
Abstract
Background
Universal health coverage means that all people can access essential health services without incurring financial hardship. Even in countries with good service coverage and financial protection, the progress towards universal health coverage may decelerate or be limited with respect to the growing older population. This study investigates the incidence/prevalence, determinants, and consequences of catastrophic health expenditure (CHE) and unmet need for healthcare and assesses the potential heterogeneity between younger (≤ 64 years) and older people (65 years≤).
Methods
Utilising an annual nationally representative survey of Japanese aged 20 years and over, we estimated the incidence of CHE and unmet need for healthcare using disaggregated estimates by household members’ age (i.e. ≤64 years vs. 65 years≤) between 2004 and 2020. Using a fixed-effects model, we assessed the determinants of CHE and unmet need along with the consequences of CHE. We also assessed the heterogeneity by age.
Results
Households with older members were more likely to have their healthcare needs met but experienced CHE more so than households without older members. The financial consequences of CHE were heterogeneous by age, suggesting that households with older members responded to CHE by reducing food and social expenditures more so than households without older members reducing expenditure on education. Households without older members experienced an income decline in the year following the occurrence of CHE, while this was not found among households with older members. A U-shaped relationship was observed between age and the probability of experiencing unmet healthcare need.
Conclusions
Households with older members are more likely to experience CHE with different financial consequences compared to those with younger members. Unmet need for healthcare is more common among younger and older members than among their middle-aged counterparts. Different types and levels of health and financial support need to be incorporated into national health systems and social protection policies to meet the unique needs of individuals and households.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Financial protection in health and access to health services
Universal health coverage (UHC) means that all people have access to essential health services without being exposed to financial hardship. Progress towards UHC has been monitored by the World Health Organization through the essential service coverage and financial protection from large household expenditure on health, or catastrophic health expenditure (CHE) [1,2,3]. The 2023 UHC Global Monitoring Report alarms that progress towards UHC is off track from the Sustainable Development Goals (SDGs) targets by 2030 even before the COVID-19 pandemic: while essential service coverage improved in almost all countries from 2000 but has stalled since 2015, CHE has worsened or hardly changed in most countries [3]. The progress towards UHC may further decelerate or be limited with respect to the growing older populations: they are more likely to experience financial difficulties associated with health expenditure or forego care owing to financial and other barriers as they tend to suffer from chronic conditions and require frequent and intense care than younger people [4, 5]. Therefore, financial protection in health and access to health services among older populations needs further investigation in terms of the determinants, consequences, and required policies in order to ensure that no one is left behind [5,6,7].
Ageing and healthcare access: CHE and unmet need
In the human capital model (i.e. Grossman model), health is affected by choices [8, 9]: Individuals optimise their lifelong utility, as determined by their health status and consumption of normal goods, subject to budget and time constraints. To avoid the deterioration of health concurrent with ageing, individuals make an investment in health, engaging in healthy behaviours, including healthcare utilisation and exercise. Even though healthcare utilisation is exogenous in some cases (e.g. use of emergency room owing to acute diseases such as stroke), disparities in health and healthcare access can arise from differences in individual’s observable characteristics (e.g. demographic and socioeconomic status) and unobserved heterogeneities (e.g. preference for healthcare services).
Disparities in health and healthcare access across different age groups and socioeconomic status can lead to heterogeneous probabilities of experiencing CHE [10,11,12,13,14,15,16,17,18] and unmet need [19,20,21,22,23,24,25] due to differences in financial conditions and health needs. Assuming that older people need more care than younger people owing to more frequent chronic conditions, health gains (or losses) from investing (or not investing) in their health can be larger among older people. These health gains can bring positive economic effects, given that large social costs arise due to health issues among older people, including productivity loss and medical and long-term care costs [26, 27]. Accordingly, older people or households with older family members are more likely to use care and experience CHE than younger people or households without older members [10,11,12,13, 16,17,18]. Conversely, the relationship between unmet need and age is complex. By using more care, older people may meet their healthcare needs. Alternatively, they may experience unmet need because they (i) eventually forego care owing to financial difficulties from CHE; or (ii) increase the chance of forgoing care from the increased number of attempts to access healthcare services due to their greater health needs, or both. Younger people may also forgo care frequently owing to their mild symptoms, high opportunity costs (i.e. workers foregoing earnings because of healthcare utilisation), and higher co-payment rates than older people in some countries. However, some studies revealed that older people tend to experience more unmet need compared to younger people [28], and others showing opposite results [21, 22, 25].
While some studies have revealed an association between unmet need and subsequent health deterioration [29, 30], evidence of the consequences of CHE remains scarce. As for health consequences, CHE can be associated with both improvement and worsening of an individual’s health, which could be related to the overuse or underuse of care and the quality of health services. However, we will not focus on its health consequences due to empirical challenges, including endogeneity, the nature of healthcare services (e.g. the incomplete contract and moral hazard induced by the supply side [31]), and the lack of an objective measure of individuals’ health status. Aside from health consequences, unmet need and financial consequences are potential outcomes of concern. First, the relationships between healthcare utilisation, CHE and unmet need are complex. Greater healthcare utilisation may satisfy an individual’s need for healthcare [32], while it can also cause subsequent CHE and financial hardship that may suppress their healthcare utilisation and lead to health deterioration. Second, CHE can affect an individual’s non-health consumption, income, and wealth through (i) financial pressure from CHE, and (ii) restricted choices in these activities because of health issues. Accordingly, the heterogeneity between younger and older people is of concern. Based on the life-cycle model [33], younger people rely on their incomes, while older people, particularly after retirement, obtain their incomes mainly from pension benefits and depend on their savings. Therefore, older people may be less likely to experience financial difficulties because their income is not linked to their health status. Moreover, even with CHE, some older people may not suffer from financial hardship as they tend to have more savings, smaller debts, and fewer expense categories (e.g. lower expenditures for education and child support) compared to younger people [34]; therefore, they may have greater ability to pay. Accordingly, the consequences of CHE and the heterogeneity across age groups must be assessed to enhance the progress monitoring of UHC and accountability.
Contributions of this study
This study’s focus on the heterogeneity between younger and older people expands the extant literature in three main ways. First, we assess the heterogeneity in the financial consequences of CHE between households with and without older members. Owing to differences in income sources, ability to pay, and consumption patterns between younger and older people, the financial consequences of CHE can vary for these groups. However, this has not been empirically assessed so far. If older people do not experience financial difficulties, even with CHE, then this suggests that in the context of population ageing, the progress monitoring of financial protection for UHC using the current approach is not sufficient, requiring more complementary indicators. Second, we analyse the relationship between age and the probability of experiencing unmet need in greater detail. In their assessment of the heterogeneity across age groups in terms of unmet healthcare need, the previous studies have not fully considered a potential non-linear relationship between age and unmet need; instead, they have assumed a linear relationship between age and unmet need or have used an arbitrary dummy variable for age (e.g. by 10 or 20 years old) [20,21,22, 25, 28]. Assessing such heterogeneity is important for understanding the determinants of unmet need because both younger and older people can forego care for different reasons. Third, we analyse the association between CHE and unmet need as this has lacked empirical investigation, and the relationship remains inconclusive. While it might be assumed that lower incidence of CHE indicates stronger financial protection which improves access to health care and results in lower unmet need, it is also conceivable that lower incidence of CHE is an indication of lower utilisation of health care owing to poorer access which results in higher unmet need.
Institutional settings
To evaluate the determinants and consequences of CHE and unmet need, understanding the institutional setting is important. Accordingly, this section provides a brief overview of Japan’s medical care system.
Healthcare insurance coverage
Under public universal health insurance, all citizens in Japan can receive one of the world’s highest levels of service coverage [35, 36]. This coverage includes a wide range of in-kind benefits and cash benefits, such as consultations, treatments, drugs, home-visit nursing, benefits related to hospitalisation (e.g. food expenses), benefits for high-cost medical expenses, dentistry, and a childbirth lump-sum allowance. Under the employee- and community-based social insurance system, insured people pay insurance premiums, which account for half of the financing source of the healthcare insurance system. To utilise medical care services, insured people bear the cost of out-of-pocket payments (OOP) at a fixed co-payment rate of 20% for pre-school children, 30% for people aged 6–69 years, 20% for people aged 70–74 years, and 10% for people aged 75 years and over (30% for people aged 70 years or over whose income level is comparable with that of employed people). These rates are identical regardless of the insured people’s residential location. Furthermore, in many regions, medical care for newborns, children, and adolescents is subsidised by the local governments; therefore, some citizens can use these services with OOP at below 20% of the co-payment rate or without OOP. Although the co-payment rates are seemingly high, they account for only about 12% of healthcare financing (the remaining 40% is managed by public expenditure), meaning that individuals can use medical care at low OOP cost.
To reduce patients’ financial burden, cost containment is required through the efficient management of the medical care system. Owing to the nature of medical care services that require professional knowledge, patients typically do not have knowledge of the services that they need (i.e. a principal-agent problem with imperfect contracts). Therefore, cost containment can be achieved through supply-side control [31]. Japan’s medical care system has three main contributors to cost containment [37]. First, outpatient services are the main ways for service delivery with a low level of inpatient care use, even with the high per-capita number of hospital beds for historical reason (i.e. the share of outpatient care is large even in tertiary hospitals). Second, the ubiquitous payment system, with the national uniform fee schedule for reimbursement, contributes to improving efficiency (i.e. reduced administrative costs) and equity (i.e. the same benefit package throughout Japan). The prices of drugs, devices, and services, mainly for outpatient services, are biennially revised on an item-by-item basis [38]. Third, peer-reviewed medical claims and on-site audits of medical records are conducted for cost containment and quality control. Therefore, patients’ financial burden is mitigated by curbing the costs of medical care through these supply-side controls.
Medical care access
Japan’s medical care system does not adopt the gatekeeping or waiting-list system used by general practitioners, meaning that patients can freely choose a clinic or a hospital for their first visit. Furthermore, there are no constraints on patients’ demands for healthcare, thus they can use healthcare services whenever they feel they need them. To utilise specialist care at large hospitals (e.g. university hospitals) without referral from a physician, patients must bear a certain amount of a premium fee: JPY7,000 (≈ USD50) at the initial visit and JPY2,500 (≈ USD20) for the follow-up visits. However, the fee for services is identical when patients receive the same treatment from any physician at a clinic or any specialist at a hospital. With this free access system, citizens institutionally have easy access to medical care services on demand.
Financial protection
Even with the low cost of OOP, patients can encounter financial difficulties from excessive OOP in instances in which they have severe or chronic health conditions and thus need intensive and continual medical care. To mitigate this, two types of financial protection are available. First, citizens can receive a tax deduction when the yearly OOP of medical care usage or over-the-counter drugs for themselves and their household members exceeds a certain amount. Second, to curb excessive financial burden, the ceiling amount for monthly OOP is determined based on an individual’s income level and age. If their OOP exceeds this level, the surplus is reimbursed or provided as in-kind benefits without OOP. When a patient reaches this level more than thrice in 12 months, the ceiling amount is reduced to lessen the financial burden. Furthermore, this financial support is available when the combined yearly costs of medical care and public long-term care become excessive; for instance, when multiple household members have long-term care needs. Some insurers provide additional financial protection by setting their own ceiling amount of medical expenditure lower than the national level.
Moreover, individuals who receive low incomes can receive financial support, such as the reduction of and exemption from insurance premiums, financial support for OOP of single-parent households who receive low incomes, and additional benefits for expenses during hospitalisation (e.g. benefits for food expenses). Some of this support varies across insurance societies in terms of eligibility and benefit levels. Furthermore, if a citizen has no assets, no family or relative to ask for financial assistance, an extremely low income (i.e. lower than the minimum cost of living), and is incapable of working owing to disease or injury, then they are eligible for public assistance. Most of these recipients are covered by medical assistance and do not have to bear the cost of insurance premiums and OOP. In sum, Japan’s medical care system provides various types of policies to ensure access to care and financial protection. Other types of financial and non-financial aids from the government are also available for those needing temporal support, including self-reliance support benefits for households with financial difficulties; injury and sickness allowance (for work-unrelated health issues among insured people of occupation-based health insurance); and postponement, reduction, or exemption of tax and social insurance premiums for other types of care than medical care (e.g. residence tax and insurance premiums for pensions and long-term care). Moreover, conditional on periods of contribution payment, individuals are eligible for disability pension benefits when they are restricted from working owing to functional limitations from health issues.
Methods
Data
The data for this study are retrieved from the Japan Household Panel Survey (JHPS/KHPS), an annual nationally representative household survey of Japanese aged 20 years or over. The JHPS/KHPS is a unification of the Keio Household Panel Survey (KHPS) and Japan Household Panel Survey (JHPS), which were originally separate but have many questionnaires in common, including those on household structure, individual attributes, academic background, employment status, and economic conditions. Both surveys adopt stratified two-stage random sampling that uses 24 regional and city classifications, with the number of survey subjects in each classification set in accordance with their population size as the first stage of sampling. Subsequently, the participants are selected from basic resident registers based on designated numbers and sampling intervals as the second stage. The KHPS was first conducted in 2004, with approximately 7,000 individuals from 4,000 households, and added new samples in 2007 and 2012. The JHPS was first conducted in 2009, with 4,000 individuals, and implemented a new sample in 2019. The recovery rates of the follow-up surveys, calculated as (Completed – Revival) / Completed in last year×100 were 82.7 – 94.2% [39]. The survey information is available in greater detail on the project website [39].
This study analysed the unbalanced panel data during 2004–2020 because not all variables used in our analyses were measured in every wave. In a study that utilises panel data, potential bias owing to sample attrition should not be ignored. To partially address non-response bias, all analyses were weighted by inverse probabilities that responded to each subsequent wave and were estimated by logit models, conditional on respondents’ age, sex, marital status, education, employment status, and residential area at the baseline. Furthermore, we restricted our analysed sample to individuals or their spouses who were household heads, since they could provide accurate information on their households compared to other household members. This led to the final sample size of at most 65,564 observations by 7,898 unique individuals.
Financial hardship
To define financial hardship owing to excessive health expenditure, we used two measures, CHE and impoverishing health expenditure (IHE), obtained from the JHPS/KHPS questionnaire on household consumption in the past month. Following the definition from previous studies and the indicator for the progress monitoring of SDG 3.8.2 [1, 40,41,42], CHE was defined as health expenditure beyond the 10% and 25% thresholds of total household consumption.
To complement CHE, IHE was measured as the changes in poverty headcount for equalised household income with and without out-of-pocket expenditure [43]. We used the country poverty line of each year from the national government [44] and imputed it by linear interpolation when the poverty lines were not provided by the government. In addition, to further complement our analysis, we used a continuous variable of the proportion of households’ total health expenditure among total consumption instead of dichotomised CHE in some analyses.
Unmet need
The JHPS/KHPS asks, ‘During the past year, did you receive treatment, such as an outpatient or inpatient service?’ There are six response options: [1] ‘Did nothing as healthy’, [2] ‘Did nothing despite having symptoms’, [3] ‘Went to a hospital or clinic’, [4] ‘Hospitalised’, [5] ‘Purchased a patent medicine’, and [6] ‘Other’. To define respondents’ unmet healthcare need, we created a dichotomised variable, coded as 1 for the response, ‘Did nothing despite having symptoms’ and 0 otherwise. We excluded those who did not need healthcare services because they were healthy. Appendix note 1 provides the descriptions of measures of financial protection and access to health services.
Empirical strategies
Financial hardship
Incidence. To illustrate the number of respondents who experienced financial hardship owing to health expenditure, we first calculated the incidence of CHE and IHE in each year of the survey. To measure the potential heterogeneity across age groups, households with at least one member aged 65 years or older (or aged 75 years or older) were compared to households with members aged 64 years or younger.
Determinants. We assessed the determinants of those experiencing financial hardship by estimating a linear probability model, expressed as follows:
where \({CHE}_{it}\) denotes the CHE status of household i in year t; \({\varvec{X}}_{it}\) is a vector of the independent variables, comprising a household’s demographic and socioeconomic variables; and \({\epsilon }_{it}\) is the stochastic disturbance. The independent variables \({\varvec{X}}_{it}\), which can affect the probability of financial hardship, comprise the following household characteristics detected in the previous studies [10,11,12,13,14,15,16,17,18]: Co-residing with at least one member aged 65 years or older, education (i.e. whether a household head graduated from university or higher), employment status (i.e. whether a household head was in paid employment), house ownership, the number of household members, and equivalised household income (gross) and savings adjusted for the 2020 base consumer price index. Contrary to some of these studies, we did not include the household heads’ age in a model to avoid collinearity with co-residence with older family members, which were the case when household heads were aged 65 years or older. When including age in the model, non-linear relationships between age and experienced CHE were considered by assessing the quadratic and cubic relationships between age and CHE. While we adopted a model with a significant coefficient for either quadratic or cubic relationships in terms of age, we used a quadratic model for the presence of neither quadratic nor cubic relationships. Income and savings, after being equivalised by household size and linearly interpolated to minimise missing data, were transformed via the inverse hyperbolic sine transformation to deal with their skewness when containing a zero value [45]. We did not include health-related variables because (i) the survey did not include rich health information on household members other than respondents, and (ii) by assuming that older age may be associated with worse health, we may have missed findings on age heterogeneity by controlling for household members’ health status, particularly when this is a consequence of older age.
We also controlled for city-by-year fixed-effects (\({\tau }_{lt}\)) and individual fixed-effects (\({u}_{i}\)). This allowed us to control for unobserved factors that occurred in city l in year t (e.g. policy changes, economic cycle, geographical location, infrastructure, and healthcare resources) and unobserved time-invariant heterogeneity across individuals (e.g. sex of respondents and preference for healthcare use). To control for high-dimensional fixed-effects, we conducted estimations using a Stata command: reghdfe [46]. To address potential correlations within individuals, we also estimated cluster robust standard errors. To better understand how the nature of CHE could differ according to the age of household members, we conducted a separate analysis of households with and without a member aged 65 years or older.
Consequences. Even though older people may experience financial hardship owing to frequent health expenditure than their younger counterparts, the financial consequences can differ because of the variation in both ability to pay and consumption patterns between younger and older people [33]. Therefore, we investigated the heterogeneity between households with and without an older member to reveal how excessive health expenditure puts pressure on other non-health household expenditures (i.e. food, culture and recreation, social relationships, and education). Furthermore, we evaluated the financial consequences of financial hardship as follows:
where the association of CHE for household i in year t-1 (\({CHE}_{it-1}\)) with financial outcomes in year t \(({F}_{it})\) is assessed, controlling for independent variables and the same fixed-effects as those in Eq. (1). For financial outcomes, we used income and savings (as defined earlier). We further evaluated the potential heterogeneity between households with and without an older member.
Unmet need
Regarding unmnet need, we conducted the analyses to answer three questions: (i) whether the probability of experiencing unmet need differed between younger and older people, (ii) whether the determinants of unmet need differed between younger and older people, and (iii) whether CHE was associated with subsequent unmet need.
Prevalence. We estimated the individual-level prevalence of respondents experiencing unmet need in addition to the heterogeneity between younger and older people. As unmet need was measured with individuals as the unit, respondents who were aged 65 years or older were compared to respondents who were 20–64 years.
Determinants. To assess the determinants of unmet need, it is important to include need variables, which directly affect an individual’s health need, and non-need variables, which indirectly affect their need [47]. Accordingly, the probability of reporting unmet need is expressed as:
where \({Need}_{it}\) denotes the need variables of individual i in year t, and \({Non-need}_{it}\) represents the non-need variables. In practice, distinguishing between need and non-need variables is not easy, since individual characteristics, such as demographic factors, can be regarded as both types of variables. For example, chronological age may be viewed as a non-need variable, while older age may be regarded as a factor that influences health status. To cover a wide range of factors, we included the respondents’ characteristics as the following demographic, socioeconomic, and health-related variables identified as determinants of unmet need by the previous studies [19, 21, 22, 24, 25, 28]: Age, marital status, employment status, house ownership, household size, equivalised household income and savings adjusted for the 2020-base price, self-rated health, smoking status (i.e. current smoker or not), alcohol consumption (i.e. current drinker or not), and per-week days of exercise. Non-linear relationships between age and experienced unmet need were considered in the same way as in the analysis of CHE. The model was estimated using a linear probability model, with additional controls for city-by-year fixed-effects and individual fixed-effects. These fixed-effects controlled for unobserved need and non-need variables, such as national-level policy changes, access to healthcare facilities at the city level, health status of individuals before joining the survey, and individual preferences for healthcare. To assess the heterogeneity across age groups, we compared the results as estimated from the respondents aged 64 years or younger with those aged 65 years or older.
CHE and unmet need
Excessive levels of health expenditure can make individuals forgo healthcare utilisation owing to budget constraints. Conversely, their need for healthcare may be met as CHE would occur from their utilisation of healthcare. Therefore, we assessed whether CHE at wave t-1 increased or decreased the probability of experiencing unmet healthcare need at wave t using a fixed-effects linear-probability model in the same manner as described earlier in the determinants of unmet need.
Results
Incidence and prevalence
The incidence of CHE among the JHPS/KHPS sample was between 8.0 and 12.4% at the 10% threshold and 1.1–2.2% at the 25% threshold during the 2004–2020 period (Appendix Table A-1). Although the health expenditure data of the JHPS/KHPS were obtained as the values in the last month of the survey, which differed from the official government estimates (i.e. the monthly average in the year, calculated by the data collected every month), our estimates were comparable to the official government estimates. Furthermore, in households in which all members were aged 64 years or younger, the incidence rate was 5.2–9.9% at the 10% threshold and 0.7–1.7% at the 25% threshold (Appendix Table A-2). Meanwhile, the incidence was higher in households in which at least one person was aged 65 years or over, at 10.9–22.9% at the 10% level and 1.9–4.2% at the 25% level. Moreover, the incidence rate of IHE was around 1% for the entire sample in 2004–2018, with a higher rate in households with older people that ranged from 1.2 to 4.0% (Appendix Table A-3). Conversely, the incidence rate was low among households that only had members aged 64 years or younger, at less than 1% in most years of the survey.
The prevalence rate of unmet need for healthcare moderately declined during the later periods of the survey, and ranged from 4.7 to 13.1% in the entire sample (Appendix Table A-4). People aged 64 years or younger were more likely to forego healthcare compared with those aged 65 years or older; the prevalence rate was 6.2–15.5% among younger people and 1.8–8.6% among older people.
Table 1 shows the descriptive statistics for the household- and individual-level variables used herein. Throughout the study period, 9.8% and 7.7% of respondents had experienced CHE at the 10% threshold and unmet healthcare need, respectively. On average, the respondents spent 4.4% of their total household consumption on health expenditure. The average age of respondents or spouses (i.e. household heads) was approximately 53 years. Among the entire sample, 31.4% of the households contained at least one member aged 65 years or over. Appendix Figure A-1 presents the differences in income and savings by the presence of an older household member and CHE status. Based on the median values, households with at least one member aged 65 years or older had lower incomes but higher savings. Among households with a member aged 65 years or over, both the incomes and savings of the households experiencing CHE were slightly lower than those without CHE experience.
Determinants
[1] CHE.
Table 2 presents the analysis results of the determinants of CHE at the 10% and 25% thresholds. Having at least one member aged 65 years or over was associated with a higher probability of experiencing CHE at the 10% threshold (\(\beta\): 0.02, standard error [SE]: 0.01), while the experience of CHE at the 25% threshold showed no association. Furthermore, households with higher incomes (\(\beta\): -0.01, SE: 0.00) and household heads who had a paid occupation (\(\beta\): -0.04, SE: 0.01) were less likely to experience CHE at the 10% threshold. The results were similar even when changing the age for a variable indicating co-residence with older household members from 65 + to 75+. CHE at the 25% threshold was associated with co-residence with a member aged 75 or older.
Table 3 shows the analysis results of the heterogeneity in the determinants of CHE by the presence of an older household member. Among the households with only members aged 64 years or younger, those with higher incomes were less likely to experience CHE. In both household types, households were less likely to experience CHE when the household heads had a paid occupation (\(\beta\): -0.04, SE: 0.01 for both types of households). Furthermore, the association between the ages of the household heads and the probability of experiencing CHE revealed a U-shaped relationship among households without older members.
[2] Unmet healthcare need.
Table 4 presents the analysis results of the determinants of unmet healthcare need. We have two main findings. First, age was associated with the probability of experiencing unmet need for healthcare. Figure 1 shows this relationship and reveals a U-shaped relationship: the lowest probability of unmet need is for the age 55–60 years. Conversely, people younger and older than 55–60 were increasingly more likely to report having forgone care. Second, only among younger people, a higher amount of savings and bad self-rated health were associated with the lower probability of experiencing unmet need while being employed was associated with the higher probability.

Age and unmet need for healthcare. Note: The presentation of this figure is based on the estimation from the model All in Table 4; Line represents marginal effects of age on experienced unmet need with the shaded area representing the 95% confidence interval
Consequences of CHE
[1] Financial consequences.
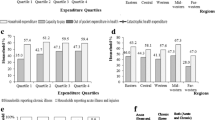
Appendix table A-5 and Fig. 2 show the results of the association between CHE and food, culture or recreation, social, and education expenditures, and their heterogeneity by the presence of an older household member. CHE at 10% was associated with lower levels of food, culture or recreation, social expenditure, and education, with coefficients ranging from − 0.03 to -0.01. Furthermore, reduced levels of food and social expenditure by CHE were more remarkable in households with older members (\(\beta\): -0.01, SE: 0.00), compared to households with only members aged 64 years or younger who were more sensitive to reducing expenditure for education. Similar results were obtained even using a continuous rate of total health expenditure among total consumption.

Heterogeneity by the presence of an older household member in the association between catastrophic health expenditure and food, culture/recreation, and social expenses. Note: CHE10 refers to catastrophic health expenditure at a 10% threshold. CI stands for a confidence interval. Each expenditure (% of total consumption) was transformed by the inverse hyperbolic sine transformation. Full results are presented in Appendix Table A-5
Appendix table A-6 and Fig. 3 present the results of the financial consequences of CHE and the heterogeneity between households with and without older members. Households with only members aged 64 years or younger were more likely to experience an income decline in the following year after experiencing CHE (\(\beta\): -0.02, SE: 0.01). Meanwhile, it was not observed among households with older members. The association between savings and CHE was not observed for both household types. With a continuous health expenditure variable, the results became less clear.

Heterogeneity by the presence of an older household member in financial consequences of catastrophic health expenditure. Note: CHE10 refers to catastrophic health expenditure at a 10% threshold. CI stands for a confidence interval
[2] CHE and unmet need.
Table 5 shows the association between CHE and unmet healthcare need in the following year; no association was observed. In contrast, the continuous variable for total health expenditure was negatively associated with unmet need.
Discussion
This study assesses the incidence/prevalence, determinants, and consequences of CHE and unmet healthcare need and the observable heterogeneities between younger and older people. We have five main findings. First, among households with older people, the incidence of experiencing CHE was high and unmet need was low, compared to their younger counterparts. Second, households with older members were more likely to experience CHE than households with only members aged 64 years or younger. Moreover, households with higher incomes and household heads in paid employment had a lower probability of experiencing CHE. Third, a U-shape relationship was observed between age and the likelihood of experiencing unmet need. Among younger people, being in paid employment had a higher probability of experiencing unmet need, while higher savings and negative self-rated health were associated with a lower probability of experiencing unmet need. Fourth, after experiencing CHE, households with older people tended to reduce their expenditure on food and social relationships more so than households with only younger members. Meanwhile, households with only younger members experienced a decline in income in the following year after experiencing CHE, while households with older members did not. Fifth, there was no association between experiencing CHE and having unmet need in the following year; however, the continuous variable for total health expenditure was negatively associated with unmet need.
Households with older members (or older people themselves) are more likely to experience CHE and have a lower prevalence of unmet need compared to households that only have younger members (or younger people). Although previous study revealed that healthcare use was negatively associated with unmet need [32], our analysis revealed no significant association between CHE and unmet need. As discussed in the Introduction section, CHE can affect unmet need both positively and negatively, cancelling out the overall effect. Specifically, greater healthcare use can reduce unmet need but can also result in CHE, going by our finding regarding continuous variable for total health expenditure. Conversely, greater healthcare use can cause financial difficulties, such as CHE, and eventually lead people to forgo needed care, resulting in greater unmet need. Moreover, by needing more care, the chance of forgoing care may increase owing to the increased number of attempts to access healthcare services. In this way, it is important to try to understand the complexity and nuances that underlie the absence of a statistical relationship between CHE and unmet need. In addition, the threshold of CHE may not be appropriate to capture financial hardship as the continuous variable for total health expenditure was associated with unmet need.
Comparing our estimate of the incidence of CHE at 10% in Japan with estimates in other regions in 2017 and 2019, it was lower than both the global and the high-income group’s medians [3, 4]. When decomposing this into households with and without older members, both of the estimates in Japan were lower than or similar to the ones in the high-income groups. Moreover, the prevalence of unmet needs among the total and older populations was lower than the ones in most countries in the World Health Organization’s regions of Americas and the Europe [35]. Based on these indicators, Japan’s situation regarding financial protection in health may be considered better than in many other countries.
CHE resulted in different consequences between households with and without older members. Experience of CHE led both types of households to reduce their expenditure on food, culture and recreation, and social relationships. Households with older members had larger reduced expenditure on food and social relationships. There are two possible interpretations of this finding, which pose a concern about the long-term deteriorative health effects of CHE. First, owing to the large financial burden of CHE, the level of these household expenditures may be suppressed. Reduction in food expenditure leads to low energy and nutrient intake, which can increase the risk of frailty among older people [48] and eventually raise functional limitations and mortality risks [49, 50]. This is one of the pathways that adverse socioeconomic circumstances lead to an increased risk of frailty [51]. Second, engagement in activities related to these expenditures may be restricted because of health or economic issues [52]. Considering that social relationships positively affect an individual’s health status [53], this may lead to further health deterioration.
Regarding the other financial consequences of CHE (e.g. income), households with only younger members were disproportionally affected. These households saw an income decline in the year following the experience of CHE. This can be interpreted based on the Grossman model [9], assuming that the main income source of younger people is their salaries, while that of older people is their pension benefits. Accordingly, the health status of younger people is inextricably linked to their income through productivity and work hours, so their salaries may decline owing to ill health. Conversely, among older people, their health status does not affect their income when the source is pension benefits. Although we did not discover any significant results regarding savings, from the median value, households with older members had obtained more savings, which potentially suggests that older people have the better ability to pay than younger people.
We also found that the probability of experiencing unmet needs was higher among younger and older people and lowest in middle-aged people; however, we were unable to explore the reason for this. The findings of previous studies are relevant here although differences in institutional settings across countries should be noted. In a Canadian survey that had a younger sample aged 12 years or over (average age of 48 years) than the JHPS/KHPS, wait time was the most common reason for unmet needs [29]. Meanwhile, among older people, economic hardship was the leading reason for unmet healthcare needs, with the additional finding that chronic conditions increased the probability of experiencing unmet needs [54]. These findings suggest that younger and older people may forgo care for different reasons. For younger people who are employed, the opportunity cost of seeking care can be an important reason for unmet healthcare needs. Here, households with employed heads were less likely to experience CHE, which may relate to forgone care owing to the opportunity cost. Furthermore, younger people may develop potentially milder symptoms, so they may not have actual or perceived need to use healthcare services. Conversely, older people may forgo care owing to financial hardship or accessibility issues arising from multiple chronic conditions. The group of 55 to 60-year-olds with the lowest prevalence of unmet need may be in the optimal situation where they experience less opportunity cost from seeking healthcare (as they are retired early or are in more senior/better employment situations which allow sick leave); have sufficient income, savings, or both; and are in relatively good health such that they do not have frequent need for healthcare or experience difficulties in accessing health facilities. While the heterogeneous reasons for unmet needs between younger and older people require further investigation, it is important for appropriate policies to respond to the different health needs of people of different ages. From the demand side, assessing whether one’s healthcare utilisation is appropriate is difficult owing to the nature of healthcare services. Therefore, it is preferable for patients if they can access healthcare whenever they feel they need it. In our analysis, negative self-rated health was associated with a lower probability of experiencing unmet healthcare needs, potentially indicating that people who perceive need are in fact able to have those needs met by the healthcare system in Japan.
Implications
Our findings suggest several policy implications. First, generous financial support is needed for younger households that experience CHE, particularly when they do not have high incomes and savings. By averting unmet healthcare needs through access to adequate cures or treatments, enabling people to return to their jobs is important to further avoid productivity loss because of health issues. Accordingly, various types of government aids are available in Japan. However, compared to employed people who are covered by occupation-based social insurance, those who enrol in community-based health insurance (e.g. self-employed and casual employees) are more vulnerable to income decline owing to health shocks. Therefore, the following approaches are suggested further.
Second, people should be encouraged to accumulate financial assets, including enrolment in private insurance, to prepare for unexpected events (that cause catastrophic expenses and income decline) through financial education and larger financial incentives (e.g. tax deduction or credit for insurance premiums). Particularly for older people, it is necessary to improve their financial capability of decumulating their financial assets, assuming that older people tend to have stable incomes and savings. Older Japanese people decumulate their wealth more slowly than predicted owing to precautionary savings and bequests [55]. With well-designed financial planning, older people may be able to better respond to necessary health expenses.
Third, the sickness allowance coverage and other types of social insurance should be expanded to include self-employed and casual employees because these people are more likely to skip necessary care owing to unavailability of these benefits and to avoid income decline. To reduce the opportunity cost of seeking care, the utilisation of over-the-counter drugs and the enhanced availability of occupational physicians and (paid) sick leave may be also helpful.
Forth, to address unmet need for healthcare among older people, it is necessary to reduce the physical barriers to accessing healthcare services. Some physical or mental functional limitations and health issues make visiting a clinic or hospital difficult for older people. Therefore, public or private sectors should consider providing home-visit or online medical care and transportation services to visit healthcare institutions.
Fifth, with many available financial protection policies, individuals may find it difficult to identify and use a service that best fits their situation. Therefore, to enhance service usability, it is imperative to encourage the diffusion and uptake of available services (e.g. via leaflets), reduce the administrative burden of applications, and provide administrative support to identify and utilise them (e.g. via consultations).
Sixth, based on the fact that the heterogeneity was observed between population subgroups, disaggregated data need to be reported for monitoring and evaluation of progress, giving a special emphasis on the vulnerable populations to improve accountability and ensure that no one is left behind.
Finally yet importantly, consequences of catastrophic health expenditure could have deteriorating impacts on individuals’ health regardless of their demographics. Depending on one’s financial status, financial protection policies in health are needed by strengthening health financing, including pooling resources and purchasing of goods and services which people suffering from financial hardship tend to use.
Limitations
This study has several limitations and remaining questions to be answered by future research. First, the JHPS/KHPS contains limited information on respondents’ health status. Therefore, we were unable to assess the health consequences of CHE and unmet need. Owing to the potential heterogeneities in the consequences of CHE and reasons for unmet need between younger and older people, the health consequences may differ between these groups.
Second, the measure for unmet need should be more precise. The JHPS/KHPS asks how respondents deal with their symptoms. As such, even foregoing care owing to mild symptoms, which may not cause the subjective need for care, can be regarded as unmet need. Therefore, a measure for unmet need should reflect an individual’s need for care including types of care forgone. Moreover, a binary measure of self-assessed unmet need can detect more unmet need among people who frequently attempt to access care [29]. Ideally, the probability of experiencing unmet need (i.e. the number of failures to access healthcare out of the number of attempts to access healthcare) should be used. However, doing so may be unrealistic owing to recall bias, so asking about the frequency of experiencing unmet need may be helpful, even though measurement error is still a concern. By better assessing unmet healthcare need based on a standardised measure, UHC monitoring needs to be strengthened [56].
Third, the CHE measure should be improved. The JHPS/KHPS contains information about monthly expenses. Even though our estimates for CHE incidence were comparable with the official estimates by utilising yearly data, yearly expenses would have been more appropriate because some of the independent variables (e.g. income and unmet healthcare need) were obtained on a yearly basis. Moreover, obtaining information on members who actually have healthcare costs and a breakdown of health expenditure by morbidity type may help to precisely assess the heterogeneity in CHE between younger and older people. Furthermore, a previous study has suggested that the definition of CHE used in the SDG Indicators overestimates its incidence among rich households and underestimates it among poor households [57]. Considering the potential differences in ability to pay between younger and older people, an alternative way to define CHE among older people or populations with large proportions of older people may be needed to reflect that they tend to have a larger amount of savings as well as more stable incomes from pension benefits. Also, a threshold of CHE (i.e. 10% of total consumption or income) may not be one-size-fits-all for populations with different demographic and socioeconomic characteristics and all countries with different health systems and socioeconomic developments. Each country may need to reflect on their contexts to define CHE for a more efficient indicator of financial hardship, which can induce significant behavioural and financial consequences. In this regard, it would be necessary to complement the indicator to identify the consequences of financial hardship associated with healthcare utilisation.
Fourth, we utilised a linear probability model to estimate the probability of experiencing CHE and unmet need for easy interpretation and controlling for high-dimensional city-by-year fixed-effects. However, it should be noted that our estimates may be biased because of model misspecification.
Fifth, as the focus of the survey is largely on the working-age population, the JHPS/KHPS does not contain many older respondents. Moreover, respondents to the survey may be biased towards healthier or richer people. In addition, if older respondents live in a long-term care facility, they are unlikely to be included in the survey. Therefore, selection bias may be a concern, especially among older people.
Finally, given that Japan’s universal health insurance system has various available financial protection policies, our findings may not be applicable in other countries that have different socioeconomic and demographic factors, health systems, and financial protection policies. Nevertheless, the findings of this study could be more important for other countries since the heterogeneity in CHE and unmet need between younger and older people as well as their negative consequences are still expected based on theoretical frameworks and existing evidence. The situation may be worse in countries where coverage of essential health services and financial protection are not better than those of Japan. Financial protection from catastrophic health expenditure has worsened globally, which leads to about two billion people facing financial hardship [3]. This suggests that the urgent need for better financial protection policies in health is common across the globe.
Conclusion
This study explores the incidence/prevalence, determinants, and consequences of CHE and unmet healthcare need and investigates the heterogeneity between younger and older people. By analysing the data from a household survey in Japan, we revealed that households with older members, 65 and over, were more likely to experience CHE with different financial consequences compared to households with only younger members under the age of 65. Households with older members responded to CHE by reducing food and social expenditures more so than households without older members reducing expenditure on education. Households without older members experienced an income decline in the year following the occurrence of CHE, while this was not found among households with older members. Unmet need for healthcare is more common among younger and older individuals than among their middle-aged counterparts, aged 55 to 60, though the health consequences of this unmet need could not be determined. To achieve UHC, different types and levels of health and financial support need to be incorporated into national health systems and social protection policies to meet the unique needs of individuals and households.
Data availability
The authors do not have the right to share the data. However, permission may be given by application through the website of the Panel Data Research Center of Keio University: https://www.pdrc.keio.ac.jp/en/paneldata/datasets/jhpskhps/.
Change history
11 March 2024
A Correction to this paper has been published: https://doi.org/10.1186/s13561-024-00495-6
Abbreviations
- UHC:
-
Universal health coverage
- SDG:
-
Sustainable Development Goals
- CHE:
-
Catastrophic health expenditure
- IHE:
-
Impoverishing health expenditure
- OOP:
-
Out-of-pocket payments
- JHPS/KHPS:
-
Japan Household Panel Survey
References
Wagstaff A, Flores G, Hsu J, Smitz M-F, Chepynoga K, Buisman LR, et al. Progress on catastrophic health spending in 133 countries: a retrospective observational study. The Lancet Global Health. 2018;6(2):e169–e79.
Hogan DR, Stevens GA, Hosseinpoor AR, Boerma T. Monitoring universal health coverage within the Sustainable Development Goals: development and baseline data for an index of essential health services. The Lancet Global Health. 2018;6(2):e152–e68.
Tracking Universal Health Coverage. 2023 global monitoring report. Geneva: World Health Organization and International Bank for Reconstruction and Development / The World Bank; 2023.
World Health Organization, The World Bank. Global monitoring report on financial protection in health 2021. Geneva; 2021.
Eozenou PH, Neelsen S, Smitz MF. Financial protection in health among the elderly - A global stocktake. Health Syst Reform. 2021;7(2):e1911067.
Macinko J, Cristina Drumond Andrade F, Bof de Andrade F, Lima-Costa MF. Universal health coverage: are older adults being left behind? Evidence from aging cohorts in twenty-three countries. Health Aff (Millwood). 2020;39(11):1951–60.
Baird K. High out-of-pocket medical spending among the poor and elderly in nine developed countries. Health Serv Res. 2016;51(4):1467–88. Epub 20160122.
Grossman M. On the Concept of Health Capital and the demand for Health. J Political Econ. 1972;80(2):223–55. Epub 255.
Grossman M. The Human Capital Model. In: Culyer AJ, Newhouse JP, editors. Handbook of Health Economics. Elsevier; 2000. pp. 347–408.
Dastan I, Abbasi A, Arfa C, Hashimi MN, Alawi SMK. Measurement and determinants of financial protection in health in Afghanistan. BMC Health Serv Res. 2021;21(1):650. Epub 20210704.
Verma VR, Kumar P, Dash U. Assessing the household economic burden of non-communicable Diseases in India: evidence from repeated cross-sectional surveys. BMC Public Health. 2021;21(1):881. Epub 20210507.
Azzani M, Roslani AC, Su TT. Determinants of household catastrophic health expenditure: a systematic review. Malaysian J Med Sciences: MJMS. 2019;26(1):15–43. Epub 2019/02/28.
Chantzaras AE, Yfantopoulos JN. Financial protection of households against health shocks in Greece during the economic crisis. Soc Sci Med. 2018;211:338–51. Epub 2018/07/18.
Gu H, Kou Y, Yan Z, Ding Y, Shieh J, Sun J, et al. Income related inequality and influencing factors: a study for the incidence of catastrophic health expenditure in rural China. BMC Public Health. 2017;17(1):727. Epub 20170920.
Aregbeshola BS, Khan SM. Determinants of catastrophic health expenditure in Nigeria. Eur J Health Econ. 2018;19(4):521–32. Epub 20170529.
Li Y, Wu Q, Xu L, Legge D, Hao Y, Gao L, et al. Factors affecting catastrophic health expenditure and impoverishment from medical expenses in China: policy implications of universal health insurance. Bull World Health Organ. 2012;90(9):664–71. Epub 20120613.
Yardim MS, Cilingiroglu N, Yardim N. Catastrophic health expenditure and impoverishment in Turkey. Health Policy. 2010;94(1):26–33.
Somkotra T, Lagrada LP. Which households are at risk of catastrophic health spending: experience in Thailand after universal coverage. Health Aff (Millwood). 2009;28(3):w467–78. Epub 20090331.
Feral-Pierssens AL, Rives-Lange C, Matta J, Rodwin VG, Goldberg M, Juvin P, et al. Forgoing health care under universal health insurance: the case of France. Int J Public Health. 2020;65(5):617–25. Epub 20200530.
Yamada T, Chen CC, Murata C, Hirai H, Ojima T, Kondo K, et al. Access disparity and health inequality of the elderly: unmet needs and delayed healthcare. Int J Environ Res Public Health. 2015;12(2):1745–72. Epub 20150203.
Hwang J. Understanding reasons for unmet health care needs in Korea: what are health policy implications? BMC Health Serv Res. 2018;18(1):557. Epub 20180716.
Jung B, Ha IH. Determining the reasons for unmet healthcare needs in South Korea: a secondary data analysis. Health Qual Life Outcomes. 2021;19(1):99. Epub 20210320.
Allin S, Grignon M, Le Grand J. Subjective unmet need and utilization of health care services in Canada: what are the equity implications? Soc Sci Med. 2010;70(3):465–72. Epub 20091114.
Guessous I, Gaspoz JM, Theler JM, Wolff H. High prevalence of forgoing healthcare for economic reasons in Switzerland: a population-based study in a region with universal health insurance coverage. Prev Med. 2012;55(5):521–7. Epub 20120823.
Nelson CH, Park J. The nature and correlates of unmet health care needs in Ontario, Canada. Soc Sci Med. 2006;62(9):2291–300. Epub 20060123.
Okamoto S, Sakamoto H, Kamimura K, Komamura K, Kobayashi E, Liang J. Economic effects of healthy ageing: functional limitation, forgone wages, and medical and long-term care costs. Health Econ Rev. 2023;13(1):28. Epub 20230510.
Wimo A, Seeher K, Cataldi R, Cyhlarova E, Dielemann JL, Frisell O, et al. The worldwide costs of Dementia in 2019. Alzheimers Dement. 2023;19(7):2865–73. Epub 20230108.
Herr M, Arvieu JJ, Aegerter P, Robine JM, Ankri J. Unmet health care needs of older people: prevalence and predictors in a French cross-sectional survey. Eur J Public Health. 2014;24(5):808–13. Epub 20131127.
Gibson G, Grignon M, Hurley J, Wang L. Here comes the SUN: self-assessed unmet need, worsening health outcomes, and health care inequity. Health Econ. 2019;28(6):727–35. Epub 2019/04/26.
Ju YJ, Kim TH, Han KT, Lee HJ, Kim W, Ah Lee S, et al. Association between unmet healthcare needs and health-related quality of life: a longitudinal study. Eur J Public Health. 2017;27(4):631–7.
Barr N. Economics of the welfare state. Oxford, UK: Oxford University Press; 2020.
Bataineh H, Devlin RA, Barham V. Unmet health care and health care utilization. Health Econ. 2019;28(4):529–42. Epub 20190128.
Browning M, Crossley TF. The life-cycle model of consumption and saving. J Econ Perspect. 2001;15(3):3–22.
Statistics Bureau, Ministry of Internal Affairs and Communications. Family Income and Expenditure Survey (Savings and Liabilities). 2022 [cited 2022 20 May]; Available from: https://www.stat.go.jp/english/data/sav/index.html.
World Health Organization., World Bank. Tracking universal health coverage: 2021 global monitoring report. 2021.
Ministry of Health, Labour and Welfare.,. Health insurance. n.d. [cited 2022 8 June]; Available from: https://www.mhlw.go.jp/english/policy/health-medical/health-insurance/index.html.
Hashimoto H, Ikegami N, Shibuya K, Izumida N, Noguchi H, Yasunaga H, et al. Cost containment and quality of care in Japan: is there a trade-off? The Lancet. 2011;378(9797):1174–82.
Ikegami N, Campbell JC. Japan’s health care system: containing costs and attempting reform. Health Aff (Millwood). 2004;23(3):26–36.
Keio University Panel Data Research Center. Japan Household Panel Survey (JHPS/KHPS). 2021 [cited 2022 4 January]; Available from: https://www.pdrc.keio.ac.jp/en/paneldata/datasets/jhpskhps/.
Xu K, Evans DB, Kawabata K, Zeramdini R, Klavus J, Murray CJL. Household catastrophic health expenditure: a multicountry analysis. The Lancet. 2003;362(9378):111–7.
Xu K, Evans DB, Carrin G, Aguilar-Rivera AM, Musgrove P, Evans T. Protecting households from catastrophic health spending. Health Aff (Millwood). 2007;26(4):972–83. Epub 2007/07/17.
United Nations Statistics Division. E-Handbook on SDG Indicators: Indicator 3.8.2. 2018 [cited 2021 29 November]; Available from: https://unstats.un.org/wiki/display/SDGeHandbook/Indicator+3.8.2.
Wagstaff A, Flores G, Smitz M-F, Hsu J, Chepynoga K, Eozenou P. Progress on impoverishing health spending in 122 countries: a retrospective observational study. The Lancet Global Health. 2018;6(2):e180–e92.
Ministry of Health, Labour and Welfare. Comprehensive survey of living conditions 2019. 2019 [cited 2021 4 November]; Available from: https://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa19/index.html.
Burbidge JB, Magee L, Robb AL. Alternative transformations to handle extreme values of the dependent variable. J Amer Statistical Assoc. 1988;83(401):123–7.
Correia S. A feasible estimator for linear models with multi-way fixed effects. Preprint at http://scorreiacom/research/hdfepdf. 2016.
Gravelle H, Morris S, Sutton M. Economic studies of equity in the consumption of health care. In: Jones AM, editor. The Elgar Companion to Health Economics, Second Edition. Massachusetts: Edward Elgar Publishing; 2012. p. 192–202.
Bartali B, Frongillo EA, Bandinelli S, Lauretani F, Semba RD, Fried LP, et al. Low nutrient intake is an essential component of frailty in older persons. J Gerontol A Biol Sci Med Sci. 2006;61(6):589–93.
Kojima G, Iliffe S, Walters K. Frailty index as a predictor of mortality: a systematic review and meta-analysis. Age Ageing. 2018;47(2):193–200.
Vermeulen J, Neyens JC, van Rossum E, Spreeuwenberg MD, de Witte LP. Predicting ADL disability in community-dwelling elderly people using physical frailty indicators: a systematic review. BMC Geriatr. 2011;11:33. Epub 20110701.
Wang J, Hulme C. Frailty and socioeconomic status: a systematic review. J Public Health Res. 2021;10(3). Epub 20210430.
Jivraj S, Nazroo J, Barnes M. Short- and long-term determinants of social detachment in later life. Aging Soc. 2015;36(5):924–45.
Umberson D, Karas Montez J. Social relationships and health: a flashpoint for health policy. J Health Soc Behav. 2010;51(1suppl):54–S66.
Kim YS, Lee J, Moon Y, Kim KJ, Lee K, Choi J, et al. Unmet healthcare needs of elderly people in Korea. BMC Geriatr. 2018;18(1):98. Epub 20180420.
Niimi Y, Horioka CY. The wealth decumulation behavior of the retired elderly in Japan: the relative importance of precautionary saving and bequest motives. J Japanese Int Economies. 2019;51:52–63.
Rosenberg M, Kowal P, Rahman MM, Okamoto S, Barber SL, Tangcharoensathien V. Better data on unmet healthcare need can strengthen global monitoring of universal health coverage. BMJ. 2023;382:e075476. Epub 20230905.
Cylus J, Thomson S, Evetovits T. Catastrophic health spending in Europe: equity and policy implications of different calculation methods. Bull World Health Organ. 2018;96(9):599–609. Epub 20180604.
Acknowledgements
We are grateful for the helpful comments from Dr Shinichi Tomioka at the World Health Organization Centre for Health Development. Also, we thank the Panel Data Research Center of Keio University for providing the data, the Japan Household Panel Survey, for a secondary analysis in this study.
Funding
This study received funding from the World Health Organization Centre for Health Development (WHO Kobe Centre: K21003), which also provided technical support in reviewing an earlier draft of this manuscript.
Author information
Authors and Affiliations
Contributions
SO played a leading role in all aspects of this study. All other authors (i.e. MS, MR, NN, KKa, KKo, EK, JS, YH, TO, and HI) made contributions through the conceptualisation of the study, and reviewing analysis and the draft, which were prepared by SO. All authors have approved the final version of the manuscript for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was not required as this study comprises a secondary analysis.
Consent for publication
Not Applicable.
Competing interests
None.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original version of this article was revised: the license copyright has been corrected to CC BY 3.0 IGO instead of Creative Commons Attribution 4.0 International License.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under the terms of the Creative Commons Attribution 3.0 IGO License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the World Health Organization, provide a link to the Creative Commons licence and indicate if changes were made. The use of the World Health Organization?s name, and the use of the World Health Organization?s logo, shall be subject to a separate written licence agreement between the World Health Organization and the user and is not authorized as part of this CC-IGO licence. Note that the link provided below includes additional terms and conditions of the licence. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/3.0/igo/.
About this article

Cite this article
Okamoto, S., Sata, M., Rosenberg, M. et al. Universal health coverage in the context of population ageing: catastrophic health expenditure and unmet need for healthcare. Health Econ Rev 14, 8 (2024). https://doi.org/10.1186/s13561-023-00475-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13561-023-00475-2