
Abstract
Background
The health impacts of loneliness and social isolation among older adults are widely acknowledged. Despite this, there is no consensus on the possible causal nature of this relationship, which could undermine effectiveness of interventions. One body of thought is that loneliness and social isolation affect health-related behaviours to indirectly damage health. However, there has not been any systematic assessment of the association between loneliness and social isolation and health-related behaviours which considers the possible impact from confounding factors and the causal direction of this association.
Methods/design
The research will comprise a systematic review and meta-analysis to address the evidence gap. EMBASE, MEDLINE, PSYCINFO, CINAHL, SocIndex, Scopus and Web of Science will be systematically searched for quantitative observational studies considering an association between loneliness/social isolation and key health-related behaviours in older adults. Two reviewers will independently check the study titles and abstracts for eligibility. Included studies will be critically appraised using Newcastle-Ottawa Scale by the lead author and checked by the second reviewer. Discrepancies in eligibility or quality assessment will be resolved via discussion or referral to a third reviewer. Results will be synthesised and reported in accordance with the Centre for Reviews and Dissemination (CRD) guidelines. This will be in the form of a descriptive summary, risk of bias assessment together with a meta-analysis and sub-group analyses (for covariate adjusted results) where sufficient heterogeneity of results is established. Finally, any associations identified will be analysed using the Bradford-Hill criteria to explore causal relationships which, if they exist, will be reported by means of a computed causations score.
Discussion
This review aims to assess the extent and causal nature of associations between loneliness/social isolation and health-related behaviours among older adults. This data will provide a comprehensive overview of the quality of the evidence base to inform stakeholders in tackling the growing public health challenges arising from loneliness/social isolation in ageing populations.
Systematic review registration
PROSPERO CRD42017020845
Similar content being viewed by others


Background
Loneliness/social isolation and ill-health
The health impacts of loneliness and social isolation are widely recognised. Evidence of their adverse impacts on mental health is particularly strong, including outcomes such as depression [1,2,3,4,5,6,7], anxiety [8], schizophrenia [9, 10], suicide [11,12,13,14] and dementia and Alzheimer’s disease [15,16,17]. The link with physical disease has been made between elevated risk among lonely or isolated people and coronary heart disease and cardiovascular conditions [18,19,20,21]. In addition, there is evidence of a significant association between loneliness and cancer [22] as well as greater susceptibility to infectious diseases [23, 24].
Although distinct concepts, loneliness and social isolation are often used interchangeably and therefore both need to be considered together in examining their health impacts. Loneliness is a perceived deficit between actual and desired quality or quantity of relationships [25]. Social isolation is the objectively quantified shortfall in an individual’s social relationships often measured in terms of social network size, diversity or frequency of contacts [26]. People can be socially isolated without feeling lonely, or feel lonely despite having an adequate quantity of social relationships.
Despite their acknowledged health impacts, both loneliness and social isolation prevalence rates have persisted over several decades [27]. With levels greatest among older people linked to loss of contemporaries, cognitive decline, disability and the loss of social roles [28,29,30], Consequently, much of the research to date on the adverse health impact from loneliness/social isolation has focused on older adults particularly for age-related health conditions [31, 32]. In addition, a number of longitudinal studies [1, 3,4,5, 15, 33] have shown the cumulative effects of loneliness/social isolation on ill-health over time thereby manifesting greatest among older adults, particularly the oldest old who receive greatest cumulative exposure [29, 34, 35]. Exacerbating these health impacts on older adults are several socio-demographic trends in recent decades. The first has been the dramatic rise in chronic long-term conditions to become the main source of morbidity and mortality among older adults. Typically, long-term conditions are associated with loneliness [1,2,3,4,5,6,7,8,9,10,11, 15,16,17,18,19,20,21,22]. Secondly, the ageing population in many countries means that there are increasing numbers of older adults living longer and at greater risk of exposure to loneliness/social isolation and their associated ill-health effects [36, 37]. Finally, increasing proportions of older adults living in single person households means that greater proportions are likely to experience loneliness and isolation which are strongly correlated with living alone [28].
The combination of socio-demographic trends and the health impacts of social isolation/loneliness has made this a major public health concern [38]. There is strong evidence of social isolation/loneliness having greater or equivalent risk to mortality than smoking or obesity respectively [39,40,41,42,43]. In response, governments in the UK are formulating national strategies [44,45,46] to tackle the effects while health and social care services have new policy commitments [47,48,49] in recognition of growing service costs from loneliness/social isolation [50]. With such governmental focus on loneliness/social isolation and preventing associated ill-health outcomes, there is an urgent need to improve our understanding of how the relationship between loneliness/social isolation and health operates to effectively intervene for those most likely to be affected.
Evidence on loneliness/social isolation and health in older adults and current gaps
Despite demographic and social trends and associated health impacts, there remain significant gaps in our understanding of the link between loneliness/social isolation and ill-health. Few studies investigate the indirect ill-health pathways via health-related behaviours and instead focus on direct biological or physiological pathways [23, 51,52,53,54,55,56,57,58]. Of those studies which do consider the association with health-related behaviours some suggest loneliness/social isolation is associated with lower physical activity [59], alcohol misuse [60] and smoking [53, 61] while others found no evidence of variation in lifestyle behaviours between lonely and non-lonely older people [23, 52, 54]. This led some to dispute the claim that health behaviours are associated with mortality and morbidity among lonely persons [62]. Added to this gap in evidence on health-related behaviours, causal link with loneliness/social isolation among older people is the role of potential confounding or effect modifying covariates, e.g. poverty and low educational attainment [63,64,65,66]. This may have important consequences in shaping effective public health interventions.
Review literature
Previous reviews on social relationships causal associations with ill-health have not employed clear definitions or included objective and broader measures of functional social support, social integration or social capital [28, 39, 40, 42, 43] or other related measures, e.g. living alone [67,68,69] or marital status [70,71,72]. Many reviews on social isolation or loneliness do not address the evidence for a causal relationship with ill-health [11, 33, 43, 50,51,52, 73,74,75]. Of the few reviews which have investigated the causal pathways, most have used a discursive theoretical approach rather than a systematic synthesis of empirical data or given limited examination of behavioural pathways [51, 52, 58]. Two reviews have specifically considered the potential indirect health risk due to lifestyle factors but these are either out of date, not systematic, not focused on older people or consider only a single health behaviour [60, 76]. In addition, only a few reviews have focused on older adults and ill-health despite prevalence of loneliness/social isolation being greatest in this group [33, 75, 77].
Aims and objectives
The aim of this study will be to synthesise and assess the evidence of the extent and nature of any association between loneliness and/or social isolation and health-related lifestyle behaviours risk including the extent due to other related factors. This will lead to a better understanding for the development of targeted and effective interventions. The key objectives are:
-
1)
To establish the extent of association between loneliness or social isolation and key health-related behaviour risks, specifically alcohol or drugs misuse, smoking, physical activity and obesity.
-
2)
To assess the evidence for any causal relationship in any associations found.
-
3)
To report whether any association found between loneliness and/or social isolation and health-related behaviours is independent of known covariates.
Methods and design
The design of this research will be a systematic review. This systematic review will be carried out in accordance with the reporting guidelines and checklist of criteria set in Preferred Reporting Items for Systematic Review (PRISMA) [78] and if appropriate the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidance for systematic review reporting.
Inclusion criteria
Study types
The review will include any interventional or observational study that quantitatively assesses the associations of loneliness/social isolation and selected health-related behaviours and the evidence of causation. Cross-sectional studies will be included for assessing associations but not causality. No date restrictions will be placed upon search. For mixed methods studies, only the quantitative element will be extracted and reviewed where it meets the inclusion criteria.
Population type
Studies involving older adult aged 50 and older. There will be no restrictions on any other participant characteristics.
Exposure measures
Studies reporting clearly defined loneliness and/or social isolation exposure measures. For the purposes of this review loneliness will be defined as a perceived deficit between the actual and desired quantity or quality of an individual’s social relationships while social isolation is an objectively measured shortfall in the level of an individual’s social contacts [25, 26]. A number of such measures have been utilised in the literature from single item to multi-dimensional scales [79,80,81,82]. Some studies interchange the terms loneliness and social isolation and an assessment will be made to allocate the exposure to the correct type.
Outcome measures
Studies including at least one key health-related risk behaviour as the outcome of interest, e.g. tobacco use, alcohol misuse, physical activity or obesity, since these are acknowledged as the primary lifestyle risk factors with a causal association upon many chronic health conditions associated with loneliness/social isolation [83, 84].
Covariates
Studies including socio-demographic and ill-health covariates on identified associations. Studies that do not contain estimates adjusted for these covariates will be included but with potentially confounded results noted.
Exclusion criteria
Studies that do not test for empirical associations between loneliness or social isolation and the specified health-related lifestyle behaviours will be excluded.
Studies utilising proxy measures of loneliness or social isolation such as ‘living alone’ or ‘marital status’ or wider measures such as social relationships or social support will be excluded since these do not represent the specific exposures of interest.
Non-English language studies will be excluded though no geographical restrictions will be applied.
Identification of eligible studies and data extraction
Search strategy
The following databases and electronic collections will be searched for relevant publications: OVID MEDLINE, OVID Nursing, EMBASE, CINAHL, PsychINFO, SocINDEX (Gerontology, Psychology, Social Sciences and Sociology categories), Social Work Online, Scopus and Web of Science. Manual hand searching of reference lists from identified studies will be undertaken for any overlooked articles or dissertations of relevance. In addition, the search will include the grey literature available from the above specified databases with no restriction made on publication type. Further grey literature will be identified via the searching of targeted websites of health organisations, older persons agencies and relevant campaigning organisations (e.g. Campaign for Loneliness). Key content experts will be contacted directly to identify any further documents (e.g. via the Campaign for Loneliness Research Hub membership). The full description of the search terms and search strategy devised for MEDLINE database is provided (see Additional file 1), which will be adapted as required for use in searching other databases.
The search strategy will use both Medical Subject Heading (MesH) terms (MEDLINE and CINAHL) and Major Subject Headings (PsychINFO) as well as keyword searching on exposure and outcomes of interest (all databases). The sensitivity and specificity of search will be maximised by use of explosion and truncating of subject terms and Boolean searching on synonyms of loneliness and the key health-related behaviours. The strategy will be reviewed by an experienced librarian to assess its quality based on Peer Review of Electronic Search Strategy (PRESS) Tier 1 checklist elements [85].
Selection of studies
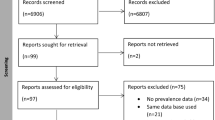
The selection of studies will follow the checklist contained in the PRISMA guidelines [86]. The lead reviewer (MM) will independently screen all retrieved study titles and abstracts to assess eligibility against the inclusion/exclusion criteria and import into RefWorks before removing any duplicates. A second reviewer will independently assess the accuracy of all screened study titles. Any discrepancies between reviewer selections will be resolved by discussion between reviewers or on reference to a third reviewer if consensus is not achieved. Full texts of potentially eligible studies will be obtained and reviewed by the lead reviewer where required to support screening of studies for final inclusion. A second reviewer will assess all potentially eligible full texts for confirming final included studies. For any papers where there is uncertainty regarding inclusion the paper will be reviewed by a third reviewer. Study authors will be contacted should clarification be required. The rationale for exclusion will be recorded as part of the screening process and reported in accordance with the stated eligibility criteria. The PRISMA search flow chart will be used to record the number of studies included and excluded at each step in the process.
Data extraction
Data extraction will be performed by the lead reviewer and checked by two secondary reviewers using a pre-defined data extraction form created in Excel and based upon Centre for Reviews and Dissemination (CRD) guidelines [87] and the Joanna Briggs Institute Data Extraction Form for Prevalence and Incidence Studies [88]. Variables will be extracted for the following key groupings: general study information, study characteristics, participant characteristics, exposure measures, outcome data and analysis/results (see Additional file 2 .
Study quality and critical appraisal
The quality of eligible studies will be appraised using the Newcastle-Ottawa Scale (NOS) [89], a tool developed specifically for assessing quality of observational epidemiological studies. Versions of the NOS tool for both case control and cohort studies will be used together with an adapted version for cross-sectional studies. The NOS assesses study bias through star rating according to selection of study groups, comparability of the groups and ascertainment of either exposure being tested for case control studies or outcome of interest for cohort studies. This assessment of quality will be undertaken by the first author and checked independently for completeness and accuracy by a second author. Any differences in the assessment of quality will be resolved via discussion between these authors and if remains unresolved upon referral to a third author.
Synthesis and analysis
The data will be categorised into each health-related behaviour outcome and loneliness or social isolation exposure type. Data from eligible studies will first be synthesised as per CRD ‘Systematic Reviews: CRD Guidance for undertaking reviews in healthcare, 2009’ guidance by means of a descriptive summary in tabular format concerning study type, exposure, participant characteristics and outcome measures. Secondly, a summary table on the quality of studies will be provided according to three potential categories of risk bias identified using the NOS tool, specifically selection, comparability and exposure/outcome.
Meta-analysis will be considered depending on the availability of data of sufficient quality and similarity for each of the exposures and health-related behaviours. As indicated by the Cochrane Handbook for Systematic Reviews [90] recommendation, the extent of heterogeneity will be assessed using the I2 statistic. Meta-analysis of studies will be carried out on pooled results where I2 < 60% using a fixed or random effects model as appropriate [90].
Individual study results (odds ratios, risk ratios, prevalent ratios) will be reported along with 95% confidence intervals (CIs). If sufficient homogeneity is identified, then results will be converted to odds ratios (ORs) where required and reported as combined ORs. Pooled ORs will be reported for the effect of loneliness/social isolation upon each category of health behaviour. Sub-group analysis will be performed on studies providing adjusted results where there are a sufficient number of studies to permit pooling of results at this level. This will be performed on groups of either partially adjusted results comprising up to two covariates (normally age and gender) or fully adjusted results for greater than two covariates. To assess for potential publication bias, funnel plots of effect estimates against sample sizes will be produced and examined for their symmetry.
A narrative synthesis will be completed if there is insufficient number, quality or similarity of data to permit a formal meta-analysis or sub-group analysis. This will follow best practice guidance on conducting narrative synthesis [91] to summarise the current state of knowledge and describe the study designs, the findings and the robustness of the evidence including the strengths and limitations of studies and the conclusions drawn from the results. This will include assessment for publication bias via a funnel plot of sample size v. effect size should there be a high proportion of studies with significant findings. The overall strength of the synthesised evidence will be assessed using GRADE (Grades of Recommendation, Assessment, Development, and Evaluation) criteria [92].
Assessment for causality
Each outcome-exposure category will be analysed according to applicable Bradford Hill criteria of causation [93] to assess whether any association between loneliness or social isolation and each health-related behaviour identified in the synthesis and analysis has a potential causal relationship. The assessed Bradford Hill criteria will include:
-
1)
Temporality
-
2)
Association (strength and significance of association)
-
3)
Dose-response relationship (or biological gradient)
-
4)
Consistency
Other Bradford Hill criteria for causality will not be applied: ‘experiment’, since there is an absence of empirical/RCT research in this area; ‘specificity’, since loneliness/social isolation have several possible outcomes; ‘coherence’, given this is usually tested by conformity of surrogate outcomes to the pathology of the ill-health outcome observed. In this review, the key lifestyle behaviours are risk factors of ill-health and so surrogates by definition; ‘plausibility’, since associations observed would be expected to have probable mechanisms posited by researchers as explanation; ‘analogy’ since alternative similar associations (e.g. from social support deficits or depression) that may be applied as analogous arguments to support causation do not assist in the key aim of this review, which is to specifically isolate the particular psycho-social construct of loneliness and objective social isolation and their causal association with the outcomes of interest.
The results from each study will be summarised to determine the overall levels of evidence for each criterion of causality for each loneliness and health behaviour category. This will be carried out by means of a causation score for each health-related behaviour and loneliness/social isolation category. The score is calculated according to the unweighted sum of the number of criteria met where a score of 4 is adjudged to be indicative of strong evidence of cause and effect relationship, a score of three to show moderate level of evidence and two or lower to indicate weak evidence [94, 95].
Discussion
This will be the first systematic review specifically focused on associations and potential causal relationships between loneliness/social isolation with health-related behaviours among older adults. In addition, it will seek to assess the role of a range of socio-demographic factors on this association. The strengths of the systematic review include clear definitions and inclusion criteria, transparent systematic approach to searching, screening, assessing and extracting which utilises standardised forms and independent review wherever possible. The systematic review will be strengthened by the appropriate use of standard reporting instruments such as PRISMA, NOS, and GRADE. Additionally, reporting will be structured and comprehensive, including critical appraisal, narrative synthesis and, if appropriate, meta-analysis.
It is timely for such a review given the growing prominence of the issue in the media [96,97,98] and health policy [45,46,47,48,49]. Such growing media and government attention recognises the socio-demographic trends fuelling loneliness and social isolation among older adults to the extent it has become an acknowledged public health challenge. Therefore, understanding the association and causal pathways between loneliness/social isolation and ill-health will be important for developing interventions and strategies to combat loneliness and social isolation.
Abbreviations
- CIs:
-
Confidence intervals
- CRD:
-
Centre for Reviews and Dissemination
- GRADE:
-
Grades of Recommendation, Assessment, Development and Evaluation
- NOS:
-
Newcastle-Ottawa Scale
- ORs:
-
Odds ratios
- PRESS:
-
Peer Review of Electronic Search Strategy
- PRISMA:
-
Preferred Reporting Items for Systematic Review
References
Green BH, Copeland JR, Dewey ME, Sharma V, Saunders PA, Davidson IA, et al. Risk factors for depression in elderly people: a prospective study. Acta Psychiatr Scand. 1992;86(3):213–7.
Prince MJ, Harwood RH, Blizard RA, Thomas A, Mann AH. Social support deficits, loneliness and life events as risk factors for depression in old age. The Gospel Oak Project VI. Psychol Med 1997;27(2):323–32.
Heikkinen R, Kauppinen M. Depressive symptoms in late life: a 10-year follow-up. Arch Gerontol Geriatr. 2004;38(3):239–50.
Cacioppo JT, Hughes ME, Waite LJ, Hawkley LC, Thisted RA. Loneliness as a specific risk factor for depressive symptoms: cross-sectional and longitudinal analyses. Psychol Aging. 2006;21(1):140–51.
Cacioppo JT, Hawkley LC, Thisted RA. Perceived social isolation makes me sad: 5-year cross-lagged analyses of loneliness and depressive symptomatology in the Chicago Health, Aging, and Social Relations Study. Psychol Aging. 2010;25(2):453–63.
Alpass FM, Neville S. Loneliness, health and depression in older males. Aging Ment Health. 2003;7(3):212–6.
Adams KB, Sanders S, Auth EA. Loneliness and depression in independent living retirement communities: risk and resilience factors. Aging Ment Health. 2004;8(6):475–85.
Anderson CA, Harvey RJ. Brief report: discriminating between problems in living: an examination of measures of depression, loneliness, shyness, and social anxiety. J Soc Clin Psychol. 1988;6(3–4):482–91.
Deniro DA. Perceived alienation in Individs with residual-type schizophrenia. Issues in Mental Health Nursing. 1995;16(3):185–200.
Neeleman J, Power MJ. Social support and depression in three groups of psychiatric patients and a group of medical controls. Soc Psychiatry Psychiatr Epidemiol. 1994;29:46–51.
Heinrich LM, Gullone E. The clinical significance of loneliness: a literature review. Clin Psychol Rev. 2006 October;26(6):695–718.
Bancroft JH, Skrimshire AM, Simkin S. The reasons people give for taking overdoses. Br J Psychiatry J Ment Sci. 1976;128:538–48.
Birtchnell J, Alarcon J. Depression and attempted suicide: a study of 91 cases seen in a casualty department. Br J Psychiatry J Ment Sci. 1971;118(544):289–96.
Nordentoft M, Rubin P. Mental illness and social integration among suicide attempters in Copenhagen. Comparison with the general population and a four-year follow-up study of 100 patients. Acta Psychiatr Scand. 1993;88(4):278–85.
Tilvis RS, Kahonen-Vare MH, Jolkkonen J, Valvanne J, Pitkala KH, Strandberg TE. Predictors of cognitive decline and mortality of aged people over a 10-year period. J Gerontol Ser A Biol Med Sci. 2004;59(3):M268–74.
Wilson RS, Krueger KR, Arnold SE, Schneider JA, Kelly JF, Barnes LL, Tang Y, Bennett DA. Loneliness and risk of Alzheimer disease. Arch Gen Psychiatry. 2007;64(2):234–40.
Kane M, Cook L. Dementia 2013: the hidden voice of loneliness. London: Alzheimer’s Society; 2013.
Heikkinen RL, Berg S, Avlund K, Timo T. Depressed mood: changes during a five-year followup in 75 year-old men and women in three Nordic localities. Aging Clin Exp Res. 2002;14:16–28.
Orth-Gomer K, Unden A, Edwards M. Social isolation and mortality in ischemic heart disease. Acta Medica Scandinavica. 1988;224(3):205–15.
Herlitz J, Wiklund I, Caidahl K, Hartford M, Haglid M, Karlsson BW, et al. The feeling of loneliness prior to coronary artery bypass grafting might be a predictor of short- and long-term postoperative mortality. Eur J Vasc Endovasc Surg. 1998;16(2):120–5.
Sorkin D, Rook KS, Lu JL. Loneliness, lack of emotional support, lack of companionship, and the likelihood of having a heart condition in an elderly sample. Ann Behav Med. 2002;24(4):290–8.
Fox CM, Harper AP, Hyner GC, Lyle RM. Loneliness, emotional repression, marital quality, and major life events in women who develop breast cancer. J Community Health. 1994;19(6):467–82.
Steptoe A, Owen N, Kunz-Ebrecht SR, Brydon L. Loneliness and neuroendocrine, cardiovascular, and inflammatory stress responses in middle-aged men and women. Psychoneuroendocrinology. 2004 June;29(5):593–611.
Pressman SD, Cohen S, Miller GE, Barkin A, Rabin BS, Treanor JJ. Loneliness, social network size, and immune response to influenza vaccination in college freshmen. Health Psychol. 2005;24(3):297.
Perlman D, Peplau LA. Toward a social psychology of loneliness. Pers Relat. 1981;3:31–56.
de Jong GJ, van Tilburg T, Dykstra P, Vangelisti A, Perlman D. Loneliness and social isolation. The Cambridge handbook of personal relationships. 2005:485–500.
Victor CR, Scambler SJ, Bowling A, Bond J. The prevalence of, and risk factors for, loneliness in later life: a survey of older people in Great Britain. Ageing & Society. 2005;25(6):357–75.
Victor C, Scambler S, Bond J, Bowling A. Being alone in later life: loneliness, social isolation and living alone. Rev Clin Gerontol. 2000;10(04):407–17.
Dykstra PA, Van Tilburg TG. Gierveld JdJ. Changes in older adult loneliness: results from a seven-year longitudinal study. Research on aging. 2005;27(6):725–47.
Wenger GC, Burholt V. Changes in levels of social isolation and loneliness among older people in a rural area: a twenty–year longitudinal study. Can J Aging. 2004;23(2):115–27.
Hawkley LC, Hughes ME, Waite LJ, Masi CM, Thisted RA, Cacioppo JT. From social structural factors to perceptions of relationship quality and loneliness: the Chicago health, aging, and social relations study. J Gerontol Ser B Psychol Sci Soc Sci. 2008;63(6):S375–84.
Cacioppo JT, Cacioppo S. Social relationships and health: the toxic effects of perceived social isolation. Soc Personal Psychol Compass. 2014;8(2):58–72.
Luanaigh CÓ, Lawlor BA. Loneliness and the health of older people. Int J Geriatr Psychiatry. 2008;23(12):1213–21.
Hawkley LC, Cacioppo JT. Aging and loneliness: downhill quickly? Curr Dir Psychol Sci. 2007;16(4):187–91.
Pinquart M, Sorensen S. Influences on loneliness in older adults: a meta-analysis. Basic Appl Soc Psychol. 2001;23(4):245–66.
World Health Organization. World report on ageing and health. Luxembourgh: World Health Organization; 2015.
World Health Organization. Global Health and Ageing. Geneva: World Health Organization; 2011.
Mcann A, Mackie P, Connacher A. Scottish isolation and loneliness: what is the sco;pe for public health action? Edinburgh: Scottish Public Health Network; 2017.
House JS, Landis KR, Umberson D. Social relationships and health. Science. 1988;241:545.
Holt-Lunstad J, Smith TB, Layton JB. Social relationships and mortality risk: a meta-analytic review. PLoS Med. 2010;7(7):859.
House JS, Robbins C, Metzner HL. The association of social relationships and activities with mortality: prospective evidence from the Techumseh community health study. Am J Epidemiol. 1982;116(1):123–40.
Barth J, Schneider S, von Kanel R. Lack of social support in the etiology and the prognosis of coronary heart disease: a systematic review and meta-analysis. Psychosom Med. 2010;72(3):229–38.
Holt-Lunstad J, Smith TB, Baker M, Harris T, Stephenson D. Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspect Psychol Sci. 2015;10(2):227–37.
Equal Opportunities Commisions. Age and Social isolation. Edinburgh: Scottish Government; 2015. Report No.: 5
Scottish Government. A connected Scotland: tackling social isolation and loneliness and building stronger communities. Strategy Conslutation Paper. Scottish Government: Edinburgh; 2018.
Department for digital, culture, media and sport. Call for evidence on approach to loneliness strategy. Consultation on Government loneliness strategy. London: Department for digital, culture, media and sport, Office for Civil Society; 2018.
Department of Health. Adult social care outcomes framework 2017/18: handbook of definitions. London: Department of Health; 2017.
Department of Health. Public health outcomes framework for England, 2013–16. London: Department of Health; 2012.
Scottish Government. Health and social care standards: my support, my life. Scottish Government: Edinburgh; 2017.
Valtorta NK, Kanaan M, Gilbody S, Hanratty B. Loneliness, social isolation and social relationships: what are we measuring? A novel framework for classifying and comparing tools. BMJ Open. 2016;6(4):e010799,2015–010799.
Hawkley LC, Cacioppo JT. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med. 2010;40(2):218–27.
Hawkley LC, Cacioppo JT. Loneliness and pathways to disease. Brain Behav Immun. 2003;17:98–105.
Lauder W, Mummery K, Jones M, Caperchione C. A comparison of health behaviours in lonely and non-lonely populations. Psychology, Health & Medicine. 2006;11(2):233–45.
Cacioppo JT, Hawkley LC, Crawford LE, Ernst JM, Burleson MH, Kowalewski RB, et al. Loneliness and health: potential mechanisms. Psychosom Med. 2002;64(3):407–17.
Kiecolt-Glaser JK, Garner W, Speicher C, Penn GM, Holliday J, Glaser R. Psychosocial modifiers of immunocompetence in medical students. Psychosom Med. 1984;46(1):7–14.
Benschop RJ, Geenen R, Mills PJ, Naliboff BD, Kiecolt-Glaser JK, Herbert TB, et al. Cardiovascular and immune responses to acute psychological stress in young and old women: a meta-analysis. Psychosom Med. 1998;60(3):290–6.
Cacioppo JT, Hawkley LC, Berntson GG, Ernst JM, Gibbs AC, Stickgold R, et al. Do lonely days invade the nights? Potential social modulation of sleep efficiency. Psychol Sci. 2002;13(4):384–7.
Cacioppo JT, Cacioppo S, Capitanio JP, Cole SW. The neuroendocrinology of social isolation. Annu Rev Psychol. 2015;66:733–67.
Hawkley LC, Thisted RA, Cacioppo JT. Loneliness predicts reduced physical activity: cross-sectional & longitudinal analyses. Health Psychol. 2009;28(3):354.
Åkerlind I, Hörnquist JO. Loneliness and alcohol abuse: a review of evidences of an interplay. Soc Sci Med. 1992;34(4):405–14.
Shankar A, McMunn A, Banks J, Steptoe A. Loneliness, social isolation, and behavioral and biological health indicators in older adults. Health Psychol. 2011;30(4):377.
Hawkley LC, Burleson MH, Berntson GG, Cacioppo JT. Loneliness in everyday life: cardiovascular activity, psychosocial context, and health behaviors. J Pers Soc Psychol. 2003;85(1):105.
de Jong Gierveld J. A review of loneliness: concept and definitions, determinants and consequences. Rev Clin Gerontol. 1998;8(01):73–80.
Mullins LC, Elston CH, Gutkowski SM. Social determinants of loneliness among older Americans. Genetic, Social, and General Psychology Monographs. 1996.
Krause N. Neighborhood deterioration and social isolation in later life. Int J Aging Hum Dev. 1993;36(1):9–38.
Belle DE. The impact of poverty on social networks and supports. Marriage Fam Rev. 1983;5(4):89–103.
Havinghurst R. Ageing in western society. The social challenge of ageing. London: Croom Helm; 1978. p. 15–44.
Hunt A. The elderly at home: a study of people aged sixty-five and over living in the Community in England in 1976. London: HMSO; 1978. Report No.: Social Survey Division, OPCS
Wenger GC, Davies R, Shahtahmasebi S, Scott A. Social isolation and loneliness in old age: review and model refinement. Ageing & Society. 1996;16(3):333–58.
Lowenthal MF, Robinson B. Social networks and isolation. Handbook of aging and the social sciences. 1976;5:432–56.
Hadley R, Webb AL. Loneliness, social isolation and old people: some implications for social policy. Age Concern; 1974.
Wenger CG. The supportive network: coping with old age. London: George Allen & Unwin; 1984.
West DA, Kellner R, Moore-West M. The effects of loneliness: a review of the literature. Compr Psychiatry. 1986;27(4):351–63.
Chen S, Conwell Y, Chiu HFK. Loneliness and aging in China–a public health problem in need of solutions. Int Psychogeriatr. 2014;26(11):1771–2.
Murphy F. Loneliness: a challenge for nurses caring for older people. Nursing older people. 2006;18(5):22–5.
Pels F, Kleinert J. Loneliness and physical activity: a systematic review. Int Rev Sport Exerc Psychol. 2016;9(1):231–60.
Courtin E, Knapp M. Social isolation, loneliness and health in old age: a scoping review. Health Soc Care Community. 2017;25(3):799–812.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–9.
de Jong GJ, Van Tilburg T. A 6-item scale for overall, emotional, and social loneliness confirmatory tests on survey data. Research on aging. 2006;28(5):582–98.
de Jong-Gierveld J, Kamphuls F. The development of a Rasch-type loneliness scale. Appl Psychol Meas. 1985;9(3):289–99.
Russell DW. UCLA Loneliness Scale (version 3): reliability, validity, and factor structure. J Pers Assess. 1996;66(1):20–40.
Hughs M, Waite L, Hawkley L, Cacioppo J. A short scale for measuring loneliness in large surveys. Research on aging. 2004;26(6):655–72.
World Health Organisation Europe. Lifestyle and behaviour change. Copenhagen: World Health Organisation; 1999. Report No.: EUR/ICP/LVNG 01 04 06
Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Comprehensive Physiology. 2012;2(2):1143–211.
Sampson M, McGowan J, Cogo E, Grimshaw J, Moher D, Lefebvre C. An evidence-based practice guideline for the peer review of electronic search strategies. J Clin Epidemiol. 2009;62(9):944–52.
Moher D, Liberati A, Tetzlaff J, Altman DG, Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
Centre for reviews and dissemination. Systematic reviews: CRD’s guidance for undertaking reviews in health care. University of York: Centre for Reviews and Dissemination; 2009.
Joanna Briggs Institute. Joanna Briggs Institute reviewers’ manual: 2014 edition. Australia: The Joanna Briggs Institute; 2014.
Wells GA, Shea BB, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses: Ottawa Hospital Research Institute [Internet]; 2014. Available from: http://www.ohri.ca/programs/clinical_epidemiology/nos_manual.pdf.
Deeks J, Higgins J, Altman D, Green S. Cochrane handbook for systematic reviews of interventions version 5.1. 0 (updated March 2011). The Cochrane Collaboration. 2011.
Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the conduct of narrative synthesis in systematic reviews. A product from the ESRC methods programme.Version. 2006;1.
Schünemann H, Brożek J, Guyatt G, Oxman A. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013: The GRADE Working Group, 2013. Available at https://gdt.gradepro.org/app/handbook/handbook.html.
HILL AB. The environment and disease: association or causation? Proceedings of the Royal Society of Medicine. 1965;58:295–300.
Henriksen M, Creaby MW, Lund H, Juhl C, Christensen R. Is there a causal link between knee loading and knee osteoarthritis progression? A systematic review and meta-analysis of cohort studies and randomised trials. BMJ Open. 2014;4(7):e005368,2014–005368.
Mente A, de Koning L, Shannon HS, Anand SS. A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch Intern Med. 2009;169(7):659–69.
Doughty S. More than three million elderly people face a life of loneliness because of family break-ups and a lack of friendly neighbour. The Daily Mail2012;15th November 2012.
Khaleeli H. Britain’s loneliness epidemic. The Guardian2013 22nd January 2013.
Tarver N. Half of adults in England experience loneliness. BBC News. 2013 18th October 2013.
Acknowledgements
We thank Rob Polson, librarian at the Centre for Health Sciences, Inverness for advising on the literature search and referencing software.
Funding
The study was funded as part of principal author’s doctorate research study by University of Stirling.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Author information
Authors and Affiliations
Contributions
MM conceived of the study, formulated its design and methodology and drafted the manuscript. HF and JC advised upon the study objectives and methodology and helped with drafting the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Author’s information
The principal author, MM, has undertaken this study as part fulfilment of his research doctorate study.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Medline Search Strategy. File contains the Medline search strategy syntax used in the review including keywords and Mesh subject headings which will be adapted for other databases included within the systematic review. (DOCX 29 kb)
Additional file 2:
Date Extraction Form Variables. File contains the details on the variables and their groupings to be extracted and recorded on the study data extraction form for the systematic review (DOCX 13 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Malcolm, M., Frost, H. & Cowie, J. Loneliness and social isolation causal association with health-related lifestyle risk in older adults: a systematic review and meta-analysis protocol. Syst Rev 8, 48 (2019). https://doi.org/10.1186/s13643-019-0968-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-019-0968-x