
Abstract
Background
Despite the efficacy and safety of DIGIFab, it is relatively expensive and has limited availability. In addition, alternative interventions, such as therapeutic plasma exchange, may need to be considered in massive digoxin overdoses. Although few case reports describe its efficacy.
Case presentation
We report a case of a 17-year-old white male patient brought by family members to our emergency department in Riyadh, Saudi Arabia. After intentionally ingesting 48 mg of digoxin tablets to commit suicide, the patient’s initial digoxin serum level was 8.04 ng/mL. The patient was resuscitated in the emergency department. After admission to the intensive care unit, the patient underwent therapeutic plasma exchange, because of insufficient DIGIFab doses. Afterward, the serum digoxin levels drastically decreased, and his symptoms reverted. The patient was successfully managed and discharged 7 days after admission.
Conclusion
Despite insufficient evidence and a limited number of case reports describing the use of extracorporeal treatment in digoxin overdose, we noted the significant impact of therapeutic plasma exchange on our patient. However, therapeutic plasma exchange’s use in routine treatment requires stronger evidence to confirm its benefits.
Similar content being viewed by others


Background
Digoxin has positive inotropic and negative chronotropic effects on the heart, and is primarily used in treating heart failure and tachydysrhythmias [1]. In clinical practice, there is a high probability of accidental intoxication with digitalis owing to the narrow therapeutic window [2]. However, the number of reported suicide cases using digoxin was significant [3,4,5,6]. Compared with other medications, massive digoxin intoxication after a suicide attempt is uncommon [1].
Management of digitalis intoxication can be challenging. Digoxin-specific antibody fragments (DIGIFab) are indicated in cases with severe symptoms or in cases of massive overdose. It is the definitive treatment for life-threatening digitalis toxicity [7]. There are other methods to accelerate the clearance of drugs from the body, including therapeutic plasma exchange (TPE); although it is unable to clear digoxin, it has shown some success, mainly in cases of renal failure [8]. Furthermore, in one study, hemoperfusion did not significantly improve digoxin clearance because of digoxin’s large distribution volume [9]. Here, we present a case that illustrates the successful use of TPE after an insufficient DIGIFab dose to treat intoxication caused by the intentional ingestion of 192 tablets of 0.25 mg digoxin in an otherwise healthy 17-year-old patient. To date, only a few case reports have described the use of such a therapeutic approach in healthy patients with digoxin overdose.
Case presentation
The patient was a 17-year-old white male, previously in good health. He was not on any medications, he was a non-smoker, and he weighed 50 kg. Regarding the social status of the patient, he was living with his family, as he was high school student. He was brought by family members to our emergency department (ED) in Riyadh, Saudi Arabia. The patient was admitted after an overdose of digoxin 4 hours before presentation in a suicide attempt. He ingested 192 tablets of 0.25 mg digoxin (total dose of 48 mg). He developed dizziness, nausea, and vomiting after ingestion. Upon presentation, his Glasgow Coma Scale (GCS) score was 14/15, as the patient’s eyes opened to verbal commands. He was slightly drowsy but responded to questions and was fully oriented. The rest of other systems examinations were all unremarkable. The patient’s vital signs were as follows: heart rate, 118/minute; blood pressure (BP), 128/90 mmHg; respiratory rate, 19 breaths/minute; and maintaining oxygen saturation, 99% on room air. The initial electrocardiogram (ECG) revealed sinus tachycardia (Fig. 1). While the patient was being assessed, he started having more symptoms, including seeing yellow hues and having a decrease in consciousness level, with a GCS score of 8/15. He responded with incomprehensible sounds, withdrawing his limbs and opening his eyes to pain. As the patient’s GCS score deteriorated, he was intubated for airway protection. After securing the patient’s airway, 50 g of activated charcoal was administered through a nasogastric tube (NGT). Shortly thereafter, despite the patient being under sedation using propofol and fentanyl infusions, he showed synchronized tonic–clonic movement of all limbs, for which he received midazolam 5 mg. Five DIGIFab vials (200 mg) were administered as a bolus after extracting all routine laboratory tests, along with serum digoxin levels and urine toxicology screening. The intensive care unit (ICU), toxicology center, and cardiology services were consulted. He was immediately transferred to the ICU for further medical management. The initial serum chemistry was normal, except for a potassium level of 2.9 mmol/L, so he received 20 mmol of potassium chloride intravenously. The toxicological levels in our patient revealed a digoxin level of 8.04 ng/mL in the blood 4 hours post-ingestion and before he received the DIGIFab. Labs results, including complete blood count (CBC) and renal and liver functions, were all within normal range. In addition, serum ethanol concentration and urine toxicology screening results were negative for cocaine, opioids, cannabis, and amphetamine. In the ICU, the patient received five vials of DIGIFab intravenously. Given the high serum digoxin level and the patient’s condition, both a dialysis line and a central venous catheter (CVC) were inserted electively, and were used later for TPE management and medication administration, respectively. TPE was performed for over 2 hours using a dual-lumen CVC, (replacement used = 2210 ml; plasma removed = 2345 ml; TBV processed = 1.1 volume). Serum digoxin measured immediately after TPE was 4.07 ng/ mL (Fig. 3). Shortly after TPE, the patient’s ECG demonstrated a first-degree heart block (Fig. 2) with a heart rate of 43 beats per minute (BPM) and T-wave inversion. Another two vials (80 mg) of DIGIFab were used. The patient was closely monitored, and serum electrolyte and digoxin levels were regularly monitored, showing a gradual decrease over time (Fig. 3). Four days after continuous monitoring, gradual improvement was marked clinically, with the absence of any ECG changes and the disappearance of any signs of digoxin overdose. Two days later, the patient was extubated and found to have hyperactive delirium with agitation; he was disoriented and was pulling on his lines. Haloperidol (5 mg) was administered. Subsequently, the patient gradually became less agitated and showed an improvement in his mental status. The following day, the patient’s mental status returned to baseline, and he was transferred to a general ward, where he underwent a psychiatric assessment and was discharged in a stable condition after 7 days of hospitalization. Upon follow-up in 6 months, a phone call was made to his legal guardian to check up on the patient, since the discharging team did not schedule any follow-up as the patient status was not needed. According to him, he is in good health and doing regular follow-up with his primary care and psychiatric physicians.

Initial electrocardiogram revealed a sinus tachycardia

Electrocardiogram revealed a sinus bradycardia, first-degree heart block with T-wave inversion in anterio-septal leads

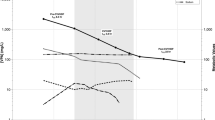
Our patient’s serum digoxin and potassium concentrations during and since presentation. Arrow (1): Initial digoxin level upon arrival 4 hours post-ingestion. Arrow (2): Digoxin level after therapeutic plasma exchange and DIGIFab. Arrow (3): Serum digoxin on second day. Arrow (4): Upon discharge
Discussion
Our article reports a case of a young and previously healthy male who ingested 192 tablets of 0.25 mg digoxin, and underwent timely and aggressive management, including immediate resuscitation, activated charcoal, DIGIFab, and TPE. This helped the patient to return back to his regular life completely healthy after 7 days of hospitalization.
Understanding the pharmacological actions of digoxin will help explain its toxic effects. It has a weak positive inotropic effect, by inhibiting the Na+–K+ ATPase pump and indirectly increasing calcium availability to the contractile elements of the myofibril [10]. Although toxicity is infrequent, it has serious clinical manifestations [11]. The case presented in this report emphasizes the different digoxin toxicity presentations and the significance of initiating aggressive and early management and considering other modalities of treatment based not only on serum drug levels but also on clinical presentation. Due to early initiation of DIGIFab, TPE, and activated charcoal, the patient showed a successful gradual response, with digoxin levels quickly declining and dramatic improvement in his clinical manifestations.
Digoxin toxicity presents nonspecifically as cardiac or non-cardiac symptoms, making diagnosis difficult [10, 12,13,14]. Gastrointestinal symptoms are the most common presentation, accounting for 30–70% of cases [15,16,17]. Cardiotoxic effects of digoxin can manifest as arrhythmias and conduction disturbances, but the frequency of these is controversial [18]. Early dysrhythmias associated with digoxin toxicity are premature ventricular contractions (PVC),
Conduction blocks in the intoxication setting can range from first-degree atrioventricular (AV) block to complete heart block, with a low incidence of sinus bradycardia and tachycardia [19]. Neuropsychiatric presentations are less common and often attributed to other causes. Few cases have reported lethargy, delirium, seizures, and visual disturbances as side effects of intoxication. Digoxin-induced seizures exhibit chronic toxicity, with frequent attacks showing metabolic and epileptiform patterns on EEG. These seizures resolve completely with digoxin toxicity treatment [20].
Digoxin toxicity is classically associated with significant hyperkalemia [21]; however, in our case, the patient had an initial potassium level of 2.9 mmol/L even before initiating the management, which goes against the classical finding of hyperkalemia reported in the literature. This is an interesting paradoxical finding, as there was no acute co-ingestion of other medications, and our patient was a healthy young male not taking any medications or supplements.
Specific therapies for digoxin toxicity have aimed at rapidly reducing the serum digoxin concentration, including the administration of DIGIFab, as it binds to digoxin, forming a complex excreted in the urine. However, despite the efficacy and safety of DIGIFab, it is expensive, and availability is limited; thus, alternative measures may need to be considered for severe intoxication [11]. Administration of DIGIFab should be based on the serum concentration or history and clinical state of the patient, supported by biological monitoring. If the clinical response after administration is not seen within 2 hours, a further dosage should be administered [20]. Using the DIGIFab dose calculation [22], total body load was calculated by multiplying the dose of digoxin ingested (48 mg) by 0.8 (digoxin bioavailability), and the total body load of digoxin was divided by the amount of digoxin neutralized per vial (0.5 mg per vial; DIGIFab dose (number of vials) = total digoxin load (mg)/0.5 mg of digoxin neutralized per vial). Based on the ingestion amount, our patient’s calculated dose was 76.8 vials. This amount was not available at our center during the initial resuscitation of the patient.
Different ECTR modalities have been used to treat digoxin toxicity. TPE and other ECTR have been suggested as possible interventions in patients with massive overdose, especially when DIGIFab is unavailable, or doses are insufficient. TPE has been shown to be potentially effective, as it removes toxic substance rapidly from the blood stream, allowing removal of protein-bound molecules and large molecular weight [23]. In our case, the choice to treat the patient with TPE was mainly driven by the insufficient availability of DIGIFab vials. However, we observed a significant improvement in patient manifestations and a reduction in digoxin serum levels (Fig. 3). However, the level of evidence was determined to be low, as the vast majority of available data evaluating the effectiveness of ECTR in digoxin poisoning in both acute and chronic ingestion are case reports and case series with no controlled trials allowing adequate comparison of the risks and benefits of TPE in digoxin toxicity [8, 9, 24, 25]. It has been suggested that starting a TPE session up to 3 hours after administration of DIGIFab will possibly maximize Fab–digoxin clearance [8]. In one study [26], a TPE removed 0.250 mg over a 90-minute session successfully, which might be explained by modifications of digoxin toxicokinetics following Fab administration. An experimental study [27] has examined the effects of both hemodialysis and plasmapheresis after induced digoxin intoxication, with the latter being more effective. However, the efficacy was mainly dependent on the plasma exchange rate. In all experiments with either hemodialysis or plasmapheresis, the levels increased again to some extent after cessation of the dialysis, which probably related to the release of the drug from tissue storage. Thus, for the effective elimination of the drug, it might be necessary to perform repetitive plasmapheresis for a certain period of time.
In our patient experience, administration of DIGIFab followed closely by a 2-hour TPE single session was probably the key of treatment efficacy.
Conclusion
Patients’ clinical response to the initial dose of DIGIFab serves as a guide for the need for further doses and the use of other adjunctive modalities, such as TPE. However, despite insufficient evidence, unavailability of clinical trials, and a limited number of case reports describing the use of ECTR in digoxin overdose, we noticed a significant effect of TPE on clinical symptoms and digoxin serum levels. However, the use of this modality for routine treatment requires stronger evidence to establish its benefits, a further protocols that can help us understand when and under what circumstances TPE can be beneficial for patients with digoxin toxicity.
Availability of data and materials
The data used to support the findings of this study are available from the corresponding author upon request.
Abbreviations
- TPE:
-
Therapeutic plasma exchange
- ICU:
-
Intensive care unit
- ED:
-
Emergency department
- ECTR:
-
Extracorporeal treatment
- CVC:
-
Central venous catheter
- GCS:
-
Glasgow coma scale
References
Ciechański E, Ciechański KL, Tchórz M. Suicidal digoxin intoxication in 61 year old patient. J Educ Health Sport. 2019;9(8):801–6.
Patocka J, Nepovimova E, Wu W, Kuca K. Digoxin: pharmacology and toxicology—a review. Environ Toxicol Pharmacol. 2020;1(79): 103400.
Hauptman PJ, Blume SW, Lewis EF, Ward S. Digoxin toxicity and use of digoxin immune fab: insights from a national hospital database. JACC Heart Failure. 2016;4(5):357–64.
Szponar J, Tchórz M, Drelich G, Gnyp L, Lewandowska-Stanek H. Severe digoxin poisoning a case study. Przegl Lek. 2011;68(8):515–7.
See I, Shehab N, Kegler SR, Laskar SR, Budnitz DS. Emergency department visits and hospitalizations for digoxin toxicity: United States, 2005 to 2010. Circulation. 2014;7(1):28–34.
Garg A, Panda S, Dalvi P, Mehra S, Ray S, Singh VK. Severe suicidal digoxin and propranolol toxicity with insulin overdose. Indian J Crit Care Med. 2014;18(3):173.
Unal S, Bayrakci B, Yasar U, Karagoz T. Successful treatment of propafenone, digoxin and warfarin overdosage with plasma exchange therapy and rifampicin. Clin Drug Investig. 2007;27:505–8.
Pellegrino M, Garofalo M. Digoxin-specific Fab and therapeutic plasma exchange for digitalis intoxication and renal failure. Am J Emerg Med. 2019;37(4):798-e3.
Mowry JB, Burdmann EA, Anseeuw K, Ayoub P, Ghannoum M, Hoffman RS, Lavergne V, Nolin TD, Gosselin S, EXTRIP workgroup. Extracorporeal treatment for digoxin poisoning: systematic review and recommendations from the EXTRIP Workgroup. Clin Toxicol. 2016;54(2):103–14.
Smith TW, Antman EM, Friedman PL, et al. Digitalis glycosides: mechanisms and manifestations of toxicity. Part I Prog Cardiovasc Dis. 1984;26:413–58.
Pincus M. Management of digoxin toxicity. Aust Prescr. 2016;39(1):18–20.
Kelly RA, Smith TW. Recognition and management of digitalis toxicity. Am J Cardiol. 1992;69:108-8G.
Smith TW, Antman EM, Friedman PL, et al. Digitalis glycosides: mechanisms and manifestations of toxicity. Part III. Prog Cardiovasc Dis. 1984;27:21–56.
Smith TW, Antman EM, Friedman PL, et al. Digitalis glycosides: mechanisms and manifestations of toxicity. Part II. Prog Cardiovasc Dis. 1984;26:495–540.
The Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med. 1997;336:525–33.
Williamson KM, Thrasher KA, Fulton KB, et al. Digoxin toxicity: an evaluation in current clinical practice. Arch Intern Med. 1998;158:2444–9.
Mahdyoon H, Battilana G, Rosman H, et al. The evolving pattern of digoxin intoxication: observations at a large urban hospital from 1980 to 1988. Am Heart J. 1990;120:1189–94.
Bauman JL, DiDomenico RJ, Galanter WL. Mechanisms, manifestations, and management of digoxin toxicity in the modern era. Am J Cardiovasc Drugs. 2006;6:77–86.
Irons GV Jr, Orgain ES. Digitalis-induced arrhythmias and their management. Prog Cardiovasc Dis. 1966;8(6):539–69.
Kerr DJ, Elliott HL, Hillis WS. Epileptiform seizures and electroencephalographic abnormalities as manifestations of digoxin toxicity. Br Med J (Clin Res Ed). 1982;284(6310):162–3. https://doi.org/10.1136/bmj.284.6310.162.
Bismuth C, Gaultier M, Conso F, Efthymiou ML. Hyperkalemia in acute digitalis poisoning: prognostic significance and therapeutic implications. Clin Toxicol. 1973;6(2):153–62. https://doi.org/10.3109/15563657308990513.
Antman EM, Wenger TL, Butler VP Jr, Haber E, Smith TW. Treatment of 150 cases of life-threatening digitalis intoxication with digoxin-specific Fab antibody fragments. Final report of a multicenter study. Circulation. 1990;81(6):1744–52. https://doi.org/10.1161/01.cir.81.6.1744.
Schutt RC, Ronco C, Rosner MH. The role of therapeutic plasma exchange in poisonings and intoxications. In: Seminars in dialysis, Vol. 25, No. 2. Oxford, UK: Blackwell Publishing Ltd, 2012, pp. 201–206
Rajpal S, Beedupalli J, Reddy P. Recrudescent digoxin toxicity treated with plasma exchange: a case report and review of literature. Cardiovasc Toxicol. 2012;12:363–8.
Zdunek M, Mitra A, Mokrzycki MH. Plasma exchange for the removal of digoxin-specific antibody fragments in renal failure: timing is important for maximizing clearance. Am J Kidney Dis. 2000;36(1):177–83.
Caputo M, Coppola E, Amaduzzi F, et al. Digitalis intoxication in a chronic hemodialysis patient: plasmapheresis and hemofiltration after FAB therapy. G Ital Nefrol. 1997;14:125–8 (Italian).
Tsuyuki M, Kawamura T, Inagaki Y. Effects of plasmapheresis on experimentally induced digitalis intoxication. J Artif Organs. 1982;11:74–7 (Japanese).
Acknowledgements
Not applicable.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
MIA and HMA supervised the study and critically reviewed the manuscript for important intellectual content. BA edited and critically reviewed the manuscript for important intellectual content. NAA helped in the data collection, assisted with writing and editing the manuscript, and critically reviewed the manuscript for important intellectual content. RMA collected and coordinated the data collection, wrote and edited the manuscript, and critically reviewed the manuscript for important intellectual content. All authors read and approved the final version of manuscript to be published.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study has been approved from the Institutional Review Board of King Saud University Medical City, and written informed consent was received from the patient’s legal guardian for publication of this case report.
Consent for publication
Written informed consent was obtained from the patient’s legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that there is no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Alhussein, R.M., Alamri, N.A., Alhashem, H.M. et al. Successful management of massive digoxin overdose using DIGIFab and therapeutic plasma exchange: a case report. J Med Case Reports 18, 135 (2024). https://doi.org/10.1186/s13256-024-04386-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13256-024-04386-6