
Abstract
Introduction
Upper Cross Syndrome is a pattern of muscle imbalance and postural dysfunction that can cause discomfort and pain. This study’s objective was to compare the effects of Pilates exercises, corrective exercises, and Alexander’s technique on upper cross syndrome in adolescent girls aged 13–16 years: a six-week intervention study.
Methods
The present study was Quasi-experimental, and its statistical population consisted of 13 to 16-year-old female students. Forty-five students who were diagnosed with upper cross syndrome were purposefully selected as samples and randomly assigned to three groups: Pilates exercises (N = 15), corrective exercises (N = 15), and Alexander’s technique (N = 15). The participants performed exercises for 60 min per session, three sessions per week, and six weeks. This study’s objective was to compare the effects of Pilates exercises, corrective exercises, and Alexander’s technique on upper cross syndrome in adolescent girls aged 13–16 years: a six-week intervention study. This study was retrospectively registered in the Iranian Registry of Clinical Trials (IRCT) on 2023-09-19 to comply with the journal’s policies. The assigned trial registration number is IRCT20230810059106N1.
Results
The results of the dependent t-test showed significant decreases in forward head angle (p = 0.0001), rounded shoulder (p = 0.001), and kyphosis (p = 0.0001) as a result of corrective exercises. There were also significant decreases in forward head angle (p = 0.0001), rounded shoulder (p = 0.002), and kyphosis (p = 0.001) after six weeks of practising Alexander’s technique. However, in the case of Pilates exercises, a significant decrease in forward head angle (p = 0.110), rounded shoulder (p = 0.598), and kyphosis (p = 0.371) was not observed. The one-way analysis of variance revealed a significant difference in the forward head angle (p = 0.012), rounded shoulders (p = 0.013), and kyphosis (p = 0.009).
Conclusions
The effect of Alexander’s technique and corrective exercises on forward head angle, rounded shoulder, and kyphosis abnormalities was almost similar and more effective than pilates exercises.
Similar content being viewed by others


Introduction
The widespread use of electronic devices like mobile phones has become essential in daily life, especially for students [1]. Prolonged use of these devices can lead to abnormal postures, causing neuromuscular imbalances and musculoskeletal conditions [2] such as upper crossed syndrome (UCS). UCS is characterized by weakened and tight muscles [3], often leading to symptoms like forward head posture and rounded shoulders [4]. These abnormal postures can also affect lung capacity and respiratory efficiency, leading to decreased exercise tolerance [5].
Pilates exercises(PE) are a modern training method that concentrates on the body, particularly the core muscles, pelvis, spine, and UCS [6]. Various studies have examined the effect of PE on lumbar lordosis and dorsal kyphosis [7, 8]. Pilates facilitates flexibility, strength, and overall body control and endurance improvements. This exercise form also focuses on body alignment, developing a strong core area, and enhancing coordination and balance. UCS is essential for maintaining body stability [9]. One of the primary methods for correcting abnormal spinal curvatures is through corrective exercises (CE), which can effectively improve alignment [10, 11]. The Corrective Exercise Specialization (CES) program by the National Academy of Sports Medicine (NASM) equips fitness professionals to evaluate and address movement dysfunctions, muscular imbalances, and posture-related concerns in their clients [11]. Studies have shown that CE based on NASM principles can improve abnormal spinal curvatures [12], and teaching proper posture can significantly reduce these abnormalities [13, 14]. The Alexander Technique (AT) is a widely practiced physical method that aims to increase body awareness and improve movement patterns [15]. The goal of the AT is to assist individuals in increasing body awareness and using this information to achieve more efficient functioning. It utilizes a teacher-student model to enable the student to become aware of their body’s sensory-motor condition and to change their habitual faulty movement patterns. The primary focus of this technique is on education rather than treatment [16]. It has been shown to be highly effective in improving balance and is recommended for individuals with UCS to enhance their overall balance and well-being [17].
Therapists have employed several methods to treat UCS, including muscle energy techniques [18], Kinesio taping [19], stretching exercises [20], pressure biofeedback [21], and other procedures. Although these methods have demonstrated effectiveness in clinical settings, they have some drawbacks. A trained rehabilitation therapist must administer the treatment; patients cannot perform it independently. Additionally, the costs associated with these treatments can be high and may not be feasible for some patients. In general, designing an effective method of treatment for this issue contributes significantly to saving a considerable portion of healthcare costs. The researchers focused on 13- to 16-year-old girls for several reasons. First, UCS is more common in girls than boys, and its prevalence increases during adolescence. Second, the teenage years in girls are a time of rapid physical and hormonal changes. These changes can affect the alignment of the spine and cause musculoskeletal problems. Third, UCS can impact posture, balance, and overall health. It can also lead to pain, headaches, and other health problems in teenage girls. Additionally, considering the prevalence of UCS among teenage girls due to improper use of mobile phones, tablets, and computers, not adhering to proper principles during walking, sitting on chairs, lying down, and carrying heavy backpacks highlights the importance of conducting this research. The study is critical because it will provide valuable information on the effectiveness of PE, CE, and AT in improving UCS among adolescent girls. UCS is a common condition that can cause pain, discomfort, and poor posture, characterized by RS, FH, and increased thoracic spine curvature. PE, CE, and AT can improve posture and reduce pain. The study aims to compare the effectiveness of these three methods in improving UCS among adolescent girls and determine which is most effective for improving posture and reducing pain in this population. This study is significant as no previous study has compared the effects of PE, CE, and AT on UCS in teenage girls. Therefore, this study aims to investigate whether six weeks of PE, CE, and AT can affect UCS differently in 13- to 16-year-old girls.
Methods
Study design and participants
The trial protocol for this study was retrospectively registered in the Iranian Registry of Clinical Trials on 2023-09-19 to comply with the journal’s policies, with the assigned approval number IRCT20230810059106N1. This research was Quasi-experimental, and its statistical population consisted of 13 to 16-year-old female students. While this design does not strictly adhere to CONSORT guidelines for randomized controlled trials, we have endeavored to report our methods and findings transparently and comprehensively.
Group allocation
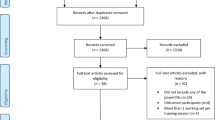
Among the ten first—and second-grade girls’ high schools in the city of Quchan(3000 students), a cluster random sampling approach was employed to select three schools (1000 students). Of the total, 308 students volunteered to participate in the research, with their parents completing the informed consent forms. Subsequently, students between 13 and 16 in these schools underwent individual assessments for UCS. Forty five students who were diagnosed with UCS selected as samples and randomly assigned to three groups: PE (N = 15), CE (N = 15), and AT (N = 15). The participants performed CE, AT, and PE for 60 min per session, three sessions per week, and for 6 weeks that presented in Consort fow chart (Fig. 1). PE and CE exercises were done in the gym and AT exercises were done in the home.
Inclusion and exclusion criteria
Participants in the study had to to simultaneously have postural abnormalities such as kyphosis, FH, and RS, and express a willingness to participate. Those with signs of illness, fractures, surgeries, joint problems, injuries in the spine, skeletal-muscular imbalances, lower limb cross syndrome, abnormal BMI, or engaging in regular physical activity for at least 6 h per week were excluded.
Measurement of the kyphosis, rounded shoulder and forward head
The Corrective Exercise Specialist conducted the measurements.
Thoracic kyphosis angle was measured with a flexicurve ruler, 50 cm in length and 2 cm wide, with the spinous processes of the T2 and T12 vertebrae serving as the starting and ending points [22, 23]. To locate the spinous process of the T2vertebra, the examiner positioned themselves behind the subject and instructed them to bend their head. This positioning revealed two prominences at the base of the cervical region, representing the spinous process of the C6 and C7 vertebrae. The examiner then asked the subject to slowly tilt their head backward by applying slight pressure to these prominences. During this movement, one of the prominences (C6) no longer remained palpable, leaving only the single prominence of the C7 vertebra. By identifying the C7 spinous process, it became easier to locate the spinous processes of the T1 and T2 vertebrae by gently tracing down the spine. In the current study, after identifying the T2vertebra, the starting point of the kyphosis curve was marked using a landmark. To determine the T12 vertebra, the Hoppenfeld method, a widely utilized technique in various studies, was employed [24]. Individuals with a kyphotic angle greater than 46.83 degrees were classified as having an increased kyphotic deformity.
The rounded shoulder angle (RSA) was measured from the vertical posteriorly to a line connecting the C7 and acromial markers [25]. A shoulder angle of more than 52 degrees is considered RS deformity [26].
Forward head angle (FHA) is measured from the vertical anterior to a line connecting the tragus and the C7 marker. The ideal angle of the head in this method is less than 36 degrees, and an angle of more than 46 degrees is considered an abnormality of the FH [26] (Fig. 2). Intraday reliability for FHA and FSA demonstrated acceptable within-day reliability (FHA = Intraclass Correlation Coefficient (ICC)(2,1) = 0.92, Standard Error of the mean (SEM) = 2_ and RSA ICC(2,1) = 0.89, SEM = 5_) based on this sub-sample [27].

Consort fow chart for enrollment and intervention

FHA measured from the vertical anteriorly to a line connecting the tragus and the C7 marker. The forward shoulder angle (RSA) was measured by measuring the angle between the vertical line running posterirly and the line connecting the markers at the C7 and acromial position [25]
Interventions
Group A: corrective exercises
The CE exercises were done in the gym, and the corrective movements specialist was responsible for supervising their performance. Selected CE was designed to correct posture and address the mentioned abnormalities through stretching exercises for shortened muscles and strengthening exercises for individuals with weak muscles. These exercises included a 5-10-minute warm-up followed by stretching exercises for the chest, hip-flexor-psoas, upper trapezius, intercostal muscles, upper neck extensors, and then strengthening exercises for the shoulder protractors, deep neck flexors, lower neck extensors, and thoracic spine extensors.
Group B: Alexander’s technique
In the AT group, parents supervised the students’ exercises at home based on the explanations and training the corrective movements specialist provided in the first session. In the AT group, adolescents were taught the considerations and habits they should remember and focus on daily. These included teaching ergonomic considerations and individual postural habits during daily activities such as standing, walking, sitting, sleeping, reading, using a computer, and other repetitive and continuous activities performed during the day. Individuals were taught and reminded of these matters one to two times per week at school. Parents reported their implementation to the researcher. Parents played a fundamental role in this program and were responsible for reminding their children of correct postural habits and points through predetermined verbal instructions throughout the day. A poster containing images displaying proper postural habits while standing, sitting, and lying down was created and made available to individuals. This poster can be installed in a suitable location at home, allowing students to maintain correct posture by observing it regularly and remembering to do so.
Group C: Pilates exercises
PE was done in the gym. The Pilates instructor trained the subjects in the Pilates group, and a corrective movement specialist supervised the training during the exercises. In the first session of PE, the group received an explanation of the basic principles that were followed in all sessions. The following steps were taken in each PE session, including checking the posture (pelvis and spinal column), controlling breathing and standing in class (about 5 min), performing Pilates breathing and stretching exercises with coach explanations (about 10 min), performing modified specific exercises (about 40 min), and returning to the initial state (5 min). The exercises started at low levels and gradually progressed until the participants could control their spinal columns in various positions. The exercise intensity was personalized based on each participant’s pain and exercise tolerance threshold. As a result, with continued exercise, the participants could do more repetitions without feeling pain or fatigue. The exercises started with 8 repetitions and ended with 16 repetitions. Each session included new exercises in addition to those from the previous session.
Data analysis procedure
We used the Shapiro-Wilk test to check for normality and Levene’s test to assess variance equality. The dependent t-test was used for within-group comparisons. We conducted one-way ANOVA with TukeyTest for multiple group comparisons to compare means pairwise. Data analysis was performed using SPSS software version 19 at a significance level of p < 0.05.
Results
The statistical indices of age, height, and weight of the participants in different training groups are shown in Table 1.
The results of the dependent t-test showed that after 6 weeks of CE and AT, there was a significant decrease in FHA, RS, and kyphosis from the pre-test to the post-test phase (Table 2). However, in the PE group, a significant decrease in FHA, RS, and kyphosis from the pre-test to the post-test phase was not observed (Table 2).
The results of the one-way analysis of variance showed that after six weeks of PE, CE, and AT, a significant difference was observed in the FHA, RS, and kyphosis between the pre-test and post-test measurements (Table 3).
The Tukey post hoc tests indicate that no significant difference was observed between the CE group and the AT group in the FHA, RS, and kyphosis (Table 4). However, a significant difference was found between the CE group and the Pilates exercises group in the FHA, RS and kyphosis. Additionally, a significant difference was observed between the AT group and the Pilates exercises group in the FHA, RS, and kyphosis(Table 4).
Discussion
To the authors’ knowledge, this is the first study that investigated comparing the effects of Pilates, corrective exercises, and Alexander’s technique on upper cross syndrome among adolescent girls’ students (ages 13–16): a six-week study. The main findings of this study were [1] Six weeks of CE and AT significantly reduced FHA, RS, and kyphosis in adolescent girls with UCS; [2] PE showed a reduction in FHA, RS, and kyphosis, but this reduction was not statistically significant; [3] There was a significant difference between the FH, RS, and kyphosis of girls in the PE, CE, and AT groups, with the CE and AT groups showing greater improvements than the PE group; [28] There was no significant difference between the mean FH of girls in the CE and AT groups; [29] There was a significant difference between the PE group and both the CE and AT groups in all three variables of FH, RS, and kyphosis. These findings suggest that CE and AT may be more effective than PE in improving UCS in adolescent girls.
The results of the dependent t-test showed that six weeks of AT significantly reduced FH angle, RS, and kyphosis in adolescent girls. Babaei et al. (2023) conducted a study on the effectiveness of the AT on the static and dynamic balance of young men with UCS. They found a significant improvement in both static and dynamic balance after the intervention [17]. Several studies have explored methods for correcting spinal abnormalities and improving posture in children and students. Cardon et al. (2001) proposed that teaching correct posture and continuous monitoring throughout the day in elementary school children is an appropriate approach [30]. Robbins (2009) observed a 75% reduction in musculoskeletal disorders by teaching students proper sitting [31]. Feingold (2002) found that teaching school children how to use backpacks correctly improved their posture, particularly in the shoulder position [32]. Heyman (2009) taught students various techniques, including correct posture, backpack use, and anatomical principles, resulting in improved posture and prevention of musculoskeletal disorders [33]. Hrysomallis et al. (2001) emphasized the importance of exercise frequency in correcting posture and recommended incorporating exercises into daily life [34]. The study focused on home teaching and retraining, aligning with previous research on the effectiveness of training programs in correcting UCS. These programs share similar effectiveness mechanisms but require time for the consolidation of good physical habits. Proper positioning, ongoing CE, and integrating exercise programs are necessary to correct physical issues. The findings emphasize the significance of teaching correct posture, providing education on backpack use, and integrating exercise programs to improve posture and prevent musculoskeletal disorders.
The results of the dependent t-test showed that 6 weeks of CE significantly reduced FH angle, RS, and kyphosis in adolescent girls. Abdullahzadeh et al.‘s (2019) study showed that eight weeks of CE based on NASM principles improved UCS in the experimental group compared to the control group [12]. Regular CE [13] and comprehensive CE along with teaching proper posture [14] had a significant effect on UCS [13, 14]. to obtain better results in their training programs, we suggest that experts pay attention to correcting abnormalities simultaneously as a new approach [35]. Zandi (2010) compared the effects of CE, postural retraining, and a combination of both on correcting UCS in adolescent girls. Significant differences were found in all variables between the CE group and the combined group. The postural retraining group showed improvements in kyphosis and forward head posture (FH), but no significant differences were observed in rounded shoulders (RS). These findings align with the present study, suggesting that the lack of stimulation of shoulder restricting muscles and the absence of attention to releasing myofascial tissues in the anterior chest region during postural retraining exercises may explain the absence of significant effects on RS [36]. The results of the studies showed that CE can improve FH posture [37], hyperkyphosis in girls [38] and boys [39], and spinal column posture [40]. These researchers recommend CE as a reliable method for improving spinal abnormalities, which can reduce the occurrence of future problems and discomfort.
Several studies have investigated the effects of PE on individuals with UCS, and the findings suggest that Pilates can provide significant benefits [41, 42]. In the present research, PE showed a reduction in FH angle, RS, and kyphosis from the pre-test to the post-test, but this reduction was insignificant. Recent studies have examined the effects of PE on individuals with various postural imbalances. Rahimi et al. (2022) surveyed middle-aged women with lower cross syndrome. They found that six weeks of PE enhanced the strength and efficiency of core stabilizer muscles, leading to improved function in both the upper and lower extremities [42]. Furthermore, de Araújo et al. (2012) found that the Pilates method was effective in reducing the degree of non-structural scoliosis, improving flexibility, and decreasing pain [41]. These findings highlight the potential benefits of PE in addressing various postural imbalances and enhancing function, alignment, and muscle strength. The results of these studies are consistent with the results of the present research. The studies support the effectiveness of Pilates exercises in targeting the muscles involved in UCS. These exercises help improve posture and muscular balance and promote body awareness. Future studies should include larger sample sizes, longer intervention durations, and control groups to establish the efficacy of PE in addressing UCS.
Previous studies support the effectiveness of EC and AT compared to PE in treating UCS. Combined exercises are more effective than independent CE and retraining [36, 43]. Some studies also report the effectiveness of physiotherapy and chiropractic interventions [18]. However, in some cases, no significant changes were observed, possibly due to qualitative evaluation methods, lack of posture assessment, or short exercise periods [44]. This study’s limitation is the small sample size of 45 students; only 15 students participated in each group. The study was conducted over six weeks, and if it had been conducted over a longer period, the effects of the interventions may have been more pronounced. Also, this study did not include a control group.
Conclusion
The study highlights the potential benefits of Pilates, CE, and AT in addressing UCS in adolescent girls. The effect of Alexander’s technique and corrective exercises on forward head angle, rounded shoulder, and kyphosis abnormalities was almost similar and more effective than pilates exercises. These interventions offer promising ways to improve posture, alignment, muscular imbalances, and body awareness. Further research is needed to confirm these findings and explore the long-term effects on UCS in this population. Early interventions targeting UCS have the potential to foster healthy postural habits and enhance overall well-being among this group.
Data availability
Not applicable.
References
Tong W-X, Li B, Han S-S, Han Y-H, Meng S-Q, Guo Q, et al. Current status and correlation of physical activity and tendency to problematic mobile phone use in college students. Int J Environ Res Public Health. 2022;19(23):15849.
Yoo W-G, Park S-Y. Effects of posture-related auditory cueing (PAC) program on muscles activities and kinematics of the neck and trunk during computer work. Work. 2015;50(2):187–91.
Gillani S, Rehman S, Masood T. Effects of eccentric muscle energy technique versus static stretching exercises in the management of cervical dysfunction in upper cross syndrome: a randomized control trial. J Pak Med Assoc. 2020;70(3):1.
Yaghoubitajani Z, Gheitasi M, Bayattork M, Andersen LL. Corrective exercises administered online vs at the workplace for pain and function in the office workers with upper crossed syndrome: randomized controlled trial. Int Archives Occup Environ Health. 2022;95(8):1703–18.
Okuro RT, Morcillo AM, Ribeiro MÂGO, Sakano E, Conti PBM, Ribeiro JD. Mouth breathing and forward head posture: effects on respiratory biomechanics and exercise capacity in children. Jornal Brasileiro De Pneumologia. 2011;37:471–9.
Caldwell K, Harrison M, Adams M, Triplett NT. Effect of Pilates and taiji quan training on self-efficacy, sleep quality, mood, and physical performance of college students. J Bodyw Mov Ther. 2009;13(2):155–63.
Afroundeh R, Saidzanozi R. Comparison of the effect of pilates and traditional corrective exercises on lumbar lordosis in female students. Sci J Rehabilitation Med. 2017;6(3):84–94.
Junges S, Gottlieb MG, Baptista RR, Quadros CBd RTL, Gomes I. Effectiveness of pilates method for the posture and flexibility of women with hyperkyphosis. Rev Bras Cienc Mov. 2012;20(1):21–33.
Srivastav P, Nayak N, Nair S, Sherpa LB, Dsouza DJ. Swiss ball versus mat exercises for core activation of transverse abdominis in recreational athletes. J Clin Diagn Res. 2016;10(12):YC01.
Patel K, Wilkinson N. Corrective exercise: a practical approach. A practical approach: Routledge; 2014.
Roshani S, Yousefi M, Sokhtezari Z, Khalil Khodaparast M. The effect of a corrective exercise program on upper crossed syndrome in a blind person. J Rehabilitation Sci Res. 2019;6(3):148–52.
Abdolahzadeh M, Daneshmandi H. The effect of an 8-week NASM corrective exercise program on upper crossed syndrome. J Sport Biomech. 2019;5(3):156–67.
Hosseini SM, Rahnama N, Barati AH. Comparing the effects of ten weeks of regular corrective exercise and corrective exercise with whole body vibration apparatus on upper cross syndrome. Stud Sport Med. 2017;8(20):89–106.
Miri H, Shahrokhi H, Dostdar Rozbahani A, Nasirzare F. Comparison of the effect of comprehensive corrective exercises with and without posture training on upper cruciate syndrome in female students. Med J Mashhad Univ Med Sci. 2022;61(5):246–65.
Kutschke IP. The effects of the Alexander technique training on neck and shoulder biomechanics and posture in healthy people. 2010.
Jain S, Janssen K, DeCelle S. Alexander technique and Feldenkrais method: a critical overview. Phys Med Rehabilitation Clin. 2004;15(4):811–25.
Babaei H, Alizadeh MH, Minoonezhad H, Movahed A. Effectiveness of the Alexander technique on the static and dynamic balance of young men with upper crossed syndrome. Sci J Rehabilitation Med. 2023;12(1):60–77.
Moore MK. Upper crossed syndrome and its relationship to cervicogenic headache. J Manipulative Physiological Ther. 2004;27(6):414–20.
Esin O, Khairullin IK, Shamsutdinova R. Upper crossed syndrome of muscle imbalance in adolescents with tension-type headache. Zhurnal Nevrologii i Psikhiatrii Imeni SS Korsakova. 2019;119(9):12–6.
Bae W-S, Lee H-O, Shin J-W, Lee K-C. The effect of middle and lower trapezius strength exercises and levator scapulae and upper trapezius stretching exercises in upper crossed syndrome. J Phys Therapy Sci. 2016;28(5):1636–9.
Kang DY. Deep cervical flexor training with a pressure biofeedback unit is an effective method for maintaining neck mobility and muscular endurance in college students with forward head posture. J Phys Therapy Sci. 2015;27(10):3207–10.
CM A. The reliability of five clinical postural alignment measures for women with osteoporosis. Physiother Can. 2000;52:286–94.
Rajabi R, Seidi F, Mohamadi F. Which method is accurate when using the flexible ruler to measure the lumbar curvature angle? Deep point or mid-point of arch. World Appli Sci. 2008;4(6):849–52.
Stanley H. Physical examination of the spine and extremities. Appleton-Century-Crofts; 1976.
Thigpen CA, Padua DA, Michener LA, Guskiewicz K, Giuliani C, Keener JD, Stergiou N. Head and shoulder posture affect scapular mechanics and muscle activity in overhead tasks. J Electromyogr Kinesiol. 2010;20(4):701–9.
Sawyer QL. Effects of forward head rounded shoulder posture on shoulder girdle flexibility, range of motion, and strength. The University of North Carolina at Chapel Hill; 2006.
Portney LG, Watkins MP. Foundations of clinical research: applications to practice. Pearson/Prentice Hall Upper Saddle River, NJ; 2009.
Risalda P, Phansopkar P, Naqvi WM. Effectiveness of active release technique verses conventional physiotherapy in management of upper cross syndrome. Indian J Forensic Med Toxicol. 2021;15(1):246–50.
Sasun AR, Jawade S, Chitale N, Chitale NV. Measuring the efficacy of myofascial rollers and post-isometric relaxation technique in relieving pain intensity and postural deviation using plumb line assessment for the treatment of upper cross syndrome in dental undergraduate (UG) students. Cureus. 2022;14(10).
Cardon G, De Bourdeaudhuij I, De Clercq D. Back care education in elementary school: a pilot study investigating the complementary role of the class teacher. Patient Educ Couns. 2001;45(3):219–26.
Robbins M, Johnson I, Cunliffe C. Encouraging good posture in school children using computers. Clin Chiropr. 2009;12(1):35–44.
Feingold AJ, Jacobs K. The effect of education on backpack wearing and posture in a middle school population. Work. 2002;18(3):287–94.
Heyman E, Dekel H. Ergonomics for children: an educational program for elementary school. Work. 2009;32(3):261–5.
Hrysomallis C, Goodman C. A review of resistance exercise and posture realignment. J Strength Conditioning Res. 2001;15(3):385–90.
Daneshmandi H, Mogharrabi Manzari M. The effect of eight weeks comprehensive corrective exercises on upper crossed syndrome. Res Sport MedicineTechnology. 2014;12(7):75–86.
Zandi S, Rajabi R. Compare the effect of three interventional programs on correction of hyper kyphosis, forward head posture, forward shoulder and UCS in 10–11 years old girls. Faculty Physical education: Tehran; 2010.
Harman K, Hubley-Kozey CL, Butler H. Effectiveness of an exercise program to improve forward head posture in normal adults: a randomized, controlled 10-week trial. J Man Manipulative Therapy. 2005;13(3):163–76.
Sokhangouei Y, Ebrahimi E, Salavati M, Keyhani MR, Kamali M. Effect of corrective exercises on chest expansion in kyphotic females. Jrehab. 2008;9(1):33–6.
Daneshmandi H, Hemtinejad MA, Shah Moradi D. Investigating changes in kyphosis and vital capacity following a correction program. Harkat. 2002;22:75–86.
Rahnama N, Bambaeichi E, Taghian F, Nazarian AB, Abdollahi M. Effect of 8 weeks regular corrective exercise on spinal columns deformities in girl students. J Isfahan Med School. 2009;27(101):676–86.
de Araújo MEA, da Silva EB, Mello DB, Cader SA, Salgado ASI, Dantas EHM. The effectiveness of the pilates method: reducing the degree of non-structural scoliosis, and improving flexibility and pain in female college students. J Bodyw Mov Ther. 2012;16(2):191–8.
Rahimi M, Piry H, Monajatipour E. Effect of six weeks of Pilates exercises on the function of upper and lower extremities of middle-aged women with lower crossed syndrome. PTJ. 2022;12(4):269–78.
Pesco MS, Chosa E, Tajima N. Comparative study of hands-on therapy with active exercises vs education with active exercises for the management of upper back pain. J Manipulative Physiological Ther. 2006;29(3):228–35.
Wright EF, Domenech MA, Fischer JR JR. Usefulness of posture training for patients with temporomandibular disorders. J Am Dent Association. 2000;131(2):202–10.
Acknowledgements
We want to thank the authors’ team members for their contributions to the success of this study.
Funding
The authors declare that they did not receive any financial support during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
NS and KK contributed to the study conception and design, and NS performed clinical examination and data collection. MS and KK participated in the methodological development and design of the statistical analysis. MS wrote the first draft of the manuscript and contributed to the comments and suggestions that significantly improved the manuscript. Finally, all the authors revised it critically for important intellectual content, agreed with the content, contributed to the current study’s refinement, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed consent was obtained from the parents, legal guardians, or next of kin for participating minors under the age of 16. The parents or legal guardians were fully informed about the nature of the study and their consent was obtained before any involvement of the minors in the research. The Human Ethics Research Committee approved this study of the Sport Sciences Research Institute of Iran according to compliance with the Ethical Standards in Research of the Ministry of Science, Research and Technology, with the code IR.SSRI.REC. 1401.1724, as well as operating under the Declaration of Helsinki. Furthermore, the trial protocol for this study retrospectively registered in the Iranian Registry of Clinical Trials on 2023-09-19 to comply with the journal’s policies, with the assigned approval number IRCT20230810059106N1. This ensures transparency and credibility in the research findings. Adhering to these registration requirements upholds the highest research ethics and transparency standards in our study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shadi, N., Khalaghi, K. & Seyedahmadi, M. Comparing the effects of Pilates, corrective exercises, and Alexander’s technique on upper cross syndrome among adolescent girls student (ages 13–16): a six-week study. BMC Sports Sci Med Rehabil 16, 143 (2024). https://doi.org/10.1186/s13102-024-00933-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-024-00933-2