
Abstract
Aims
Cross-sectional studies have demonstrated the association of skeletal muscle mass with metabolic-associated fatty liver disease (MAFLD), while longitudinal data are scarce. We aimed to explore the impact of changes in relative skeletal muscle mass on the MAFLD treatment response.
Methods
MAFLD patients undergoing magnetic resonance imaging-based proton density fat fraction for liver fat content (LFC) assessments and bioelectrical impedance analysis before and after treatment (orlistat, meal replacement, lifestyle modifications) were enrolled. Appendicular muscle mass (ASM) was adjusted by weight (ASM/W).
Results
Overall, 256 participants were recruited and divided into two groups: with an ASM/W increase (n=166) and without an ASM/W increase (n=90). There was a great reduction in LFC in the group with an ASM/W increase (16.9% versus 8.2%, P < 0.001). However, the change in LFC in the group without an ASM/W increase showed no significant difference (12.5% versus 15.0%, P > 0.05). △ASM/W Follow-up-Baseline [odds ratio (OR)=1.48, 95% confidence interval (CI) 1.05-2.07, P = 0.024] and △total fat mass (OR=1.45, 95% CI 1.12-1.87, P = 0.004) were independent predictors for steatosis improvement (relative reduction of LFC ≥ 30%). The subgroup analysis showed that, despite without weight loss, decrease in HOMA-IR (OR=6.21, 95% CI 1.28-30.13, P=0.023), △total fat mass Baseline -Follow-up (OR=3.48, 95% CI 1.95-6.21, P <0.001 and △ASM/W Follow-up-Baseline (OR=2.13, 95% CI 1.12-4.05, P=0.022) independently predicted steatosis improvement.
Conclusions
ASM/W increase and loss of total fat mass benefit the resolution of liver steatosis, independent of weight loss for MAFLD.
Similar content being viewed by others


Introduction
Metabolic-associated fatty liver disease (MAFLD), a new nomenclature renamed nonalcoholic fatty liver disease (NAFLD) [1], has become a predominant cause of chronic liver disease globally. Paralleling the obesity epidemic, MAFLD affects an estimated 38.77% of the general population worldwide according to a recent meta-analysis [2]. MAFLD encompasses pathologic traits from simple steatosis to steatohepatitis and fibrosis, which continue to progress to cirrhosis or hepatocellular carcinoma, a recent meta-analysis reported that the annual incidence of hepatocellular carcinoma was 1·8 cases per 1000 person-years in patients with MAFLD [3]. Moreover, numerous clinical studies have demonstrated that MAFLD is closely associated with higher risks of extrahepatic diseases, including type 2 diabetes mellitus (T2DM), cardiovascular disease and chronic kidney diseases [4]. However, there is no approved pharmacotherapy internationally for treating MAFLD to date [1].
Skeletal muscle has been recognized as an important endocrine organ responsible for glucose utilization facilitated by insulin, and the loss of skeletal muscle mass may reduce insulin-mediated glucose disposal [5]. Sarcopenia is characterized by the severe loss of skeletal muscle mass accompanied by progressively reduced muscle strength and physical performance [6]. Mounting studies have demonstrated that lower skeletal muscle mass or sarcopenia is correlated with the prevalence of MAFLD [7,8,9,10,11], more severe steatosis [10, 12,13,14,15] and significant fibrosis [12,13,14,15,16,17] confirmed by biopsy or noninvasive examination, such as transient elastography. Nevertheless, longitudinal studies investigating the relationship between low muscle mass and the severity of steatosis as well as fibrosis in MAFLD are limited. Moreover, the effect of skeletal muscle mass on the MAFLD treatment response is not fully understood. Loss of skeletal muscle mass has been reported to cause metabolic impairments and further aggravate MAFLD [18]; however, evidence regarding the association between changes in skeletal muscle mass and the progression or improvement of MAFLD is scarce.
Magnetic resonance imaging-based proton density fat fraction (MRI-PDFF) is a quantitative and accurate method that is used to assess liver fat content (LFC) [19]. MRI-PDFF has been proven to have excellent diagnostic value for LFC and histologic steatosis in MAFLD patients [20] and is more sensitive to longitudinal changes in steatosis than biopsy [21]. Therefore, MRI-PDFF is regarded as a precise technique for assessing the severity of steatosis and can be utilized in clinical studies to evaluate the relative change in LFC [22, 23].
In this study, we aimed to determine (1) the association of relative skeletal muscle mass or its changes measured by bioelectrical impedance analysis (BIA) with the changes in severity of steatosis and fibrosis in MAFLD patients and (2) the influence of changes in skeletal muscle mass on liver function and insulin resistance based on longitudinal research.
Materials and methods
Study participants
This was a prospective single-center observational cohort study conducted in the First Affiliated Hospital, Sun Yat-sen University, from January 2017 to August 2022. The study design was approved by the institutional ethics committee for clinical research of the First Affiliated Hospital, Sun Yat-sen University (Approval number: [2014] 112). All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional research committee and with the Helsinki Declaration of 1975. All patients signed written informed consent forms.
The subjects were consecutively enrolled according to the following inclusion criteria: (a) age ≥ 18 years; (b) diagnosed with MAFLD based on the international expert consensus in 2020 [24]; and (c) underwent at least two examinations with MRI-PDFF and bioelectrical impedance analysis (BIA). All participants were required to complete a face-to-face interview questionnaire regarding demographic information, smoking, alcohol consumption, medical history and drug use. The following exclusion criteria were applied: (a) hepatocellular carcinoma based on imaging evidence; (b) decompensated cirrhosis; (c) hepatitis B (hepatitis B surface antigen positive for over six months) and hepatitis C (positive for hepatitis C antibody) infection; (d) excessive alcohol consumption (> 20 g/week for males or > 10 g/week for females); (e) auto-immune hepatitis; (f) coronary heart disease, heart failure, chronic kidney disease and malignancies; (g) pregnancy and breastfeeding; and (h) use of drugs that induce steatosis such as steroids, amiodarone or tamoxifen.
Clinical and laboratory indices
Anthropometric indices, including weight, height, waist circumference and blood pressure, were measured by two well-trained physicians. Body mass index (BMI) was calculated as weight/height2 (kg/m2). After a 12-hour overnight fast, a venous blood sample was drawn from all patients and subsequently tested by the laboratory. Biochemical parameters, including alanine aminotransferase (ALT), aspartate aminotransferase (AST), γ-glutamyl transpeptidase GGT), alkaline phosphatase (ALP), total lipid profiles, fasting serum glucose (FSG), fasting insulin (FIN) and uric acid (UA), were assayed by the Abbott c8000 Automatic Biochemistry Analyzer (Abbott, Abbott Park, IL, USA). The normal upper limit for ALT was set to 30 U/L for males and 19 U/L for females [25]. Obesity was defined as BMI ≥ 25kg/m2 [26]. Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated using the following equation: HOMA-IR = FSG (mmol/L) *FIN (μU/mL)/22.5 [24]. Insulin resistance was defined as HOMA-IR ≥2.5 [27].
Radiology examination
MRI-PDFF of the upper abdomen was conducted with a 3.0-Tesla MRI scanner (SIEMENS 3.0T MAGNETOM Verio, Siemens, Munchen, Germany) in all participants for LFC quantification at baseline and follow-up visits. The scanning protocol and imaging parameters were in accordance with those of our previous published study [28]: TE1 2.5 ms; TE2 3.7 ms; repetition time 5.47 ms; 5° flip angle; ±504.0 kHz per pixel receiver bandwidth; and slice thickness, 3.0 mm. The LFC was evaluated with an irregularly shaped region of interest covering the entire liver in 21 sequential slices by two trained radiologists who were blinded to the aim of the study.
The liver stiffness measurement (LSM) was performed by two-dimensional shear wave elastography (2D-SWE, Aix-en-Provence, France) at the first clinic visit and follow-up. The physicians who conducted the 2D-SWE had over 5 years of experience with ultrasound measurement.
Body composition measurements and skeletal muscle mass measurements
The BIA was utilized to assess the body composition of all participants with a segmental multifrequency BIA device (TANITA, MC-980MA, Japan) according to the manufacturer’s instructions. The BIA technique showed good correlation with dual-energy X-ray absorptiometry, which was validated for the assessment of body composition [29, 30]. The patients were instructed to stand on the electrodes under the toes and heels, and hold a handle in each hand, after fasted overnight (at least 8 hours). All participants spread apart their limbs to ensure that their arms didn’t touch the trunk and the thighs were not in contact, remaining motionless for 40 seconds during the measurement. The impedance for each segments including four limbs and the trunk were measured and the device calculated skeletal muscle mass by regression equations developed by Yamada et al [31]. The appendicular skeletal muscle mass (ASM) was calculated by the sum of the lean muscle mass of the upper and lower limbs. The skeletal muscle mass index (SMI) was calculated by dividing the ASM by body weight (kg), expressed as a percentage (ASM/body weight × 100%).
Treatment and follow-up
Patients received orlistat intervention, meal replacement or routine treatment at baseline and maintained it until the last follow-up. Subjects who chose the orlistat intervention received orlistat (120 mg, 3 times/day for 24 weeks) without additional treatment. Orlistat administration was confirmed by prescription and recorded during clinic visits, as described in our previous study [23]. Those who chose meal replacement were given a nutrient composition of 40% to 50% of calories from carbohydrates, 20% to 35% from protein, and 25% to 30% from fat, which was provided by Jintong Special Medical Food Co., Ltd. (Guangzhou, China), without additional treatment. Patients who refused orlistat or meal replacement and received lifestyle modifications were instructed to restrict carbohydrate and fat intake in daily life as well as to exercise 3 times a week, 30 minutes each term, according to the World Health Organization Global Strategy on Diet, Physical Activity and Health [32]. Every patient was provided with a portable manual with personalized dietary and exercise suggestions based on sex, age, BMI and medical history. In regard to patients with therapy indications for FSG and lipid profiles, drug treatments were added as guideline recommendations [33, 34]. Patients were instructed to complete two visits over the 6-month enrollment period. Clinical and laboratory parameters were collected and BIA, MRI-PDFF and 2D-SWE were performed at baseline and follow-up. The baseline LFC was compared with that at the follow-up visit. The change in LFC was calculated by subtracting follow-up LFC from LFC at baseline visit (△LFC Baseline-Follow-up). The improvement of steatosis was defined as a relative reduction of liver fat fraction with MRI-PDFF ≥ 30% (△LFC= LFC Baseline-Follow-up/ LFC Baseline ≥ 30%) [35]. The change in SMI was calculated as △ASM/W Follow-up-Baseline.
Statistical analysis
The quantitative variables were expressed as the mean ± standard deviation (SD) when they followed a normal distribution; otherwise, they were presented as the median (interquartile range). The baseline characteristics were compared with the independent Student’s t test or nonparametric test for continuous variables and the chi-square test for categorical variables. Pairwise t tests were applied to compare parameters at baseline and those at follow-up. Univariate and multivariate logistic regression analyses were utilized to determine independent associations between either baseline ASM/W or change in ASM/W and the improvement of steatosis. The factors which were significant in univariate logistic regression analysis were included in the multivariate logistic regression analysis. We also conducted a subgroup analysis defined by the change in weight and baseline BMI (BMI ≥ 25kg/m2, <25 kg/m2). Correlations of changes in ASM/W with changes in LFC and HOMA-IR were performed with Spearman’s correlation analysis. In addition, receiver operating characteristic (ROC) curve analysis was used to test the predictive value of the change in ASM/W for the improvement of ALT, LFC and HOMA-IR. The Youden index was applied to determine the cut-off values that maximized sensitivity and specificity. Two-sided P values < 0.05 were considered as statistically significant. Statistical analyses were performed with IBM SPSS statistical software (version 25.0, Chicago, IL, USA) and GraphPad Prism 8 (Inc, USA).
Results
Baseline characteristics of the study population
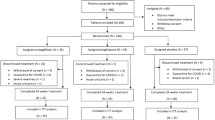
A total of 301 patients were enrolled initially, and they were excluded for reasons such as decompensated cirrhosis (n=3), hepatitis B surface antigen positivity (n=30), and excess alcohol intake (n=12). Therefore, 256 MAFLD patients were ultimately recruited, consisting of 146 (57.0%) subjects who showed improvement at follow-up and 110 (43.0%) subjects who did not. In this study, 16, 10 and 230 patients chose orlistat, meal replacement and lifestyle modifications. The subgroup analysis based on the treatment suggested that the patients in lifestyle treatment gained the significant ASM/W (%) increase (32.2±4.1 vs 33.4±4.3, P<0.001) and the improvement of liver steatosis [14.9 (9.0, 22.7) vs 9.0 (5.9, 15.0), P<0.001; Supplementary table 1]. All 256 participants were divided into two groups based on the change in ASM/W, with an increase in ASM/W (△ASM/W Follow-up-Baseline >0) and without an increase in ASM/W (△ASM/W Follow-up-Baseline ≤0). Figure 1 shows the change in ASM/W from baseline in all patients and in the subgroups without and with weight loss. The maximum and minimum △ASM/W Follow-up-Baseline were 7.70%, 3.57%, 7.70%, and -5.36%, -5.36% and -1.50%, respectively. The baseline characteristics of the subjects are presented in Table 1. There were no significant differences in demographics, anthropometry, metabolic profiles, liver stiffness, body composition, intervention or drug use between the two groups. Interestingly, patients with an increase in ASM/W had worse liver function than patients without an increase in ASM/W, such as higher ALT, AST and GGT (all P < 0.05), and more severe hepatic steatosis with higher LFC (P < 0.001) at baseline.

Waterfall plot of change in ASM/W from baseline in all (A) patients and the subgroups without and with weight loss (B, C). △ASM/W =ASM/W Follow-up-Baseline
Changes in anthropometric, biochemical, and hepatic status with or without ASM/W increase
By design, at follow-up, a significant decrease in weight and waist circumference was observed in the group with an increase in ASM/W (both P < 0.001), while a significant increase in weight (P < 0.001) and no significant changes in waist circumference (P > 0.05) were observed in the group without an increase in ASM/W (Fig. 2A and B). In the group with ASM/W elevation, insulin resistance and liver function improved at follow-up compared with those at baseline with a decrease in HOMA-IR and ALT (both P < 0.001) although the liver function at baseline was worse in this group; however, no similar improvements were found in the group without ASM/W elevation (Fig. 2C and D). In spite of a worse steatosis at baseline, the LFC and liver stiffness at follow-up were reduced significantly compared with those at baseline only in the group with an increase in ASM/W (both P < 0.001); however, there were no significant differences in the group without an increase in ASM/W, despite a lower LFC at baseline (Fig. 2E, F).

Changes in weight (A), waist circumference (B), homeostatic model assessment of insulin resistance (C), alanine aminotransferase (D), liver fat content (E), and liver stiffness (F) in groups with or without ASM/W increase. ASM, appendicular skeletal mass; ASM/W, ASM/weight; HOMA-IR, homeostatic model assessment of insulin resistance. The ASM/W increase was determined as △ASM/W>0. △ASM/W =ASM/W Follow-up-Baseline. The numbers on the top of the boxes represent medians. *P<0.05; **P<0.01; ***P<0.001; ns, not significant
Subgroup analysis divided by weight, ASM and ASM/W change
To determine the effect of change in weight, ASM/W and ASM on the improvement of steatosis, all patients were performed subgroup analysis according to with weight loss (WL), an increase in ASM/W (ASM/WI) and ASM (ASMI) or not. With WL (WL+) was defined as △Weight Baseline-Follow-up >0 and without WL (WL-, -:referred to without) as △Weight Baseline-Follow-up ≤0. With ASM/WI (ASM/WI+, +:referred to with) and without ASM/WI (ASM/WI-) were defined as △ASM/W Follow-up-Baseline >0 and ≤0. With ASMI (ASMI+) and without ASMI (ASMI-) were defined as △ASM Follow-up-Baseline >0 and ≤0. There were three classifications, each consisting of 4 subgroups: ① without WL and without ASM/WI (WL-ASM/WI-), without WL and with ASM/WI (WL-ASM/WI+), with WL and without ASM/WI (WL+ ASM/WI-); with WL and ASM/WI (WL+ ASM/WI+); ② without ASMI and ASM/WI (ASMI-ASM/WI-), without ASMI and with ASM/WI (ASMI-ASM/WI+), with ASMI and without ASM/WI (ASMI+ ASM/WI-); with ASMI and ASM/WI (ASMI+ ASM/WI+); ③ without WL and without ASMI (WL-ASMI-), without WL and with ASMI (WL-ASMI+), with WL and without ASMI (WL+ ASMI-); with WL and ASMI (WL+ ASMI+). The comparison of baseline and follow-up characteristics in four groups were shown in Supplementary table 2, 3 and 4.
A significant reduction in HOMA-IR (2.6 verse 2.2, P<0.001), ALT (53U/L verse 29U/L, P<0.001), LFC (16.5% verse 7.9%, P<0.001) and liver stiffness (5.9 kPa verse 5.8kPa, P<0.001) at follow-up compared with those at baseline in the WL+ ASM/WI+ group (Fig. 3A, B, C, D). Nevertheless, only LFC decreased significantly in the WL-ASM/WI+ group (17.3% verse 8.8%, P=0.001; Fig. 3C). There is also a significant improvement in HOMA-IR (2.5 verse 1.9, 2.7 verse 2.3, both P<0.001), ALT (54U/L verse 30U/L, 51U/L verse 30U/L, both P<0.001) and LFC (15.3% verse 7.4%, 17.4% verse 8.3%, both P<0.001) at follow-up compared with those at baseline in the ASMI- ASM/WI+ and ASMI+ ASM/WI+ groups (Supplementary figure 1A, B, C). Similarly, significant improvement in HOMA-IR (2.7 verse 2.1, 2.7 verse 2.3, both P<0.001), ALT (49U/L verse 31U/L, 53U/L verse 30U/L, both P<0.001), LFC (16.5% verse 7.9%, P<0.001) were observed in WL+ASMI- and WL+ASMI+ groups (Supplementary figure 2A, B, C). In WL-ASMI+ group, LFC reduced significantly (13.3% verse 8.8%, P<0.001) even though without improvement in HOMA-IR, ALT and liver stiffness (Supplementary figure 2A, B, C, D).

Changes in HOMA-IR (A), ALT (B), LFC (C), liver stiffness (D) in the groups classified by changes in weight and ASM/W. ASM, appendicular skeletal mass; ASM/W, ASM/weight; HOMA-IR, homeostatic model assessment of insulin resistance. Weight loss was defined as △weight>0. △weight=weight Baseline-Follow-up. The ASM/W increase was determined to be △ASM/W>0. △ASM/W =ASM/W Follow-up-Baseline. WL-, without weight loss; WL+, with weight loss; ASM/WI-, without ASM/W increase; ASM/WI +, with ASM/W increase. *P<0.05; **P<0.01; ***P<0.001; ns, not significant
Predictors of steatosis improvement
We analyzed the factors in the binary logistic regression model of liver steatosis improvement (relative reduction of LFC ≥ 30%). For all patients, decrease in weight, decrease in HOMA-IR, △ASM/W Follow-up-Baseline and △Total fat mass Baseline -Follow-up were identified as predictors of hepatic steatosis improvement in univariate analysis (supplementary table 5). After multivariate analysis, △ASM/W Follow-up-Baseline [odds ratio (OR)=1.48, 95% confidence interval (CI) 1.05-2.07, P = 0.024] and △Total fat mass Baseline -Follow-up (OR=1.45, 95% CI 1.12-1.87, P = 0.004) were found to be predictors of the improvement in liver steatosis (Fig. 4A). However, ASM/W and total fat mass at baseline and the different treatments were not significantly associated with liver steatosis remission.

The predictors of improvement of liver fat content in univariate and multivariate logistic regression analysis in all subjects (A), patients without and with weight loss (B, C), patients with a BMI <25kg/m2 and BMI ≥25kg/m2 (D, E). The improvement of liver steatosis was defined as the liver fat content (LFC) ≥30% relative decline compared with baseline in MRI-PDFF (LFC Baseline-Follow-up/ LFC Baseline≥30%). ASM, appendicular skeletal mass; ASM/W, ASM/weight; HOMA-IR, homeostatic model assessment of insulin resistance. Decrease in Weight was defined as △Weight Baseline-Follow-up >0; Decrease in HOMA-IR was defined as △HOMA-IR Baseline-Follow-up >0
Logistic analysis was conducted in the subgroups divided by weight loss, which was designed to explore the impact of weight loss on the hepatitis steatosis and ASM/W, the univariate analysis was shown in Supplementary table 5. In patients with weight loss, 113 (72.4%) achieved hepatic steatosis remission at follow-up, multivariate logistic regression analysis showed that △total fat mass Baseline -Follow-up (OR=3.03, 95% CI 2.03-4.53, P<0.001) for predicting improvement of fat infiltration of liver (Fig. 4C). However, in patients without weight loss, 33 (33.0%) patients in this group showed improvement of hepatic steatosis, in addition to decrease in HOMA-IR (OR=6.21, 95% CI 1.28-30.13, P=0.023) and △total fat mass Baseline -Follow-up (OR=3.48, 95% CI 1.95-6.21, P <0.001), △ASM/W Follow-up-Baseline (OR=2.13, 95% CI 1.12-4.05, P=0.022) was observed as the independent predictor of steatosis improvement (Fig. 4B).
Subgroup analysis determined by obesity (BMI ≥ 25 kg/m2 and BMI < 25 kg/m2) was also performed to explore the factors associated with steatosis improvement. The baseline characteristics of the two subgroups are shown in Supplementary table 6 and the univariate analysis was shown in supplementary table 7. At follow-up, 50 (55.6 %) and 96 (57.8 %) subjects showed improvement in the group without and with obesity. In patients without obesity, multivariate logistic regression analysis after adjustment cofounders showed that △ASM/W Follow-up-Baseline (OR=2.65, 95% CI 1.42-4.92, P=0.020) was an independent predictor of steatosis improvement (Fig. 4D). Among patients with obesity, decrease in HOMA-IR (OR=9.27, 95% CI 2.17-39.56, P=0.003) and △body fat mass Baseline -Follow-up (OR=2.11, 95% CI 1.24-3.59, P = 0.006) remained significant predictors for the remission of steatosis (Fig. 4E). Subgroup analysis defined by BMI ≥ 30 kg/m2 and BMI < 30 kg/m2) was also conducted. Multivariate logistic regression analysis showed that △ASM/W Follow-up-Baseline (OR=3.06, 95% CI 2.14-5.64, P<0.001) independently predicted steatosis improvement in subjects with BMI < 30 kg/m2, while could not predict in patients BMI ≥ 30 kg/m2 (Supplementary table 8).
Correlation between the change in ASM/W and the change in LFC and HOMA-IR
The associations of △ASM/W Follow-up-Baseline with △LFC Baseline-Follow-up and △HOMA-IR Baseline-Follow-up were analyzed using Spearman’s correlation analysis. The △ASM/W Follow-up-Baseline was positively related to △LFC Baseline-Follow-up (r=0.576, P<0.001) and △HOMA-IR Baseline-Follow-up (r=0.330, P<0.001, Fig. 5A, B).

Correlation of △ASM/W with △LFC (A) and △HOMA-IR (B) in all patients. HOMA-IR, homeostatic model assessment of insulin resistance; ALT, alanine aminotransferase, LFC, liver fat content; ASM, appendicular skeletal mass; ASM/W, ASM/weight. Receiver operating characteristic curve of △ASM/W for predicting normalization of HOMA-IR in subjects with insulin resistance at baseline (n=116, C), normalization of ALT in subjects with elevation of ALT at baseline (n=194, D), △LFC reduction ≥30% in the entire cohort (n=256, E). △ASM/W=ASM/W Follow-up-Baseline; △HOMA-IR=HOMA-IR Baseline-Follow-up; △LFC= LFC Baseline-Follow-up. Insulin resistance was defined as a homeostasis model assessment of insulin resistance ≥2.5, and normalization of HOMA-IR was defined as a homeostasis model assessment of insulin resistance<2.5 at follow-up in this cohort. Elevation of ALT was defined as alanine aminotransferase ≥30 U/L in males and ≥19 U/L in females, and the normalization of ALT was determined when alanine aminotransferase <30 U/L in males and <19 U/L in females at follow-up in this cohort. LFC relative reduction was calculated as relative △LFC Baseline-Follow-up/ LFC Baseline
Predictive values of △ASM/W Follow-up-Baseline for MAFLD treatment outcomes
We constructed an ROC curve to evaluate the predictive power of △ASM/W Follow-up-Baseline for normalization of HOMA-IR in subjects with insulin resistance at baseline (n=116), normalization of ALT in patients with elevated ALT at baseline (n=194) and △LFC reduction ≥30% in the entire cohort (n=256). The areas under the curves (AUCs) for normalization of HOMA-IR (Fig. 5C), normalization of ALT (Fig. 5D) and steatosis improvement (Fig. 5E) were 0.749 (95% CI 0.631-0.866, P<0.001), 0.699 (95% CI 0.623-0.786, P<0.001) and 0.832 (95% CI 0.779-0.885, P<0.001), respectively. The cut-off values of △ASM/W Follow-up-Baseline were 0.76%, 0.70% and 0.11%, with sensitivities of 75.8%, 82.6 and 86.9% and specificities of 39.3%, 33.3% and 30.5%, respectively.
Discussion
In this prospective longitudinal study, we first explored the relationship between the change in ASM/W and the improvement of MAFLD evaluated by MRI-PDFF in Asian adults with MAFLD. We observed that the increase in ASM/W and decrease in total fat mass were independently associated with the remission of hepatic steatosis, accompanied by significant improvements in insulin sensitivity and liver function in the group with an increase in ASM/W. These associations persisted after further adjustment for change in weight.
Several previous studies have reported that a lower SMI was associated with more severe liver steatosis evaluated by ultrasonography or liver histology [10, 12, 13, 36] but were limited to cross-sectional settings. Data focused on the relationship of the baseline SMI and change in SMI with MAFLD are scarce. A 10-year retrospective cohort study involving 4398 initially MAFLD-free subjects suggested that a progressive increase in fat mass and a loss of ASM/W were associated with incident MAFLD diagnosed by ultrasonography [37]. A 7-year longitudinal study including 12624 subjects reported that the baseline SMI and an increase in SMI were positively associated with the improvement of MAFLD determined by the hepatic steatosis index (HSI) if present at baseline [27]. In line with this, an association between an increase in ASM/W and the resolution of hepatic steatosis determined by a relative reduction in LFC obtained by MRI-PDFF was observed in this study. In addition, the logistic regression analysis suggested that this association was independent of weight change. ROC analysis showed that the cut-off value of △ASM/W Follow-up-Baseline for predicting steatosis improvement was 0.14%. Moreover, we also found that a decrease in total fat mass was independently and positively related to the resolution of steatosis.
The underlying mechanism linking skeletal muscle mass and MAFLD has yet to be explored and may include insulin resistance, changes in myokines, chronic inflammation and physical inactivity [38]. It is acknowledged that skeletal muscle is the primary organ responsible for whole-body insulin-mediated glucose utilization, and a reduction in glucose disposal caused by the loss of skeletal muscle mass may further result in insulin resistance [39]. Insulin resistance causes lipolysis of adipose tissue and increases the uptake of free fatty acids, contributing to the accumulation of triglycerides in the liver [40]. On the other hand, insulin resistance leads to skeletal muscle reduction by inhibiting protein synthesis in skeletal muscle through the mammalian target of rapamycin complex 1 (mTORC1) or ribosomal protein S6 kinase beta-1 (S6 K1) pathway and exacerbating proteolytic gluconeogenesis [41,42,43]. The increase in SMI was significantly associated with the improvement in insulin resistance, which was revealed by a 7-year longitudinal study [27]. Similarly, we also found that an increase in ASM/W was positively correlated with a decrease in HOMA-IR in the correlation analysis and could predict the normalization of HOMA-IR in the ROC analysis. Therefore, elevation of ASM/W may promote the improvement of steatosis by alleviating insulin resistance. However, decreased HOMA-IR was not an independent predictor for the remission of steatosis, suggesting that insulin resistance partly participated in the association of changes in ASM/W and the development or resolution of MAFLD. Myokines such as interleukin-6 and irisin, chronic low-grade inflammation and oxidative stress may also be involved [43].
It has been reported that weight loss is significantly associated with remission of MAFLD [44, 45]. In the present study, the relationships between the increase in ASM/W as well as the decrease in total fat mass and liver steatosis resolution determined by MRI-PDFF were first reported. The logistic regression analysis suggested that an increase in ASM/W is an independent predictor for steatosis improvement. The predicting value of loss of weight for remission of steatosis disappeared in multivariate regression analysis, which may be caused by adjustment of the change in total fat mass. And the main reason for weight loss is decrease in fat mass. In this study, the subgroup analysis based on the changes in weight and ASM/W also provided evidence that an increase in ASM/W is related to a reduction in LFC, regardless of weight loss. In the logistic regression analysis based on whether weight loss, the change of ASM/W was still the independent predictor of improvement of liver steatosis, which demonstrated the positive impact of increase of ASM/W on remission of fatty liver.
To investigate the effect of an increase in ASM/W on hepatic steatosis change in patients with or without obesity, logistic analysis was performed in the subgroups defined by BMI. Decrease in HOMA-IR and a decline in total fat mass independently predict the resolution of liver steatosis in subjects with obesity, suggesting that weight loss may be the primary intervention for these patients. Meanwhile, increasing skeletal muscle mass to improve insulin resistance is also essential. Comparatively, an increase in ASM/W was an independent predictor in participants without obesity, indicating that increasing skeletal muscle mass is the main therapeutic strategy for MAFLD patients without obesity, rather than weight loss. This suggests that increasing skeletal muscle mass can be a promising therapy for MAFLD [46, 47], especially for MAFLD without obesity (BMI<25kg/m2). For MAFLD with obesity (BMI≥25kg/m2), weight (fat) loss as well as decreasing HOMA-IR are important interventions to improve liver steatosis.
The association between SMI and liver fibrosis has been confirmed in several published studies [12,13,14, 16, 17] which concluded that low skeletal muscle mass was associated with more severe fibrosis, but all of these findings were cross-sectional. In the current study, we explored the relationship between changes in ASM/W and changes in liver stiffness. Liver stiffness showed a significant decrease at follow-up compared with that at baseline in the group with an ASM/W increase. This result was in accordance with the conclusions reported by previous studies. However, the conclusion needs to be further validated because a small percentage (6, 2.3%) of patients were defined as having liver fibrosis with a baseline LSM > 7.1 kPa, and most of the rest were determined to have no fibrosis with an LSM ≤7.1 kPa in this study. Therefore, further long-term longitudinal research with a large number of subjects with high LSM is needed.
There are some limitations in this study. First, the main limitation of the study is the lack of the assessment of skeletal muscle mass, which can be evaluated by MRI-PDFF, however, it was not available in this study. It will be the purpose in our future studies associated with MAFLD and skeletal muscle. Second, the sample size was small; therefore, the subgroup analysis with a small number of subjects may weaken the reliability of the conclusion. Besides, due the limitations of small sample size regarding orlistat (n=16) and meal replacement treatments (n=10), subgroup analysis of the associations among different interventions and skeletal muscle mass did not provide sufficient statistical power to demonstrate and further prospective studies with larger sample sizes are needed to identify. Thirdly, this study was implemented in a single center, and more multicenter studies are warranted to provide more powerful evidence. Third, despite the fact that hepatic steatosis remission was evaluated by MRI-PDFF instead of histology, the gold standard, MRI-PDFF was an accurate and invasive technique for assessing the severity of steatosis and could be an alternative method in large-scale population studies.
Conclusions
In summary, our study suggested that an increase in relative skeletal muscle mass and decrease in total fat mass over time may have a significant beneficial effect on improving the resolution of liver steatosis, independent of weight loss. Increasing skeletal muscle mass might be a strategy for the additive efficacy of MAFLD, especially for patients without obesity. Loss of total fat mass and improvement of insulin resistance are effective strategies for MAFLD with obesity. However, more multicenter longitudinal studies based on large populations are needed to confirm our findings.
Availability of data and materials
Some or all datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Abbreviations
- MAFLD:
-
Metabolic associated fatty liver disease
- LFC:
-
Liver fat content
- ASM:
-
Appendicular skeletal mass
- ASM/W:
-
ASM/weight
- BMI:
-
Body mass index
- MRI-PDFF:
-
Magnetic resonance imaging-based proton density fat fraction
- BIA:
-
Bioelectrical impedance analysis
- WC:
-
Waist circumference
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- GGT:
-
γ-glutamyl transpeptidase
- ALP:
-
Alkaline phosphatase
- FSG:
-
Fasting serum glucose
- FIN:
-
Fasting insulin
- UA:
-
Uric acid
- LSM:
-
Liver stiffness measurement
- SMI:
-
Skeletal muscle mass index
- ROC:
-
Receiver operating characteristic
- AUC:
-
Areas under the curves
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- HOMA-IR:
-
Homeostatic model assessment of insulin resistance
- WL:
-
Weight loss
- ASM/WI:
-
an increase in ASM/W
- ASMI:
-
an increase in ASM
References
Eslam M, Newsome PN, Sarin SK, Anstee QM, Targher G, Romero-Gomez M, et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J Hepatol. 2020;73(1):202–9.
Chan KE, Koh TJL, Tang ASP, Quek J, Yong JN, Tay P, et al. Global Prevalence and Clinical Characteristics of Metabolic-associated Fatty Liver Disease: A Meta-Analysis and Systematic Review of 10 739 607 Individuals. J Clin Endocrinol Metab. 2022;107(9):2691–700.
Li J, Zou BY, Yeo YH, Feng YM, Xie XY, Lee DH, et al. Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999-2019: a systematic review and meta-analysis. Lancet Gastroenterol. 2019;4(5):389–98.
Adams LA, Anstee QM, Tilg H, Targher G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut. 2017;66(6):1138–53.
Severinsen MCK, Pedersen BK. Muscle-Organ Crosstalk: The Emerging Roles of Myokines (vol 41, pg 594, 2020). Endocr Rev. 2021;42(1):97–9.
Chen LK, Woo J, Assantachai P, Auyeung TW, Chou MY, Iijima K, et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J Am Med Dir Assoc. 2020;21(3):300.
Hong HC, Hwang SY, Choi HY, Yoo HJ, Seo JA, Kim SG, et al. Relationship Between Sarcopenia and Nonalcoholic Fatty Liver Disease: The Korean Sarcopenic Obesity Study. Hepatology. 2014;59(5):1772–8.
Wang YM, Zhu KF, Zhou WJ, Zhang Q, Deng DF, Yang YC, et al. Sarcopenia is associated with the presence of nonalcoholic fatty liver disease in Zhejiang Province, China: a cross-sectional observational study. Bmc Geriatr. 2021;21(1):55.
Gan D, Wang L, Jia MH, Ru Y, Ma YY, Zheng WF, et al. Low muscle mass and low muscle strength associate with nonalcoholic fatty liver disease. Clin Nutr. 2020;39(4):1124–30.
Chung GE, Kim MJ, Yim JY, Kim JS, Yoon JW. Sarcopenia Is Significantly Associated with Presence and Severity of Nonalcoholic Fatty Liver Disease. J Obes Metab Syndr. 2019;28(2):129–38.
Lee YH, Jung KS, Kim SU, Yoon HJ, Yun YJ, Lee BW, et al. Sarcopaenia is associated with NAFLD independently of obesity and insulin resistance: Nationwide surveys (KNHANES 2008-2011). J Hepatol. 2015;63(2):486–93.
Petta S, Ciminnisi S, Di Marco V, Cabibi D, Camma C, Licata A, et al. Sarcopenia is associated with severe liver fibrosis in patients with non-alcoholic fatty liver disease. Aliment Pharm Ther. 2017;45(4):510–8.
Koo BK, Kim D, Joo SK, Kim JH, Chang MS, Kim BG, et al. Sarcopenia is an independent risk factor for non-alcoholic steatohepatitis and significant fibrosis. J Hepatol. 2017;66(1):123–31.
Guo W, Zhao X, Miao MY, Liang XR, Li XN, Qin P, et al. Association Between Skeletal Muscle Mass and Severity of Steatosis and Fibrosis in Non-alcoholic Fatty Liver Disease. Front Nutr. 2022;9:883015.
Hsieh YC, Joo SK, Koo BK, Lin HC, Kim W. Muscle alterations are independently associated with significant fibrosis in patients with nonalcoholic fatty liver disease. Liver Int. 2021;41(3):494–504.
Lee YH, Kim SU, Song K, Park JY, Kim DY, Ahn SH, et al. Sarcopenia Is Associated With Significant Liver Fibrosis Independently of Obesity and Insulin Resistance in Nonalcoholic Fatty Liver Disease: Nationwide Surveys (KNHANES 2008-2011). Hepatology. 2016;63(3):776–86.
Kim KH, Kim BK, Park JY, Kim DY, Ahn SH, Han KH, et al. Sarcopenia assessed using bioimpedance analysis is associated independently with significant liver fibrosis in patients with chronic liver diseases. Eur J Gastroen Hepat. 2020;32(1):58–65.
Poggiogalle E, Donini LM, Lenzi A, Chiesa C, Pacifico L. Non-alcoholic fatty liver disease connections with fat-free tissues: A focus on bone and skeletal muscle. World J Gastroenterol. 2017;23(10):1747–57.
Raptis DA, Fischer MA, Graf R, Nanz D, Weber A, Moritz W, et al. MRI: the new reference standard in quantifying hepatic steatosis? Gut. 2012;61(1):117–27.
Gu JL, Liu SS, Du SX, Zhang Q, Xiao JH, Dong QJ, et al. Diagnostic value of MRI-PDFF for hepatic steatosis in patients with non-alcoholic fatty liver disease: a meta-analysis. Eur Radiol. 2019;29(7):3564–73.
Noureddin M, Lam J, Peterson MR, Middleton M, Hamilton G, Le TA, et al. Utility of Magnetic Resonance Imaging Versus Histology for Quantifying Changes in Liver Fat in Nonalcoholic Fatty Liver Disease Trials. Hepatology. 2013;58(6):1930–40.
Dulai PS, Sirlin CB, Loomba R. MRI and MRE for non-invasive quantitative assessment of hepatic steatosis and fibrosis in NAFLD and NASH: Clinical trials to clinical practice. J Hepatol. 2016;65(5):1006–16.
Ye J, Wu Y, Li F, Wu T, Shao C, Lin Y, et al. Effect of orlistat on liver fat content in patients with nonalcoholic fatty liver disease with obesity: assessment using magnetic resonance imaging-derived proton density fat fraction. Therap Adv Gastroenterol. 2019;12:1756284819879047.
Eslam M, Sarin SK, Wong VW, Fan JG, Kawaguchi T, Ahn SH, et al. The Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Hepatol Int. 2020;14(6):889–919.
Prati D, Taioli E, Zanella A, Della Torre E, Butelli S, Del Vecchio E, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med. 2002;137(1):1–10.
Fan JG, Kim SU, Wong VW. New trends on obesity and NAFLD in Asia. J Hepatol. 2017;67(4):862–73.
Kim G, Lee SE, Lee YB, Jun JE, Ahn J, Bae JC, et al. Relationship Between Relative Skeletal Muscle Mass and Nonalcoholic Fatty Liver Disease: A 7-Year Longitudinal Study. Hepatology. 2018;68(5):1755–68.
Dong Z, Luo Y, Zhang ZW, Cai HS, Li YB, Chan T, et al. MR Quantification of Total Liver Fat in Patients with Impaired Glucose Tolerance and Healthy Subjects. Plos One. 2014;9(10):e111283.
Kim M, Shinkai S, Murayama H, Mori S. Comparison of segmental multifrequency bioelectrical impedance analysis with dual-energy X-ray absorptiometry for the assessment of body composition in a community-dwelling older population. Geriatr Gerontol Int. 2015;15(8):1013–22.
Peniche DBR, Giorguli GR, Aleman-Mateo H. Accuracy of a predictive bioelectrical impedance analysis equation for estimating appendicular skeletal muscle mass in a non-Caucasian sample of older people. Arch Gerontol Geriat. 2015;61(1):39–43.
Yamada Y, Nishizawa M, Uchiyama T, Kasahara Y, Shindo M, Miyachi M, et al. Developing and Validating an Age-Independent Equation Using Multi-Frequency Bioelectrical Impedance Analysis for Estimation of Appendicular Skeletal Muscle Mass and Establishing a Cutoff for Sarcopenia. Int J Env Res Pub He. 2017;14(7):809.
Waxman A, World Health A. WHO global strategy on diet, physical activity and health. Food Nutr Bull. 2004;25(3):292–302.
Jia W, Weng J, Zhu D, Ji L, Lu J, Zhou Z, et al. Standards of medical care for type 2 diabetes in China 2019. Diabetes Metab Res Rev. 2019;35(6):e3158.
Yu KH, Chen DY, Chen JH, Chen SY, Chen SM, Cheng TT, et al. Management of gout and hyperuricemia: Multidisciplinary consensus in Taiwan. Int J Rheum Dis. 2018;21(4):772–87.
Tamaki N, Munaganuru N, Jung J, Yonan AQ, Loomba RR, Bettencourt R, et al. Clinical utility of 30% relative decline in MRI-PDFF in predicting fibrosis regression in non-alcoholic fatty liver disease. Gut. 2022;71(5):983–90.
Pan XY, Liu WY, Zhu PW, Li G, Tang LJ, Gao F, et al. Low skeletal muscle mass is associated with more severe histological features of non-alcoholic fatty liver disease in male. Hepatol Int. 2022;16(5):1085–93.
Lee MJ, Kim EH, Bae SJ, Kim GA, Park SW, Choe J, et al. Age-Related Decrease in Skeletal Muscle Mass Is an Independent Risk Factor for Incident Nonalcoholic Fatty Liver Disease: A 10-Year Retrospective Cohort Study. Gut. Liver. 2019;13(1):67.
Bhanji RA, Narayanan P, Allen AM, Malhi H, Watt KD. Sarcopenia in Hiding: The Risk and Consequence of Underestimating Muscle Dysfunction in Nonalcoholic Steatohepatitis. Hepatology. 2017;66(6):2055–65.
Kalyani RR, Corriere M, Ferrucci L. Age-related and disease-related muscle loss: the effect of diabetes, obesity, and other diseases. Lancet Diabetes Endo. 2014;2(10):819–29.
Utzschneider KM, Kahn SE. Review: The role of insulin resistance in nonalcoholic fatty liver disease. J Clin Endocr Metab. 2006;91(12):4753–61.
Fujita S, Rasmussen BB, Cadenas JG, Drummond MJ, Glynn EL, Sattler FR, et al. Aerobic exercise overcomes the age-related insulin resistance of muscle protein metabolism by improving endothelial function and Akt/mammalian target of rapamycin signaling. Diabetes. 2007;56(6):1615–22.
Guillet C, Prod'homme M, Balage M, Gachon P, Giraudet C, Morin L, et al. Impaired anabolic response of muscle protein synthesis is associated with S6K1 dysregulation in elderly humans. Faseb J. 2004;18(11):1586.
Azevedo VZ, Silaghi CA, Maurel T, Silaghi H, Ratziu V, Pais R. Impact of Sarcopenia on the Severity of the Liver Damage in Patients With Non-alcoholic Fatty Liver Disease. Front Nutr. 2022;8:774030.
Zelber-Sagi S, Lotan R, Shlomai A, Webb M, Harrari G, Buch A, et al. Predictors for incidence and remission of NAFLD in the general population during a seven-year prospective follow-up. J Hepatol. 2012;56(5):1145–51.
Sinn DH, Kang D, Cho SJ, Paik SW, Guallar E, Cho J, et al. Weight change and resolution of fatty liver in normal weight individuals with nonalcoholic fatty liver disease. Eur J Gastroen Hepat. 2021;33:E529–E34.
Hallsworth K, Fattakhova G, Hollingsworth KG, Thoma C, Moore S, Taylor R, et al. Resistance exercise reduces liver fat and its mediators in non-alcoholic fatty liver disease independent of weight loss. Gut. 2011;60(9):1278–83.
Bacchi E, Negri C, Targher G, Faccioli N, Lanza M, Zoppini G, et al. Both Resistance Training and Aerobic Training Reduce Hepatic Fat Content in Type 2 Diabetic Subjects With Nonalcoholic Fatty Liver Disease (the RAED2 Randomized Trial). Hepatology. 2013;58(4):1287–95.
Acknowledgements
We are grateful to Professor Aihua Lin from Department of Medical Statistics, School of Public Health, Sun Yat-sen University provide assistance in statistical analysis to this study.
Funding
This study is supported by National Natural Science Foundation of China (81870404, 82100648), Guangdong Basic and Applied Basic Research Foundation (2022A151501225369) and China postdoctoral science foundation (2020M683128).
Author information
Authors and Affiliations
Contributions
Bihui Zhong and Shuyu Zhuo: Conceptualization, Methodology. Ting Zhou and Junzhao Ye: Investigation, Data Curation, Formal analysis, Writing original Draft. Ling Luo: Data Curation. Wei Wang: Software, Visualization. Shiting Feng: Validation, Supervision. Zhi Dong: Writing - Review and Editing. All authors were involved in writing the paper and had final approval of the submitted and published versions.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All procedures followed were in accordance with the Declaration of Helsinki principles and was approved by the institutional ethics committee for clinical research of the First Affiliated Hospital, Sun Yat-sen University (Approval number: [2014] 112). Informed consent was obtained from all patients for being included in the study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Supplementary figure 1.
Changes in HOMA-IR (A), ALT (B), LFC (C), liver stiffness (D) in the groups classified by changes in ASM and ASM/W. ASM, appendicular skeletal mass; ASM/W, ASM/weight; HOMA-IR, homeostatic model assessment of insulin resistance. Supplementary figure 2. Changes in HOMA-IR (A), ALT (B), LFC (C), liver stiffness (D) in the groups classified by changes in weight and ASM. ASM, appendicular skeletal mass; ASM/W, ASM/weight; HOMA-IR, homeostatic model assessment of insulin resistance. Supplementary table 1. Comparison of the baseline and follow-up characteristics in patients from three subgroups with different treatments. Supplementary table 2. Comparison of the baseline and follow-up characteristics in patients classified by weight and ASM/W change. Supplementary table 3. Comparison of the baseline and follow-up characteristics in patients classified by ASM and ASM/W change. Supplementary table 4. Comparison of the baseline and follow-up characteristics in patients classified by weight and ASM change. Supplementary table 5. Factors associated with improvement of liver fat content* in univariate logistic regression analysis in all subjects and the subgroup classified by with and without weight loss. Supplementary table 6. Comparison of the baseline characteristics in the subgroup classified by BMI <25kg/m2 and BMI≥25kg/m2. Supplementary table 7. Factors associated with improvement of liver fat content* in univariate and multivariate logistic regression analysis in subjects classified by BMI <25kg/m2 and BMI≥25kg/m2. Supplementary table 8. Factors associated with improvement of liver fat content* in univariate and multivariate logistic regression analysis in subjects classified by BMI <30kg/m2 and BMI≥30kg/m2.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhou, T., Ye, J., Luo, L. et al. Restoring skeletal muscle mass as an independent determinant of liver fat deposition improvement in MAFLD. Skeletal Muscle 13, 23 (2023). https://doi.org/10.1186/s13395-023-00333-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13395-023-00333-z