
Abstract
Objectives
To develop and compare noninvasive models for differentiating between combined hepatocellular-cholangiocarcinoma (cHCC-CCA) and HCC based on serum tumor markers, contrast-enhanced ultrasound (CEUS), and computed tomography (CECT).
Methods
From January 2010 to December 2021, patients with pathologically confirmed cHCC-CCA or HCC who underwent both preoperative CEUS and CECT were retrospectively enrolled. Propensity scores were calculated to match cHCC-CCA and HCC patients with a near-neighbor ratio of 1:2. Two predicted models, a CEUS-predominant (CEUS features plus tumor markers) and a CECT-predominant model (CECT features plus tumor markers), were constructed using logistic regression analyses. Model performance was evaluated by the area under the curve (AUC), sensitivity, specificity, and accuracy.
Results
A total of 135 patients (mean age, 51.3 years ± 10.9; 122 men) with 135 tumors (45 cHCC-CCA and 90 HCC) were included. By logistic regression analysis, unclear boundary in the intratumoral nonenhanced area, partial washout on CEUS, CA 19-9 > 100 U/mL, lack of cirrhosis, incomplete tumor capsule, and nonrim arterial phase hyperenhancement (APHE) volume < 50% on CECT were independent factors for a diagnosis of cHCC-CCA. The CECT-predominant model showed almost perfect sensitivity for cHCC-CCA, unlike the CEUS-predominant model (93.3% vs. 55.6%, p < 0.001). The CEUS-predominant model showed higher diagnostic specificity than the CECT-predominant model (80.0% vs. 63.3%; p = 0.020), especially in the ≤ 5 cm subgroup (92.0% vs. 70.0%; p = 0.013).
Conclusions
The CECT-predominant model provides higher diagnostic sensitivity than the CEUS-predominant model for CHCC-CCA. Combining CECT features with serum CA 19-9 > 100 U/mL shows excellent sensitivity.
Critical relevance statement
Combining lack of cirrhosis, incomplete tumor capsule, and nonrim arterial phase hyperenhancement (APHE) volume < 50% on CECT with serum CA 19-9 > 100 U/mL shows excellent sensitivity in differentiating cHCC-CCA from HCC.
Key points
1. Accurate differentiation between cHCC-CCA and HCC is essential for treatment decisions.
2. The CECT-predominant model provides higher accuracy than the CEUS-predominant model for CHCC-CCA.
3. Combining CECT features and CA 19-9 levels shows a sensitivity of 93.3% in diagnosing cHCC-CCA.
Graphical Abstract

Similar content being viewed by others
Introduction
Combined hepatocellular-cholangiocarcinoma (cHCC-CCA) accounts for 0.4–4.2% of primary liver cancer cases and demonstrates hepatocytic and biliary differentiation in the same tumor [1]. In routine practice, a marked overlap in clinical conditions has been observed between cHCC-CCA and hepatocellular carcinoma (HCC) [2, 3].
However, the treatment strategies for cHCC-CCA and HCC differ. For example, liver transplantation has been accepted as an effective curative-intent treatment option for HCC, but it is not recommended for cHCC-CCA because of frequent recurrence (54% at 5 years) and suboptimal long-term survival (41% at 5 years) [4,5,6]. Lymph node dissection is recommended for resectable cHCC-CCA, while it is not routinely performed for HCC [1, 7]. Local treatment and systematic therapy are established treatment options for unresectable HCCs [8, 9], but whether they have therapeutic benefits for unresectable cHCC-CCAs is controversial [6, 10]. Thus, the accurate differential diagnosis between cHCC-CCA and HCC is critical for appropriate therapeutic decision-making.
Contrast-enhanced ultrasound (CEUS) and contrast-enhanced computed tomography (CECT) are two of the main imaging modalities for diagnosing liver tumors [11, 12], and each of these modalities has different imaging principles and advantages. CEUS is performed with pure blood contrast and can continuously evaluate macro- and microvascular perfusion within tumors [13]. CECT uses a small molecule contrast agent that can assess the entire liver during a standard examination and has demonstrated clear advantages over CEUS in detecting tumors and extrahepatic lymph metastases [14]. Previous studies have explored the potential of combining laboratory results with CEUS or CECT for differentiating cHCC-CCA from HCC but have yielded suboptimal diagnostic performances (sensitivity for cHCC-CCA: 32.5 to 74.4%) [2, 15,16,17,18]. No studies have compared the diagnostic efficacy of CEUS and CECT in differentiating cHCC-CCA from HCC. It is also uncertain which imaging examination is best for diagnosing probable HCC/cHCC-CCA in high-risk patients.
Here, we aimed to develop diagnostic models integrating clinical and readily accessible CEUS and CECT features to differentiate between cHCC-CCA and HCC in a propensity score-matched study and to compare the two models.
Patients and methods
Patients
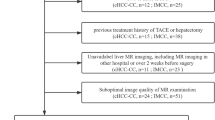
From January 2010 to December 2021, patients who underwent curative-intent liver resection for surgically proven HCC or cHCC-CCA were consecutively enrolled. The inclusion criteria were as follows: (a) pathologically proven HCC or cHCC-CCA, (b) both CECT and CEUS examinations within 1 month before surgery, and (c) chronic hepatitis B/C virus infection or cirrhosis. Patients were excluded if (a) they had received any prior antitumoral treatment, (b) key laboratory data were not available, or (c) CECT and/or CEUS images were degraded or missing. The inclusion and exclusion flowchart is shown in Fig. 1.

Flowchart of included patients. cHCC-CCA, combined hepatocellular-cholangiocarcinoma; HCC, hepatocellular carcinoma; CEUS, contrast-enhanced ultrasound; CECT, contrast-enhanced computed tomography
Imaging acquisition
The imaging acquisition recommendation and the detailed parameters are presented in eMethods 1 in Supplement 1.
Imaging analysis
All image analyses were conducted on a per-lesion basis by two ultrasonographers (K-Y.Z. and J-Y.H., with 8 and 10 years of experience in CEUS images, respectively) and two radiologists (Y.Z. and Y-D.C., with 8 and 11 years of experience in liver imaging in CECT images, respectively). All disagreements between the reviewers regarding the imaging features were resolved by consensus. For patients with multiple lesions, the largest targeted lesion was selected for feature-related analyses.
CEUS
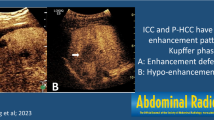
The CEUS imaging features and LI-RADS categories according to ACR CEUS LI-RADS version 2017 [19], along with tumor size, number, cirrhosis, enhanced level in the arterial phase/portal venous phase/late phase (AP/PVP/LP), etc., were evaluated. The following non-LI-RADS imaging features that have been associated with cHCC-CCA or HCC were also evaluated: (a) tumor supply artery: present vs. absent [20, 21]; (b) circumscribed enhancement: poor vs. good [20, 21]; (c) the boundary in the intratumoral nonenhanced area: clear vs. unclear [21]; (d) the proportion of washout: partial vs. complete; and (e) intratumoral vein: present vs. absent [21,22,23]. The detailed definitions of the imaging features are presented in eMethods 2 in Supplement 1 and typical cases are shown in Fig. 2a.

The definition of the partial imaging features of the lesions on CEUS (a) and CECT (b)
CECT
The CECT imaging features and LI-RADS categories according to ACR CECT LI-RADS version 2018 [24], along with tumor size and number, were evaluated. The following non-LI-RADS imaging features that have been associated with cHCC-CCA or HCC were also evaluated: (a) cirrhosis: present vs. absent [25]; (b) semiquantitative characteristics for quantifying hypervascular components, including the nonrim arterial phase hyperenhancement (APHE) volume ratio (< 50% vs. ≥ 50%) and nonperipheral washout volume ratio (< 50% vs. ≥ 50%); (c) tumor capsule integrity: complete vs. incomplete [7]; (d) tumor margin: smooth vs. nonsmooth [26]; and (e) tumor growth subtype (Eggel’s growth classification as assumed on CT): type 1 (single nodular type), type 2 (single nodular type with extranodular growth), and type 3 (multiple confluent nodules) [27]. The detailed definitions of the imaging features are presented in eMethods 2 in Supplement 1 and typical cases are shown in Fig. 2b.
Histopathology analysis
The pathological characteristics of the lesions were retrospectively recorded according to the pathological reporting system in our hospital. These included the maximum size of the main lesion (the largest lesion in the case of multiple lesions), the Edmondson-Steiner grade of the HCC, and the HCC/intrahepatic cholangiocarcinoma (ICC)-predominant components of cHCC-CCA [28].
Statistical analysis
Propensity score-matching was performed to minimize the effect of potential selection bias and confounding factors between patients with HCC and cHCC-CCA.
The predictive models, based separately on tumor markers and CEUS and CECT features, were constructed using logistic regression analyses, and their performance was compared with that of pathology. The variables with p < 0.05 by the χ2 test or Fisher’s exact test were entered into the univariate logistic analysis, and the multicollinearity between the univariate variables was assessed using Spearman’s correlation analysis and by computing the variance inflation factor (VIF). If the absolute value of the correlation coefficient (ACC) was ≥ 0.6 or the VIF was > 10 between two variables, the variable with the higher odds ratio (OR) were selected for multivariate logistic analysis. Therefore, all independent variables that were associated with cHCC-CCA in univariate analyses were input into a multivariate logistic regression model using the backward stepwise method while adjusting for the same covariates as above. The diagnostic models were illustrated as nomograms based on their correlation coefficients in the multivariate logistic analysis.
Model discrimination was assessed by computing the area under the receiver operating characteristic curve (AUC) value and compared using the DeLong test. Model calibration was evaluated by the Hosmer–Lemeshow (H-L) test and calibration curves. The McNemar test was used to compare pairwise sensitivities, specificities, and accuracies of the two diagnostic models. The subgroup comparison of the diagnostic efficacy between CEUS and CECT was also evaluated for smaller lesions, with a diameter of 5 cm.
All statistical analyses were performed with the R software (R Foundation for Statistical Computing, version 3.2.5, http://www.r-project.org/) and MedCalc (version 10.4). A two-tailed adjusted p < 0.05 was statistically significant.
Results
Patients
A total of 971 patients were initially identified. After propensity score matching, 135 patients (mean age, 51.3 ± 10.9 years, 122 males [90.4%]) with 135 nodules (45 cHCC-CCAs and 90 HCCs) were included for further analysis.
Serum CA 19-9 > 100 U/mL was more frequently found in patients with cHCC-CCA than in those with HCC (11.1% vs. 2.2%, p = 0.029), while serum AFP > 400 μg/L was more frequently observed in patients with HCC than in those with cHCC-CCA (36.7% vs. 20.0%, p = 0.050). The key clinical features of the patients are summarized in Table 1.
Imaging features and interrater agreement
Based on the CEUS LI-RADS classification, 46.6% and 37.8% of cHCC-CCA patients were classified as LR-4/5 and LR-M, respectively; for HCC, 65.6% and 20% were classified as LR-4/5 and LR-M, respectively. Based on the CECT LI-RADS classification, 44.5% and 51.1% of cHCC-CCA patients were classified as LR-4/5 and LR-M, respectively, compared with 76.7% for LR-4/5 and 12.2% for LR-M among the HCC patients.
On CEUS, the following features were more frequent in patients with cHCC-CCA than in those with HCC: hypoenhancement in the PVP images (88.9% vs. 64.4%), unclear boundary in the intratumoral nonenhanced area (71.1% vs. 37.8%), and partial washout (71.1% vs. 40.0%). The baseline CEUS imaging features of all lesions are presented in Table 2.
On CECT, the following features were more commonly observed in cHCC-CCA: nonrim APHE volume < 50% (57.8% vs. 12.2%), rim APHE (37.8% vs. 5.6%), nonperipheral washout volume < 50% (48.9% vs. 20.0%), peripheral washout (48.9% vs. 8.9%), LR-M category (51.1% vs. 12.2%), and incomplete tumor capsule (60.0% vs. 40.0%). The following features were more frequently detected for HCC: cirrhosis (68.9% vs. 44.4%) and single nodular type (tumor growth subtype 1) (68.9% vs. 51.1%). The baseline CECT imaging features of all lesions are presented in Table 3.
Cohen’s kappa values ranged from 0.312 to 0.765 for CEUS and from 0.380 to 0.717 for CECT. The interrater agreement of imaging features on CEUS and CECT are summarized in eTable 3 in Supplement 1.
The efficiency of the imaging models for cHCC-CCA
The CEUS-predominant model
The CEUS-predominant model was developed by combining CEUS features and tumor markers (AFP > 400 μg/L and CA 19-9 > 100 U/mL). The univariate variable selection is presented in eMethods 3 in Supplement 1. By multivariate regression analysis, unclear boundary in the intratumoral nonenhanced area (OR = 2.765; 95% confidence interval [CI]: 1.209, 6.541; p = 0.018) and partial washout (OR = 2.607; 95% CI: 1.152, 6.079; p = 0.023) were independent factors for a diagnosis of cHCC-CCA (shown in Table 4). The AUC value of the prediction model was 0.720 (95% CI: 0.632, 0.808). The sensitivity, specificity, and accuracy were 55.6%, 80.0%, and 71.9%, respectively. Regression coefficient-based nomograms were constructed based on the CEUS-predominant model (Fig. 3a). The calibration curve of the nomogram for the probability of cHCC-CCA demonstrated good agreement between prediction and observation (eFigure 1a). The H-L test yielded a nonsignificant statistic (p = 1.000).

Nomograms of the CEUS-predominant (a) and CECT-predominant models (b)
The CECT-predominant model
The CECT-predominant model was developed by combining CECT features and tumor markers. The univariate variable selection is presented in eMethods 3 in Supplement 1. On multivariate regression analysis, CA 19-9 > 100 U/mL (OR = 8.573; 95% CI: 1.217, 82.845; p = 0.038), cirrhosis (OR = 0.308; 95% CI: 0.113, 0.795; p = 0.017), incomplete tumor capsule (OR = 7.348; 95% CI: 2.394, 25.929; p < 0.001), and nonrim APHE volume < 50% (OR = 11.180; 95% CI, 3.475, 41.419; p < 0.001) were found to be independent factors for diagnosing cHCC-CCA (shown in Table 4). The AUC value of the prediction model was 0.874 (95% CI: 0.816, 0.931), with a sensitivity, specificity, and accuracy of 93.3%, 63.3%, and 73.3%, respectively. A regression coefficient-based nomogram was constructed based on the CECT-predominant model (Fig. 3b). The calibration curve of the nomogram for the probability of cHCC-CCA demonstrated good agreement between prediction and observation (eFigure 1b). The H-L test yielded a nonsignificant statistic (p > 0.05).
Comparison between the imaging models
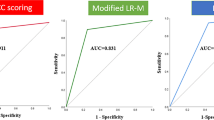
The diagnostic performance was compared between the CEUS-predominant model and the CECT-predominant model (shown in Table 5 and Fig. 4). The CECT-predominant model had a higher diagnostic sensitivity (93.3%) than the CEUS-predominant model (55.6%; p < 0.001) but a lower diagnostic specificity (CECT vs. CEUS: 63.3% vs. 80.0%; p = 0.020). The two models had comparable diagnostic accuracy (CECT vs. CEUS: 73.3% vs. 71.9%; p = 0.583). In addition, we compared the AUC values between the models and found that the AUC value of the CECT-predominant model (AUCCECT = 0.874, 95% CI: 0.816, 0.931) was higher than that of the CEUS-predominant model (AUCCEUS = 0.720, 95% CI: 0.632, 0.808; p = 0.001, Fig. 5).

CEUS and CECT images of a 56-year-old man with chronic hepatitis B and CA 19-9 < 100 U/mL. A 7.3-cm mass was detected in segment IV of the liver (A). A hypoechoic mass with poor boundary on conventional ultrasound (A, a); on CEUS, the mass showed hyperenhancement, a nonsmooth tumor margin (stars), and tumor supply artery (arrowhead) at 18 s (A, b); in the late phase (179 s), the hyperenhanced area in the arterial phase of mass exhibited partial washout with partial isoenhancement (stars) and partial hypoenhancement area (arrowhead, A, c). Based on these features, the likelihood of this mass being diagnosed as cHCC-CCA was smaller than 30% according to the CEUS-predominant model (B). There was no obvious cirrhotic liver background, and the mass showed low density on abdominal CT image (A, d), rim enhancement and < 50% nonrim enhancement (mainly the right posterior part of the lesion, arrow) in the arterial phase (A, e), “washout” absence, nonsmooth tumor margin, and a thin incomplete enhanced capsule (arrow) seen in the portal venous phase (A, f). Based on these features, the likelihood of this mass being diagnosed as cHCC-CCA was higher than 90.0% according to the CECT-predominant model (C). The mass was pathologically proven to be combined hepatocellular-cholangiocarcinoma

The diagnostic performance of the CEUS-predominant and CECT-predominant models was assessed through ROC curve and AUC analyses
Subgroup analysis for the CEUS-predominant and CECT-predominant models
For the smaller nodules (≤ 5 cm, based on the pathology results) group, the CECT-predominant model had higher diagnostic sensitivity for cHCC-CCA than the CEUS-predominant model (88.5% vs. 50.0%; p = 0.006), while the CEUS-predominant model presented better diagnostic specificity than the CECT-predominant model (92.0% vs. 70.0%; p = 0.013). The two models showed comparable diagnostic performance in differentiating cHCC-CCA from HCC (AUCCECT = 0.792 vs. AUCCEUS = 0.710; p = 0.226, shown in eFigure 2a). In the > 5 cm subgroup, the CECT-predominant model had perfect diagnostic sensitivity for cHCC-CCA (100% vs. 63.2% of the CEUS-predominant model; p = 0.016). Its ROC curve is shown in eFigure 2b. The detailed diagnostic performance is shown in Table 5.
Discussion
Combining tumor biomarkers and imaging features is critical in diagnosing cHCC-CCA due to its overlapping features with HCC. This propensity score-matched study found that approximately 44.4% of cHCC-CCAs on CEUS and 26.7% of cHCC-CCAs on CECT were evaluated as LR-5, which can easily mimic HCC. Therefore, we constructed and compared two imaging-predominant diagnostic models based on clinical data and nodule features on CEUS and CECT imaging to identify cHCC-CCA. The results indicated that the CECT-predominant model exhibited nearly perfect diagnostic sensitivity (93.3%), which was significantly higher than that of the CEUS-predominant model (55.6%; p < 0.001). On the other hand, the CEUS-predominant model demonstrated commendable diagnostic specificity, particularly for lesions smaller than 5 cm (92.0% vs. 70.0%; p = 0.013).
Cirrhosis detected by CECT is highly suggestive of HCC. In this study, we found that few at-risk patients with cHCC-CCA had a cirrhotic liver background due to the different origins of HCC and cHCC-CCA, which is similar to the findings of the latest studies [24, 29,30,31]. Additionally, this study revealed that cHCC-CCA patients exhibited higher rates of nonrim APHE with a volume < 50%. This finding is congruent with a previous study that reported a larger HCC component (p = 0.014) and a smaller ICC component (p = 0.001) in the hypervascular group of cHCC-CCA patients during pathological analysis [32]. In addition, capsular enhancement is usually considered a major imaging feature of HCC [24, 33]. In the present study, we observed a higher frequency of incomplete tumor capsules in cHCC-CCA than in HCCs. Similar to the observation of “unclear boundaries” on CEUS, the presence of an incomplete capsule is likely associated with infiltrative tumor growth of the ICC portion in cHCC-CCA [15, 34]. Interestingly, ten out of 12 cHCC-CCAs, classified as LR-5 based on CECT LI-RADS classification, were indeed reclassified as cHCC-CCA based on the CECT-predominant model in this study, which may help improve the diagnostic specificity of LR-5 for HCC in future clinical practice.
On CEUS images, the presence of unclear boundaries in the intratumoral nonenhanced areas was an independent risk factor for cHCC-CCA. This might be elucidated by the fibrotic pathological findings (relying on the ICC component), similar to previous findings [21, 35]. The presence of washout on CEUS with SonoVue reflects the intratumoral vascular supply. Therefore, ICCs often present earlier and with more complete washout compared to HCCs [36]. Consequently, partial washout could frequently be observed in cHCC-CCA lesions that contain both HCC and ICC components. Notably, tumor differentiation is correlated with the presence of washout, as demonstrated by the findings of Iavarone et al. [37]. This study also observed that grade 2–3 HCCs exhibited higher rates of partial washout than lower grade HCCs (grade 1 or 2) (19/37 vs. 17/52; p = 0.079). This finding might provide valuable prognostic information for future studies in this field.
Several studies have evaluated the performance of imaging characteristics in differentiating cHCC-CCA and HCC in recent years [15, 18, 31, 38, 39]. The model developed in this study, which combined CECT features and CA 19-9 levels to distinguish cHCC-CCA, was put into a visual form as a nomogram and demonstrated a remarkable sensitivity of 93.3%, showing better performance than previous ones (ranging from 40 to 73.8% [15, 18, 38]. We hope that our findings can offer valuable guidance in two aspects. First, the remarkably high sensitivity for cHCC-CCA could effectively diagnose lesions that do not support a definite diagnosis of HCC, which might improve the diagnostic specificity of HCC in routine clinical practice. In addition, the CECT-predominant model exhibited a low specificity of 63.3%, which could lead to misdiagnosis or underdiagnosis of a higher number of HCC cases, which would limit the therapeutic options for HCC (e.g., liver transplantation). Given this, adding CEUS to CECT could improve the overall diagnostic accuracy, especially for lesions less than 5 cm.
Some limitations of this study should be mentioned. First, there was an unavoidable selection bias due to the single-center retrospective nature of the study, although we used PSM to lessen this bias. Second, no validation data were available to test and refine our models due to the limited size of the cHCC-CCA population. Third, we did not include ICC patients in this differential diagnostic study due to the limited number of ICC patients with HCC risk factors. Finally, the results of this study were based on a case-control design rather than a cohort design, which might not reflect real-world clinical epidemiological conditions. Therefore, large-scale multicenter studies are warranted to validate our findings.
Conclusions
The CECT-predominant model provides higher diagnostic sensitivity compared to the CEUS-predominant model for cHCC-CCA. Combining the CECT features with serum CA 19-9 > 100 U/mL showed excellent diagnostic sensitivity in differentiating cHCC-CCA from HCC, while the CEUS features could enhance diagnostic specificity, especially in the ≤ 5 cm subgroup.
Availability of data and materials
The datasets used or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- AFP:
-
Alpha-fetoprotein
- APHE:
-
Arterial phase hyperenhancement
- CA 19-9:
-
Carbohydrate antigen 19-9
- CECT:
-
Contrast-enhanced computed tomography
- CEUS:
-
Contrast-enhanced ultrasound
- cHCC-CCA:
-
Combined hepatocellular-cholangiocarcinoma
- CI:
-
Confidence interval
- HBV:
-
Hepatitis B virus
- HCC:
-
Hepatocellular carcinoma
- HCV:
-
Hepatitis C virus
- LI-RADS:
-
Liver Imaging Reporting and Data System
- LR:
-
Liver Imaging Reporting and Data System category
- OR:
-
Odds ratio
- PSM:
-
Propensity score matching
- PVP:
-
Portal venous phase
- TIV:
-
Tumor in vein
References
Beaufrère A, Calderaro J, Paradis V (2021) Combined hepatocellular-cholangiocarcinoma: an update. J Hepatol 74:1212–1224. https://doi.org/10.1016/j.jhep.2021.01.035
Ye J, Xie X, Liu B et al (2017) Imaging features on contrast-enhanced ultrasound and clinical characteristics of hepatitis B virus-related combined hepatocellular-cholangiocarcinoma: comparison with hepatitis B virus-related hepatocellular carcinoma. Ultrasound Med Biol 43:2530–2536. https://doi.org/10.1016/j.ultrasmedbio.2017.07.016
Sagrini E, Iavarone M, Stefanini F et al (2019) Imaging of combined hepatocellular-cholangiocarcinoma in cirrhosis and risk of false diagnosis of hepatocellular carcinoma. United European Gastroenterol J 7:69–77. https://doi.org/10.1177/2050640618815378
Li DB, Si XY, Wang SJ et al (2019) Long-term outcomes of combined hepatocellular-cholangiocarcinoma after hepatectomy or liver transplantation: a systematic review and meta-analysis. Hepatobiliary Pancreat Dis Int 18:12–18. https://doi.org/10.1016/j.hbpd.2018.10.001
Reig M, Forner A, Rimola J et al (2022) BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol 76:681–693. https://doi.org/10.1016/j.jhep.2021.11.018
Kim EJ, Yoo C, Kang HJ et al (2021) Clinical outcomes of systemic therapy in patients with unresectable or metastatic combined hepatocellular-cholangiocarcinoma. Liver Int 41:1398–1408. https://doi.org/10.1111/liv.14813
Kim H, Park MS, Choi JY et al (2009) Can microvessel invasion of hepatocellular carcinoma be predicted by pre-operative MRI? Eur Radiol 19:1744–1751. https://doi.org/10.1007/s00330-009-1331-8
Na SK, Choi GH, Lee HC et al (2018) The effectiveness of transarterial chemoembolization in recurrent hepatocellular-cholangiocarcinoma after resection. PLoS One 13:e0198138. https://doi.org/10.1371/journal.pone.0198138
Yau T, Park J-W, Finn RS et al (2022) Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol 23:77–90. https://doi.org/10.1016/S1470-2045(21)00604-5
Trikalinos NA, Zhou A, Doyle MBM et al (2018) Systemic therapy for combined hepatocellular-cholangiocarcinoma: a single-institution experience. J Natl Compr Canc Netw 16:1193–1199. https://doi.org/10.6004/jnccn.2018.7053
General Office of National Health Commission (2022) Standard for diagnosis and treatment of primary liver cancer (2022 edition). J Clin Hepatol 38:306–321 https://kns.cnki.net/kcms/detail/22.1108.R.20220130.1411.002.html
Marrero JA, Kulik LM, Sirlin CB et al (2018) Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology 68:723–750. https://doi.org/10.1002/hep.29913
Claudon M, Dietrich CF, Choi BI et al (2013) Guidelines and good clinical practice recommendations for Contrast Enhanced Ultrasound (CEUS) in the liver - update 2012: a WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultrasound Med Biol 39:187–210. https://doi.org/10.1016/j.ultrasmedbio.2012.09.002
Ayuso C, Rimola J, Vilana R et al (2018) Diagnosis and staging of hepatocellular carcinoma (HCC): current guidelines. Eur J Radiol 101:72–81. https://doi.org/10.1016/j.ejrad.2018.01.025
Yang JZY, Li JW, Shi YY et al (2020) Contrast-enhanced ultrasound in association with serum biomarkers for differentiating combined hepatocellular-cholangiocarcinoma from hepatocellular carcinoma and intrahepatic cholangiocarcinoma. World J Gastroenterol 24:7325–7337. https://doi.org/10.3748/wjg.v26.i46.7325
Huang XWHY, Chen LD, Wang Z et al (2018) Potential diagnostic performance of contrast-enhanced ultrasound and tumor markers in differentiating combined hepatocellular-cholangiocarcinoma from hepatocellular carcinoma and cholangiocarcinoma. J Med Ultrason 45:231–241. https://doi.org/10.1007/s10396-017-0834-1
Zhang HCZT, Hu RF, Wu L (2020) Contrast-enhanced ultrasound imaging features and clinical characteristics of combined hepatocellular cholangiocarcinoma: comparison with hepatocellular carcinoma and cholangiocarcinoma. Ultrasonography 4:356–366. https://doi.org/10.14366/usg.19093
Zhou Y, Yin S, Zhao L et al (2022) CEUS and CT/MRI LI-RADS in association with serum biomarkers for differentiation of combined hepatocellular-cholangiocarcinoma from hepatocellular carcinoma. Front Oncol 12:897090. https://doi.org/10.3389/fonc.2022.897090
Lyshchik A, Kono Y, Dietrich CF et al (2018) Contrast-enhanced ultrasound of the liver: technical and lexicon recommendations from the ACR CEUS LI-RADS working group. Abdom Radiol (NY) 43:861–879. https://doi.org/10.1007/s00261-017-1392-0
Catalano O, Nunziata A, Lobianco R et al (2005) Real-time harmonic contrast material-specific US of focal liver lesions. Radiographics 25:333–349
Chen LD, Ruan SM, Lin Y et al (2019) Comparison between M-score and LR-M in the reporting system of contrast-enhanced ultrasound LI-RADS. Eur Radiol 29:4249–4257. https://doi.org/10.1007/s00330-018-5927-8
Chen L-D, Xu H-X, Xie X-Y et al (2010) Intrahepatic cholangiocarcinoma and hepatocellular carcinoma: differential diagnosis with contrast-enhanced ultrasound. Eur Radiol 20:743–753. https://doi.org/10.1007/s00330-009-1599-8
Xu H-X, Lu M-D, Liu G-J et al (2006) Imaging of peripheral cholangiocarcinoma with low-mechanical index contrast-enhanced sonography and SonoVue: initial experience. J Ultrasound Med 25:23–33
Chernyak V, Fowler KJ, Kamaya A et al (2018) Liver Imaging Reporting and Data System (LI-RADS) Version 2018: imaging of hepatocellular carcinoma in at-risk patients. Radiology 289:816–830. https://doi.org/10.1148/radiol.2018181494
Dodd GD, Baron RL, Oliver JH et al (1999) Spectrum of imaging findings of the liver in end-stage cirrhosis: part I, gross morphology and diffuse abnormalities. AJR Am J Roentgenol 173:1031–1036
Ariizumi S, Kitagawa K, Kotera Y et al (2011) A non-smooth tumor margin in the hepatobiliary phase of gadoxetic acid disodium (Gd-EOB-DTPA)-enhanced magnetic resonance imaging predicts microscopic portal vein invasion, intrahepatic metastasis, and early recurrence after hepatectomy in patients with hepatocellular carcinoma. J Hepatobiliary Pancreat Sci 18:575–585. https://doi.org/10.1007/s00534-010-0369-y
Hui AM, Takayama T, Sano K et al (2000) Predictive value of gross classification of hepatocellular carcinoma on recurrence and survival after hepatectomy. J Hepatol 33:975–979. https://doi.org/10.1016/s0168-8278(00)80131-2
Cong WM, Bu H, Chen J et al (2016) Practice guidelines for the pathological diagnosis of primary liver cancer: 2015 update. World J Gastroenterol 22:9279–9287. https://doi.org/10.3748/wjg.v22.i42.9279
Yeh MM (2010) Pathology of combined hepatocellular-cholangiocarcinoma. J Gastroenterol Hepatol 25:1485–1492. https://doi.org/10.1111/j.1440-1746.2010.06430.x
Kono Y, Lyshchik A, Cosgrove D et al (2017) Contrast Enhanced Ultrasound (CEUS) Liver Imaging Reporting and Data System (LI-RADS®): the official version by the American College of Radiology (ACR). Ultraschall Med 38:85–86. https://doi.org/10.1055/s-0042-124369
Lu L, Zhang C, Yu X et al (2022) The value of contrast-enhanced magnetic resonance imaging enhancement in the differential diagnosis of hepatocellular carcinoma and combined hepatocellular cholangiocarinoma. J Oncol 2022:4691172. https://doi.org/10.1155/2022/4691172
Park SH, Lee SS, Yu E et al (2017) Combined hepatocellular-cholangiocarcinoma: gadoxetic acid-enhanced MRI findings correlated with pathologic features and prognosis. J Magn Reson Imaging 46:267–280. https://doi.org/10.1002/jmri.25568
International Consensus Group for Hepatocellular NeoplasiaThe International Consensus Group for Hepatocellular N (2009) Pathologic diagnosis of early hepatocellular carcinoma: a report of the international consensus group for hepatocellular neoplasia. Hepatology 49:658–664. https://doi.org/10.1002/hep.22709
Kim TH, Kim H, Joo I et al (2020) Combined hepatocellular-cholangiocarcinoma: changes in the 2019 World Health Organization histological classification system and potential impact on imaging-based diagnosis. Korean J Radiol 21:1115–1125. https://doi.org/10.3348/kjr.2020.0091
Xu HX, Chen LD, Liu LN et al (2012) Contrast-enhanced ultrasound of intrahepatic cholangiocarcinoma: correlation with pathological examination. Br J Radiol 85:1029–1037. https://doi.org/10.1259/bjr/21653786
Wildner D, Bernatik T, Greis C et al (2015) CEUS in hepatocellular carcinoma and intrahepatic cholangiocellular carcinoma in 320 patients - early or late washout matters: a subanalysis of the DEGUM multicenter trial. Ultraschall Med 36:132–139. https://doi.org/10.1055/s-0034-1399147
Iavarone M, Sangiovanni A, Forzenigo LV et al (2010) Diagnosis of hepatocellular carcinoma in cirrhosis by dynamic contrast imaging: the importance of tumor cell differentiation. Hepatology 52:1723–1730. https://doi.org/10.1002/hep.23903
Guo L, Li X, Zhang C et al (2023) Radiomics based on dynamic contrast-enhanced magnetic resonance imaging in preoperative differentiation of combined hepatocellular-cholangiocarcinoma from hepatocellular carcinoma: a multi-center study. J Hepatocell Carcinoma 10:795–806. https://doi.org/10.2147/jhc.S406648
Li CQ, Zheng X, Guo HL et al (2022) Differentiation between combined hepatocellular carcinoma and hepatocellular carcinoma: comparison of diagnostic performance between ultrasomics-based model and CEUS LI-RADS v2017. BMC Med Imaging 22:36. https://doi.org/10.1186/s12880-022-00765-x
Acknowledgements
We thank American Journal Experts (https://china.aje.com/) for the professional writing service.
Funding
This work was supported by the National Natural Scientific Foundation of China [grant number 82171952].
Author information
Authors and Affiliations
Contributions
JY: conceptualization; data curation; formal analysis; writing original draft. YZ: conceptualization; investigation; methodology; writing original draft. WygB: data curation; formal analysis; investigation; methodology; resources. YdC: investigation; writing, review and editing. JyH: data curation. KyZ: data curation. HJ: writing, review and editing; formal analysis. BS: formal analysis. ZxH: conceptualization; writing, review and editing. QL: conceptualization; funding acquisition; writing, review and editing. All authors had access to the study data and reviewed and approved the final manuscript for publication.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This single-center retrospective study was approved by the Institutional Review Board of West China Hospital, Sichuan University, and the requirement for informed patient consent was waived.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests. Bin Song is a member of the Insights into Imaging Editorial Board; he has not taken part in the review or selection process of this article.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplement 1: eMethods 1.
Imaging acquisition protocols eMethods 2. Variable definition eMethods 3. The univariable selection of the CEUS-predominant and the CECT-predominant model eTable 1. Vascular phases of the liver lesions on CEUS eTable 2. Multi-phase contrast-enhanced CT scan eTable 3. The kappa analysis of imaging features assessment on CEUS and CECT between reviewers eTable 4. The multicollinearity analysis between variables of the CEUS-predominant model eTable 5. The multicollinearity analysis between variables of the CECT-predominant model eFigure 1. The calibration analysis of the CEUS-predominant model and the CECT-predominant models eFigure 2. The ROC curve of the two models in the subgroup analysis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yang, J., Zhang, Y., Bao, Wyg. et al. Comparison contrast-enhanced CT with contrast-enhanced US in diagnosing combined hepatocellular-cholangiocarcinoma: a propensity score-matched study. Insights Imaging 15, 44 (2024). https://doi.org/10.1186/s13244-023-01576-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13244-023-01576-6