
Abstract
Background
The Global Initiative for Asthma recommends the use of as-needed low-dose inhaled corticosteroid (ICS)-formoterol as a preferred controller therapy for patients with mild asthma. These recommendations were based, in part, on evidence from the SYGMA 1 and 2 studies of as-needed budesonide-formoterol. This analysis aimed to compare the cost-effectiveness of as-needed budesonide-formoterol to low-dose maintenance ICS plus as-needed short-acting β2-agonist (SABA) in patients with mild asthma.
Methods
A Markov cohort model was designed that included three possible health states (non-exacerbation, severe exacerbation, and death) to compare as-needed budesonide-formoterol 200–6 μg to twice-daily budesonide 200 μg maintenance therapy (low-dose ICS) plus as-needed terbutaline 0.5 mg (SABA). The deterministic base-case analysis used severe exacerbation, adverse event (AE), and healthcare resource use data from SYGMA 2, and was conducted from a Canadian public payer perspective with a 50-year time horizon, and a discount rate of 1.5% per annum. Moderate exacerbation was modelled on data from SYGMA 1 in sensitivity analyses. Utility values were derived from SYGMA 2 quality of life data. All-cause- and asthma-related mortality rates and costs (reported in 2019 Canadian dollars) were based on published data, using Canada-specific values where available. One-way deterministic sensitivity, probabilistic sensitivity, and eight scenario analyses were conducted to examine the robustness of the results.
Results
As-needed budesonide-formoterol was the dominant treatment option in the base-case analysis, providing incremental cost savings of $9882 per patient and quality-adjusted life year (QALY) gains of 0.002 versus low-dose maintenance ICS plus as-needed SABA over a 50-year time horizon. Using a willingness-to-pay threshold of $50,000/QALY ($100,000/QALY), as-needed budesonide-formoterol had a 94% (95%) probability of being cost-effective compared with maintenance ICS plus as-needed SABA. Cost-saving was mostly driven by lower overall medication and AE-related costs. As-needed budesonide-formoterol remained the dominant treatment in sensitivity and scenario analyses.
Conclusions
As-needed budesonide-formoterol is a cost-saving option for the treatment of mild asthma from the perspective of the Canadian public payer compared with low-dose maintenance ICS plus as-needed SABA.
Similar content being viewed by others


Background
Asthma is a chronic inflammatory disease of the airways, which is of significant public health concern in Canada [1]; approximately 2.6 million Canadians aged ≥ 12 years were living with asthma in 2018, representing 8.3% of the population [1, 2]. There is a substantial economic burden associated with asthma, and it has been estimated that sub-optimal asthma control will cost $213 billion and result in a loss of 1.38 million quality-adjusted life years (QALY) in Canada between 2014 and 2033 [3]. Mild asthma is common, occurring in 50–75% of patients with asthma [4], and although patients with more severe disease are responsible for the largest proportion of healthcare resource use [5], a considerable proportion of healthcare resource use is also attributable to patients with poorly controlled mild asthma [5, 6].
Previous Global Initiative for Asthma (GINA) reports have recommended daily maintenance inhaled corticosteroids (ICS) with short-acting β2-agonists (SABA) reliever therapy for the treatment of mild asthma [7]. However, real-world adherence to maintenance ICS treatment is typically poor, with patients tending to rely on SABA to manage their symptoms [8,9,10]. Overuse of SABA is prevalent [8, 9, 11], and monotherapy with SABA, i.e. without concomitant ICS use, is associated with an increased risk of exacerbations [9, 11, 12]. In Canada, inappropriate and excessive use of SABA has been observed [13, 14], with one study estimating that 28% of patients used at least three SABA canister refills per year without concomitant ICS prescriptions [14], and another suggesting up to a 1.4-fold increase in risk of annual exacerbations when SABA use is ≥ 3 canister refills per year (versus ≤ 2 refills per year) [15].
Given these risks, and the lack of an anti-inflammatory effect with SABA alone as initial therapy in mild asthma [10], the Canadian Thoracic Society guidelines define overuse of SABA as > 2 canisters in a year [16]. Daily ICS plus as-needed SABA is recommended as first line controller therapy in mild asthma, with as-needed budesonide-formoterol recommended as an alternative in patients ≥ 12 years with poor adherence to daily medication despite substantial asthma education and support [16]. Due to the risk of low adherence to the ICS component (thus subjecting the patient to SABA monotherapy) in previous guidelines, the latest GINA report now recommends symptom-driven as-needed low-dose ICS in combination with the long-acting β2-agonist (LABA), formoterol, as the preferred reliever for patients ≥ 12 years requiring GINA Step 1–2 treatment, i.e., when symptoms occur up to 4–5 days per week [17].
This therapeutic approach is supported by the results of two pivotal 52-week, double-blind, randomized controlled trials, SYGMA 1 [18] and SYGMA 2 [19], in patients with mild asthma, and two open-label, 52-week studies in patients with mild-to-moderate asthma (PRACTICAL) [20] or mild asthma (Novel START) [21], as well as a complementary systematic review and meta-analysis [22]. SYGMA 1, SYGMA 2 and Novel START demonstrated a comparable annual rate of severe exacerbations between as-needed budesonide-formoterol and twice daily budesonide maintenance (low-dose ICS) plus as-needed terbutaline (SABA), whereas the rate was significantly lower with as-needed budesonide-formoterol in the PRACTICAL study [20]. In the two studies that included an as-needed SABA arm, SYGMA 1 [18] and Novel START [21], the exacerbation rate was significantly lower with as-needed budesonide-formoterol than as-needed terbutaline.
On the basis of this evidence, budesonide-formoterol as anti-inflammatory reliever therapy was approved in Canada in September 2019 for patients aged ≥ 12 years with mild persistent asthma [23, 24]. A recent study found that as-needed budesonide-formoterol is cost-effective versus maintenance ICS plus as-needed SABA from a UK healthcare payer’s perspective [25], but this strategy has not been assessed from a Canadian perspective.
Canada has a public healthcare system that is managed by provincial and territorial governments to deliver medically necessary healthcare services to all legal residents. However, medication costs are covered only for those on low income, those enrolled in income-based universal programs, or other population groups that may require enhanced coverage for higher drug costs [26]. For the rest of the population, medication costs are paid either out-of-pocket or through private (usually employer) health insurance. For patients with chronic respiratory conditions this can represent an onerous economic burden.
In Canada, in addition to clinical efficacy data, information on the economic value of health technologies (e.g., medications) is a formal requirement for the adoption of such technologies into the healthcare system. Therefore, the primary objective of this study was to compare the cost-effectiveness of as-needed budesonide-formoterol to low-dose maintenance ICS plus as-needed SABA from a Canadian public payer perspective in patients with mild asthma.
Materials and methods
This study is reported according to the Consolidated Health Economic Evaluation Reporting Standards guidelines [27].
We developed a discrete-time Markov model to simulate the trajectory of mild asthma and the impact of treatment. A Markov cohort model is a well-accepted method for modelling asthma outcomes and their associated costs and impact on quality of life [28,29,30].
Patient population
The eligible patient population was that of the SYGMA studies [18, 19], i.e., asthma patients ≥ 12 years of age with a documented clinical diagnosis of mild asthma (GINA 2012 criteria [31]), either uncontrolled on as-needed SABA alone or controlled on regular low-dose ICS or a leukotriene receptor antagonist plus as-needed SABA.
Cost-effectiveness model
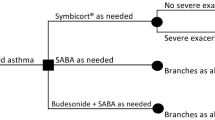
The Markov model had three health states (Fig. 1): (i) non-exacerbation; (ii) severe exacerbation; and (iii) death. Consistent with the American Thoracic Society/European Respiratory Society definition, a severe exacerbation was defined as a deterioration of asthma requiring the use of systemic corticosteroids (SCS) for at least 3 days, an emergency department (ED) visit resulting in SCS treatment, or inpatient care [32]. Moderate exacerbations data, sourced from SYGMA 1, were only included in the sensitivity analyses; such events were defined as a deterioration of asthma requiring a change in prescribed treatment, i.e., initiation of additional ICS to avoid progression to a severe exacerbation [18].

Base-case model structure. ED: emergency department
This model was designed from a public payer perspective, with only direct healthcare costs considered in the base-case analysis. We adopted a time horizon of 50 years to cover the lifetime of the majority of patients. The model used weekly cycles, reflecting the duration of asthma exacerbations observed in SYGMA 2 [19]. A discount rate of 1.5% per annum for both costs and outcomes was applied, as per the Canadian Agency for Drugs and Technologies in Health (CADTH) guidelines [33].
All patients entered the model in the non-exacerbation health state. Healthcare resource utilization data and health-related quality of life data from SYGMA 2 provided inputs for the model in this state. During each cycle of the model, patients either transitioned to a new health state or remained in their current state, with transitions according to a probability distribution derived from clinical data from SYGMA 2. Patients remained in the exacerbation health state for one cycle before transitioning to one of the other health states. Transitions to death had two components of risk: asthma-related risk of death and population level age- and gender-specific risk of death (background mortality) in Canada. In the sensitivity analyses, when the withdrawal health state was used, patients who transitioned to the withdrawal health state remained there for the rest of the time horizon or until death.
Results are presented as incremental costs per patient, incremental QALY per patient, and the incremental costs per QALY gained. All costs were reported in 2019 Canadian dollars ($). The inputs to the base-case model, as well as the main variables tested in the sensitivity analyses, are summarized in Table 1.
Treatment comparisons
The Canadian Thoracic Society guidelines recommend the use of SABA as a reliever in individuals with mild asthma on ICS monotherapy [16], which is the same as the comparator group in the SYGMA studies. The treatment groups in SYGMA 1 and SYGMA 2 from which clinical data were sourced for this analysis were the as-needed budesonide-formoterol 200–6 μg (Symbicort® Turbuhaler®, AstraZeneca) group, with 1277 patients in SYGMA 1 and 2089 in SYGMA 2, and the twice-daily budesonide 200 μg maintenance therapy (low-dose ICS; Pulmicort® Turbuhaler®, AstraZeneca) plus as-needed terbutaline 0.5 mg (SABA; Turbuhaler®, AstraZeneca) group, with 1282 patients in SYGMA 1 and 2087 in SYGMA 2 [18, 19].
Source of clinical data
Clinical efficacy evidence for the base-case analysis was derived from SYGMA 2 [19]. Inputs were annual severe exacerbation rates, stratified by three different severe exacerbation types (use of SCS; ED visit plus SCS; inpatient hospitalization—based on resources used), and proportions of adverse events (AEs) (Table 1). The relative frequency of severe exacerbations in SYGMA 2 was as follows: (i) use of SCS: 81.9% with as-needed budesonide-formoterol versus 78.4% with budesonide maintenance plus as-needed terbutaline; (ii) ED visit plus SCS: 10.2% versus 15.2%, respectively; and (iii) inpatient hospitalization: 7.9% versus 6.4%, respectively.
The most common AEs in SYGMA 2 (occurring in ≥ 2% of patients) were used: viral upper respiratory tract infection (viral URTI), URTI, bronchitis, pharyngitis, headache, allergic rhinitis, and influenza. Annual risk of AEs for each treatment were considered relevant to the model for patients in the non-exacerbation health state. To test the robustness of the results to variations in AE rates, a scenario analysis was completed that assigned no AEs to each comparator.
Treatment effect
The annual rates of severe exacerbation in SYGMA 2 were 0.11 [95% confidence interval (CI): 0.10–0.13] with as-needed budesonide-formoterol and 0.12 (95% CI 0.10–0.14) with budesonide maintenance plus as-needed terbutaline [19]. To convert the annual exacerbation rates from SYGMA 2 to transition probabilities, they were recalculated as a weekly rate and then converted to weekly probabilities using the formula p = 1-exp(-r), where p is probability and r is the rate [34]. In extrapolating treatment effects beyond the follow-up time of the SYGMA studies, we assumed a fixed treatment effect, with no effect waning over time. The distribution of the model cohort among the three severe exacerbation types remained the same over the time horizon of the model.
Source of mortality data
This analysis accounted for asthma-related and all-cause mortality. General population mortality data adjusted by age and gender were sourced from Canadian life tables [35]. It was assumed that asthma-related mortality can only occur from the exacerbation state. Deaths due to asthma exacerbations were modelled based on previously published data [36,37,38]. For exacerbations requiring hospital admission, this cost-effectiveness analysis used mortality data from Watson et al. [37] combined with Roberts et al. [36], and for exacerbations not requiring a hospital admission (i.e., ED visit and use of SCS) from Watson et al. [37], combined with data from the National Review of Asthma Deaths (NRAD) 2017 [38]. The annual risk of death related to severe asthma exacerbations is summarized in Additional file 1: Table S1. Annual risks were converted to a weekly risk and added to the risk of death for the general population.
Resource use and costs
We used the Ontario Drug Benefit Formulary/Comparative Drug Index (May 2020) to derive drug acquisition costs [39]. Derivation of total drug acquisition costs per day in each treatment group is shown in Table 2; costs per day for ICS maintenance therapy were based on the prescribed dose (i.e., two inhalations per day) of the most commonly prescribed maintenance ICS and SABA reliever for mild asthma in Canada (fluticasone propionate and salbutamol, respectively [40]). Based on best practice recommendations [33, 41], ICS maintenance therapy costs were calculated assuming full utilization (Table 2), therefore a scenario analysis was conducted to test whether costs based on actual maintenance ICS utilization as reported in SYGMA 2 (i.e. mean percentage of daily doses 62.8% [19]) influenced the outcome of the analysis.
The costs of severe exacerbations were calculated for each exacerbation type using healthcare resource utilization data from SYGMA 2 and Canadian unit costs (Additional file 1: Table S2). Specifically, SCS cost per day was calculated using the unit cost of prednisolone for a mean daily dose of 45 mg multiplied by the mean number of days SCS was used in SYGMA 2. The cost of an ED visit plus SCS was calculated using the unit cost of an ED visit ($412.87) added to SCS costs per day, calculated as described above. Hospitalization costs per stay ($9322) were calculated using weighted 2019 costs from the Ontario Case Costing Initiative Cost Analysis Tool (Code J441) [42], and mean length of stay in SYGMA 2 (6.9 days). The weekly costs of the non-exacerbation health state were added to the severe exacerbation costs, as it was assumed that patients experiencing a severe asthma exacerbation would still incur the weekly monitoring costs related to non-exacerbation. Healthcare costs associated with moderate exacerbations also included weekly monitoring costs as well as direct exacerbation costs.
Non-exacerbation health state costs were based on healthcare resource utilization data from SYGMA 2 (e.g., number of specialist, ED and general practitioner visits), and associated standard specific unit costs in 2017 [43] (Additional file 1: Table S3). Costs associated with the non-exacerbation health state were included in the base-case analysis (Table 1).
Sources of utility data
Utility data were collected in SYGMA 2 using the EuroQoL-5 Dimension-5 Level, and were used to provide utility weights in the model. The utility value for the non-exacerbation health state in the base-case analysis was 0.867, taken from the SYGMA 2 trial for patients not experiencing any exacerbation (Table 1). Severe exacerbations were associated with a decrement of utility (disutility), which was derived from a previous study by Lloyd et al. [44]. The study did not include a disutility value for a severe exacerbation requiring an ED visit plus SCS, so this was assumed to be − 0.15, the midway between the utility among patients requiring the use of SCS (− 0.10) and those requiring inpatient hospitalization (− 0.20) (Table 1). The disutility of the exacerbation was applied for the duration of the exacerbation.
Treatment withdrawal
Withdrawal was defined as discontinuation of treatment due to development of study-specific withdrawal criteria or due to AEs. Withdrawal was not included in the base-case analysis but it was included in the sensitivity analysis where withdrawal health states included step up from SABA alone to GINA Step 2 (daily low-dose ICS plus as-needed SABA or as-needed low-dose ICS-formoterol), and from Step 2 to Step 3 (low-dose ICS-LABA plus as-needed SABA or as-needed low-dose ICS-formoterol for patients prescribed maintenance and reliever therapy) [45]. Annual risks of withdrawal used in the sensitivity analysis were derived from SYGMA 1 and SYGMA 2 (0.8% and 0.7% with as-needed budesonide-formoterol, respectively, versus 1.2% and 1.1% with maintenance ICS plus as-needed SABA) (Table 1).
Analyses
Deterministic base-case analysis
The base-case analysis was based on point estimates of the previously described parameters. The main outcomes were total discounted costs and QALY with as-needed budesonide-formoterol compared with low-dose ICS plus as-needed SABA, as well as incremental costs and QALY. From these, the incremental costs per QALY was calculated to determine the dominant treatment strategy.
Probabilistic sensitivity analysis
Probabilistic sensitivity analysis (PSA) was performed using Monte Carlo simulations to incorporate uncertainty in the evidence base, involving the use of 1000 iterations. The methodology for assigning probability distributions for these simulations is described in Table 1. Where the information characterizing the parameter distribution was not available, we assumed a variance-to-mean ratio of 10%. PSA outcomes are shown in the form of a cost-effectiveness plane and cost-effectiveness acceptability curves (CEACs). The former depicts the joint distribution of incremental costs and QALY, whereas the latter presents the probability of cost-effectiveness at a range of willingness-to-pay (WTP) values for one QALY.
Deterministic sensitivity analyses
One-way deterministic sensitivity analyses (DSA) were performed to identify variables that influenced model results. In one analysis, the discount rate was changed to 0% and 3% (base-case 1.5%). Additionally, different values were examined for cohort starting age, severe exacerbation rates, cost units, ICS dose (inhalations/day), and (dis)utility values. Annual rates of withdrawal were also included in the one-way DSA. Finally, in a separate analysis, we included moderate exacerbations and associated cost and disutility values, based on data from SYGMA 1 (Table 1).
Scenario analyses
A series of probabilistic scenario analyses were performed to determine the robustness of the results to variations in several parameters at once. These analyses, which utilized 1000 PSA iterations, were as follows: Scenario 1 = discount rate of 0% for costs and benefits; Scenario 2 = discount rate of 3.0% for costs and benefits; Scenario 3 = time horizon of 2 years; Scenario 4 = time horizon of 10 years; Scenario 5 = societal perspective; and Scenario 6 = budesonide (Pulmicort®) as the ICS in the low-dose maintenance ICS plus as-needed SABA group; Scenario 7 = set utilization rate of ICS to 62.8%, as per the ICS maintenance group in SYGMA 2; and Scenario 8 = removal of AEs from the analysis.
Results
Base-case analysis
The estimated discounted total costs of treatment per patient over a 50-year time horizon were $36,439 with as-needed budesonide-formoterol and $46,321 with low-dose maintenance ICS plus as-needed SABA. The largest difference in costs were drug acquisition costs per day and AE-related costs (Table 3). Discounted QALY over a 50-year time horizon were 25.923 with as-needed budesonide-formoterol and 25.921 with maintenance ICS treatment plus as-needed SABA. Therefore, as-needed budesonide-formoterol was the dominant treatment, given its incremental cost savings of $9882 per patient and QALY gains of 0.002 versus maintenance ICS plus as-needed SABA over the 50-year time horizon.
Probabilistic sensitivity analysis
The results of the PSA are shown in Fig. 2. The CEACs (Fig. 3) showed that the probability of as-needed budesonide-formoterol being cost-effective, i.e., of being within the WTP threshold of $50,000 per QALY gained compared with maintenance ICS plus as-needed SABA was 94%. The probability of being within a WTP threshold of $100,000 per QALY was 95%.

Cost-effectiveness plane for as-needed budesonide-formoterol versus low-dose ICS plus as-needed SABA. ICS: inhaled corticosteroid; QALY: quality-adjusted life year; SABA: short-acting β2-agonist

Cost-effectiveness acceptability curve for as-needed budesonide-formoterol versus low-dose maintenance ICS plus as-needed SABA. Vertical line on graph indicates WTP threshold of $50,000. bid: twice daily; ICS: inhaled corticosteroid; SABA: short-acting β2-agonist; WTP: willingness-to-pay threshold
Deterministic sensitivity analysis
As-needed budesonide-formoterol was the dominant treatment strategy in all variations assessed in the one-way DSA; although the impact on the model differed for each variable studied, the model was not sensitive to any one parameter.
Scenario analyses
As-needed budesonide-formoterol was the dominant treatment strategy in all eight of the scenarios shown in Table 4, including shorter time horizons [2 or 10 years] and lower (0%) or higher (3.0%) discount rates than in the base-case analysis. As-needed budesonide-formoterol was dominant over the shorter time horizons because, although QALY gains were equal between treatment groups (both 0.000), the incremental cost savings per patient were $662 over a time horizon of 2 years and $3061 over 10 years. Incremental cost savings and QALY gains from the societal perspective with as-needed budesonide-formoterol were broadly similar to that observed in the base-case analysis, with an incremental cost saving of $9882 per patient and QALY gains of 0.002 versus maintenance ICS plus as-needed SABA. With budesonide as the ICS in the low-dose maintenance ICS group, as-needed budesonide-formoterol was associated with a cost saving of $14,431 and a QALY gain of 0.002. Moreover, as-needed budesonide-formoterol continued to be cost-saving and produce additional QALY gains in the scenarios that adjusted the utilization rate of ICS and removed AE rates.
Discussion
In this economic evaluation, as-needed budesonide-formoterol was the dominant treatment option compared with low-dose maintenance ICS therapy plus as-needed SABA in patients with mild asthma over a 50-year time horizon from a Canadian public payer perspective, with costs savings of $9882 per patient. These findings support those of a cost-effectiveness analysis from the UK healthcare payer perspective, which made similar treatment comparisons based on SYGMA 2 data [25].
An important finding in both the SYGMA 1 and SYGMA 2 studies is observed treatment adherence. In the budesonide maintenance groups, 79% of patients in SYGMA 1 were adherent to daily ICS [18]; this value was 63% in SYGMA 2, although daily adherence reminders were not given, unlike in SYGMA 1 [19]. These values are much higher than real-world ICS adherence rates that are typically reported (22–63%) [46]. Despite such differences in adherence, the results of our analysis are relevant to real-world practice, as patients less adherent to their daily ICS maintenance tend to rely on additional SABA instead [47]. This is associated with an increased risk of severe exacerbations, and thus related costs including ED visits, hospitalizations and SCS use [48]. A Canadian study found that SABA overuse is associated with a 45% increase in risk of an asthma-related hospital admission, a 25% increase in risk of asthma-related ED visits and a concomitant increase in direct asthma-related costs of 6% [13]. More recent evidence highlights that SABA overuse remains an ongoing issue in the management of patients with asthma in Canada [14, 15]. Approximately 60% of patients with asthma made ≥ 3 SABA canister claims annually in a study that used data from a Nova Scotia healthcare administrative database [14]. This SABA overuse was significantly (p < 0.01) associated with an increased number of asthma-related outpatient visits.
The cost saving associated with as-needed budesonide-formoterol versus low-dose maintenance ICS plus as-needed SABA was driven by lower direct healthcare costs, specifically drug acquisition costs per day, and lower AE costs. This was despite the base-case using a 100% utilization rate of maintenance ICS, i.e., two inhalations per day per the prescribing information. However, to reflect the more realistic utilization rate in SYGMA 2 (there were no maintenance medication reminders [19]), we ran a scenario analysis using the SYGMA 2 ICS utilization rate, and found this did not alter the dominance of as-needed budesonide-formoterol over maintenance ICS plus as-needed SABA. Our decision to derive ICS use from the prescribing information is supported by the Patented Medicine Prices Review Board’s Budget Impact Analysis guidelines, which specify that the dosing frequency used should be according to the product monograph or a public drug plan database, or other applicable drug plan data [41]. CADTH guidelines also state that where costs are directly calculated or imputed, they should reflect the full economic cost borne by the decision-maker [33]. Lower direct AE-related costs in our model could be due to the lower proportion of patients with potential local corticosteroid-related AEs in SYGMA 2 with as-needed budesonide-formoterol [49]. Prior Canadian pharmacoeconomic studies reported that medication costs comprised the largest proportion of annual direct asthma costs (64–68%) [6, 50], which may explain why differences in drug costs underpinned the saving in overall direct costs. AEs were included in our model in part because of recommendations in the CADTH guidelines that health interventions should be assessed in terms of the potential for harms, especially harms that are clinically meaningful and therefore are likely to impact costs [33]. However, as our scenario analysis showed, as-needed budesonide-formoterol was the dominant treatment even without AEs included in the model. Finally, Canada’s publicly funded healthcare system is directed to select treatments for funding by examining their cost and effect trade-off; our study provides evidence of the cost-effectiveness of as-needed budesonide-formoterol as a treatment option for patients with mild asthma.
Given the healthcare system perspective, we did not include indirect costs in the base-case analysis, but these were accounted for in a scenario analysis from the societal perspective. This takes into account the additional burden to the individual and society of time off work, workplace productivity loss [51], functional impairment and caregiver time [52], and out-of-pocket drug costs. When the model was run from the societal perspective, as-needed budesonide-formoterol remained dominant in the cost-effectiveness analysis. These results support previous findings from a Canadian cost-effectiveness study in patients with asthma uncontrolled on maintenance ICS or on maintenance daily ICS-LABA therapy: budesonide-formoterol as maintenance and reliever therapy was shown to be cost-saving on an annual basis from a societal perspective compared with the standard of care [53]. In the current analysis, the total incremental cost saving with as-needed budesonide-formoterol versus low-dose maintenance ICS plus as-needed SABA from the societal perspective was similar to that from the public payer perspective (both $9882). This may be explained, at least in part, by the nature of the societal costs included in this analysis. These were productivity loss, based on days off work per year, which were minimal (0.19 days for all patients in SYGMA 2).
The incremental QALY gain with as-needed budesonide-formoterol was small versus low-dose maintenance ICS plus as-needed SABA treatment. This was likely attributable to using annual severe exacerbations rates as the measure of clinical effectiveness, which were not only similar between the two treatments in SYGMA 2 [19], but also relatively low compared with what would be expected in patients with moderate or severe asthma. Furthermore, had we included mild and moderate exacerbations in the base-case analysis, it is possible that the results would have been even more favorable towards as-needed budesonide-formoterol. Nevertheless, the robustness of our modelling was confirmed by sensitivity analyses.
Limitations of this analysis include those of all Markov models, i.e., that it relies on assumptions, including that transitions between health states are not dependent on the time spent by the patient in any health state or on the sequence of events that preceded it, and that health states are mutually exclusive. There was also the potential for ‘double counting’ in some cases of death, as some of the deaths reported in the NRAD study [38] may also have been included in all-cause mortality estimates. While the model was based on a 50-year time horizon, the clinical efficacy data did not extend beyond 1 year of follow-up. Other limitations were the exclusion of mild and moderate exacerbations from the base-case analysis, as well as withdrawal from treatment. However, whilst withdrawal was not modelled in the main analysis, the sensitivity analysis showed it had no real impact. This is because the benefit and costs of both therapies are accrued for as long as they are taken; therefore, low adherence or withdrawal might narrow the difference in costs and QALY between treatment groups but would not change the direction of the results. Notwithstanding these limitations, the various sensitivity and scenarios analyses we conducted confirmed our model was robust.
Conclusions
From a Canadian public payer perspective, as-needed budesonide-formoterol is a cost-effective treatment over the lifetime of patients with mild asthma for whom the alternative treatment option is low-dose maintenance ICS therapy plus as-needed SABA.
Availability of data and materials
Data underlying the findings described in this manuscript may be obtained in accordance with AstraZeneca’s data sharing policy described at https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure.
Abbreviations
- AE:
-
Adverse event
- CEAC:
-
Cost-effectiveness acceptability curves
- CI:
-
Confidence interval
- DSA:
-
Deterministic sensitivity analyses
- ED:
-
Emergency department
- GINA:
-
Global Initiative for Asthma
- ICS:
-
Inhaled corticosteroids
- LABA:
-
Long-acting β2-agonist
- NRAD:
-
National Review of Asthma Deaths
- PSA:
-
Probabilistic sensitivity analysis
- QALY:
-
Quality-adjusted life years
- QoL:
-
Quality of life
- SABA:
-
Short-acting β2-agonist
- SCS:
-
Systemic corticosteroid
- URTI:
-
Upper respiratory tract infection
- WTP:
-
Willingness to pay
References
Public Health Agency of Canada. Report from The Canadian Chronic Disease Surveillance System: asthma and chronic obstructive pulmonary disease (COPD) in Canada, 2018. Ottawa, ON: Public Health Agency of Canada; 2018. Report No.: Public Health Agency of Canada.
Statistics Canada. Asthma by age group: statistics Canada; 2018. https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310009608. Accessed 30 Mar 2020.
Zafari Z, Sadatsafavi M, Chen W, FitzGerald JM. The projected economic and health burden of sub-optimal asthma control in Canada. Respir Med. 2018;138:7–12.
Dusser D, Montani D, Chanez P, de Blic J, Delacourt C, Deschildre A, et al. Mild asthma: an expert review on epidemiology, clinical characteristics and treatment recommendations. Allergy. 2007;62(6):591–604.
Chapman KR. Impact of ‘mild’ asthma on health outcomes: findings of a systematic search of the literature. Respir Med. 2005;99(11):1350–62.
Sadatsafavi M, Lynd L, Marra C, Carleton B, Tan WC, Sullivan S, et al. Direct health care costs associated with asthma in British Columbia. Can Respir J. 2010;17(2):74–80.
Global Initiative for Asthma. GINA report, global strategy for asthma management and prevention: GINA. 2018. https://ginasthma.org/wp-content/uploads/2018/04/wms-GINA-2018-report-V1.3-002.pdf. Accessed 03 Dec 2020.
Tavakoli H, Mark FitzGerald J, Lynd LD, Sadatsafavi M. Predictors of inappropriate and excessive use of reliever medications in asthma: a 16-year population-based study. BMC Pulm Med. 2018;18(1):33.
Reddel HK, FitzGerald JM, Bateman ED, Bacharier LB, Becker A, Brusselle G, et al. GINA 2019: a fundamental change in asthma management: treatment of asthma with short-acting bronchodilators alone is no longer recommended for adults and adolescents. Eur Respir J. 2019;53(6):1901046.
O’Byrne PM, Jenkins C, Bateman ED. The paradoxes of asthma management: time for a new approach? Eur Respir J. 2017;50(3): 1701103.
Nwaru BI, Ekstrom M, Hasvold P, Wiklund F, Telg G, Janson C. Overuse of short-acting beta2-agonists in asthma is associated with increased risk of exacerbation and mortality: a nationwide cohort study of the global SABINA programme. Eur Respir J. 2020. https://doi.org/10.1183/13993003.01872-2019.
Stanford RH, Shah MB, D’Souza AO, Dhamane AD, Schatz M. Short-acting beta-agonist use and its ability to predict future asthma-related outcomes. Ann Allergy Asthma Immunol. 2012;109(6):403–7.
FitzGerald JM, Tavakoli H, Lynd LD, Al Efraij K, Sadatsafavi M. The impact of inappropriate use of short acting beta agonists in asthma. Respir Med. 2017;131:135–40.
Noorduyn N, Soliman M, Johnston K, Christina Q, Hernandez P, Penz E. SABA overreliance and physician visits in Canada [abstract 4645]. Eur Respir J. 2020;56(3):4645.
Quint J, Arnetorp S, Janson C, Boarino S, Kocks JW, Gilbert I et al. Short-acting ß2-agonist use in asthma in Western societies. European Respiratory Society International Congress; 7–9 Sept 2020.
Yang CL, Hicks EA, Mitchell P, Reisman J, Podgers D, Hayward KM, et al. Canadian thoracic society guideline—a focused update on the management of very mild and mild asthma. Can J Respir Crit Care Sleep Med. 2021. https://doi.org/10.1080/24745332.2021.1877043.
Global Initiative for Asthma. 2021 GINA report, global strategy for asthma management and prevention 2021. www.ginasthma.org/reports. Accessed 26 July 2021.
O’Byrne PM, FitzGerald JM, Bateman ED, Barnes PJ, Zhong N, Keen C, et al. Inhaled combined budesonide–formoterol as needed in mild asthma. N Engl J Med. 2018;378(20):1865–76.
Bateman ED, Reddel HK, O’Byrne P, Barnes PJ, Zhong N, Keen C, et al. As-needed budesonide–formoterol versus maintenance budesonide in mild asthma. N Engl J Med. 2018;378(20):1877–87.
Hardy J, Baggott C, Fingleton J, Reddel HK, Hancox RJ, Harwood M, et al. Budesonide-formoterol reliever therapy versus maintenance budesonide plus terbutaline reliever therapy in adults with mild to moderate asthma (PRACTICAL): a 52-week, open-label, multicentre, superiority, randomised controlled trial. Lancet. 2019;394(10202):919–28.
Beasley R, Holliday M, Reddel HK, Braithwaite I, Ebmeier S, Hancox RJ, et al. Controlled trial of budesonide-formoterol as needed for mild asthma. N Engl J Med. 2019;380(21):2020–30.
Hatter L, Bruce P, Braithwaite I, Holliday M, Fingleton J, Weatherall M, et al. ICS-formoterol reliever versus ICS and SABA reliever in asthma: a systematic review and meta-analysis. ERJ Open Res. 2020. https://doi.org/10.1183/23120541.00701-2020.
AstraZeneca Canada Inc. Symbicort® Turbuhaler® (budesonide/formoterol) product monograph 2019. https://www.astrazeneca.ca/en/our-medicines.html. Accessed 4 Mar 2020.
Symbicort® Turbuhaler® now approved by Health Canada for mild, persistent, moderate, or severe asthma [press release]. Mississauga, ON: AstraZeneca Canada, 30 Sep 2019.
FitzGerald JM, Arnetorp S, Smare C, Gibson D, Coulton K, Hounsell K, et al. The cost-effectiveness of as-needed budesonide/formoterol versus low-dose inhaled corticosteroid maintenance therapy in patients with mild asthma in the UK. Respir Med. 2020;171: 106079.
Health Canada Government of Canada. Canada’s Health Care System 2020. https://Canada.ca. Accessed 30 March 2020.
Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, et al. Consolidated health economic evaluation reporting standards (CHEERS) statement. Value Health. 2013;16(2):e1-5.
Rodriguez-Martinez CE, Nino G, Castro-Rodriguez JA. Cost-utility analysis of daily versus intermittent inhaled corticosteroids in mild-persistent asthma. Pediatr Pulmonol. 2015;50(8):735–46.
Fuhlbrigge AL, Bae SJ, Weiss ST, Kuntz KM, Paltiel AD. Cost-effectiveness of inhaled steroids in asthma: impact of effect on bone mineral density. J Allergy Clin Immunol. 2006;117(2):359–66.
Chouaid C, Vergnenegre A, Vandewalle V, Liebaert F, Khelifa A, et al. The costs of asthma in France: an economic analysis by a Markov model. Rev Mal Respir. 2004;21(3 Pt 1):493–9.
Global Initiative for Asthma. GINA report, global strategy for asthma management and prevention 2012. https://ginasthma.org/gina-reports/. Accessed 21 Jan 2021.
Reddel HK, Taylor DR, Bateman ED, Boulet LP, Boushey HA, Busse WW, et al. An official American Thoracic Society/European Respiratory Society statement: asthma control and exacerbations: standardizing endpoints for clinical asthma trials and clinical practice. Am J Respir Crit Care Med. 2009;180(1):59–99.
The Canadian Agency for Drugs and Technologies in Health (CADTH). CADTH guidelines for the economic evaluation of health technologies Canada. Ottawa: CADTH; 2017.
Fleurence RL, Hollenbeak CS. Rates and probabilities in economic modelling: transformation, translation and appropriate application. Pharmacoeconomics. 2007;25(1):3–6.
Statistics Canada. Life tables Canada, provinces and territories, 1980/1982 to 2015/2017 2019. https://www150.statcan.gc.ca/n1/en/catalogue/84-537-X2019001. Accessed 6 Feb 2020.
Roberts NJ, Lewsey JD, Gillies M, Briggs AH, Belozeroff V, Globe DR, et al. Time trends in 30 day case-fatality following hospitalisation for asthma in adults in Scotland: a retrospective cohort study from 1981 to 2009. Respir Med. 2013;107(8):1172–7.
Watson L, Turk F, James P, Holgate ST. Factors associated with mortality after an asthma admission: a national United Kingdom database analysis. Respir Med. 2007;101(8):1659–64.
Royal College of Physicians. Why asthma still kills. The national review of asthma deaths (NRAD) 2014. https://www.rcplondon.ac.uk/projects/outputs/why-asthma-still-kills. Accessed 30 Mar 2020.
Ontario Ministry of Health. Ontario drug benefit formulatry/comparative drug index Ontario: Queen’s Printer for Ontario. 2019. https://www.formulary.health.gov.on.ca/formulary/. Accessed 5 Mar 2020.
IQVIA. IQVIA Canada. 2019 public claims database. https://iqvia.com/locations/canada. Accessed 2019.
Patented Medicine Prices Review Board. Budget impact analysis guidelines 2020. https://www.canada.ca/content/dam/pmprb-cepmb/documents/reports-and-studies/budget-impact-analysis-guidelines/PMPRB-BIA-Guidlines-en.pdf. Accessed 22 Sept 2021.
Ontario Ministry of Health and Long-Term Care (MOHLTC)—Health Data Branch. Ontario case costing initiative (OCCI) 2019. https://hsim.health.gov.on.ca/hdbportal/. Accessed 2019.
Ontario Health Insurance Plan (OHIP). OHIP schedule of benefits and fees: Ontario Ministry of Health. 2017. http://www.health.gov.on.ca/en/pro/programs/ohip/sob/. Accessed 6 Mar 2020.
Lloyd A, Price D, Brown R. The impact of asthma exacerbations on health-related quality of life in moderate to severe asthma patients in the UK. Prim Care Respir J. 2007;16(1):22–7.
Global Initiative for Asthma. GINA report, global strategy for asthma management and prevention 2019. https://ginasthma.org/gina-reports/. Accessed May 2020.
Barnes CB, Ulrik CS. Asthma and adherence to inhaled corticosteroids: current status and future perspectives. Respir Care. 2015;60(3):455–68.
Rabe KF, Adachi M, Lai CK, Soriano JB, Vermeire PA, Weiss KB, et al. Worldwide severity and control of asthma in children and adults: the global asthma insights and reality surveys. J Allergy Clin Immunol. 2004;114(1):40–7.
Anis AH, Lynd LD, Wang XH, King G, Spinelli JJ, Fitzgerald M, et al. Double trouble: impact of inappropriate use of asthma medication on the use of health care resources. CMAJ. 2001;164(5):625–31.
Fitzgerald JM, O’Byrne P, Bateman ED, Barnes PJ, Zheng J, Ivanov S, et al. Safety of as-needed budesonide-formoterol in mild asthma: data from the two phase III SYGMA studies. Drug Saf. 2021. https://doi.org/10.1007/s40264-020-01041-z.
Bedouch P, Sadatsafavi M, Marra CA, FitzGerald JM, Lynd LD. Trends in asthma-related direct medical costs from 2002 to 2007 in British Columbia, Canada: a population based-cohort study. PLoS ONE. 2012;7(12): e50949.
Wong A, Tavakoli H, Sadatsafavi M, Carlsten C, FitzGerald JM. Asthma control and productivity loss in those with work-related asthma: a population-based study. J Asthma. 2017;54(5):537–42.
Ismaila AS, Sayani AP, Marin M, Su Z. Clinical, economic, and humanistic burden of asthma in Canada: a systematic review. BMC Pulm Med. 2013;13:70.
Sears MR, Boulet LP, Laviolette M, Fitzgerald JM, Bai TR, Kaplan A, et al. Budesonide/formoterol maintenance and reliever therapy: impact on airway inflammation in asthma. Eur Respir J. 2008;31(5):982–9.
GlaxoSmithKline. Flovent HFA, Flovent Diskus: product monograph Mississauga, Ontario: GlaxoSmithKline. 2018. https://ca.gsk.com/en-ca/products/flovent/. Accessed 5 Mar 2020.
Acknowledgements
The authors would like to thank Tracy Harrison and Stefan Courtney of inScience Communications, Springer Healthcare Ltd, UK, for providing medical writing support, which was funded by AstraZeneca in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Funding
AstraZeneca funded the study and had a role in study design, data collection, data analysis, data interpretation, and writing of the report. The corresponding author had full access to all the data and had final responsibility to submit for publication.
Author information
Authors and Affiliations
Contributions
All authors contributed to the review. In addition, MS, JMF, PMO, MS, NS and SMG contributed to the study concept and design and data interpretation. CV contributed to data acquisition and data interpretation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Mohsen Sadatsafavi has received honoraria from Boehringer Ingelheim, GlaxoSmithKline, and AstraZeneca, and research funding directly into his research accounts at the University of British Columbia from Boehringer Ingelheim and AstraZeneca (all unrelated to this work). J Mark FitzGerald reports grants and personal fees from AstraZeneca during the conduct of the study; grants paid to his institution from Canadian Institute for Health Research, National Institutes for Health, AllerGen NCE, AstraZeneca, Novartis, Boehringer Ingelheim, GlaxoSmithKline and Sanofi-Aventis outside the submitted work; personal fees from GlaxoSmithKline, Novartis, Sanofi Regeneron and Boehringer Ingelheim and is a Member of the Global Initiative for Asthma (GINA) Board and Science Committee. Paul M O’Byrne reports grants and personal fees from AstraZeneca during the conduct of the study; grants and personal fees from GlaxoSmithKline; personal fees from Menarini, Chiesi and Cipla; grants from MedImmune, AllerGen NCE, Genentech, Novartis, Merck and Bayer outside of the submitted work. Mena Soliman, Niroshan Sriskandarajah and Sarowar Muhammad Golam are employees of AstraZeneca. Colin Vicente is Managing Director of PIVINA Consulting Inc., which received funding from AstraZeneca to complete the cost-effectiveness analysis.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Annual risk of death related to severe asthma exacerbation. Table S2. Derivation of severe exacerbation costs (Canadian $, 2019). Table S3. Annual asthma healthcare resource utilization use and unit costs in the non-exacerbation health state.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sadatsafavi, M., FitzGerald, J.M., O’Byrne, P.M. et al. The cost-effectiveness of as-needed budesonide-formoterol versus low-dose inhaled corticosteroid maintenance therapy in patients with mild asthma in Canada. Allergy Asthma Clin Immunol 17, 108 (2021). https://doi.org/10.1186/s13223-021-00610-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13223-021-00610-w