
Abstract
Background
Anomalies in primary teeth are comparatively fewer than in the permanent teeth. The presence of a primary canine with two roots is very rare. An unusual anomaly like this may lead to problems during extraction or exfoliation. Emphasis on the importance of anomalies is required for proper diagnosis and to facilitate a better treatment outcome.
Case presentation
The present case report describes a case of a bilateral bi-rooted primary maxillary canines diagnosed during a radiographic examination in a 9-year-old Saudi boy. To the best of our knowledge, this is the first case of bi-rooted primary maxillary canine reported from the region of Saudi Arabia.
Conclusion
This case report aims to increase awareness of the morphological alterations in primary canines and to emphasize the importance of diagnosis and radiographic examination using different angles. Clinicians should consider all the possible tooth variations during routine intra-oral and radiographic examinations to facilitate a better treatment outcome and to avoid unwanted complications.
Similar content being viewed by others


Background
The primary and the permanent teeth are subject to considerable variation in their form, size, number, and structure of the dental tissues. Abnormalities in tooth morphology in primary teeth are comparatively fewer than in the permanent teeth [1]. The presence of a single root in a primary canine has been described as a normal and the most common form of root morphology. However, few cases have been reported regarding the presence of a bi-rooted primary canine, the first being in 1941 [2]. It has been seen that the prevalence of bi-rooted primary canines is higher in the maxilla than in the mandible and they seem to occur bilaterally [3]. Although, the exact etiology of this anomaly is unknown, it has been suggested that an ingrowth of a tissue from Hertwig’s epithelial root sheath may be a possible cause [4]. This case report describes a case of bi-rooted primary maxillary canines occurring bilaterally. The present case report aims to increase awareness about the morphological alterations in primary canines and to emphasize the importance of diagnosis and radiographic examination using different angles.
Case presentation
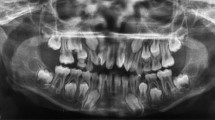
On 3 April 2017, a 9-year-old Saudi boy with a complaint of missing teeth in maxillary anterior region visited the Department of Preventive Dental Science, Faculty of Dentistry, Najran University, Saudi Arabia. On 15 April 2017, he underwent a clinical examination which revealed: unerupted permanent maxillary lateral incisors; decay in tooth numbers 54, 55, 62, 64, 65, 26, 84, 74, 75, and 85 (Federation Dentaire Internationale notation); and anterior crossbite between tooth numbers 53 and 83. Radiographic examination revealed bi-rooted bilateral maxillary canines (53 and 63) (Fig. 1). On 25 April 2017, a treatment plan was made followed by: pulpotomy and stainless steel crowns in tooth numbers 55, 74, and 75; extraction of 54, 62, 64, 65, and 85; composite restoration in 84; amalgam restoration in 26; and fissure sealant was placed on 16, 36, and 46. Space evaluation and orthodontic consultation to facilitate the eruption of permanent maxillary lateral incisors (12 and 22) was done and extraction of bilateral primary canines (53 and 63) was indicated. Following extraction, the presence of two roots was confirmed by careful examination. The right primary maxillary canine had two separate roots (mesial and distal) (Fig. 2), whereas the left primary maxillary canine had two roots (mesial and distal) which were connected (Fig. 2). His parents were informed about the root anomaly and our patient was kept under careful observation to evaluate proper eruption of unerupted permanent lateral incisors (Table 1).

The arrows in the figure indicate (a) Orthopantomogram (OPG) showing Bilateral Birooted primary maxillary canines. (b) Periapical radiograph showing the presence of two roots in primary right maxillary canine. (c) Periapical radiograph showing the presence of two roots in primary left maxillary canine

a Primary right maxillary canine showing two separate roots (mesial and distal). b Primary left maxillary canine showing two roots (mesial and distal) which are connected
Discussion and conclusion
A bi-rooted primary canine is an extremely rare dental anomaly with high prevalence in maxilla rather than in the mandible and it occurs more frequently in male children. To the best of our knowledge, this is the first reported case in an Arab child. A list of cases with bi-rooted primary maxillary canine from all over the world is presented in Table 2. The diagnosis and identification of tooth morphology are the main factors for an appropriate plan of treatment. A primary radiograph is significant as it helps in the identification or uncertainties of anatomical variations. Bifurcations in the roots can be seen when the X-ray has no superimposition of images [23]. In the present case, the two roots were evident in a radiograph. However, this may sometimes be difficult due to crowding of teeth. Hence, radiographic images must be cautiously analyzed to infer and recognize particulars that might propose the presence of bifurcations [24].
The standard morphology of the primary canine includes a slender, long, and tapering root which is double the size (in length) of the crown. It has been explained that during normal root formation, at the dental organ’s cervical loop, the outer and the inner enamel epithelia multiply in the form of a double layer of cells called Hertwig’s epithelial root sheath. The inner and outer epithelia of enamel turn at the future cementoenamel junction, producing the epithelial diaphragm. The primary apical foramen is enclosed by the rim of this sheath. An unknown aspect in multi-rooted teeth stimulates continued morphodifferentiation. Tongue-like extensions of the horizontal diaphragm grow and extend toward each other, and fuse by differential growth. For every new secondary apical foramen, a root will be developed [25].
Although trauma and other disturbances may affect morphodifferentiation, improved expression of the gene starting the differential growth of Hertwig’s epithelial root sheath or a defect in the dental lamina through the initial stage of formation of the root is thought to develop double roots [20]. In the present case, the presence of two roots in primary canines bilaterally cannot be attributed to a specific cause. Hence, when an anomaly like this happens, difficulty during exfoliation or extraction may happen. The permanent canine has to reabsorb both the roots of the primary canine evenly to facilitate its normal eruption. During extraction, the clinician should confirm that the crown of the underlying permanent tooth is not trapped in order to prevent accidental removal of the underlying developing permanent tooth bud.
In conclusion, clinicians should consider all the possible tooth variations during routine intra-oral and radiographic examinations to facilitate a better treatment outcome and to avoid unwanted complications. Also, the presence of two roots in primary canines bilaterally cannot be attributed to a specific cause in the present report and further studies are needed for the proper treatment of this anomaly.
Availability of data and materials
Data sharing does not apply to this article as no datasets were generated or analyzed during the current study.
References
Talebi M, Parisay I, Khorakian F, Bagherian M. Bi-rooted primary maxillary canines: A case report. J Dent Res Dent Clin Dent Prospects. 2010;4(3):101.
Brown CK. Bilateral bifurcation of the maxillary deciduous cuspids. Oral Surg Oral Med Oral Pathol Oral Radiol. 1975;40(6):817.
Saravia ME. Bilateral birooted maxillary primary canines: report of two cases. ASDC J Dent Child. 1991;58(2):154–5.
Kelly JR. Birooted primary canines. Oral Surg Oral Med Oral Pathol Oral Radiol. 1978;46(6):872.
Takano H. Supernumerary rooted primary mandibular right canine. Shika Geppo. 1941;21:48–50.
Kurosu K, Hattori R, Sugiyama J. Anomalies of the deciduous teeth. Shikai Tenbo. 1968;31:505–17.
Yasunaga M, Tagashira N, Miura K, Inoue T. A case report; bilateral bifurcation of the maxillary and mandibular deciduous cuspids. Japanese J Pediatr Dent. 1987;16:224–9.
Hata Y, Itoh T, Nishimura Y, Uchida N, Mamiya M. An interesting case of lower bilateral bifurcarcated root canines in deciduous dentition. Kanagawa Shigaku. 1979;14:177–83.
Krolls SO, Donahue AH. Double-rooted maxillary primary canines. Oral Surg Oral Med Oral Pathol. 1980;49:379.
Chow MH. Bilateral double-rooted maxillary primary canines an abbreviated case report. Oral Surg Oral Med Oral Pathol. 1980;50:219.
Bryant RHJ, Bowers DF. Four birooted primary canines: report of case. ASDC J Dent Child. 1982;49:441–2.
Bimstein E, Bystrom EB. Birooted bilateral maxillary primary canines. ASDC J Dent Child. 1982;49:217–8.
Paulson RB, Gottlieb LJ, Sciulli PW, Schneider KN. Double-rooted maxillary primary canines. ASDC J Dent Child. 1985;52:195–8.
Jones JE, Hazelrigg CO. Birooted primary canines. Oral Surg Oral Med Oral Pathol. 1987;63:499–500.
Hayutin DJ, Ralstrom CS. Primary maxillary bilateral birooted canines: Report of two cases. ASDC J Dent Child. 1992;59:235–7.
Ott NW, Ball RN. Birooted primary canines: report of three cases. Pediatr Dent. 1996;18:328–30.
Winkler MP, Ahmad R. Multirooted anomalies in the primary dentition of Native Americans. J Am Dent Assoc. 1997;128:1009–11.
Mochizuki K, Ohtawa Y, Kubo S, Machida Y, Yakushiji M. Bifurcation, birooted primary canines: a case report. Int J Paediatr Dent. 2001;11:380–1.
Atac AS, Cetinguc A. Primary maxillary bi-lateral birooted canines: Report of two cases. Hacettepe Dishekimligi Fa-KultesiDergisi. 2005;29:24–8.
Orhan AI, Sari S. Double-rooted primary canines: A report of three cases. J Indian Soc Pedod Prev Dent. 2006;24(4):204.
Dhanpal PK, King NM. Bilateral bimaxillary bi-rooted primary canines: report of a case. J Clin Pediatr Dent. 2009;34(1):113–16.
Guler C. Inonu Universitesi Saglik Bilimleri Dergisi. 2012;2:57–9.
Shanna R, Pécora JD, Lumley PJ, Walmsley AD. The external and internal anatomy of human mandibular canine teeth with two roots. Dent Traumatol. 1998;14(2):88–92.
Victorino FR, Bernardes RA, Baldi JV, Moraes IG, Bernardinelli N, Garcia RB, Bramante CM. Bilateral mandibular canines with two roots and two separate canals: case report. Braz Dent J. 2009;20(1):84–6.
Ten Cate AR. Oral Histology: Development, Structure and Function. 2nd ed. St. Louis: CV Mosby Co; 1985. p. 69–72.
Acknowledgements
Not applicable.
Funding
None to declare.
Author information
Authors and Affiliations
Contributions
AA was involved in the diagnosis, clinical management, and treatment of the patient and also drafted the final manuscript. The author read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
No ethical committee approval is required for the case report.
Consent for publication
Written informed consent was obtained from the patient’s parents for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The author declares that he has no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Assiry, A. Bi-rooted primary maxillary canines: a case report. J Med Case Reports 13, 261 (2019). https://doi.org/10.1186/s13256-019-2174-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13256-019-2174-9