by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP; grant numbers: 2019/05616-6 and 2019/26899-6)
GGA has been supported financially by FAPESP (grant numbers: 2014/ 11948-8 and 2019/25032-9) and by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES).
MDT has received a British Council award to support a studentship focused on research into carnosine (grant number: 209524711).
Author information
Authors and Affiliations
Contributions
JJM and CS conceived the study idea. All authors contributed to the design of the systematic review. JJM and PAS contributed to the data analysis plan. All authors contributed to the write-up and editing of the manuscript and approved the final manuscript. CS takes responsibility, and acts as a guarantor, for the content of the protocol.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
JJM, PAS, LS, and KEJS declare no competing interests.
CS is the recipient of funding to support a PhD programme of work from Natural Alternatives International (NAI) and has received β-alanine supplements free of charge from NAI for use in experimental investigations; NAI has also supported open access page charges for some manuscripts.
GGA has been a co-investigator on projects partially supported by NAI.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Supporting information.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Matthews, J.J., Dolan, E., Swinton, P.A. et al. The effect of carnosine or β-alanine supplementation on markers of glycaemic control and insulin resistance in human and animal studies: a protocol for a systematic review and meta-analysis. Syst Rev 9, 282 (2020). https://doi.org/10.1186/s13643-020-01539-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-020-01539-8