
Abstract
Background
Resistance to dopamine agonists is not uncommonly seen in prolactinomas. However, development of resistance to dopamine agonists after an initial period of robust treatment response is rare, and only 39 cases have been reported in the past four decades. We describe a Chinese man with this rare condition and explored the postulated mechanisms that may explain this phenomenon. We compiled similar cases that were previously reported and compared their etiology, progress, and response to treatment. On the basis of these cases, we derived a list of differential diagnoses to consider in patients with secondary resistance to dopamine agonists.
Case presentation
A 63-year-old Chinese man presented with blurred vision and was subsequently diagnosed with a macroprolactinoma. He had initial response to cabergoline but developed secondary resistance to it after 5 years. The prolactinoma continued to grow, and his serum prolactin remained markedly elevated despite adherence to escalating dosages of cabergoline up to 6 mg/week. The patient finally underwent transsphenoidal surgery and was found to have a sparsely granulated lactotroph tumor with Ki-67 index of 5%. Postoperatively, there was improvement in his serum prolactin level, although he still required treatment with cabergoline at 6 mg/week.
Conclusions
Surgery can facilitate disease control in patients with prolactinomas that develop secondary resistance to dopamine agonists. Malignant prolactinoma is an important differential diagnosis in this group of patients, especially when serum prolactin remains markedly elevated despite resolution or stability of the primary pituitary lesion, suggesting a metastatic source of prolactin secretion.
Similar content being viewed by others

Background
Prolactinomas account for 30–60% of pituitary tumors [1, 2] and occur in 44.4–62.7 per 100,000 patients in cross-sectional studies [2, 3]. Dopamine agonists (DA) are the drugs of choice to treat prolactinomas. DA normalize prolactin (PRL) levels in more than 90% of people with microprolactinomas and in 77% of people with macroprolactinomas, and reduce tumor size in up to 89% of cases [4]. However, up to 10% of patients with microprolactinomas and less than 20% of patients with macroprolactinomas may not achieve normoprolactinemia or reduction in tumor size with DA therapy [5]. About 25% of people with prolactinomas are resistant to bromocriptine (BRC) and 10–15% are resistant to cabergoline (CAB) [6]. Most cases of DA resistance are apparent soon after starting therapy, and these patients are considered to have primary DA resistance. Rarely, patients develop hyperprolactinemia and/or tumor enlargement after an initial period of remarkable response, and these patients are considered to have secondary DA resistance. We describe a Chinese man with macroprolactinoma who developed secondary DA resistance and explore the possible mechanisms and clinical implications of this phenomenon. Our case report is the first to compile previous case reports on prolactinomas with secondary DA resistance to provide a comparison on their etiology, progress, and response to treatment. On the basis of these case reports, we derived a list of differential diagnoses to consider in this group of patients.
Methods
We searched PubMed for articles published using the terms “aggressive prolactinoma,” “bromocriptine,” “cabergoline,” “CV 205-502,” “dopamine agonist,” “dopamine agonist resistance,” “Ki-67,” “macroprolactinoma,” “malignant prolactinoma,” “microprolactinoma,” “pergolide,” “prolactinoma,” “prolactin-secreting adenoma,” “quinagolide,” and “secondary resistance.” We summarized available articles describing secondary DA resistance and contacted authors for clarification when there were inadequate or ambiguous data.
Case presentation
A 63-year-old Chinese man presented in November 2014 with gradual blurring of vision in his left eye for 3 months. His past medical history included type 2 diabetes mellitus, hypertension, and hyperlipidemia. He has no family history of pituitary or endocrine disorders. He was found to have bitemporal hemianopia and magnetic resonance imaging (MRI) showed a 2.4 × 2.0 × 2.0 cm (craniocaudal, transverse, and anteroposterior dimensions) lesion in the pituitary fossa with suprasellar extension and encasement of his left cavernous sinus. The MRI and perimetry in December 2014 are shown in Figs. 1A and B, and 2A respectively.

MRIs. A, B December 2014, C, D June 2015, E, F February 2020

Perimetry A December 2014, B June 2015, C December 2019
He reported no headache, diplopia, lethargy, postural dizziness, cold or heat intolerance, galactorrhea, or reduced frequency in shaving. He was not Cushingoid or acromegalic, and was clinically euthyroid. There was no postural hypotension. He had mild gynecomastia bilaterally and no galactorrhea. His blood tests showed PRL > 470 ug/L (reference: 4.0–15.2), free thyroxine 10.7 pmol/L (reference: 11.8–24.6), thyroid stimulating hormone 0.564 mU/L (reference: 0.270–4.200), early morning total testosterone 5.16 nmol/L (reference: 9.90–27.80), follicle stimulating hormone 4.8 IU/L (reference: 1.5–12.4), luteinizing hormone 4.1 IU/L (reference: 1.7–8.6), early morning cortisol 190 nmol/L (reference 171–536), adrenocorticotropic hormone 8.6 pmol/L (reference: 1.6–13.9), and insulin-like growth factor 1 153 ug/L (reference: 75–212). His peak cortisol with the Cosyntropin test was 667 nmol/L. He was diagnosed with a macroprolactinoma with hypogonadotropic hypogonadism and central hypothyroidism.
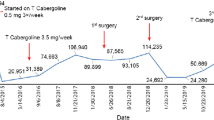
CAB 1 mg/week and levothyroxine 25 mcg daily was started in December 2014 with good biochemical and radiological response of the macroprolactinoma. There was improvement in his visual field defects. The MRI and perimetry in June 2015 are shown in Figs. 1C and D, and 2B respectively. He defaulted treatment after February 2017 and the macroprolactinoma had expanded in size by the time he returned to the endocrinology clinic in December 2019. His left eye vision and visual field defects had deteriorated then. The MRI in February 2020 and perimetry in December 2019 are shown in Figs. 1E and F, and 2C, respectively. CAB was resumed at 1.5 mg/week since December 2019.
However, the patient failed to show biochemical and radiological response despite adherence to escalating dosages of CAB after December 2019. Adherence was assessed on the basis of direct questioning of the patient and his next-of-kin as well as counting leftover cabergoline tablets. He reported no side effects with cabergoline. His PRL trend, tumor size, and medications are summarized in Table 1. He was referred to the neurosurgeons in December 2021 for consideration of surgery in view of tumor growth despite high doses of CAB and he finally agreed to surgery in September 2022. During the transsphenoidal surgery, a highly vascular tumor with a firm, adherent capsule was noted. Histology confirmed the presence of a lactotroph macroadenoma that was sparsely granulated and the tumor cells were strongly positive for PIT-1 and PRL. The Ki-67 index was 5% and no mitotic activity was seen. The hyperprolactinemia improved postoperatively from 236.6 ug/L to 100.8 ug/L and he was treated with CAB 2 mg/week.
Six weeks after surgery, he presented with acute deterioration of his vision on the left but MRI showed stable postoperative changes without significant compression on his optic tracts. His hyperprolactinemia had stagnated at 99.9 ug/L, so CAB was increased back to 6 mg/week and levothyroxine was increased in a stepwise manner to 100 mcg daily.
Discussion
Results of literature search
Between 1981 and 2022, at least 39 cases of prolactinomas with secondary DA resistance (excluding our case) have been reported in Europe, North and South America, Asia, and Australia. There was adequate information to confirm secondary DA resistance in 18 of these cases. Of the 39 cases, 12 were male, 11 were female, and the gender was not reported in 16 cases. The age of the patients was between 22 and 70 years. A total of 15 cases had macroprolactinomas, 3 had microprolactinomas, and the tumor size was not reported in 21 cases. The time to developing secondary DA resistance was between 10 months and 15 years. Four cases were treated with androgen or estrogen therapy prior to developing secondary DA resistance [7,8,9,10]. Importantly, ten cases were ultimately found to have malignant prolactinomas [9, 11,12,13,14,15,16]. The Ki-67/MIB-1 index was reported in seven cases. Of these, five cases had Ki-67 index > 3% [8, 10, 12, 17, 18], two cases had MIB-1 > 3% [19], and two cases had Ki-67 index < 3% [20, 21]. In eight cases, p53 staining was performed. Of these, three cases were positive [8, 19] and five were negative [17, 18, 20, 21]. We were unable to perform p53 staining in our institute. However, it appears from the available case reports that p53 correlates poorly with the clinical aggressiveness of prolactinomas with secondary DA resistance, while the Ki-67/MIB-1 index appears to be higher in aggressive prolactinomas. The reported cases with secondary DA resistance are summarized in Table 2. The baseline characteristics of these cases are summarized in Table 3.
Definition and frequency of DA resistance
There is no standardized definition for DA resistance. The most commonly used definition is failure to normalize PRL and/or reduce tumor volume by at least 50% using conventionally maximum or maximally tolerated doses of DA (for example, BRC 7.5 mg/day or CAB 2 mg/week) [5, 6, 22,23,24]. Doses of CAB up to 12 mg/week and BRC up to 30 mg/day were required in rare cases to achieve control of prolactinomas [25]. Ono et al. also recommend using DA at the maximum tolerated dose for at least 12 months before concluding that DA resistance is present [25].
There is also no proposed definition for secondary DA resistance. This makes it difficult to ascertain the frequency of secondary DA resistance. Furthermore, a significant proportion of cases of secondary DA resistance were reported before CAB was commercially available in 1992, so some of these may not be true cases of DA resistance. The majority of the reported cases of secondary DA resistance had achieved normoprolactinemia before PRL levels started to rise. Ten of these cases did not achieve normoprolactinemia, but most of them had reduction of PRL by more than 80% from baseline [9, 12, 15, 17, 19, 21, 26], with the exception of two cases where PRL fell by 48% [13] and 73% [14]. The PRL level in our patient had fallen by 84% from baseline in the initial 26 months of treatment before he developed secondary DA resistance. Thereafter, his PRL level stagnated between 144.4 ug/Land 282.5 ug/L despite escalating CAB from 1.5 mg/week to 6 mg/week. Given his remarkable initial response to CAB, we believe there should be no debate on the development of secondary DA resistance in this patient.
Differential diagnoses of secondary DA resistance
Before concluding that a patient has secondary DA resistance, it is pertinent to exclude non-adherence to therapy. There is also a need to consider if the patient has a non-lactotroph pituitary adenoma with stalk effect. Stalk effect can sometimes happen when the tumor comprises two populations of lactotroph and non-lactotroph cells; the non-lactotroph component causes the stalk effect while the lactotroph component caused the initial improvement with DA [17]. Occasionally, the tumor may expand due to hemorrhage, exerting a new stalk effect after an initial response. Certain medications such as spiramycin [27] may accelerate BRC clearance and reduce its efficacy. Gonadal steroid replacement may induce DA resistance in lactotrophs, and this was seen in four cases with secondary DA resistance [7,8,9,10]. An important differential diagnosis is malignant prolactinoma, which was reported in at least 10 of the 39 cases of secondary DA resistance [9, 11,12,13,14,15,16]. The PRL levels in such cases tended to be markedly elevated despite resolution or stability of the primary pituitary lesions, prompting exploration of additional foci of PRL secretion that led to discovery of metastases. Other differential diagnoses include pregnancy, physiologic causes of hyperprolactinaemia (for example, stress), interim development of pathologic causes of hyperprolactinaemia (for example, renal or hepatic impairment), and introduction of new medications (for example, antipsychotics).
Mechanisms of secondary DA resistance
DA bind to dopamine type 2 receptors (D2R) in prolactinomas resulting in inhibition of PRL secretion as well as reduction of tumor size [28]. True DA resistance has been attributed to various D2R defects in prolactinomas. Breidahl et al. demonstrated that secondary DA resistance in their patient developed due to growth of a population of lactotrophs that had reduced D2R expression [26]. Some lactotrophs may also produce structurally abnormal D2R that have reduced DA binding capacity [19, 29, 30]. The loss of D2R expression or affinity to DA may arise from late mutations in tumor cells [20], explaining the secondary resistance. D2R is expressed as short and long isoforms in human beings. The short isoform induces intracellular signalling via the MAPK and PI3k pathways while the long isoform inhibits these pathways [31]. A lower ratio of the short-to-long isoform has been shown to reduce the response of lactotrophs to DA [19, 30, 32, 33]. We were unable to perform D2R staining in our institute and were thus unable to ascertain if the secondary DA resistance in this patient was due to reduced D2R density.
It has been postulated that angiogenic factors (for example, vascular endothelial growth factor) promote tumor cell proliferation and angiogenesis in prolactinomas resistant to DA [17, 34]. This may confer the aggressive and invasive behavior of such tumors. The prolactinoma in our patient was noted to be highly vascular. However, we were unable to test for the presence of angiogenic factors in our institute.
Secondary DA resistance was previously reported in four cases that received gonadal steroid replacement [7,8,9,10]. Similarly, our patient started exhibiting secondary DA resistance after he was started on testosterone replacement therapy. This can probably be explained by the aromatization of testosterone to estrogen, which then regulates PRL gene expression, downregulates D2R, and stimulates lactotroph hyperplasia [35, 36]. However, in the prospective study conducted by Auriemma et al., DA resistance was not seen in nine hypogonadal males with prolactinomas who were started on testosterone replacement therapy. These patients had improvements in their metabolic profiles instead [37]. Molitch et al. [6] recommended the addition of aromatase inhibitors to counteract the estrogenic effect from testosterone therapy on the basis of a case report by Gillam et al. [38].
DA resistance has also been attributed to cell signalling defects. For example, defects in nerve growth factor (NGF) can disrupt autocrine growth factor signalling pathways in lactotrophs and disinhibit cell proliferation, causing prolactinomas to develop DA resistance [39]. Response to DA was restored after prolactinoma cells were exposed to NGF [40] in cell culture studies. Filamin-A is a cytoskeleton protein that is involved in D2R expression and function. D2R cannot be trafficked to the cell membrane in the absence of filamin-A [41]. Prolactinomas with DA resistance have reduced filamin-A expression, and inhibition of filamin-A expression using small interfering ribonucleic acids led to DA resistance [42]. In addition, micro ribonucleic acids may interfere with intracellular signalling and induce fibrosis in DA-resistant prolactinomas [43], resulting in failure of tumor volume reduction [17].
Treatment strategies in secondary DA resistance
In patients who developed resistance to BRC, switching to CAB is a reasonable first-line strategy. This is because CAB has superior efficacy in normalizing PRL levels and reducing tumor size due to its higher affinity for D2R, leading to better cytocidal effects [44,45,46]. About 33% of patients with macroprolactinomas fail to achieve tumor shrinkage by at least 50% using BRC. Of these, 70% respond to CAB [6]. CAB also has superior side effect profile compared with other DA [45, 47, 48].
In patients with concurrent hypopituitarism or central hypothyroidism, we recommend thyroid replacement therapy to keep the serum free thyroxine in the upper half of the reference interval. As thyrotropin releasing hormone stimulates prolactin release [49], the negative feedback exerted by thyroxine on hypothalamic thyrotropin releasing hormone secretion can help to reduce the stimulation of prolactin release.
Our patient was recommended for surgical resection after high doses of CAB failed to normalize his PRL and reduce tumor volume. Surgical resection was also performed in 17 of the reported cases. Three of the reported cases with secondary DA resistance received DA therapy in conjunction with surgery and achieved reduction in PRL by more than 50% after surgery [18, 20, 26]. A total of 11 cases had surgery and required extra treatment modalities (for example, radiotherapy) in addition to DA therapy. Of these, three achieved reductions in PRL by more than 50% [18, 21, 50]. Thus, it appears that response to surgical resection is variable. Surgical resection has the additional advantage of providing tissue samples for immunohistological evaluation for cellular atypia, mitotic burden, and proliferation index. None of the cases treated with somatostatin analogue [17], tamoxifen [11], and chemotherapy [15] achieved significant reduction in PRL levels. Temozolomide was proposed as a plausible option by Sbardella [8] et al. We recommend a low threshold for repeating MRI in patients whose histopathological samples showed high proliferative indices (for example, Ki-67 index > 3%), and who have unexpected or unexplained rise in PRL from their postoperative baseline, as this group of patients appear to be at higher risk for local recurrence and metastases. We also recommend further imaging to detect metastases if the MRI were to show stable changes in the parasellar region in this group of patients.
Conclusion
Secondary DA resistance in prolactinomas is a rare phenomenon and has been reported to occur up to 15 years after presentation. Mixed tumors, D2R defects, and abnormal cell signalling pathways may explain the development of secondary DA resistance. Importantly, malignant prolactinomas need to be considered as a differential diagnosis in such cases. Early surgery for tumor resection or debulking may confer additional biochemical control and provide tissue for immunohistological evaluation.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AP:
-
Anteroposterior
- BRC:
-
Bromocriptine
- CAB:
-
Cabergoline
- CC:
-
Craniocaudal
- DA:
-
Dopamine agonists
- D2R:
-
Dopamine type 2 receptors
- DXT:
-
Radiotherapy
- EOD:
-
Every other day
- F:
-
Female
- F–S:
-
Fridays to Sundays
- FT4:
-
Free thyroxine
- GHD:
-
Growth hormone deficiency
- HPF:
-
High power field
- LT4:
-
Levothyroxine
- M:
-
Male
- M–F:
-
Mondays to Fridays
- MRI:
-
Magnetic resonance imaging
- M–T:
-
Mondays to Thursday
- NA:
-
Not available
- NGF:
-
Nerve growth factor
- OM:
-
Once daily
- P:
-
Pergolide
- PRL:
-
Prolactin
- PRLoma:
-
Prolactinoma
- Q:
-
Quinagolide
- RI:
-
Reference interval
- S:
-
Surgery
- S–S:
-
Saturdays to Sundays
- T:
-
Testosterone cypionate
- TR:
-
Transverse
- ULN:
-
Upper limit of normal
References
Clayton RN. Sporadic pituitary tumours: from epidemiology to use of databases. Baillieres Best Pract Res Clin Endocrinol Metab. 1999;13(3):451–60.
Daly AF, Rixhon M, Adam C, Dempegioti A, Tichomirowa MA, Beckers A. High prevalence of pituitary adenomas: a cross-sectional study in the province of Liege. Belgium J Clin Endocrinol Metab. 2006;91(12):4769–75.
Fernandez A, Karavitaki N, Wass JAH. Prevalence of pituitary adenomas: a community-based, cross-sectional study in Banbury (Oxfordshire, UK). Clin Endocrinol (Oxf). 2010;72(3):377–82.
Bevan JS, Webster J, Burke CW, Scanlon MF. Dopamine agonists and pituitary tumor shrinkage. Endocr Rev. 1992;13(2):220–40.
Di Sarno A, Landi ML, Cappabianca P, Di Salle F, Rossi FW, Pivonello R, et al. Resistance to cabergoline as compared with bromocriptine in hyperprolactinemia: prevalence, clinical definition, and therapeutic strategy. J Clin Endocrinol Metab. 2001;86(11):5256–61.
Molitch ME. Management of medically refractory prolactinoma. J Neurooncol. 2014;117(3):421–8.
Delgrange E, Crabbé J, Donckier J. Late development of resistance to bromocriptine in a patient with macroprolactinoma. Horm Res Paediatr. 1998;49(5):250–3.
Sbardella E, Farah G, Fathelrahman A, Cudlip S, Ansorge O, Karavitaki N, et al. A macroprolactinoma becoming resistant to cabergoline and developing atypical pathology. Endocrinol Diabetes Metab Case Rep. 2016;2016:78.
Scheithauer BW, Randall RV, Laws ER, Kovacs KT, Horvath E, Whitaker MD. Prolactin cell carcinoma of the pituitary. Clinicopathologic, immunohistochemical, and ultrastructural study of a case with cranial and extracranial metastases. Cancer. 1985;55(3):598–604.
Zornitzki T, Knobler H, Nass D, Hadani M, Shimon I. Increased MIB-1/Ki-67 Labeling index as a predictor of an aggressive course in a case of prolactinoma. Horm Res Paediatr. 2004;61(3):111–6.
Assies J, Verhoeff NPLG, Bosch DA, Hofland LJ. Intracranial dissemination of a macroprolactinoma. Clin Endocrinol (Oxf). 1993;38(5):539–46.
Kars M, Roelfsema F, Romijn JA, Pereira AM. Malignant prolactinoma: case report and review of the literature. Eur J Endocrinol. 2006;155(4):523–34.
Martin NA, Hales M, Wilson CB. Cerebellar metastasis from a prolactinoma during treatment with bromocriptine: Case report. J Neurosurg. 1981;55(4):615–9.
Petrossians P, De Herder W, Kwekkeboom D, Lamberigts G, Stevenaert A, Beckers A. Malignant Prolactinoma Discovered by D2 Receptor Imaging. J Clin Endocrinol Metab. 2000;85(1):398–401.
Petterson T, MacFarlane IA, MacKenzie JM, Shaw MD. Prolactin secreting pituitary carcinoma. J Neurol Neurosurg Psychiatry. 1992;55(12):1205–6.
Pernicone PJ, Scheithauer BW, Sebo TJ, Kovacs KT, Horvath E, Young WF, et al. Pituitary carcinoma: A clinicopathologic study of 15 cases. Cancer. 1997;79(4):804–12.
Mallea-Gil MS, Cristina C, Perez-Millan MI, Villafañe AMR, Ballarino C, Stalldecker G, et al. Invasive giant prolactinoma with loss of therapeutic response to cabergoline: expression of angiogenic markers. Endocr Pathol. 2009;20(1):35–40.
McCall D, Hunter SJ, Cooke RS, Herron B, Sheridan B, Atkinson AB. Unusual late development of dopamine agonist resistance in two women with hyperprolactinaemia associated with transition from micro to macroadenoma. Clin Endocrinol (Oxf). 2006;12:3.
Shimazu S, Shimatsu A, Yamada S, Inoshita N, Nagamura Y, Usui T, et al. Resistance to dopamine agonists in prolactinoma is correlated with reduction of dopamine D2 receptor long isoform mRNA levels. Eur J Endocrinol. 2012;166(3):383–90.
Alberiche Ruano M, Boronat Cortés M, Ojeda Pino A, Rodriguez Perez C, Gracía Nuñez M, Marrero Arencibia D, et al. Acquired resistance to cabergoline: progression from initially responsive micro to macroprolactinoma. Pituitary. 2010;13(4):380–2.
Behan LA, Draman MS, Moran C, King T, Crowley RK, O’Sullivan EP, et al. Secondary resistance to cabergoline therapy in a macroprolactinoma: a case report and literature review. Pituitary. 2011;14(4):362–6.
Melmed S, Casanueva FF, Hoffman AR, Kleinberg DL, Montori VM, Schlechte JA, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(2):273–88.
Delgrange E, Daems T, Verhelst J, Abs R, Maiter D. Characterization of resistance to the prolactin-lowering effects of cabergoline in macroprolactinomas: a study in 122 patients. Eur J Endocrinol. 2009;160(5):747–52.
Vroonen L, Jaffrain-Rea ML, Petrossians P, Tamagno G, Chanson P, Vilar L, et al. Prolactinomas resistant to standard doses of cabergoline: a multicenter study of 92 patients. Eur J Endocrinol. 2012;167(5):651–62.
Ono M, Miki N, Kawamata T, Makino R, Amano K, Seki T, et al. Prospective study of high-dose cabergoline treatment of prolactinomas in 150 patients. J Clin Endocrinol Metab. 2008;93(12):4721–7.
Breidahl HD, Topliss DJ, Pike JW. Failure of bromocriptine to maintain reduction in size of a macroprolactinoma. BMJ. 1983;287(6390):451–2.
Dallabonzana D, Spelta B, Oppizzi G, Tonon C, Luccarelli G, Chiodini PG. Reenlargement of macroprolactinomas during bromocriptine treatment: report of two cases. J Endocrinol Invest. 1983;6:47–50.
Pivonello R, Ferone D, Lombardi G, Colao A, Lamberts SWJ, Hofland LJ. Novel insights in dopamine receptor physiology. Eur J Endocrinol. 2007;156:S13-21.
Pellegrini I, Rasolonjanahary R, Gunz G, Bertrand P, Delivet S, Jedynak CP, et al. Resistance to bromocriptine in prolactinomas. J Clin Endocrinol Metab. 1989;69(3):500–9.
Caccavelli L, Feron F, Morange I, Rouer E, Benarous R, Dewailly D, et al. Decreased expression of the two D2 dopamine receptor isoforms in bromocriptine-resistant prolactinomas. Neuroendocrinology. 1994;60(3):314–22.
Radl D, De Mei C, Chen E, Lee H, Borrelli E. Each individual isoform of the dopamine D2 receptor protects from lactotroph hyperplasia. Mol Endocrinol Baltim Md. 2013;27(6):953–65.
Kukstas LA, Domec C, Bascles L, Bonnet J, Verrier D, Israel JM, et al. Different expression of the two dopaminergic D2 receptors, D2415 and D2444, in two types of lactotroph each characterised by their response to dopamine, and modification of expression by sex steroids. Endocrinology. 1991;129(2):1101–3.
Wu ZB, Zheng WM, Su ZP, Chen Y, Wu JS, Wang CD, et al. Expression of D2RmRNA isoforms and ERmRNA isoforms in prolactinomas: correlation with the response to bromocriptine and with tumor biological behavior. J Neurooncol. 2010;99(1):25–32.
Gürlek A, Karavitaki N, Ansorge O, Wass JAH. What are the markers of aggressiveness in prolactinomas? Changes in cell biology, extracellular matrix components, angiogenesis and genetics. Eur J Endocrinol. 2007;156(2):143–53.
Freeman ME, Kanyicska B, Lerant A, Nagy G. Prolactin: structure, function, and regulation of secretion. Physiol Rev. 2000;80(4):1523–631.
Grattan DR. 60 YEARS OF NEUROENDOCRINOLOGY: The hypothalamo-prolactin axis. J Endocrinol. 2015;226(2):T101-122.
Auriemma RS, Galdiero M, Vitale P, Granieri L, Lo Calzo F, Salzano C, et al. Effect of chronic cabergoline treatment and testosterone replacement on metabolism in male patients with prolactinomas. Neuroendocrinology. 2015;101(1):66–81.
Gillam MP, Middler S, Freed DJ, Molitch ME. The novel use of very high doses of cabergoline and a combination of testosterone and an aromatase inhibitor in the treatment of a giant prolactinoma. J Clin Endocrinol Metab. 2002;87(10):4447–51.
Missale C, Losa M, Sigala S, Balsari A, Giovanelli M, Spano PF. Nerve growth factor controls proliferation and progression of human prolactinoma cell lines through an autocrine mechanism. Mol Endocrinol Baltim Md. 1996;10(3):272–85.
Missale C, Boroni F, Losa M, Giovanelli M, Zanellato A, Dal Toso R, et al. Nerve growth factor suppresses the transforming phenotype of human prolactinomas. Proc Natl Acad Sci U S A. 1993;90(17):7961–5.
Lin R, Canfield V, Levenson R. Dominant negative mutants of filamin A block cell surface expression of the D2 dopamine receptor. Pharmacology. 2002;66(4):173–81.
Peverelli E, Mantovani G, Vitali E, Elli FM, Olgiati L, Ferrero S, et al. Filamin-A is essential for dopamine d2 receptor expression and signaling in tumorous lactotrophs. J Clin Endocrinol Metab. 2012;97(3):967–77.
Hu B, Mao Z, Du Q, Jiang X, Wang Z, Xiao Z, et al. miR-93-5p targets Smad7 to regulate the transforming growth factor-β1/Smad3 pathway and mediate fibrosis in drug-resistant prolactinoma. Brain Res Bull. 2019;149:21–31.
Sabuncu T, Arikan E, Tasan E, Hatemi H. Comparison of the effects of cabergoline and bromocriptine on prolactin levels in hyperprolactinemic patients. Intern Med Tokyo Jpn. 2001;40(9):857–61.
Webster J, Piscitelli G, Polli A, Ferrari CI, Ismail I, Scanlon MF. A comparison of cabergoline and bromocriptine in the treatment of hyperprolactinemic amenorrhea. N Engl J Med. 1994;331(14):904–9.
Eguchi K, Kawamoto K, Uozumi T, Ito A, Arita K, Kurisu K. Effect of cabergoline, a dopamine agonist, on estrogen-induced rat pituitary tumors. In Vitro Culture Studies Endocr J. 1995;42(3):413–20.
Verhelst J, Abs R, Maiter D, van den Bruel A, Vandeweghe M, Velkeniers B, et al. Cabergoline in the treatment of hyperprolactinemia: a study in 455 patients. J Clin Endocrinol Metab. 1999;84(7):2518–22.
Di Sarno A, Landi ML, Marzullo P, Di Somma C, Pivonello R, Cerbone G, et al. The effect of quinagolide and cabergoline, two selective dopamine receptor type 2 agonists, in the treatment of prolactinomas. Clin Endocrinol (Oxf). 2000;53(1):53–60.
Jackson IM. Thyrotropin-releasing hormone. N Engl J Med. 1982;306(3):145–55.
Kupersmith MJ, Kleinberg D, Warren FA, Budzilovitch G, Cooper P. Growth of prolactinoma despite lowering of serum prolactin by bromocriptine. Neurosurgery. 1989;24(3):417–23.
Brue T, Pellegrini I, Priou A, Morange I, Jaquet P. Prolactinomas and resistance to dopamine agonists. Horm Res. 1992;38(1–2):84–9.
Laboy-Ortiz IE, Velez-Maymí S, Hernán Martínez J, Trinidad R, Mangual M, Sanchez A, et al. Secondary resistance to dopamine agonist after thirteen months of successful treatment in a 42 years old man. Boletin Asoc Medica. 2016;108(10066):29–34.
Astafeva LI, Kadashev BA, Trunin II. Rotin DL [Development of secondary resistance to dopamine agonists in a patient with giant prolactinoma]. Zh Vopr Neirokhir Im N N Burdenko. 2010;4:48–51.
Acknowledgements
Not applicable.
Funding
The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
E-LT wrote the main manuscript and prepared the figures and tables. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Domain Specific Review Board of the National Healthcare Group has confirmed that no ethical approval is required.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tng, EL., Teo, A.E.D. & Aung, A.T. Macroprolactinoma with secondary resistance to dopamine agonists: a case report and review of the literature . J Med Case Reports 17, 96 (2023). https://doi.org/10.1186/s13256-023-03820-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13256-023-03820-5