
Abstract
Introduction
The onset of puberty is associated with a shift in the circadian timing of sleep, leading to delayed sleep initiation [i.e., later sleep onset time (SOT)] due to later bedtimes and/or longer sleep onset latency (SOL). Several genome-wide association studies (GWAS) have identified genes that may be involved in the etiology of sleep phenotypes. However, circadian rhythms are also epigenetically regulated; therefore, epigenetic biomarkers may provide insight into the physiology of the pubertal sleep onset shift and the pathophysiology of prolonged or delayed sleep initiation.
Results
The gene-wide analysis indicated differential methylation within or around 1818 unique genes across the sleep initiation measurements using self-report, actigraphy (ACT), and polysomnography (PSG), while GWAS-informed analysis yielded 67 genes. Gene hits were identified for bedtime (PSG), SOL (subjective, ACT and PSG) and SOT (subjective and PSG). DNA methylation within 12 genes was associated with both subjective and PSG-measured SOL, 31 with both ACT- and PSG-measured SOL, 19 with both subjective and ACT-measured SOL, and one gene (SMG1P2) had methylation sites associated with subjective, ACT- and PSG-measured SOL.
Conclusions
Objective and subjective sleep initiation in adolescents is associated with altered DNA methylation in genes previously identified in adult GWAS of sleep and circadian phenotypes. Additionally, our data provide evidence for a potential epigenetic link between habitual (subjective and ACT) SOL and in-lab SOT and DNA methylation in and around genes involved in circadian regulation (i.e., RASD1, RAI1), cardiometabolic disorders (i.e., FADS1, WNK1, SLC5A6), and neuropsychiatric disorders (i.e., PRR7, SDK1, FAM172A). If validated, these sites may provide valuable targets for early detection and prevention of disorders involving prolonged or delayed SOT, such as insomnia, delayed sleep phase, and their comorbidity.
Similar content being viewed by others


Background
The onset of puberty is associated with a shift in the circadian timing of sleep leading to delayed sleep initiation, as bedtimes become later or sleep onset latency (SOL) prolonged [1]. This shift toward a later sleep onset time (SOT) is due to maturational changes in the circadian and sleep homeostatic systems as children transition to adolescence [2]. Falling asleep requires circadian, homeostatic, de-arousal and cognitive processes [3], which are highly regulated by the interplay of environmental, psychosocial and biological factors. Understanding the cellular mechanisms of adolescents’ sleep onset may provide valuable targets for early detection and prevention of disorders involving prolonged (i.e., homeostatic) or delayed (i.e., circadian) SOT, such as insomnia disorder, delayed sleep phase disorder and their comorbidity. Indeed, inadequate sleep is highly prevalent in adolescents and is associated with multiple medical and psychiatric disorders [4,5,6,7,8]. In addition, inadequate adolescent sleep is a predictor of future sleep disorders in adulthood [9,10,11].
Several genome-wide association studies (GWAS) in adults have identified single-nucleotide polymorphisms (SNPs) in genes associated with sleep and circadian disorders [12,13,14,15,16]. These GWAS have included metabolic, cell-cycle, synaptic, and circadian-related (i.e., clock) genes. Epigenetic factors may explain the difference between the different SNPs identified across these GWAS investigations. Circadian rhythms are generated through the cyclical expression of specific genes [17] and are heavily regulated by environmental factors, such as the light–dark cycle, diet, heat/cold, among others [18]. DNA methylation (DNAm), the addition of a methyl group to the 5-carbon of cytosine in a Cytosine-phosphate-Guanine (CpG) dinucleotide, is one of the mechanisms by which environmental factors interact with gene expression [19, 20]. DNAm changes are promising biomarkers for developing diagnostic and therapeutic tools partly because they can be seen early in disease processes and the lifespan [21, 22]. Previous studies have identified epigenetic changes associated with inadequate sleep [23]. For example, aberrant DNAm profiles have been identified in adult obstructive sleep apnea syndrome and circadian rhythm shift-work disorder [24, 25], as well as abnormal methylation patterns of clock genes in neurodegenerative and psychiatric disorders [26,27,28]. This suggests that the etiology of inadequate sleep may have an epigenetic component.
However, of the prior studies that examined DNAm and sleep in humans, most investigated a small sample of adults with specific sleep disorders [29, 30], and few studies have included sleep measures when studying DNAm in children or adolescents. In children, a meta-analysis found a longitudinal association between actigraphy (ACT)-measured sleep duration and cord blood methylation, but there were no associations for parent-reported sleep measures or cross-sectional associations between DNAm and sleep among children [31]. To our knowledge, three previous studies have investigated DNAm changes associated with sleep phenotypes in adolescence. Huang and colleagues reported an association between subjective sleep duration and DNAm of the circadian-controlled gene, DOCK1 in 18- to 19-year-olds [32]. Jansen and colleagues identified an association between objective sleep duration and the metabolic genes PPARA and HSD11B2 in 14-year-old girls [33]. Koopman-Verhoeff and colleagues identified an association between ACT-estimated sleep duration and methylation in a module of inter-correlated CpG sites in 10-year-olds [34]. None of these previous studies examined the association between DNAm and sleep initiation phenotypes in adolescents, a key process that deviates during this developmental stage. Additionally, few studies measure objective and subjective sleep outcomes within the same individuals, which may not provide the same results; for example, subjective SOL, as per self-reports, and objective SOL, as per ACT or PSG, assess equally relevant but different dimensions of the same psychobiological process. Self-reports of sleep do not always match or align with objective (i.e., ACT or PSG) measures of sleep [35], as sleep is both a neurobiologically-controlled physiologic need and an observed and modifiable behavior that may be perceived or experienced differently under similar physiologic conditions, as depicted in Fig. 1.

A comparison of sleep initiation measurement methods for two sample participants. Bedtime, sleep onset latency (SOL), and sleep onset time (SOT) are depicted for polysomnography (PSG), actigraphy (ACT), and self-report (SR). PSG SOT is measured as the onset of sleep stage N2, depicted as S2. ACT SOT is calculated from movements and can underestimate sleep latency. SR is measured using participant questionnaires
To fill the gap in understanding the epigenetic underpinnings of sleep initiation in adolescents, we performed two sets of analyses investigating the association of DNAm with subjective (i.e., self-reported) and objective (i.e., ACT-measured and in-lab PSG) bedtime, SOL and SOT in adolescents. First, we analyzed intragenic and surrounding methylation sites measured broadly throughout the genome (i.e., gene-wide DNAm). Second, we analyzed specific genes based on previous sleep-related GWAS investigations (i.e., GWAS-informed DNAm) [12,13,14,15,16]. We hypothesized that a later SOT, beyond that expected for a developmental shift in adolescence, will be associated with DNAm in genes previously identified to be involved in sleep regulation and adverse health outcomes.
Results
Characteristics of the sample
The demographic characteristics of the 263 participants with DNAm data are presented in Table 1. The sample had an average age of 17 years [13,14,15,16,17,18,19,20,21,22,23], 55.9% were male, and 23.2% identified as a racial/ethnic minority. Participants self-reported an average bedtime at 23:40, an average SOL of 24.1 min, and an average SOT at 24:06. When using at-home ACT, participants showed an average bedtime at 23:59, SOL of 7.5 min, and a SOT at 24:07. During in-lab PSG, participants had an average bedtime at 22:00, SOL of 25.7 min, and a SOT at 22:26.
Overall DNAm findings
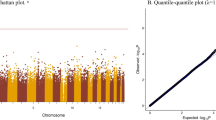
Among the 166,158 analyzable cytosine-phosphate-guanine (CpG) sites, 122,924 intragenic and surrounding sites were annotated onto 12,685 unique genes, while the remaining intergenic sites were not used for the analysis. The gene-wide analysis resulted in 2789 significant sites in 1818 unique genes across the 9 sleep measurements, and the GWAS-informed analysis resulted in 120 sites in 67 unique genes. These sites were statistically significant with q-values < 0.05 (i.e., p-values adjusted for false discovery rate). Manhattan plots for each analysis are located in Additional file 1: Figure S2, and a summary of the number of significant sites for each sleep measure is in Table 2. Additionally, all significant sites are included in Additional file 2.
Enrichment analyses
Both the hypergeometric and permutation tests suggested enrichment of methylation changes among sleep-related genes for subjective bedtime (Phypergeometric = 0.007, Ppermutation = 0.04), PSG-measured bedtime (Phypergeometric < 0.001, Ppermutation = 0.005), and subjective SOT (P hypergeometric < 0.001, Ppermutation = 0.003). The remaining sleep measurements did not show enrichment of sleep-related genes for either the hypergeometric or permutation tests. The hypergeometric and permutation test p-values are summarized in Additional file 1: Table S1. The gene ontology pathway analysis suggested GO terms were overrepresented in PSG-bedtime and SOL by all three measurements after FDR adjustment. The remaining sleep measures did not show enrichment of any GO terms. The top 10 significant biological process (BP) pathways for each analysis are summarized in Table 3, while the remainder are listed in Additional file 2.
DNAm sites associated with sleep initiation
The top 10 genes from the gene-wide analysis can be found in Table 4 for each of the nine sleep metrics. The top 10 GWAS-informed genes can be found in Table 5 for each of the nine sleep metrics. Self-reported and ACT-measured bedtimes were not significantly associated with any sites after adjustment for false discovery rate (q values > 0.05). PSG-measured bedtime was associated with DNAm of 1301 sites within 991 unique genes included in the gene-wide analysis and 62 sites within 37 GWAS-informed genes.
Self-reported SOL was associated with differential DNAm of 460 sites in 374 genes included in the gene-wide analysis and 31 sites within 20 GWAS-informed genes.
ACT-measured SOL was associated with DNAm of 610 sites within 362 genes included in the gene-wide analysis and 18 sites within 11 genes included in the GWAS-informed analysis. Of these genes, 19 from the gene-wide analysis and one (RASGRF2) from the GWAS-informed analysis were also associated with self-reported SOL.
PSG-measured SOL was associated with 442 sites within 277 genes from the gene-wide analysis and 10 sites within 10 genes from the GWAS-informed analysis. Of these genes, 12 from the gene-wide analysis and none from the GWAS-informed analysis were also associated with self-reported SOL. Furthermore, of the PSG-measured SOL-associated genes, 31 from the gene-wide analysis and 1 (CD59) from the GWAS-informed analysis were also associated with ACT-measured SOL. One gene (SMG1P2) from the genome-wide analysis was associated with SOL measured by all three methods.
Self-reported SOT was associated with methylation levels in the promotor region of a single gene (MUC20) after adjusting for false discovery rate, while ACT-measured SOT was not significantly associated with any sites after adjustment for false discovery rate (q values > 0.05). PSG-measured SOT was associated with 249 sites in 161 genes from the gene-wide analysis and 7 sites within 7 genes from the GWAS-informed analysis. There was a significant overlap between the significant genes associated with PSG-measured SOT and SOL, with 157 genes associated with both.
Discussion
In a population-based sample of adolescents, we detected changes in leukocyte methylation levels associated with markers of sleep initiation within several genes, including some previously identified in GWAS studies of sleep-related phenotypes in adults. Our data provide evidence for a potential epigenetic link between a delayed sleep onset in youth, measured subjectively or objectively, with specific genes involved in circadian regulation (i.e., RASD1, RAI1), cardiometabolic disorders (i.e., FADS1, WNK1, SLC5A6), and neuropsychiatric disorders (i.e., PRR7, SDK1, FAM172A). Adolescence is a period of maturational changes in the circadian and sleep homeostatic systems, which can lead to a shift towards later sleep onset. Thus, understanding the cellular mechanisms and sequelae when these changes deviate from what is developmentally expected and result in prolonged or delayed sleep initiation may provide valuable targets for early detection and prevention of comorbid disorders.
Many of the genes identified in the present study were associated with either bedtime or SOL, but not both. while these measures are related, we expect the gene associations with each to be different, as conceptually depicted in Fig. 1. For example, if two individuals report a late bedtime (1:00 am) but have different SOL (10 vs. 60 min) and only SOL shows significant DNAm for a specific gene, it suggests that the circadian timing of sleep may not have a strong epigenetic association if there is physiologic sleep ability (10 min sleep latency). In contrast, difficulty falling asleep (60 min sleep latency) does have a significant epigenetic association with that site. We also found differential associations with subjective versus objective measures of sleep initiation, which aligns with prior research showing that subjective and objective sleep measures do not always align (Fig. 2) and capture different aspects of sleep behavior and physiology [35].

Correlation matrix among sleep initiation measures. The correlation matrix displays the relationships among the different measures of sleep initiation. These measures include bedtime, SOL, and SOT measured by self-report, ACT, and PSG. The color and size of each circle represent the correlation coefficient. The p-value for each correlation is indicated in the matrix: *p < 0.05, **p < 0.01,***p < 0.001
Interestingly, we did not find significant sites for habitual bedtime as measured by self-report or ACT, but there was signal for bedtime in the lab for the PSG study. In-lab bedtime was standardized with a range from 21:00 to 23:00 for participants to select from; thus, the significant gene sites identified may be likely a result of individual preference within the allowed timeframe that was provided. Although in-lab sleep initiation does not correlate well with at-home sleep initiation (Fig. 2), in-lab PSG is a test for the participants’ physiologic ability to initiate sleep under controlled environmental conditions and may have served to test the function of the de-arousal processes needed to fall asleep.
Circadian regulation
Methylation changes in sleep-related genes identified in GWAS studies were found to be significantly enriched in the hypergeometric and permutation analysis for bedtime (subjectively and PSG-measured) and subjective SOT. No enrichment of sleep-related genes was observed for the remaining sleep initiation measurements. This may be due to the fact that measuring methylation in peripheral blood did not allow us to identify methylation changes in CLOCK genes that may be occurring at the central nervous system (CNS) level. Despite an overall lack of enrichment of sleep-related genes, we observed that DNAm levels in several GWAS-informed genes were related to sleep initiation, including SOL. These associations may be the result of methylation changes in circadian-related genes, such as RASD1 and RAI1, or may be a peripheral consequence of prolonged or delayed sleep initiation. Previously, mutations in RASD1 mutations have been associated with self-reported circadian preference [36], and mutations in RAI1, an important gene involved in circadian melatonin secretion, have been shown to cause abnormal chronology of the sleep–wake cycle and sleep maintenance disorders [37]. In our study population, decreased methylation at different sites within RAI1 and RASD1 was significantly associated with a later bedtime, a longer SOL and a later SOT, as assessed by objective measures. Thus, our DNAm findings further support that sleep initiation in adolescents is tightly linked to genes involved in the regulation of circadian rhythms and, that, later sleep initiation may lead to hypomethylation of specific genes.
Cardiometabolic disorders
Metabolic processes, including glucose and lipid metabolism as well as insulin secretion, are tightly regulated by the circadian system [38]. Sleep disorders have been liked to an increased risk of metabolic-related disorders such as obesity, insulin resistance, hypertension, and type 2 diabetes [39,40,41]. These associations may be mediated by changes in methylation levels of genes involved in metabolic homeostasis (SLC5A6), blood pressure (WNK1), and lipid metabolism (FADS1). We found that increased methylation at one site within SLC5A6 was significantly associated with a later PSG-measured bedtime, while decreased methylation at a nearby site was associated with a longer ACT-measured SOL. SLC5A6, a gene involved in biotin and pantothenic acid uptake, has been shown to have decreased expression in mice after circadian disruption [42]. We found that decreased methylation in WNK1, a gene regulated by the circadian protein Per1 and involved in blood pressure regulation [43], was associated with longer ACT-measured SOL. We found that increased methylation of FADS1 was associated with a later PSG-measured bedtime, while decreased methylation at a nearby site was associated with a longer PSG-measured SOL. Increased methylation in FADS1 has been associated with decreased FADS1 expression and an altered fatty acid profile [44]. These findings further support the idea that prolonged sleep initiation in adolescents may be linked to cardiometabolic health at the epigenetic level.
Neuropsychiatric disorders
The relationship between inadequate sleep and adverse neuropsychiatric outcomes is well-established, as sleep and circadian disturbances are transdiagnostic across neurodevelopmental, psychopathological, and neurocognitive disorders [45]. Sleep disturbances are common in mood disorders, such as major depressive disorder (MDD), and are consistently associated with psychosis as well as most neurodegenerative disorders, including Alzheimer’s disease (AD). Although methylation at some CpG sites does not necessarily reflect changes in brain tissue for many sites [46], the GO pathway analysis showed an overall overrepresentation of methylation changes in genes involved in neural development with longer habitual SOL measured subjectively and objectively. Additionally, we identified significant methylation sites in individual genes that have been previously linked to neuropsychiatric disorders, including depressive disorders (FAM172A), internalizing disorders (SDK1), and neurodegenerative disorders (PRR7).
We found that increased DNAm in FAM172A was significantly associated with a later bedtime, as preferred by subjects for the PSG study. FAM172A is a tumor suppressor that has been associated with MDD [47], and maternal circadian disruption has been associated with placental FAM172A methylation levels [48]. Previous studies have shown a link between a later bedtime preference and MDD [49], and one potential mechanism for this link could involve methylation. We also found that increased methylation in SDK1 was significantly associated with a longer SOL, as assessed subjectively but not objectively. SDK1 mutations have been associated with anxiety disorders [50], and blood methylation levels in SDK1 have been associated with different forms of psychopathology [51, 52]. Individuals who suffer from anxiety may report taking a long time to fall asleep because anxiety may continue beyond physiologic sleep onset occurs and prolongs the experience of being awake in bed. Our adolescent data further suggests an epigenetic link between difficulty initiating sleep, as measured by subjective reports of SOL, and mental health disorders. Additionally, decreased methylation of PRR7, a gene associated with higher-order cognitive functions [53] and linked to neural cell death in neurodegenerative disorders [54], was found to be associated with longer SOL, as objectively assessed by PSG and ACT. These findings provide initial evidence that difficulty initiating sleep during adolescence may contribute to neurocognitive disorders through epigenetic mechanisms.
Strengths and limitations
Compared to previous studies exploring the relationship between DNAm and measures of sleep, several strengths of our current study may be noted. Our study's use of multiple measures of sleep initiation, including bedtime, SOL, and SOT, allows for a more comprehensive understanding of the relationship between sleep initiation and methylation patterns. Furthermore, we used a combination of both subjective (self-report) and objective (ACT, PSG) measures to better disentangle the multidimensional nature of sleep initiation as both an objectively measurable and perceived phenomenon. We also measured sleep in two distinct contexts: ad-libitum in the home environment (ACT) and under controlled laboratory conditions (PSG). This methodology allowed us to capture a more complete picture of the de-arousal process required for sleep initiation. These relationships were measured in a randomly selected population-based sample of adolescents. Despite these strengths, it is important to acknowledge the limitations of the study. First, there were missing data in the raw methylation sequencing data, which was a result of using a novel whole-genome methylation sequencing technique on the low-yield DNA samples. To maintain the validity of our results, we deliberately excluded those sites with < 10 × coverage or those that were available from < 50% of the sample. In the enrichment analyses, we further limited the scope to CpG sites located within GWAS-informed genes. Second, the sample size (N = 263) of DNA samples was small for genetic studies. Third, DNAm was measured in peripheral blood for a phenotype that is highly centrally regulated. Although some CpG sites have correlation between blood and brain tissue [46], blood DNAm could be a result of environmental or biological factors or outcomes of sleep disturbances or their comorbidities. It is likely that there are epigenetic associations in sleep regulatory regions of the brain that were not detected in our study. Finally, the cross-sectional nature of the analyses does not allow for causal inference. Despite these limitations, our discovery study provides valuable preliminary findings on DNAm and sleep initiation in adolescents.
Conclusions
In conclusion, we observed in a population-based sample of adolescents that sleep initiation was associated with aggregated changes in DNAm from peripheral blood leukocytes in genes previously associated with circadian and cardiometabolic regulation as well as with neuropsychiatric disorders. We further identified associations between methylation in specific genes and sleep initiation measured subjectively and objectively. However, it should be noted that further validation and replication studies are needed to confirm these findings. Nevertheless, these identified methylation changes may provide valuable targets for early detection and prevention of disorders involving prolonged or delayed sleep initiation, such as insomnia, delayed sleep phase and their comorbidities.
Methods
Participants
We analyzed data from 263 adolescents from the Penn State Child Cohort (PSCC). The recruitment and procedures for each study visit have been published elsewhere [55,56,57]. In brief, 700 children aged 5–12 years were randomly recruited from central Pennsylvania in 2002–2006. Of those, 421 we reexamined in 2010–2013 as adolescents aged 12–23 years (90% of them were younger than 19 years) [58]. No significant differences in demographic characteristics were observed between the 421 reexamined and the 279 lost for the adolescent exam [11, 56]. All participants were evaluated in the Clinical Research Center at Penn State University College of Medicine, including a complete clinical history, physical examination, self-reported questionnaires, a 9-h fixed-time PSG recording in sound-, light-, and temperature-controlled rooms, morning blood draws, and 7-nights at-home ACT monitoring. A total of 263 participants’ morning blood was processed for assaying for DNAm, as described in detail below. Written informed consent from the parent/legal guardian and participants 18 years or older and assent from those younger than 18 were all obtained.
Sleep initiation measures
Self-reported retrospective questionnaires assessed for bedtime with the questions, “At what time do you go to bed on weekdays?” and, “At what time do you go to bed on weekends?”. Each subject’s weighted average bedtime was calculated as [(5 * weekdays bedtime in hh:mm + 2 * weekends bedtime in hh:mm)/7 nights]. Self-reported SOL was assessed with the question, “How long does it take you to fall asleep at bedtime?” and recorded in minutes. SOT was calculated by adding weighted average bedtime in hh:mm + SOL in minutes, converted to hh:mm.
An in-lab PSG study was recorded for nine hours in bed from the time of “lights out” (21:00–23:00) until the time of “lights on” (06:00–08:00) to provide a standardized measure of physiologic sleep under controlled in-lab conditions. All PSG recordings were performed on digital electroencephalography, electrooculography, electromyography, electrocardiography and respiratory measures (TWin Recording and Analysis, Grass Telefactor, West Warwick, RI, USA) with a sampling rate of 200 Hz and filter settings at 0.1–70.0 Hz. Independent RPSGTs visually scored all PSG recordings in 30-s epochs following standard criteria and were blind from the participants’ characteristics [59]. In the present study, PSG-identified bedtime was defined as the time of “lights out,” ranging from 21:00 to 23:00, based on the participants’ preference within that range. SOL in minutes was defined as the time elapsed from “lights out” to the first epoch scored as stage 2 [59]. SOT was calculated by adding PSG “lights out” in hh:mm + PSG SOL in minutes, converted to hh:mm.
A 7-night at-home ACT monitoring was performed by participants wearing a tri-axis accelerometer device (GT3X + , Actigraph LLC, Pensacola, FL, USA) for consecutive nights on the wrist of the non-dominant hand. Participants recorded “bedtime” and “rising time” daily in a log, which served to reconcile the bedtimes and rising times objectively recorded by the ACT device. After carefully examining and removing artifacts from the ACT data, all records were scored using Sadeh’s algorithm built in Actilife software (Actigraph LLC, Pensacola, FL, USA). ACT data with fewer than five nights of measurements were excluded. Each subject’s average bedtime was extracted from the seven consecutive nights and recorded in hh:mm. SOL recorded in minutes was also extracted from the automatic scoring in Actilife. SOT was calculated by adding ACT bedtime in hh:mm + ACT SOL in minutes, converted to hh:mm.
Genome-wide methylation assay
A total of 391 participants out of the 421 adolescents consented to a blood draw. Fasting peripheral blood samples were collected from each participant and stored at − 80 °C until use. DNA from peripheral blood leukocytes was extracted and subjected to reduced representation bisulfite sequencing (RRBS) using a modified method that has been used in prior studies [60, 61]. Single nucleotide resolution of DNAm in CpG sites and surrounding regions were detected using Illumina HiSeq. 2500. This highly sensitive, multiplexed method generated a specific, reduced representation of the genome of DNA fragments enriched for CpG dinucleotides. Briefly, genomic DNA (minimum 5 ng) was digested with a methylation-insensitive restriction enzyme, MspI, which recognizes CCGG. The digested DNA fragments were purified and subjected to adapter ligation and size selection by AMPure magnetic beads (Beckman Coulter Inc., Brea, CA, USA.). The resulting libraries, covering the target size range between 40 to 200 bp, were quantified by Kapa Library Quantification Kit (Kapa Biosystems Inc., Wilmington, MA, USA). Equimolar libraries were pooled, and unmethylated cytosines (C) were converted to uracils (U) with bisulfite, amplified by polymerase chain reaction, and sequenced. The degree of methylation of each fragment, estimated from the number of converted reads compared to the unconverted reads in each CpG, was calculated. Base calls of bisulfite-treated sequencing reads with phred quality scores < 20 and length < 35 bp were trimmed, and the adaptor was cut using trim_galore V0.3.3 (Babraham Bioinformatics, Cambridge, UK). The resulting reads were mapped to the hg19 assembly, and methylation calls were performed using Bismark v0.10.1 (Babraham Bioinformatics, Cambridge, UK). After alignment, approximately 1.6 million methylation levels were detected at more than 10 × coverage.
Statistical analyses
To ensure the validity of the DNAm data and statistical inferences of the analyses, we excluded bases with < 10 × coverage or available from < 50% samples, leaving a total of 166,158 analyzable sites. Among the 391 blood samples, 263 yielded an adequate amount of DNA to be sequenced. There was no significant difference in the major demographic characteristics between the subjects whose DNA was sequenced and the original cohort, as previously reported [61]. We used multivariable-adjusted linear regression models to investigate the relationship between sleep initiation measurements and DNAm. In these models for bedtime, SOL and SOT, the respective sleep measurement and site-specific methylation levels were treated as dependent and independent variables, respectively, while adjusting for age, race, sex, BMI percentile, and batch effects. Sites from the converged models were annotated based on the hg19 assembly in R [62]. Gene borders were extended to include − 1500 bp upstream and + 500 bp downstream the gene boundaries. All intragenic and surrounding sites were then taken forward for enrichment analyses. A q value < 0.05 was used to determine the significance of the gene-wide and GWAS-informed analysis using the Benjamini and Hochberg method to adjust for the false discovery rate (FDR) [63]. All analyses were performed by using R [64].
Enrichment analyses
We identified a list of genes previously determined to be related to sleep and circadian phenotypes in GWAS [13,14,15,16]; thus, the intragenic sites were categorized into gene-wide sites and GWAS-informed sites. Gene-set enrichment was assessed with a hypergeometric test and a permutation test with 1000 permutations [65]. These tests compared the distribution of CpG sites, whose methylation level was associated with each sleep measure at p < 0.05 level intragenic to gene-wide and GWAS-informed genes. To test for functional enrichment of significant sites, we performed gene ontology (GO) pathway analysis on genes annotated to CpGs with significant FDR [63] adjusted p-values (i.e., q-values) using the limma package in R [66].
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Carskadon MA. Patterns of sleep and sleepiness in adolescents. Pediatrician. 1990;17(1):5–12.
Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed phase in adolescence. Sleep Med. 2007;8(6):602–12.
de Zambotti M, Goldstone A, Forouzanfar M, Javitz H, Claudatos S, Colrain IM, et al. The falling asleep process in adolescents. Sleep. 2019;43(6):312.
Bal C, Öztürk A, Çiçek B, Özdemir A, Zararsız G, Ünalan D, et al. The relationship between blood pressure and sleep duration in Turkish children: a cross-sectional study. J Clin Res Pediatr Endocrinol. 2018;10(1):51–8.
de Zambotti M, Goldstone A, Colrain IM, Baker FC. Insomnia disorder in adolescence: diagnosis, impact, and treatment. Sleep Med Rev. 2018;39:12–24.
Fernandez-Mendoza J, Calhoun SL, Vgontzas AN, Li Y, Gaines J, Liao D, et al. Insomnia phenotypes based on objective sleep duration in adolescents: depression risk and differential behavioral profiles. Brain Sci. 2016;6(4):E59.
Liu JW, Tu YK, Lai YF, Lee HC, Tsai PS, Chen TJ, et al. Associations between sleep disturbances and suicidal ideation, plans, and attempts in adolescents: a systematic review and meta-analysis. Sleep. 2019;42(6):zsz054.
Meltzer LJ, Williamson AA, Mindell JA. Pediatric sleep health: It matters, and so does how we define it. Sleep Med Rev. 2021;57: 101425.
Dregan A, Armstrong D. Adolescence sleep disturbances as predictors of adulthood sleep disturbances—a cohort study. J Adolesc Health. 2010;46(5):482–7.
Armstrong D, Dregan A. A population-based investigation into the self-reported reasons for sleep problems. PLoS ONE. 2014;9(7): e101368.
Fernandez-Mendoza J, Lenker KP, Calhoun SL, Qureshi M, Ricci A, Bourchtein E, et al. Trajectories of insomnia symptoms from childhood through young adulthood. Pediatrics. 2022;149(3): e2021053616.
Jagannath A, Taylor L, Wakaf Z, Vasudevan SR, Foster RG. The genetics of circadian rhythms, sleep and health. Hum Mol Genet. 2017;26(R2):R128–38.
Jones SE, van Hees VT, Mazzotti DR, Marques-Vidal P, Sabia S, van der Spek A, et al. Genetic studies of accelerometer-based sleep measures yield new insights into human sleep behaviour. Nat Commun. 2019;10(1):1585.
Dashti HS, Jones SE, Wood AR, Lane JM, van Hees VT, Wang H, et al. Genome-wide association study identifies genetic loci for self-reported habitual sleep duration supported by accelerometer-derived estimates. Nat Commun. 2019;10(1):1100.
Nishiyama T, Nakatochi M, Goto A, Iwasaki M, Hachiya T, Sutoh Y, et al. Genome-wide association meta-analysis and Mendelian randomization analysis confirm the influence of ALDH2 on sleep durationin the Japanese population. Sleep. 2019;42(6):zsz046.
Doherty A, Smith-Byrne K, Ferreira T, Holmes MV, Holmes C, Pulit SL, et al. GWAS identifies 14 loci for device-measured physical activity and sleep duration. Nat Commun. 2018;9(1):5257.
Hurley JM, Loros JJ, Dunlap JC. Circadian oscillators: around the transcription-translation feedback loop and on to output. Trends Biochem Sci. 2016;41(10):834–46.
Troynikov O, Watson CG, Nawaz N. Sleep environments and sleep physiology: a review. J Therm Biol. 2018;78:192–203.
Morales-Lara D, De-la-Peña C, Murillo-Rodríguez E. Dad’s snoring may have left molecular scars in your DNA: the emerging role of epigenetics in sleep disorders. Mol Neurobiol. 2018;55(4):2713–24.
Law PP, Holland ML. DNA methylation at the crossroads of gene and environment interactions. Essays Biochem. 2019;63(6):717–26.
Cortese R. Epigenetics of sleep disorders: an emerging field in diagnosis and therapeutics. Diagn Basel Switz. 2021;11(5):851.
Kim H, Wang X, Jin P. Developing DNA methylation-based diagnostic biomarkers. J Genet Genomics Yi Chuan Xue Bao. 2018;45(2):87–97.
Qureshi IA, Mehler MF. Epigenetics of sleep and chronobiology. Curr Neurol Neurosci Rep. 2014;14(3):432.
White AJ, Kresovich JK, Xu Z, Sandler DP, Taylor JA. Shift work, DNA methylation and epigenetic age. Int J Epidemiol. 2019;48(5):1536–44.
Nanduri J, Semenza GL, Prabhakar NR. Epigenetic changes by DNA methylation in chronic and intermittent hypoxia. Am J Physiol-Lung Cell Mol Physiol. 2017;313(6):L1096–100.
Liu HC, Hu CJ, Tang YC, Chang JG. A pilot study for circadian gene disturbance in dementia patients. Neurosci Lett. 2008;435(3):229–33.
Rotter A, Asemann R, Decker A, Kornhuber J, Biermann T. Orexin expression and promoter-methylation in peripheral blood of patients suffering from major depressive disorder. J Affect Disord. 2011;131(1):186–92.
Lin Q, Ding H, Zheng Z, Gu Z, Ma J, Chen L, et al. Promoter methylation analysis of seven clock genes in Parkinson’s disease. Neurosci Lett. 2012;507(2):147–50.
Gaine ME, Chatterjee S, Abel T. Sleep deprivation and the epigenome. Front Neural Circuits. 2018. https://doi.org/10.3389/fncir.2018.00014.
Lahtinen A, Puttonen S, Vanttola P, Viitasalo K, Sulkava S, Pervjakova N, et al. A distinctive DNA methylation pattern in insufficient sleep. Sci Rep. 2019;9(1):1193.
Sammallahti S, Koopman-Verhoeff ME, Binter AC, Mulder RH, Cabré-Riera A, Kvist T, et al. Longitudinal associations of DNA methylation and sleep in children: a meta-analysis. Clin Epigenetics. 2022;14(1):83.
Huang H, Zhu Y, Eliot MN, Knopik VS, McGeary JE, Carskadon MA, et al. Combining human epigenetics and sleep studies in caenorhabditis elegans: a cross-species approach for finding conserved genes regulating sleep. Sleep. 2017;40(6):zsx063.
Jansen EC, Dolinoy DC, O’Brien LM, Peterson KE, Chervin RD, Banker M, et al. Sleep duration and fragmentation in relation to leukocyte DNA methylation in adolescents. Sleep. 2019;42(9):zsz121.
Koopman-Verhoeff ME, Mulder RH, Saletin JM, Reiss I, van der Horst GTJ, Felix JF, et al. Genome-wide DNA methylation patterns associated with sleep and mental health in children: a population-based study. J Child Psychol Psychiatry. 2020;61(10):1061–9.
Matthews KA, Patel SR, Pantesco EJ, Buysse DJ, Kamarck TW, Lee L, et al. Similarities and differences in estimates of sleep duration by polysomnography, actigraphy, diary, and self-reported habitual sleep in a community sample. Sleep Health. 2018;4(1):96–103.
Hu Y, Shmygelska A, Tran D, Eriksson N, Tung JY, Hinds DA. GWAS of 89,283 individuals identifies genetic variants associated with self-reporting of being a morning person. Nat Commun. 2016;2(7):10448.
Poisson A, Nicolas A, Bousquet I, Raverot V, Gronfier C, Demily C. Smith-Magenis syndrome: molecular basis of a genetic-driven melatonin circadian secretion disorder. Int J Mol Sci. 2019;20(14):3533.
Panda S. Circadian physiology of metabolism. Science. 2016;354(6315):1008–15.
Kim CE, Shin S, Lee HW, Lim J, Lee JK, Shin A, et al. Association between sleep duration and metabolic syndrome: a cross-sectional study. BMC Public Health. 2018;18(1):720.
Tobaldini E, Costantino G, Solbiati M, Cogliati C, Kara T, Nobili L, et al. Sleep, sleep deprivation, autonomic nervous system and cardiovascular diseases. Neurosci Biobehav Rev. 2017;74(Pt B):321–9.
Vgontzas AN, Fernandez-Mendoza J, Liao D, Bixler EO. Insomnia with objective short sleep duration: the most biologically severe phenotype of the disorder. Sleep Med Rev. 2013;17(4):241–54.
He L, Hamm JA, Reddy A, Sams D, Peliciari-Garcia RA, McGinnis GR, et al. Biotinylation: a novel posttranslational modification linking cell autonomous circadian clocks with metabolism. Am J Physiol Heart Circ Physiol. 2016;310(11):H1520-1532.
Richards J, Ko B, All S, Cheng KY, Hoover RS, Gumz ML. A role for the circadian clock protein Per1 in the regulation of the NaCl co-transporter (NCC) and the with-no-lysine kinase (WNK) cascade in mouse distal convoluted tubule cells. J Biol Chem. 2014;289(17):11791–806.
He Z, Zhang R, Jiang F, Zhang H, Zhao A, Xu B, et al. FADS1-FADS2 genetic polymorphisms are associated with fatty acid metabolism through changes in DNA methylation and gene expression. Clin Epigenetics. 2018;10(1):113.
Winkelman JW, de Lecea L. Sleep and neuropsychiatric illness. Neuropsychopharmacol Off Publ Am Coll Neuropsychopharmacol. 2020;45(1):1–2.
Braun PR, Han S, Hing B, Nagahama Y, Gaul LN, Heinzman JT, et al. Genome-wide DNA methylation comparison between live human brain and peripheral tissues within individuals. Transl Psychiatry. 2019;31(9):47.
Howard DM, Adams MJ, Clarke TK, Hafferty JD, Gibson J, Shirali M, et al. Genome-wide meta-analysis of depression identifies 102 independent variants and highlights the importance of the prefrontal brain regions. Nat Neurosci. 2019;22(3):343–52.
Clarkson-Townsend DA, Everson TM, Deyssenroth MA, Burt AA, Hermetz KE, Hao K, et al. Maternal circadian disruption is associated with variation in placental DNA methylation. PLoS ONE. 2019;14(4): e0215745.
Antypa N, Vogelzangs N, Meesters Y, Schoevers R, Penninx BWJH. Chronotype associations with depression and anxiety disorders in a large cohort study. Depress Anxiety. 2016;33(1):75–83.
Meier SM, Trontti K, Purves KL, Als TD, Grove J, Laine M, et al. Genetic variants associated with anxiety and stress-related disorders: a genome-wide association study and mouse-model study. JAMA Psychiat. 2019;76(9):924–32.
Roberts AL, Gladish N, Gatev E, Jones MJ, Chen Y, MacIsaac JL, et al. Exposure to childhood abuse is associated with human sperm DNA methylation. Transl Psychiatry. 2018;8(1):194.
Rautiainen MR, Paunio T, Repo-Tiihonen E, Virkkunen M, Ollila HM, Sulkava S, et al. Genome-wide association study of antisocial personality disorder. Transl Psychiatry. 2016;6(9): e883.
Lee JJ, Wedow R, Okbay A, Kong E, Maghzian O, Zacher M, et al. Gene discovery and polygenic prediction from a genome-wide association study of educational attainment in 1.1 million individuals. Nat Genet. 2018;50(8):1112–21.
Kravchick DO, Karpova A, Hrdinka M, Lopez-Rojas J, Iacobas S, Carbonell AU, et al. Synaptonuclear messenger PRR7 inhibits c-Jun ubiquitination and regulates NMDA-mediated excitotoxicity. EMBO J. 2016;35(17):1923–34.
Bixler EO, Vgontzas AN, Lin HM, Liao D, Calhoun S, Fedok F, et al. Blood pressure associated with sleep-disordered breathing in a population sample of children. Hypertens Dallas Tex 1979. 2008;52(5):841–6.
Bixler EO, Fernandez-Mendoza J, Liao D, Calhoun S, Rodriguez-Colon SM, Gaines J, et al. Natural history of sleep disordered breathing in prepubertal children transitioning to adolescence. Eur Respir J. 2016;47(5):1402–9.
He F, Bixler EO, Liao J, Berg A, Imamura Kawasawa Y, Fernandez-Mendoza J, et al. Habitual sleep variability, mediated by nutrition intake, is associated with abdominal obesity in adolescents. Sleep Med. 2015;16(12):1489–94.
Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC. The age of adolescence. Lancet Child Adolesc Health. 2018;2(3):223–8.
Iber C, Ancoli-Israel S, Chesson A, Quan S. The AASM manual for the scoring of sleep and associated events: rules, ter minology and technical specifications. Westchester, IL: American Academy of Sleep Medicine; 2007.
Sun YW, El-Bayoumy K, Imamura Kawasawa Y, Salzberg A, Aliaga C, Gowdahalli K, et al. Abstract 4454: genome-wide analysis of DNA methylation induced by environmental carcinogen dibenzo[def, p]chrysene in ovarian tissues of mice. Cancer Res. 2016;76:4454.
He F, Berg A, Imamura Kawasawa Y, Bixler EO, Fernandez-Mendoza J, Whitsel EA, et al. Association between DNA methylation in obesity-related genes and body mass index percentile in adolescents. Sci Rep. 2019;9(1):2079.
Carlson M, Maintainer BP. TxDb.Hsapiens.UCSC.hg19.knownGene: Annotation package for TxDb object(s). R package version 3.2.2. 2015
Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Ser B Methodol. 1995;57(1):289–300.
R Core Team. R: A language and environment for statistical computing [Internet]. Vienna, Austria: R Foundation for Statistical Computing; 2021. https://www.R-project.org/
Goeman JJ, Bühlmann P. Analyzing gene expression data in terms of gene sets: methodological issues. Bioinforma Oxf Engl. 2007;23(8):980–7.
Ritchie ME, Phipson B, Wu D, Hu Y, Law CW, Shi W, et al. Limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 2015;43(7):e47–e47.
Acknowledgements
Not applicable
Funding
NIH Awards Number R01HL136587, R01MH118308, R01HL97165, R01HL63772, UL1TR000127.
Author information
Authors and Affiliations
Contributions
ML ran the linear regression and enrichment analysis and interpreted the results and was a major contributor in writing the manuscript. FH processed the DNA methylation datasets and contributed to statistical analyses. YIK performed DNA methylation assays. AB was involved with the processing the DNA methylation dataset. ANV was a major contributor in writing the manuscript. DL secured funding and was involved in the study design, data collection, and supervised statistical analyses. EOB secured funding and was involved with the design and recruitment of the participants. JFM secured funding and was involved in the study design, data collection, and was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
For all data and samples collected, written informed consent from the parent/legal guardian and participants 18 years or older, and assent from those younger than 18, were all obtained. The study was approved by Penn State Institutional Review Board.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Table S1: Enrichment Analysis p-values and Supplementary
Additional file 2.
Significant results for the all-gene and GWAS-informed analyses.Significant Pathway Analysis Results.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Larsen, M., He, F., Kawasawa, Y.I. et al. Objective and subjective measures of sleep initiation are differentially associated with DNA methylation in adolescents. Clin Epigenet 15, 136 (2023). https://doi.org/10.1186/s13148-023-01553-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13148-023-01553-2