
Abstract
Background
High dietary glycaemic index (GI) and load (GL) have been associated with increased risk of various cardiometabolic conditions. Among the molecular potential mechanisms underlying this relationship, DNA methylation has been studied, but a direct link between high GI and/or GL of diet and global DNA methylation levels has not been proved yet. We analyzed the associations between GI and GL and global DNA methylation patterns within an Italian population.
Results
Genomic DNA methylation (5mC) and hydroxymethylation (5hmC) levels were measured in 1080 buffy coat samples from participants of the Moli-sani study (mean(SD) = 54.9(11.5) years; 52% women) via ELISA. A 188-item Food Frequency Questionnaire was used to assess food intake and dietary GI and GL for each participant were calculated. Multiple linear regressions were used to investigate the associations between dietary GI and GL and global 5mC and 5hmC levels, as well as the proportion of effect explained by metabolic and inflammatory markers. We found negative associations of GI with both 5mC (β (SE) = − 0.073 (0.027), p = 0.007) and 5hmC (− 0.084 (0.030), p = 0.006), and of GL with 5mC (− 0.14 (0.060), p = 0.014). Circulating biomarkers did not explain the above-mentioned associations. Gender interaction analyses revealed a significant association of the gender-x-GL interaction with 5mC levels, with men showing an inverse association three times as negative as in women (interaction β (SE) = − 0.16 (0.06), p = 0.005).
Conclusions
Our findings suggest that global DNA methylation and hydroxymethylation patterns represent a biomarker of carbohydrate intake. Based on the differential association of GL with 5mC between men and women, further gender-based separate approaches are warranted.
Similar content being viewed by others

Background
Excessive intake of carbohydrates favoring higher glucose levels has been extensively linked to clinical outcomes including cardiometabolic diseases [1] and neurological disorders [2]. Indeed, increasing evidence in population studies supports a strong relationship between quality and quantity of carbohydrates ingested with foods and increased risk of certain types of cancers [3, 4], diabetes [5, 6] and cardiovascular diseases [7,8,9]. This is likely explained through carbohydrates’ direct implications in regulating blood glucose levels, as well as in changing postprandial hormonal and metabolic responses in humans [10]. For these reasons, increasing attention has been given in the last decades to control the quantity and quality of carbohydrates’ dietary intake in clinical practice, through specific indices.
Among these, glycaemic index (GI) and glycaemic load (GL) represent two common dietary indices increasingly used to measure and control carbohydrate intake in people affected by cardiometabolic disorders, like diabetes [11]. GI [12], generally calculated from International GI tables [13, 14], is a measure of carbohydrate quality and refers to the postprandial blood glucose increase in response to a given carbohydrate intake, when compared with a reference food (either glucose or white bread). GL represents instead an indicator of both quality and quantity of carbohydrates and is calculated by multiplying the GI of a food item with the available carbohydrate content [11]. While both higher GI and higher GL have been associated with increased disease risk [3,4,5,6,7,8,9], their relationship with potential molecular mechanisms underlying cardiometabolic dysfunction remains largely neglected.
Altered DNA methylation patterns, particularly the level of methylation (5mC) and hydroxymethylation (5hmC) in the genome, have been often associated with type 2 diabetes (T2D) and with a general oxidative stress status [15,16,17,18].
Investigations focusing on the relationship between DNA methylation patterns and dietary GI and GL mainly consist of interventional studies on maternal dietary habits, aimed at detecting methylation changes in the offspring [19]. Geraghty et al. [20] analyzed DNA methylation levels at 771,484 CpGs sites across the genome in free DNA from cord blood serum in 60 newborns involved in the ROLO study. The methylome of low GI intervention newborns was found to be significantly lower than in controls [20]. By comparing two groups of pregnant women following a reduced vs. an increased carbohydrate diet, Yan et al. observed specific placenta DNA methylation changes at genes involved in insulin regulation, namely PLIN1, CPT1B, SSTR4 and CIDEA [21]. In a recent observational study, Alick et al. [22] found out that a maternal periconceptional diet characterized by a high glycaemic loading was associated with poorer neurodevelopmental status of children, in particular anxiety-related behavior, and with an increased mean methylation level of the imprint control region of SGCE/PEG10.
In spite of these suggestive independent lines of evidence, we are not aware of any study so far investigating the relationship between global methylation patterns and glycaemic index and load of diet, assessing both measures in the same subjects. Such a design would help in (1) building a closer relationship between nutritional and genome methylation patterns and (2) identifying the potential implications of dietary habits, which are of remarkable importance for cardiometabolic patients, on novel epigenetic measures.
In the present study, we aimed at investigating the associations between both GI and GL and global DNA methylation within an Italian population cohort enrolled in the Moli-sani study. We already reported a fine-grained analysis of global DNA methylation patterns at different nutritional levels in the same cohort, identifying a direct relationship between daily intake of zinc and global DNA methylation [23]. Here, we focused on dietary glycaemic indices to build a bridge with altered epigenetic patterns potentially underlying metabolic conditions.
Results
The characteristics of the analyzed sub-cohort (N = 1080 with at least an epigenetic measure available) are summarized elsewhere [23] and in Table 1. Compared to the whole Moli-sani cohort, the population under study showed similar sex ratio (48.0% vs 48.1% men) but slightly lower age (mean (SD) age 54.9 (11.5) year vs 55.8 (12.0) years, p < 0.0001), due to the removal of prevalent CVD cases. Similarly, in the analyzed sub-cohort there was a lower prevalence of diabetes (3.6% vs 5.0%, p = 0.02) and hyperlipidemia (4.2% vs 7.9%), as well as a higher energy intake (2210.19 kcal/d vs 2079.01 kcal/d, p < 0.0001). Overall, there was no systematic difference between the analyzed sub-cohort and the whole Moli-sani population, except those due to removal of individuals with history of CVD.
Association analyses of glycaemic parameters in the analyzed sub-cohort (Table 2) revealed significant negative associations of GI with both 5mC (standardized β (Standard Error) = − 0.073 (0.027), p = 0.007) and 5hmC (β (SE) = − 0.084 (0.030), p = 0.006) measured on buffy coat samples from the studied subjects. A significant negative association was also observed between GL and 5mC (β (SE) = − 0.146 (0.060), p = 0.015), but not with 5hmC. These associations remained significant after additional adjustments for other potential confounding factors like use of metformin (Additional file 1: Table S1).
In the mediation analysis of different circulating biomarkers—including C-reactive protein (CRP), glucose, C-peptide, insulin, total cholesterol, LDL, HDL—no significant proportion of the above- mentioned associations was explained by any of the circulating markers tested (Table 3).
Gender interaction analyses revealed a significant association of the interaction term between gender and glycaemic load with 5mC levels (interaction β (SE) = − 0.16 (0.06), p = 0.005), with men showing an inverse association more than three times as large as in women (Table 4). No other significant interactive associations were detected.
Discussion
Here we report, for the first time, a concordant negative association between two measurements reflecting carbohydrates’ quality and quantity (GI and GL), and global methylation levels measured within the same subjects from a general population. These associations resisted correction for several factors influencing hypomethylation, including use of metformin [24, 25] or self-reported diabetic status.
Nutritional factors, among all the environmental stimuli, can affect epigenetics both transiently and chronically [26,27,28]. The specific epigenetic changes caused by sustained hyperglycaemia are the basis for the establishment of the so-called metabolic memory [29] and are the means by which exposure to high glucose exerts its long-lasting detrimental effects on human health in the context of cancer [30], diabetes [31,32,33,34] and CVD [35,36,37]. Global hypomethylation is a generally accepted hallmark of cancer [38]. More controversial are the published studies that consider global DNA methylation levels and CVD or diabetes. However, lower global DNA methylation (5mC), evaluated with a similar technique to the one used in this study, has been generally associated with clinical and subclinical CVD phenotypes including hypertension, atherosclerosis, coronary artery disease and increased CVD risk in postmenopausal women [38,39,40,41,42]. Very few studies have investigated global DNA methylation in the context of diabetes and metabolic syndrome, generally reporting lower 5mC and 5hmC levels [16, 17] although not always consistently [18].
Consuming high GL foods is known to cause an increase in blood glucose and insulin levels with consequent increase in plasma-free fatty acids [43]. All together these factors contribute to lower insulin sensitivity and to the development of dyslipidemia [10, 43, 44]. Though some controversial data have been published on the topic, several observational studies have supported these findings by identifying a direct association between dietary GL and glucose metabolism parameters [45,46,47,48,49,50,51,52]. Based on this, GI and GL have been extensively considered and validated as risk factors for chronic diseases [3,4,5,6,7,8,9]. Therefore, identifying a possible molecular mechanism linking these variables to health outcomes could bare important opportunities to identify a novel marker for clinical risk assessment.
Higher GI and GL in the studied Moli-sani sub-cohort were associated with lower global methylation and hydroxymethylation levels in the genome. Although to our knowledge there are no such comparable studies in the field, we evaluated our findings in relation to previous studies on the link between T2D and genomic methylation patterns. Indeed, our observations are partly concordant with previous epidemiological evidence of lower hydroxymethylation levels found in diabetic patients compared to controls and with the functional evidence that glucose treatment increases 5hmC levels in specific cell lines like PBMCs, HUVECs and TF-1 [16]. This mechanism is mediated by downregulation of TET2 (ten-eleven translocation 2 protein) levels, an enzyme involved in the conversion of 5-methylcytosine into 5-hydroxymethylcytosine in the genome. This effect is counterbalanced by metformin treatment, which increases TET2 stability and 5hmC levels [16]. Our findings are also in line with previous reports of decreased 5mC levels in T2D patients compared to controls, also after adjustment for use of metformin. Conversely, contrasting evidence of higher 5mC and 5hmC levels in peripheral blood cells of poorly controlled compared to well-controlled diabetic patients and healthy controls has been reported [18]. Moreover, the lack of evidence of mediation by glucose, insulin and C-peptide in the link between dietary glycaemic indices and methylation patterns suggests that other biomarkers should be investigated to explain the significant associations observed here. Therefore, further studies aimed at disentangling the link between dietary glycaemic parameters and altered genomic methylation are needed to clarify the mechanisms linking nutrition, methylation patterns and diabetes-related traits.
Another interesting finding in our study was that some of the significant associations observed were not concordant between genders. Prominently, the decrease in methylation levels per SD increase of glycaemic load was more than three times as negative in men compared to women. If supported by independent studies, these findings may open a gender-based perspective on the investigation of potential effects of dietary glycaemic quantity, with immediate translational implications for the control of carbohydrate intake in patients also based on their gender. In view of the known link between metabolic and cardiovascular diseases [7,8,9], 5hmC could represent a specific novel marker for cardiometabolic risk prediction in women.
Limitations and implications for future studies
Although this study has the merit to provide a contribution to the molecular epidemiology of the relationship between DNA methylation and glucose-related dietary patterns, an aspect very scarcely investigated yet in the field of nutrigenomics, we need to acknowledge some limitations of the present work. The FFQ used in this study was not specifically designed to evaluate dietary GI and GL, but to provide estimates of total carbohydrate and total energy intake. Furthermore, GI and GL estimates derived from FFQs may not take into account several factors that can influence the postprandial glycaemic response, such as varying meal frequency, varying cooking methods or chewing habits. Also, dietary data were self-reported and this may lead to recall bias. Similarly, the cross-sectional setting does not allow to establish clear directionality of effect between glycaemic parameters and epigenetic modifications, nor does it give any precise information linking glycaemic nutritional parameters, altered methylation patterns and chronic disease risk. Also, the possibility of residual confounding by unmeasured factors cannot be fully excluded. This—along with the low number of T2D cases (< 40) in the analyzed sub-cohort—did not allow to test potential mediation effects of methylation patterns in the link between dietary parameters and diabetes, which was instead used as a covariate. Finally, our global measure of DNA methylation/hydroxymethylation does not allow to further explore potential mechanisms linking a specific gene or pathway to quality and quantity of carbohydrate intake, which makes it difficult to understand the functional meaning of these associations.
Conclusions
This study represents, to the best of our knowledge, the first attempt to investigate the relationship between methylation patterns in the genome and dietary glycaemic parameters in the same individual from an adult population cohort. Our findings suggest that global DNA methylation and hydroxymethylation patterns can be used as biomarkers of carbohydrate intake. Further approaches are necessary to better understand the gender-based potential effects of dietary GI and GL.
Methods
Study population
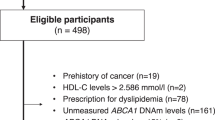
The study population was already described in Noro et al. [23] and composed of a randomly selected sub-cohort of 1,160 participants of the Moli-sani study (N = 24,325; 49.20% men; age ≥ 35 years, recruited between 2005 and 2010) [53, 54]. Subjects with incomplete dietary questionnaires or with missing values in the studied variables were excluded from the analysis to a final number of 1080 subjects.
DNA extraction and global DNA methylation assessment
We used a silica matrix-based method to extract buffy coat DNA as described in [55]. Out of the original 1160 DNA samples, 1140 were selected based on their DNA quality to be further used in the methylation study (see below). We used the MethylFlash Global DNA Methylation (5mC) ELISA Easy Kit (colorimetric) and the MethylFlash Hydroxymethylated DNA 5hmC Quantification Kit (colorimetric) (EpiGentek), according to the manufacturer’s instructions, to assess global levels of 5-methylcytosine (5mC) and 5-hydroxymethylcytosine (5hmC), respectively. DNA methylation quality control and statistical analyses were performed using R (The R Project, 2020; https://www.r-project.org/).
We overall measured 5mC and 5hmC global levels for 1214 samples (including 1,140 original and 74 duplicate samples). Of these, samples with absorbance optical density (OD) values below the mean of negative controls plus 2 standard deviations (SDs) for both global methylation measurements were set to missing as described [23]. We additionally excluded: (1) 17 and 2 outlier samples for 5mC and 5hmC, respectively, defined as samples with absolute values of standardized methylation levels above 3 standard deviations; and (2) all prevalent CVD cases (56 and 58 samples for 5mC and 5hmC, respectively) to exclude reverse causality of CVD on methylation levels [56]. Finally, 1067 samples for 5mC and 1075 samples for 5hmC were used in the following statistical analyses. 5mC and 5hmC showed a modest but significant inverse correlation (Pearson’s r = − 0.21, p = 1.1 × 10–11). For both 5mC and 5hmC, the study population distributions were approaching normality (Additional file 1: Figure S1a, b).
Dietary assessment and calculation of dietary glycaemic index and load
Food intake during the year before enrollment was assessed by the Italian version of the semiquantitative EPIC food frequency questionnaire (FFQ) [57]. The FFQ contains 14 sections (i.e., pasta/rice, soup, meat (excluding salami and other cured meats), fish, raw vegetables, cooked vegetables, eggs, sandwiches, salami and other cured meats, cheese, fruit, bread/wine, milk/coffee/cakes and herbs/spices) with 248 questions concerning 188 different food items.
Frequencies and quantities of each food were linked to Italian Food Tables [58] using a specifically designed software in order to obtain estimates of daily intake of macro- and micronutrients plus energy.
The average dietary GI for each volunteer was calculated as the sum of the GIs of each food item consumed, multiplied by the average daily amount consumed and the percentage of carbohydrate content, all divided by the total daily carbohydrate intake. The GL was calculated similarly except that there was no division by total carbohydrate intake.
Generally, the more digestible a carbohydrate is, the higher its GI will be. Some carbohydrates are absorbed quickly and lead to rapid rise in blood glucose (high GI), while others release glucose more slowly (low GI).
The glycaemic load (GL), instead, was calculated by multiplying the GI of each specific food for its total carbohydrate content (g), then dividing by 100 [59]. GL is therefore meant to represent the actual increase of blood glucose caused by ingesting a given quantity of carbohydrates contained in a portion of food.
Dietary GI and GL for each study participant were calculated as the sum of the GIs and GLs of all foods consumed in the diet [60]. GI and GL showed a modest positive correlation (r = 0.13, p = 1.3 × 10–5) and were their distributions approached normality in the population under study (Additional file 1: Figure S2a, b).
Covariates assessment and selection
Several covariates were considered or tested as potential confounders of the relationship between glycaemic index (GI) and load (GL) and global DNA methylation levels (5mC/5hmC).
Among them, sex and age were selected by default, since they are typical confounding factors which influence both methylation measures [61, 62] and nutritional patterns [63]. Similarly, energy intake (kcal/day) was included because also the amount of eaten food might influence participant methylation levels [64], as was educational attainment (defined as completed school level: primary, lower, upper secondary and post-secondary), which is associated with both methylation [65] and nutritional patterns [66]. White blood cell (granulocytes, monocytes, lymphocytes) fractions were also included by default to account for their heterogeneity, since global DNA methylation was measured on DNA extracted from these cells.
Other variables—including smoking habits, leisure time physical activity, abdominal obesity, alcohol intake, diabetes, hyperlipidaemia and cancer (as defined previously)—were added to the models since they showed a univariate trend of association with both the nutritional exposure and the methylation outcome (p < 0.2). The definition of covariates is reported in Additional file 1.
Statistical analyses
Statistical analyses were carried out in R (https://www.r-project.org/). The association between GI and GL of diet (exposures) and standardized global methylation levels (outcome) was analyzed through linear regressions (lm() function in R), separately for 5mC and 5hmC, adjusting for different potential confounders of these relationship, which included age, sex and educational attainment, white blood cell fractions, smoking, leisure time physical activity, abdominal obesity, alcohol intake, prevalent diabetes, hyperlipidaemia and cancer (see Supplementary Methods for definitions and details on selection).
Sensitivity analyses were carried out to disentangle significant associations detected, through further adjusting them for use of metformin—an antidiabetic drug with known altering effects on DNA methylation (24)—so as to ensure that the detected associations were independent from this factor.
Moreover, we performed mediation analyses through the mediate function of the mediation package (https://cran.r-project.org/web/packages/mediation/), to estimate the proportion of association between dietary glycaemic indices (GI and GL) and methylation measures (5mC/5hmC) explained by different circulating biomarkers, including high sensitivity C-reactive protein (CRP, tagging circulating inflammation), glucose, insulin and C-peptide levels (tagging glucose homeostasis) and total, LDL and HDL cholesterol.
Similarly, we performed gender interaction association analyses for both exposures and both outcomes mentioned above, to detect potential gender-specific associations.
Availability of data and materials
The data underlying this article will be shared on reasonable request to the corresponding author. The data are stored in an institutional repository (https://repository.neuromed.it) and access is restricted by the ethical approvals and the legislation of the European Union.
Abbreviations
- 5mC:
-
5-Methylcitosine
- 5hmC:
-
5-Hydroxymethylcitosine
- CRP:
-
C-reactive protein
- CVD:
-
Cardiovascular disease
- FFQ:
-
Food frequency questionnaire
- GI:
-
Glycaemic index
- GL:
-
Glycaemic load
- HDL:
-
High-density lipoprotein
- LDL:
-
Low-density lipoprotein
- MDS:
-
Mediterranean Diet Score
- OD:
-
Optical density
- SD:
-
Standard deviation
- T2D:
-
Type 2 diabetes
- TET:
-
Ten-eleven translocation protein
References
Sievenpiper JL. Low-carbohydrate diets and cardiometabolic health: the importance of carbohydrate quality over quantity. Nutr Rev. 2020;78(Suppl 1):69–77.
Carneiro L, Leloup C. Mens Sana in Corpore Sano: does the glycemic index have a role to play? Nutrients. 2020;12(10):2989.
Long T, Liu K, Long J, Li J, Cheng L. Dietary glycemic index, glycemic load and cancer risk: a meta-analysis of prospective cohort studies. Eur J Nutr. 2022.
Turati F, Galeone C, Augustin LSA, La Vecchia C. Glycemic index, glycemic load and cancer risk: an updated meta-analysis. Nutrients. 2019;11(10):2342.
Bhupathiraju SN, Tobias DK, Malik VS, Pan A, Hruby A, Manson JE, et al. Glycemic index, glycemic load, and risk of type 2 diabetes: results from 3 large US cohorts and an updated meta-analysis. Am J Clin Nutr. 2014;100(1):218–32.
Livesey G, Taylor R, Livesey HF, Buyken AE, Jenkins DJA, Augustin LSA, et al. Dietary glycemic index and load and the risk of type 2 diabetes: a systematic review and updated meta-analyses of prospective cohort studies. Nutrients. 2019;11(6):1280.
Mirrahimi A, Chiavaroli L, Srichaikul K, Augustin LS, Sievenpiper JL, Kendall CW, et al. The role of glycemic index and glycemic load in cardiovascular disease and its risk factors: a review of the recent literature. Curr Atheroscler Rep. 2014;16(1):381.
Jayedi A, Soltani S, Jenkins D, Sievenpiper J, Shab-Bidar S. Dietary glycemic index, glycemic load, and chronic disease: an umbrella review of meta-analyses of prospective cohort studies. Crit Rev Food Sci Nutr. 2020:1–10.
Dwivedi AK, Dubey P, Reddy SY, Clegg DJ. Associations of glycemic index and glycemic load with cardiovascular disease: updated evidence from meta-analysis and cohort studies. Curr Cardiol Rep. 2022.
Ludwig DS. The glycemic index: physiological mechanisms relating to obesity, diabetes, and cardiovascular disease. JAMA. 2002;287(18):2414–23.
Willett W, Manson J, Liu S. Glycemic index, glycemic load, and risk of type 2 diabetes. Am J Clin Nutr. 2002;76(1):274S-S280.
Jenkins DJ, Wolever TM, Taylor RH, Barker H, Fielden H, Baldwin JM, et al. Glycemic index of foods: a physiological basis for carbohydrate exchange. Am J Clin Nutr. 1981;34(3):362–6.
Atkinson FS, Foster-Powell K, Brand-Miller JC. International tables of glycemic index and glycemic load values: 2008. Diabetes Care. 2008;31(12):2281–3.
Atkinson FS, Brand-Miller JC, Foster-Powell K, Buyken AE, Goletzke J. International tables of glycemic index and glycemic load values 2021: a systematic review. Am J Clin Nutr. 2021;114(5):1625–32.
Wu X, Zhang Y. TET-mediated active DNA demethylation: mechanism, function and beyond. Nat Rev Genet. 2017;18(9):517–34.
Wu D, Hu D, Chen H, Shi G, Fetahu IS, Wu F, et al. Glucose-regulated phosphorylation of TET2 by AMPK reveals a pathway linking diabetes to cancer. Nature. 2018;559(7715):637–41.
Luttmer R, Spijkerman AM, Kok RM, Jakobs C, Blom HJ, Serne EH, et al. Metabolic syndrome components are associated with DNA hypomethylation. Obes Res Clin Pract. 2013;7(2):e106–15.
Pinzon-Cortes JA, Perna-Chaux A, Rojas-Villamizar NS, Diaz-Basabe A, Polania-Villanueva DC, Jacome MF, et al. Effect of diabetes status and hyperglycemia on global DNA methylation and hydroxymethylation. Endocr Connect. 2017;6(8):708–25.
Lecorguille M, Teo S, Phillips CM. Maternal dietary quality and dietary inflammation associations with offspring growth, placental development, and DNA methylation. Nutrients. 2021;13(9):3130.
Geraghty AA, Sexton-Oates A, O’Brien EC, Alberdi G, Fransquet P, Saffery R, et al. A low glycaemic index diet in pregnancy induces DNA methylation variation in blood of newborns: results from the ROLO randomised controlled trial. Nutrients. 2018;10(4):455.
Yan W, Zhang Y, Wang L, Yang W, Li C, Wang L, et al. Maternal dietary glycaemic change during gestation influences insulin-related gene methylation in the placental tissue: a genome-wide methylation analysis. Genes Nutr. 2019;14:17.
Alick CL, Maguire RL, Murphy SK, Fuemmeler BF, Hoyo C, House JS. Periconceptional maternal diet characterized by high glycemic loading is associated with offspring behavior in NEST. Nutrients. 2021;13(9):3180.
Noro F, Marotta A, Bonaccio M, Costanzo S, Santonastaso F, Orlandi S, et al. Fine-grained investigation of the relationship between human nutrition and global DNA methylation patterns. Eur J Nutr. 2021;61:1231–43.
Elbere I, Silamikelis I, Ustinova M, Kalnina I, Zaharenko L, Peculis R, et al. Significantly altered peripheral blood cell DNA methylation profile as a result of immediate effect of metformin use in healthy individuals. Clin Epigenetics. 2018;10(1):156.
Solomon WL, Hector SBE, Raghubeer S, Erasmus RT, Kengne AP, Matsha TE. Genome-wide DNA methylation and LncRNA-associated DNA methylation in metformin-treated and -untreated diabetes. Epigenomes. 2020;4(3):19.
Jirtle RL, Skinner MK. Environmental epigenomics and disease susceptibility. Nat Rev Genet. 2007;8(4):253–62.
Portela A, Esteller M. Epigenetic modifications and human disease. Nat Biotechnol. 2010;28(10):1057–68.
Simmons R. Epigenetics and maternal nutrition: nature v. nurture. Proc Nutr Soc. 2011;70(1):73–81.
Berezin A. Metabolic memory phenomenon in diabetes mellitus: achieving and perspectives. Diabetes Metab Syndr. 2016;10(2 Suppl 1):S176–83.
Lee C, An D, Park J. Hyperglycemic memory in metabolism and cancer. Horm Mol Biol Clin Investig. 2016;26(2):77–85.
Sommese L, Zullo A, Mancini FP, Fabbricini R, Soricelli A, Napoli C. Clinical relevance of epigenetics in the onset and management of type 2 diabetes mellitus. Epigenetics. 2017;12(6):401–15.
Intine RV, Sarras MP Jr. Metabolic memory and chronic diabetes complications: potential role for epigenetic mechanisms. Curr Diab Rep. 2012;12(5):551–9.
El-Osta A, Brasacchio D, Yao D, Pocai A, Jones PL, Roeder RG, et al. Transient high glucose causes persistent epigenetic changes and altered gene expression during subsequent normoglycemia. J Exp Med. 2008;205(10):2409–17.
Cooper ME, El-Osta A. Epigenetics: mechanisms and implications for diabetic complications. Circ Res. 2010;107(12):1403–13.
Paneni F, Beckman JA, Creager MA, Cosentino F. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. Eur Heart J. 2013;34(31):2436–43.
Paneni F, Volpe M, Luscher TF, Cosentino F. SIRT1, p66(Shc), and Set7/9 in vascular hyperglycemic memory: bringing all the strands together. Diabetes. 2013;62(6):1800–7.
Costantino S, Ambrosini S, Paneni F. The epigenetic landscape in the cardiovascular complications of diabetes. J Endocrinol Investig. 2019;42(5):505–11.
Wilson AS, Power BE, Molloy PL. DNA hypomethylation and human diseases. Biochim Biophys Acta. 2007;1775(1):138–62.
Soriano-Tarraga C, Jimenez-Conde J, Giralt-Steinhauer E, Mola M, Ois A, Rodriguez-Campello A, et al. Global DNA methylation of ischemic stroke subtypes. PLoS ONE. 2014;9(4): e96543.
Castro R, Rivera I, Struys EA, Jansen EE, Ravasco P, Camilo ME, et al. Increased homocysteine and S-adenosylhomocysteine concentrations and DNA hypomethylation in vascular disease. Clin Chem. 2003;49(8):1292–6.
Nanayakkara PW, Kiefte-de Jong JC, Stehouwer CD, van Ittersum FJ, Olthof MR, Kok RM, et al. Association between global leukocyte DNA methylation, renal function, carotid intima-media thickness and plasma homocysteine in patients with stage 2–4 chronic kidney disease. Nephrol Dial Transplant. 2008;23(8):2586–92.
Ramos RB, Fabris V, Lecke SB, Maturana MA, Spritzer PM. Association between global leukocyte DNA methylation and cardiovascular risk in postmenopausal women. BMC Med Genet. 2016;17(1):71.
Augustin LS, Franceschi S, Jenkins DJ, Kendall CW, La Vecchia C. Glycemic index in chronic disease: a review. Eur J Clin Nutr. 2002;56(11):1049–71.
Aston LM. Glycaemic index and metabolic disease risk. Proc Nutr Soc. 2006;65(1):125–34.
van Aerde MA, Witte DR, Jeppesen C, Soedamah-Muthu SS, Bjerregaard P, Jorgensen ME. Glycemic index and glycemic load in relation to glucose intolerance among Greenland’s Inuit population. Diabetes Res Clin Pract. 2012;97(2):298–305.
Hosseinpour-Niazi S, Sohrab G, Asghari G, Mirmiran P, Moslehi N, Azizi F. Dietary glycemic index, glycemic load, and cardiovascular disease risk factors: Tehran Lipid and Glucose Study. Arch Iran Med. 2013;16(7):401–7.
Murakami K, Sasaki S, Takahashi Y, Okubo H, Hosoi Y, Horiguchi H, et al. Dietary glycemic index and load in relation to metabolic risk factors in Japanese female farmers with traditional dietary habits. Am J Clin Nutr. 2006;83(5):1161–9.
Levitan EB, Cook NR, Stampfer MJ, Ridker PM, Rexrode KM, Buring JE, et al. Dietary glycemic index, dietary glycemic load, blood lipids, and C-reactive protein. Metabolism. 2008;57(3):437–43.
Ma Y, Li Y, Chiriboga DE, Olendzki BC, Hebert JR, Li W, et al. Association between carbohydrate intake and serum lipids. J Am Coll Nutr. 2006;25(2):155–63.
Denova-Gutierrez E, Huitron-Bravo G, Talavera JO, Castanon S, Gallegos-Carrillo K, Flores Y, et al. Dietary glycemic index, dietary glycemic load, blood lipids, and coronary heart disease. J Nutr Metab. 2010;2010.
Slyper A, Jurva J, Pleuss J, Hoffmann R, Gutterman D. Influence of glycemic load on HDL cholesterol in youth. Am J Clin Nutr. 2005;81(2):376–9.
Fernandes AC, Marinho AR, Lopes C, Ramos E. Dietary glycemic load and its association with glucose metabolism and lipid profile in young adults. Nutr Metab Cardiovasc Dis. 2022;32(1):125–33.
Iacoviello L, Bonanni A, Costanzo S, De Curtis A, Di Castelnuovo A, Olivieri M, Zito F, Donati MB, de Gaetano G. The MOLI-SANI Project, a randomized, prospective cohort study in the Molise region in Italy; design, rationale and objectives. Ital J Public Health. 2007;4:110–8.
Di Castelnuovo A, Costanzo S, Persichillo M, Olivieri M, de Curtis A, Zito F, et al. Distribution of short and lifetime risks for cardiovascular disease in Italians. Eur J Prev Cardiol. 2012;19(4):723–30.
Malferrari G, Monferini E, DeBlasio P, Diaferia G, Saltini G, Del Vecchio E, et al. High-quality genomic DNA from human whole blood and mononuclear cells. Biotechniques. 2002;33(6):1228–30.
Zhong J, Agha G, Baccarelli AA. The role of DNA methylation in cardiovascular risk and disease: methodological aspects, study design, and data analysis for epidemiological studies. Circ Res. 2016;118(1):119–31.
Pala V, Sieri S, Palli D, Salvini S, Berrino F, Bellegotti M, et al. Diet in the Italian EPIC cohorts: presentation of data and methodological issues. Tumori. 2003;89(6):594–607.
Salvini S PM, Gnagnarella P, Maissoneuve P, Turrini A. Banca dati composizione degli alimenti per studi epidemiologici in Italia. Milano: European Isntitute of Oncology. 1998.
Sieri S, Agnoli C, Pala V, Grioni S, Brighenti F, Pellegrini N, et al. Dietary glycemic index, glycemic load, and cancer risk: results from the EPIC-Italy study. Sci Rep. 2017;7(1):9757.
Sieri S, Krogh V. Dietary glycemic index, glycemic load and cancer: an overview of the literature. Nutr Metab Cardiovasc Dis. 2017;27(1):18–31.
Horvath S. DNA methylation age of human tissues and cell types. Genome Biol. 2013;14(10):R115.
Hannum G, Guinney J, Zhao L, Zhang L, Hughes G, Sadda S, et al. Genome-wide methylation profiles reveal quantitative views of human aging rates. Mol Cell. 2013;49(2):359–67.
Drewnowski A, Shultz JM. Impact of aging on eating behaviors, food choices, nutrition, and health status. J Nutr Health Aging. 2001;5(2):75–9.
Samblas M, Milagro FI, Martinez A. DNA methylation markers in obesity, metabolic syndrome, and weight loss. Epigenetics. 2019;14(5):421–44.
van Dongen J, Bonder MJ, Dekkers KF, Nivard MG, van Iterson M, Willemsen G, et al. DNA methylation signatures of educational attainment. NPJ Sci Learn. 2018;3:7.
Bonaccio M, Di Castelnuovo A, de Gaetano G, Iacoviello L. Socioeconomic gradient in health: mind the gap in “invisible” disparities. Ann Transl Med. 2020;8(18):1200.
Acknowledgements
BI was supported by the Fondazione Umberto Veronesi, Milan, Italy, that is gratefully acknowledged. The Moli-sani study research group thanks the Associazione Cuore Sano ONLUS (Campobasso, Italy) for cultural support, and is grateful to the BiomarCaRE (Biomarkers for Cardiovascular Risk Assessment in Europe) Consortium. Moli-sani Study Investigators: The enrollment phase of the Moli-sani study was conducted at the Research Laboratories of the Catholic University in Campobasso (Italy), the follow-up of the Moli-sani cohort is being conducted at the Department of Epidemiology and Prevention of the IRCCS Neuromed, Pozzilli, Italy. Steering Committee: Licia Iacoviello*°(Chairperson), Giovanni de Gaetano* and Maria Benedetta Donati*. Scientific Secretariat: Marialaura Bonaccio*, Americo Bonanni*, Chiara Cerletti*, Simona Costanzo*, Amalia De Curtis*, Augusto Di Castelnuovo§, Alessandro Gialluisi*°, Francesco Gianfagna°§, Mariarosaria Persichillo*, Teresa Di Prospero* (Secretary). Safety and Ethical Committee: Jos Vermylen (Catholic University, Leuven, Belgio) (Chairperson), Renzo Pegoraro (Pontificia Accademia per la Vita, Roma, Italy), Antonio Spagnolo (Catholic University, Roma, Italy). External Event Adjudicating Committee: Deodato Assanelli (Brescia, Italy), Livia Rago (Campobasso, Italy). Baseline and Follow-up Data Management: Simona Costanzo* (Coordinator), Marco Olivieri (Campobasso, Italy), Teresa Panzera*. Data Analysis: Augusto Di Castelnuovo§ (Coordinator), Marialaura Bonaccio*, Simona Costanzo*, Simona Esposito*, Alessandro Gialluisi*°, Francesco Gianfagna°§, Sabatino Orlandi*, Emilia Ruggiero*, Alfonsina Tirozzi*. Biobank, Molecular and Genetic Laboratory: Amalia De Curtis* (Coordinator), Sara Magnacca§, Fabrizia Noro*, Alfonsina Tirozzi*. Recruitment Staff: Mariarosaria Persichillo* (Coordinator), Francesca Bracone*, Teresa Panzera*. Communication and Press Office: Americo Bonanni*. Regional Institutions: Direzione Generale per la Salute—Regione Molise; Azienda Sanitaria Regionale del Molise (ASReM, Italy); Agenzia Regionale per la Protezione Ambientale del Molise (ARPA Molise, Italy); Molise Dati Spa (Campobasso, Italy); Offices of vital statistics of the Molise region. Hospitals: Presidi Ospedalieri ASReM: Ospedale A. Cardarelli—Campobasso, Ospedale F. Veneziale—Isernia, Ospedale San Timoteo—Termoli (CB), Ospedale Ss. Rosario—Venafro (IS), Ospedale Vietri—Larino (CB), Ospedale San Francesco Caracciolo—Agnone (IS); Casa di Cura Villa Maria—Campobasso; Ospedale Gemelli Molise—Campobasso; IRCCS Neuromed—Pozzilli (IS). *Department of Epidemiology and Prevention, IRCCS Neuromed, Pozzilli, Italy. °Department of Medicine and Surgery, University of Insubria, Varese, Italy. §Mediterranea Cardiocentro, Napoli, Italy. Moli-sani Study Past Investigators are available at https://www.moli-sani.org/?page_id=173.
Funding
The enrollment phase of the Moli-sani study was supported by research grants from the Pfizer Foundation (Rome, Italy), the Italian Ministry of University and Research (MIUR, Rome, Italy)–Programma Triennale di Ricerca, Decreto no.1588 and Instrumentation Laboratory, Milan, Italy. This work was also partially funded by the European Union’s Horizon 2020 research and innovation program under the Marie Sklodowska-Curie (grant agreement No 798841 to BI), by the Italian Ministry of Health (GR 2018-12366528 to BI and AG and Ricerca Corrente 2022–2024). Funders had no role in study design; collection, analysis or interpretation of data, the writing of the manuscript or the decision to submit the article for publication.
Author information
Authors and Affiliations
Consortia
Contributions
BI, LI and AG designed the research; FN conducted the methylation analysis; AM and FS contributed to the methylation experiments; MB, SC, AT and ADeC provided essential materials; AG and FS analyzed data and performed statistical analysis; FG and SO contributed to the statistical analysis; FB and SC managed the database; FN, FS, BI and AG wrote the paper; BI, AG and LI had primary responsibility for final content; and CC, MBD, GdG, ADiC and LI conceived the Moli-sani study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Moli-sani study complies with the Declaration of Helsinki and was approved by the Ethical Committee of the Catholic University of Rome, Italy. All participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Definition of covariates. Definition of all the covariates used in the study. Table S1. Sensitivity analyses of glycaemic dietary parameters with methylation and hydroxymethylation measures.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Noro, F., Santonastaso, F., Marotta, A. et al. Association of nutritional glycaemic indices with global DNA methylation patterns: results from the Moli-sani cohort. Clin Epigenet 14, 189 (2022). https://doi.org/10.1186/s13148-022-01407-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13148-022-01407-3