
Abstract
Background
The performing of jump and landing in futsal simultaneous with divided attention is one of the most common mechanisms of non-contact anterior cruciate ligament (ACL) injury. Neuromuscular training has effectively reduced the risk of ACL injury, but the effect of neurocognitive training has received less attention. This study investigated the effect of combining 8 weeks of neuromuscular training with dual cognitive tasks on the landing mechanics of futsal players with knee ligament dominance defects.
Methods
Thirty male futsal players (mean ± SD: age: 21.86 ± 3.27 years) with knee ligament dominance defects were purposefully identified by the tuck jump test and were randomly divided into the intervention and the control group. The intervention group performed dual task (DT) training for three weekly sessions for 8 weeks and 60 min each, while the control group only did activities of daily living. During the drop vertical jump test, 2D landing kinematics in two moments of initial contact (IC) and full flexion (FF) were assessed. Data were analyzed by means of 2 × 2 repeated measures ANOVA followed by post hoc comparison (Bonferroni) at the significance level of (α ≤ 0.05).
Results
A significant improvement was observed in the intervention group compared to the control group for the dynamic knee valgus at IC (F1,28 = 6.33; P = 0.02, ES = 0.31) and FF (F1,28 = 13.47; P = 0.003, ES = 0.49), knee flexion at IC (F1,28 = 20.08; P = 0.001, ES = 0.41) and FF (F1,28 = 13.67; P = 0.001, ES = 0.32), ankle dorsiflexion at IC (F1,28 = 37.17; P = 0.001, ES = 0.72) and FF (F1,28 = 14.52; P = 0.002, ES = 0.50), and trunk flexion at FF (F1,28 = 20.48; P = 0.001, ES = 0.59) angles. Changes in the trunk flexion at IC (F1,28 = 0.54; P = 0.47, ES = 0.03) and trunk lateral flexion at IC (F1,28 = 0.006; P = 0.93, ES = 0.00) and FF (F1,28 = 2.44; P = 0.141, ES = 0.148) angles were not statistically significant.
Conclusions
DT training compared to the control group improved landing mechanics in futsal players with knee ligament dominance defects.
Trial registration: Current Controlled Trials using the IRCT website with ID number IRCT20210602051477N1 prospectively registered on 20/06/2021.
Similar content being viewed by others


Background
In a national survey in the Netherlands, futsal, with an injury incidence of 55.2 per 10 000 h of sports participation, was among the ten sports with a higher injury rate [1]. Knee injuries are common among individuals participating in team sports, such as futsal [2]. Jumping and landing are the most common mechanisms of non-contact anterior cruciate ligament (ACL) injury [3]. More than one-third of non-contact ACL injuries in football frequently occur after landing from a jump [3]. The landing technique is complex and influenced by biomechanical, neuromuscular, and neurocognitive defects, so a stiff landing with minimum flexion in the trunk, hip, knee, and ankle causes a peak of the ground reaction force and increases the risk of ACL injury [4]. Inability to trunk control and hip movements can lead to increased internal rotation and adduction of the femur, eventually resulting in dynamic knee valgus (DKV) and increased forces acting on ACL [5]. Limitation of the ankle dorsiflexion range of motion during landing is also associated with decreased knee flexion in the sagittal plane and increased DKV in the frontal plane, which puts excessive tension on the ACL [6]. Sigward et al. [7] indicated that individuals with limited ankle dorsiflexion range of motion exhibited more DKV during landing.
In a sports competition, futsal players must perform several tasks simultaneously, including controlling the ball, decision-making, considering the opponent's movements, and performing sport-specific patterns [8]. These conditions cause more attention to cognitive stimuli and failure to follow the safe kinematic pattern during jumping and landing, which may expose a person to an ACL injury [9]. In fact, when the attentional demand for cognitive stimuli is greater than a certain amount due to the limited capacity of attention, the performance of other tasks performed simultaneously may be affected [10].
Studies examining the effects of more sport-specific cognitive tasks also appear to indicate that athletes exhibit more high-risk landing biomechanics when they must divide their attention (e.g., less hip and knee flexion, greater vertical ground reaction forces, and DKV) [11, 12]. Farvardin et al. [13] showed that adding a cognitive load to the kicking mechanics of futsal players in dual-task (DT) conditions reduces knee and hip flexion and more significant sagittal plane knee loading, which can increase the risk of ACL injury. Athletic performance is typically assessed under conditions associated with performing a sport-specific pattern simultaneously with decision-making and divided attention, known as DT [14]. In addition, it has been stated an athlete who is a deficit at DT may not be able to appropriately monitor neuromuscular control associated with the sport-specific tasks [9].
Neuromuscular defects (trunk, leg, quadriceps, and ligament dominance) are considered modifiable risk factors highly associated with ACL injury [15]. Knee ligament dominance deficit, or DKV, occurs when the motor control strategies adopted by the athlete do not provide sufficient dynamic stability for the knee joint. As a result, a significant portion of the ground reaction force during landing is absorbed by ligaments [16]. The tuck jump test consists of repeated plyometric activities that identify neuromuscular factors associated with ACL injury [17].
Neuromuscular training programs, including lower extremity strengthening, plyometric exercises, and proprioception training, are likely to reduce the risk of ACL injury by modifying movement patterns and pre-programmed feedforward strategies during jumps and landings [18]. Neuromuscular training aimed at reducing DKV angles and improving stability and coordination is considered important in ACL injury prevention [19]. Nagano et al. [20] reported that jumping and balance exercises positively affect knee mechanics. Despite various injury prevention programs, the incidence of ACL injury in athletes is increasing [21, 22]. Current training programs focus mainly on the individual's motor performance and do not consider cognitive challenges. Consequently, there is probably a gap between traditional injury prevention programs [23].
Neurocognitive factors such as reaction time, focus of attention, visual motor control, processing speed, and DT may influence injury risk via alterations to neuromuscular control during sport-specific tasks [21]. Evidence suggests that neurocognitive deficits play a key role in developing neuromuscular and biomechanical defects associated with ACL injury [24]. Likewise, athletes' poorer reaction time and processing speed have been identified as predictors of ACL injury [25]. Neurocognitive deficits can be considered modifiable risk factors that can be corrected with neuromuscular and cognitive training [4]. Neurocognitive approaches may be the missing link in ACL injury prevention exercises [26]. DT training is defined as performing two or more exercises (motor + cognitive) simultaneously [27]. Previous studies have shown that DT training leads to the development of new perceptual strategies, improvement of decision-making and attentional focus [28], enhanced retention and sustained attention [29], and finally, reduction of DT interference [27, 30]. To develop a valid training protocol for injury prevention, cognitive tasks should be considered, which may determine the limitation of the effectiveness of ACL injury prevention training programs [31]. The ability to maintain dynamic stability of the knee joint under conditions associated with cognitive challenges is crucial in preventing ACL injuries [10].
Adding cognitive tasks to neuromuscular training may improve lower extremity mechanics during jumping and landing [24]. A review by Moreira et al. [32] investigated the effect of DT training on the performance of athletes. It concluded that although DT training reduces performance in the short term, it improves working memory and attentional control in the long term. Sarulatha et al. [33] showed that progressive DT training improves motor function in older adults with balance disorders. DT and multi-task exercises can increase the capability of people to overcome the limited central nervous system processing capacity [34]. However, to our knowledge, no studies have targeted DT training to reduce the risk of ACL injury in athletes with neuromuscular defects.
This study aimed to investigate the effects of combining 8 weeks of neuromuscular training with dual cognitive tasks on the landing mechanics of futsal players with knee ligament dominance defects. Therefore, “does DT training improve landing mechanics in futsal players with knee ligament dominance defects?”. We hypothesized that a combined 8-week neuromuscular dual cognitive task training program would improve 2D kinematic measures of drop landings compared to a control group. The present study's findings can provide researchers with a new approach to ACL injury prevention training that targets the effect of cognitive tasks similar to competition conditions and can also increase the effectiveness of neuromuscular training.
Methods
Study design
Before data collection, this study was approved by the ethics committee of the Sports Sciences Research Institute with ID number (IR.SSRI.REC.1400.1071). Thirty male futsal players participated in this parallel-group randomized controlled trial (RCT) that was prospectively registered as a clinical trial with the code (IRCT20210602051477N1) in the Iranian Registry of Clinical Trials, date of first registration 20/06/2021. The allocation ratio (1:1) of the intended numbers of participants in each of the control and intervention groups. All participants were informed of the study procedures and signed an informed consent form prior to participating, per the Declaration of Helsinki.
Participants
A priori power analysis (G*Power©, version 3.1.9.2, University of Dusseldorf, Dusseldorf, Germany) to obtain 80% statistical power with an alpha of 0.05, a beta of 0.20, and a medium effect size of 0.06, determined we would need 12 participants per group (a total sample size of 24 participants). Allowing a dropout rate of 10% and improved final statistical power, we enrolled 15 participants per group (total sample size of 30 participants). This effect size was comparable to previous research reporting changes in landing mechanics after neuromuscular training [18].
Eligibility criteria
Inclusion criteria included futsal players with knee ligament dominance deficit identified by the tuck jump test [15], men in the age range of 18–30 years, and normal body mass index [35], history of participation in futsal in the past three years, 4 sessions per week [36], and not participating in injury prevention training programs in the last year. Subjects who showed DKV during the tuck jump test were identified as those with knee ligament dominance defects.
Exclusion criteria included a history of neuromuscular disorders, ACL injury or lower extremity and trunk injury requiring surgery during the last six months [37], visible malalignment in the lower extremity and trunk [10], or any medical disorder that affects the cognitive process and tasks [14], the subjects’ dissatisfaction and unwillingness to perform the research process, the lack of subjects contribution in two consecutive training sessions and three non-consecutive training sessions.
Randomization
Randomization was performed by an independent investigator unfamiliar with the testing protocol using a random allocation rule. The letters A and B were identified as markers for random groups assignment and were placed in sealed opaque envelopes in a box. Another researcher opened envelopes and proceeded with training according to the group assignment. These letters were numbered randomly selected and placed one after the other. Thus, the participants were divided into two groups A (intervention = 15) and B (control = 15). Group allocation was concealed using an opaque envelope until after athletes had been enrolled in the study to minimize potential bias. In the current study, a single-blind method was used where only participants were tried to be blinded from the study. For this purpose, the intervention and control groups went about their daily lives (futsal exercises, four weekly sessions). In addition, the intervention group also received DT training, and the control group continued futsal exercises without any information about the conditions of the other subjects.
The subjects were asked to perform an initial warm-up before the test to prevent injury. The pre-test warm-up protocol took 5 min and included squats with body weight (2 sets—8 repetitions), bipedal vertical jump (2 sets—5 repetitions), running, and dynamic stretching movements [10]. The post-test was conducted 1 week after the intervention for all subjects. The location of data collection and intervention group exercises for maximum application and generalizability was in the place of indoor soccer, especially for futsal players.
Interventions included a combined 8-week neuromuscular training program with dual cognitive tasks performed simultaneously by the intervention group. After 8 weeks, a post-test was applied in pre-test conditions for both control and experimental groups, and the collected data were analyzed (Fig. 1).

Consort flow diagram
Outcome measurements
The current study used the tuck jump test to identify futsal players with knee ligament dominance defects (an increased reliance on frontal plane control compared to sagittal plane control). The drop vertical jump test, video camera, and kinovea software were used to investigate the landing mechanics.
2D kinematics with intraclass correlation-coefficient (ICC = 0.90–0.99) based on the Dingenen et al. [38] and the kinovea software (kinovea, version 0.8.15, USA), have been reported as valid and reliable [39]. In this study, two standard cameras (Samsung Galaxy Note 4, N910S, Korea) recorded drop vertical and tuck jump tests simultaneously. A camera was located on the sagittal plane, and a camera was placed on the frontal plane to record the subjects' movements at a distance of 3 m [15]. The cameras sat on a tripod perpendicular to the plane at a height of 65 cm and recorded the videos synchronously. Free video software (kinovea, version 0.8.15, USA) was used for recording videos [39]. Knee flexion, trunk flexion, and ankle dorsiflexion in the sagittal plane and trunk lateral flexion, and DKV in the frontal plane were measured.
2 × 2 (group × time) repeated measures ANOVA was used for each variable to compare the kinematic angles in the two moments of Initial Contact (IC) and Full Flexion (FF).
Procedures
Tuck jump test
The tuck jump test is a valid and reliable method with an intraclass correlation-coefficient (ICC = 0.94–0.96) to assess and diagnose neuromuscular deficits associated with an ACL injury [17]. Subjects were instructed to place their feet on the ground in the middle of a marked rectangle. This test involves performing continuous jumps with maximum height for ten seconds. Basic instructions given about how to perform the test included information about lifting the knees to hip height and trying to land on the same spot with their feet shoulder-width apart. Participants were not allowed to perform more than two tests before data collection. Each athlete carried out continuous tuck jumps on the designated spot after receiving basic instructions again about how to complete the trial. The knee ligament dominance was defined in the tuck jump test when knee valgus appeared at the landing and foot placement was not shoulder-width apart [15].
Landing mechanics
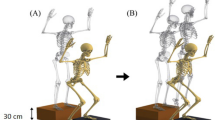
Biomechanical patterns at landing can be assessed during the drop vertical jump test [40]. The subject stood with his feet shoulder-width apart on a box of 40 cm in height. Subjects were instructed to drop directly down the box and immediately perform a maximum vertical jump; both raised their arms like a basketball rebound. The drop vertical jump has been proven valid and reliable, with a reliability coefficient greater than (0.93) [16]. Three successful jumps and a 30-s rest were performed between each jump. The trial was discarded and repeated if both feet did not land on the ground, if the athlete jumped off the box instead of dropping during the test. To standardize the jump height, a ball was placed above the subjects (Fig. 2). A baseline assessment of landing mechanics was completed for each participant upon enrollment.

Drop vertical jump (DVJ): A Initial stance. B Initial contact. C Full flexion. D Max vertical jump
Neuromuscular training with dual cognitive tasks
Following completion of baseline testing, athletes in the intervention group participated in an 8-week progressive neuromuscular training program with dual cognitive tasks under the supervision of two experienced examiners. The neuromuscular training program based on those proposed by Ghanati et al. [18] consisted of 8 weeks of sport-specific training, agility, balance, neuromuscular coordination, strength training, proprioception, and plyometrics. Neuromuscular training programs include double-leg squats, walking lunges, single-leg squats, double-leg drop jumps, single-leg stance on an unstable surface, single-leg countermovement jumps, horizontal bounds, single-leg standing long jumps (Table 1) [18]. All squat exercises were performed with body weight, and a balance ball was used to stand a single leg on an unstable surface. This training protocol, program components, time, type, and repetition were recommended to prevent ACL injury. The neuromuscular training program consisted of three sessions per week during weeks 1–6 and two sessions per week during weeks 7–8 (22 sessions total). Training program interventions included 10 min of submaximal warm-up on a stationary bike, 40 min of exercise, 30 to 60 s of rest between each set, and 5 min to cool down. Finally, the total exercise time was between 45 and 60 min. The neuromuscular training program used in this study has been previously described and shown to reduce high-risk landing mechanics in healthy athletes [18]. It is important to note that all neuromuscular training sessions were performed simultaneously with cognitive tasks (DT training).
The cognitive tasks mainly included functional responses to sensory stimuli, verbal and visual memory, motor learning, speech, attention, and inhibition and were performed simultaneously with neuromuscular training [41]. Determining the ideal distance between stimuli to perform a DT was challenging. If the stimulus is faster than one to one and a half seconds, it was shown that cognitive error increases [42]. Therefore, using a two-second interval between stimuli is appropriate for healthy individuals in the present study; cognitive interventions with a time interval of 2 s were presented [42]. For instance, the subject must perform mathematics calculations simultaneously with all squat exercises.
It has been shown that more than three errors in neuromuscular control or one severe error indicate that the athlete is not ready to add neurocognitive challenges to neuromuscular training. Therefore, this criterion was used to control the training intensity [24]. Two experienced athletic trainers were used to implement the training protocol and the accuracy of performing cognitive tasks and monitoring the training process. The instructions were applied before each training session. In the first week, the external and internal focus of attention instructions were used to teach subjects the correct joint alignment and proper movement pattern. The full description of the neuromuscular DT cognitive training program is described in Table 2.
Data analysis
To obtain 2D kinematic data, videos recorded by the 2 digital cameras at 30 frames per second were imported into kinovea software. The kinematic variables, including the articulated angles (DKV and knee flexion, ankle dorsiflexion, trunk flexion, and trunk lateral flexion) were extracted after modeling the lower extremities and trunk in this software. We placed reflective markers on the episternum, acromion process, anterior superior iliac spine (ASIS), great trochanter, medial and lateral epicondyles of the femur, medial and lateral malleoli [37], middle of the knee joint, and middle of the ankle joint [43] for 2D kinematic analysis.
The ankle dorsiflexion angle was the angle between the line formed by the lateral epicondyle of the femur and the lateral malleolus and a second line connecting the lateral malleolus and fifth metatarsal heads [43]. The trunk flexion angle was defined as the angle formed between the acromion and the greater trochanter and a line perpendicular to the ground. The trunk lateral flexion angle was defined as the angle between the line formed by both sides of the ASIS and the line formed by the midpoint of the ASIS and episternum. The knee flexion angle was defined by the angle between the line formed by the greater trochanter and lateral epicondyle of the femur and the line formed by the lateral epicondyle of the femur and lateral malleoli. DKV angle was computed using the angle between the line formed between the markers at the ASIS and the middle of the knee joint and the line formed from the markers on the middle of the knee joint to the middle of the ankle joint [37]. The middle of the ankle joint was defined at the midpoint of the medial and lateral malleoli markers, and the middle of the knee joint was defined at the midpoint of the medial and lateral femoral epicondyle markers [44]. Dingenen et al. [43] showed that measurements using the 2D kinematics method is valid and reliable and strongly correlate with data obtained by the 3D kinematics method.
2D kinematics were recorded at the two moments of IC and FF [3]. IC of the first landing phase was defined as the first frame in which ground contact was observed. In contrast, the FF angle was defined as the maximum angle between the femur and shank segments during the ground contact phase [45].
Statistical analysis
To assess the normality of data distribution and homogeneity of variances, Shapiro–Wilk and Levene’s tests were used, respectively. Descriptive statistics were calculated for all variables, and mean, and standard deviation (SD) were reported. Independent samples t-test was applied to compare the demographic characteristics of the two groups. Then, according to the research design, Two-factor ANOVA test 2 (group: experimental, control) × 2 (time: pre-test, post-test) with a group x condition interaction was used to analyze the within and between group evaluation over the eight-week DT training. If a significant interaction effect was found between factors, post-hoc analyses (paired t -test) with Bonferroni adjustment for Pairwise comparisons were applied. Within group factor (pre-test to post-test) as a main effect of time and between-group as a main effect of the group were considered. Percentage changes from pre-test to post-test were calculated. Effect sizes (ES) using partial eta squared were calculated to increase the analysis power. ES were classified as small (0.01), moderate (0.06), and large (0.14) [46]. A modified intention to treat analysis based on the complete case method was used. In this method, since one person was randomly removed from each control and intervention group, they were excluded from the study. The analysis was performed only on those who completed the pre-test and post-test. Findings were analyzed at a significance level of 95%, with a statistical significance of (P < 0.05) and performed using IBM SPSS software (SPSS, version 26, Chicago; IL).
Results
After completing the data collection form, the subjects (mean ± SD; age: 21.86 ± 3.27 years, weight: 68.91 ± 9.55 kg, height: 175.6 ± 6.49 cm, body mass index: 22.36 ± 2.29 kg/m2) were purposefully selected and randomly divided into intervention (n = 15) and control (n = 15) groups (Table 3). Two subjects were lost to follow-up due to personal reasons (control group, n = 1 and intervention group, n = 1). No adverse events were reported (Fig. 1). There was no significant difference between age (P = 0.27), weight (P = 0.63), height (P = 0.71), body mass index (P = 0.54), and sports history (P = 0.11) of both control and intervention groups (Table 3). Pre-test comparisons revealed no significant differences between groups at baseline testing for all 2D kinematic variables (P > 0.05) (Table 4). Therefore, the results of the Shapiro-Wilks and Levene’s tests confirmed that the data were normally distributed, and the variances were homogeneous (P > 0.05). All subjects participated in the pre-test and post-test after 8 weeks.
As per Table 4, repeated measures ANOVA results revealed significant effects of the 8-week DT training. Significant group × time interaction effects were found for the DKV at IC (F1,28 = 6.77; P = 0.01; ES = 0.19), knee flexion at IC (F1,28 = 6.29; P = 0.01; ES = 0.18), knee flexion at FF (F1,28 = 10.07; P = 0.004; ES = 0.26), ankle dorsiflexion at IC (F1,28 = 12.17; P = 0.002; ES = 0.30), and trunk flexion at FF (F1,28 = 18.28; P = 0.001; ES = 0.39) angles. Additionally, significant main effects of time were found for the DKV at FF (F1,28 = 9.67; P = 0.004; ES = 0.25), knee flexion at IC (F1,28 = 14.65; P = 0.001; ES = 0.34), knee flexion at FF (F1,28 = 4.22; P = 0.04; ES = 0.13), ankle dorsiflexion at IC (F1,28 = 16.36; P = 0.001; ES = 0.36), and ankle dorsiflexion at FF (F1,28 = 11.24; P = 0.002; ES = 0.28) angles. The main effect of the group was significant at the knee flexion at FF (F1,28 = 17.42; P = 0.001; ES = 0.38), and ankle dorsiflexion at FF (F1,28 = 5.63; P = 0.02; ES = 0.16) angles.
Post hoc tests showed significant differences in the DKV at IC (F1,28 = 6.33; P = 0.02; ES = 0.31), DKV at FF (F1,28 = 13.47; P = 0.003; ES = 0.49), knee flexion at IC (F1,28 = 20.08; P = 0.001; ES = 0.41), knee flexion at FF (F1,28 = 13.67; P = 0.001; ES = 0.32), ankle dorsiflexion at IC (F1,28 = 37.17; P = 0.001; ES = 0.72), ankle dorsiflexion at FF (F1,28 = 14.52; P = 0.002; ES = 0.50), and trunk flexion at FF (F1,28 = 20.48; P = 0.001; ES = 0.59) angles in the intervention group compared to the control group. However, there was no significant difference between the pre-test and post-test in the control group. Changes in the trunk flexion at IC (F1,28 = 0.54; P = 0.47; ES = 0.03), trunk lateral flexion at IC (F1,28 = 0.006; P = 0.93, ES = 0.00), and trunk lateral flexion at FF (F1,28 = 2.44; P = 0.141, ES = 0.148) angles in the intervention group compared to the control group were not statistically significant (Table 4).
Discussion
The present study aimed to investigate the effect of combining 8 weeks of neuromuscular training with dual cognitive tasks on the landing mechanics of futsal players with knee ligament dominance defects. The current study results demonstrated significant improvements in the DKV, knee flexion, and ankle dorsiflexion at both moments of IC and FF and trunk flexion at FF in the intervention group compared to the control group. However, changes in the trunk lateral flexion in both moments of IC and FF, and trunk flexion at IC in the intervention group compared to the control group was not statistically significant. The results supported the primary hypothesis statistically that a combined 8-week neuromuscular dual cognitive task training program would improve 2D kinematic measures of drop landings compared to a control group.
Previous studies have used DT training to improve the quality of life, gait, physical performance, and balance in the elderly [33, 47] and patients with musculoskeletal disorders [48]. Also, some studies have used DT to examine landing mechanics [10, 42]. Almonroeder et al. [11] concluded that adding cognitive tasks to jumping and landing activities reduced knee flexion angle and increased DKV and ground reaction force compared to alone jumping and landing training. This was the first study to examine the effect of DT training to prevent ACL injury in athletes with neuromuscular defects.
The human body is considered an inter-connected kinetic chain in which compensation movements or defects in one area cause functional defects in other parts of the body [49]. In fact, the movements of a joint are affected by the adjacent joints and affect them as well [50]. Biomechanical patterns that increase the DKV, decrease hip, knee, and trunk flexion, excessive trunk lateral flexion, and ankle dorsiflexion limitation increase the risk of ACL injury [5]. The limitation of the dorsiflexion range of motion prevents the ankle from achieving its closed-pack position and increases the probability of compensation movement patterns [51]. Decreasing trunk flexion in athletes increases the tension on quadriceps muscles to maintain the body's center of gravity and may cause ACL injury [5]. The trunk lateral flexion results in the displacement of the center of gravity and ground reaction force vector to the side, which in the form of kinematic chain reactions, compensates the knee in a dynamic valgus position [16]. Increasing the DKV angle leads to the athlete being near the position of no return, increasing the risk of ACL injury. In addition, Jumping and landing with the knee near full extension is a common mechanism of ACL injury [52].
Previous studies have shown that neuromuscular training improves the DKV and knee flexion angles and decreases the risk of ACL injury in people with biomechanical defects [53, 54]. Myer et al. [55] found that neuromuscular training positively influences lower extremities and thus prevents ACL injuries. However, there is a need to increase the effectiveness of these exercises. Despite comprehensive ACL injury prevention programs, ACL injuries occur considerably due to incorrect movement patterns [10], less compliance with injury prevention training programs to sports [8], and transfer deficiency from conscious awareness to automatic movements, unconscious and unpredictable sport-specific [56]. Athletes perform dynamic movements and cognitive processes simultaneously during the competition. Consequently, ACL injury prevention training programs should be similar to what happens in competition and cognitive challenges [14].
Fitts and Posner determined a model of motor learning that includes three stages: cognitive, associative, and automation, which can be used to learn how to add cognitive challenges to neuromuscular training [24]. The first step in learning is the cognitive stage skill, in which athletes learn how to perform movements and neuromuscular control properly [57]. Following the training progress, the individual enters a stage of associative in which cognitive challenges can be added to neuromuscular training [58]. The highest stage of learning a skill is the automation stage, in which a person can perform neuromuscular training with a safe movement pattern and without needing cognitive attention [57]. At this stage, difficult cognitive tasks can be combined with neuromuscular exercises [24]. Suppose athletes demonstrate good neuromuscular control in the cognitive stage. In that case, neurocognitive challenges (e.g., DT) can be added to their training to assess their readiness to progress to associative, and automation stages [24]. DT is related to two theories of automatic and controlled information processing. Automatic processing is fast and spontaneous, whereas controlled processing is slow and requires working memory and attention control [32]. Probably, DT training improves the transfer of motor skills from the control stage of information processing to the automatic stage [24, 32]. It has been shown that DT training in children improves the transfer effect in the cognitive domain [59].
DT training involves a combination of neuromuscular training with cognitive tasks that increase the subjects' ability to overcome processing limitations in the central nervous system, ultimately leading to the transfer and automation of movement patterns [32, 59]. Training with DT increases the excitability of the brain's dorsolateral prefrontal cortex, which is associated with performing DT, and may reduce the interference of these tasks in competition conditions [30]. Wollesen et al. [59] showed that DT training might improve cognitive and motor performance in children and adolescents. Likewise, Jaiswal et al. [60] revealed that 4 weeks of DT training improves static and dynamic balance, proprioception, pain, strength, and ankle range of motion in participants with chronic ankle instability. In contrast, Cakir et al. [61] investigated the effects of 6 weeks of DT training on physical fitness. They concluded that DT training might improve postural control and does not significantly affect lower limb power.
Given the findings, the neuromuscular dual cognitive tasks training program improved some kinematic indicators (DKV, knee flexion, ankle dorsiflexion at IC and FF, and trunk flexion at FF) landing, which can significantly decrease the risk of ACL injury in athletes. Indeed, DT training had a more effect on the lower limbs' kinematic variables. Reduced ankle dorsiflexion, trunk and knee flexion in the sagittal plane, and increased DKV and trunk lateral flexion in the frontal plane may collectively increase the risk of ACL injury [5]. Aerts et al. [54] showed that neuromuscular training significantly improves maximal knee and hip flexion, and trunk flexion and reduces the DKV angles during jumping and landing. However, this study used only jump and landing exercises.
Regarding not observing significant differences in trunk flexion at IC and trunk lateral flexion at IC and FF angles, it has been shown that core stability training improved trunk neuromuscular control in athletes [62]. One of the possible reasons for the difference in the results can be stated that most of the mentioned studies targeted participants with trunk dominance defects and used special training for core stability [62, 63]. Therefore, changes in the subjects were more significant, while the subjects of the present study were individuals with knee ligament dominance defects. Hence, it can be concluded that core stability exercises are more effective in trunk neuromuscular control compared to DT training. In addition, it is possible that the test was not challenging enough to show differences. Consequently, the researcher guessed that the differences would probably be more obvious if the single-legged drop jump test had been used instead of double-legged drop vertical jump test. The low sample size was another possible reason.
We believe that the results of our study provide valuable insight into the effects of DT training in athletes with neuromuscular defects. It is recommended that coaches, physiotherapists, and rehabilitation specialists should use DT training to improve safe landing mechanics and decrease the risk of ACL injury in futsal players with biomechanical and neuromuscular defects. As in all studies, limitations arise that can affect the results. To our knowledge, this was the first study to investigate landing mechanics during drop vertical jump tests before and after neuromuscular training simultaneously with dual cognitive tasks. Therefore, comparing our results with existing literature was difficult. First, our study only included male futsal players at high risk of ACL injury identified by the tuck jump test. As a result, we cannot generalize our findings to female athletes and patients with ACL injuries. Second, is the lack of using 3D kinematics as a gold standard for assessing landing mechanics. Third, we did not use another group to do neuromuscular training alone. Therefore, we cannot determine if the changes observed in our subjects were due to the neuromuscular training or the emphasis on adding cognitive tasks. Another limitation is that the dual cognitive task included in the DT training (e.g., Forward and backward counting, naming months of the year, simple mathematical problems) is not relevant to futsal. Probably, the use of special DT training will lead to better transfer and retention. For instance, cognitive training can involve the athlete paying attention to teammates' movements instead of simple mathematical problems. Finally, if drop vertical jump, including additional cognitive demands, was used to assess the landing mechanics, the sport-specific tasks were better simulated.
Conclusion
Neuromuscular training with dual cognitive tasks (DT training) improved landing mechanics (dynamic knee valgus, knee flexion, and ankle dorsiflexion in both moments of IC and FF, and trunk flexion at FF angles) in futsal players with knee ligament dominance defects. It is recommended that rehab trainers should use DT training to decrease the risk of ACL injury in futsal players.
Availability of data and materials
The datasets used and/or analyzed during the current study are publicly available from the corresponding author upon reasonable request.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- ES:
-
Effect size
- IC:
-
Initial contact
- FF:
-
Full flexion
- ASIS:
-
Anterior superior iliac spine
- SD:
-
Standard deviation
- DKV:
-
Dynamic knee valgus
- RCT:
-
Randomized controlled trial
- DT:
-
Dual-task
References
Schmikli SL, Backx FJ, Kemler HJ, Van Mechelen W. National survey on sports injuries in the Netherlands: target populations for sports injury prevention programs. Clin J Sport Med. 2009;19(2):101–6.
Junge A, Dvorak J. Injury risk of playing football in Futsal World Cups. Br J Sports Med. 2010;44(15):1089–92.
Giesche F, Wilke J, Engeroff T, Niederer D, Hohmann H, Vogt L, et al. Are biomechanical stability deficits during unplanned single-leg landings related to specific markers of cognitive function? J Sci Med Sport. 2020;23(1):82–8.
DiStefano LJ, Root HJ, Frank BS, Padua DA. Implementation strategies for ACL injury prevention programs. In: Noyes FR, Barber-Westin S, editors. ACL injuries in the female athlete: causes, impacts, and conditioning programs. Berlin: Springer Berlin Heidelberg; 2018. p. 625–39. https://doi.org/10.1007/978-3-662-56558-2_27.
Alentorn-Geli E, Myer GD, Silvers HJ, Samitier G, Romero D, Lázaro-Haro C, et al. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: mechanisms of injury and underlying risk factors. Knee Surg Sports Traumatol Arthrosc. 2009;17(7):705–29.
Grindstaff TL, Beazell JR, Magrum EM, Hertel J. Assessment of ankle dorsiflexion range of motion restriction. Athl Train Sports Health Care. 2009;1(1):7–8.
Sigward SM, Ota S, Powers CM. Predictors of frontal plane knee excursion during a drop land in young female soccer players. J Orthop Sports Phys Ther. 2008;38(11):661–7.
Heidarnia E, Letafatkar A, Khaleghi-Tazji M, Grooms D. Comparing the effect of a simulated defender and dual-task on lower limb coordination and variability during a side-cut in basketball players with and without anterior cruciate ligament injury. J Biomech. 2022;133:110965.
Herman DC, Zaremski JL, Vincent HK, Vincent KR. Effect of neurocognition and concussion on musculoskeletal injury risk. Curr Sports Med Rep. 2015;14(3):194.
Dai B, Cook RF, Meyer EA, Sciascia Y, Hinshaw TJ, Wang C, et al. The effect of a secondary cognitive task on landing mechanics and jump performance. Sports Biomech. 2018;17(2):192–205.
Almonroeder TG, Kernozek T, Cobb S, Slavens B, Wang J, Huddleston W. Cognitive demands influence lower extremity mechanics during a drop vertical jump task in female athletes. J Orthop Sports Phys Ther. 2018;48(5):381–7.
Fedie R, Carlstedt K, Willson JD, Kernozek TW. Effect of attending to a ball during a side-cut maneuver on lower extremity biomechanics in male and female athletes. Sports Biomech. 2010;9(3):165–77.
Farvardin F, Almonroeder TG, Letafatkar A, Thomas AC, Ataabadi PA. The effects of increasing cognitive load on support limb kicking mechanics in male futsal players. J Mot Behav. 2022;54(4):438–46.
Ness BM, Zimney K, Kernozek T, Schweinle WE, Schweinle A. Incorporating a dual-task assessment protocol with functional hop testing. Int J Sports Phys Ther. 2020;15(3):407.
Fort-Vanmeerhaeghe A, Montalvo AM, Lloyd RS, Read P, Myer GD. Intra-and inter-rater reliability of the modified tuck jump assessment. J Sports Sci Med. 2017;16(1):117.
Hewett TE, Myer GD, Ford KR, Heidt RS Jr, Colosimo AJ, McLean SG, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33(4):492–501.
Herrington L, Myer GD, Munro A. Intra and inter-tester reliability of the tuck jump assessment. Phys Ther Sport. 2013;14(3):152–5.
Ghanati HA, Letafatkar A, Almonroeder TG, Rabiei P. Examining the influence of attentional focus on the effects of a neuromuscular training program in male athletes. J Strength Cond Res. 2020;36:1568.
Hewett TE, Myer GD. Reducing knee and anterior cruciate ligament injuries among female athletes–a systematic review of neuromuscular training interventions. J Knee Surg. 2005;18(01):82–8.
Nagano Y, Ida H, Akai M, Fukubayashi T. Effects of jump and balance training on knee kinematics and electromyography of female basketball athletes during a single limb drop landing: pre-post intervention study. Sports Med Arthrosc Rehabil Ther Technol. 2011;3(1):1–8.
Grooms DR, Onate JA. Neuroscience application to noncontact anterior cruciate ligament injury prevention. Sports Health. 2016;8(2):149–52.
Herman DC, Barth JT. Drop-jump landing varies with baseline neurocognition: implications for anterior cruciate ligament injury risk and prevention. Am J Sports Med. 2016;44(9):2347–53.
Gokeler A, Seil R, Kerkhoffs G, Verhagen E. A novel approach to enhance ACL injury prevention programs. J Exp Orthop. 2018;5(1):1–6.
Walker JM, Brunst CL, Chaput M, Wohl TR, Grooms DR. Integrating neurocognitive challenges into injury prevention training: a clinical commentary. Phys Ther Sport. 2021;51:8–16.
Swanik CB, Covassin T, Stearne DJ, Schatz P. The relationship between neurocognitive function and noncontact anterior cruciate ligament injuries. Am J Sports Med. 2007;35(6):943–8.
Faltus J, Criss CR, Grooms DR. Shifting focus: a clinician’s guide to understanding neuroplasticity for anterior cruciate ligament rehabilitation. Curr Sports Med Rep. 2020;19(2):76–83.
Rezola-Pardo C, Arrieta H, Gil SM, Yanguas JJ, Iturburu M, Irazusta J, et al. A randomized controlled trial protocol to test the efficacy of a dual-task multicomponent exercise program in the attenuation of frailty in long-term nursing home residents: aging-ONDUAL-TASK study. BMC Geriatr. 2019;19(1):1–9.
Bherer L, Kramer AF, Peterson MS, Colcombe S, Erickson K, Becic E. Transfer effects in task-set cost and dual-task cost after dual-task training in older and younger adults: further evidence for cognitive plasticity in attentional control in late adulthood. Exp Aging Res. 2008;34(3):188–219.
Fleddermann M-T, Heppe H, Zentgraf K. Off-court generic perceptual-cognitive training in elite volleyball athletes: task-specific effects and levels of transfer. Front Psychol. 2019;10:1599.
Kimura T, Matsuura R. Additional effects of a cognitive task on dual-task training to reduce dual-task interference. Psychol Sport Exerc. 2020;46:101588.
Almonroeder TG, Kernozek T, Cobb S, Slavens B, Wang J, Huddleston W. Divided attention during cutting influences lower extremity mechanics in female athletes. Sports Biomech. 2019;18(3):264–76.
Moreira PED, Dieguez GTdO, Bredt SdGT, Praça GM. The acute and chronic effects of dual-task on the motor and cognitive performances in athletes: a systematic review. Int J Environ Res Public Health. 2021;18(4):1732.
Sarulatha Haridass DMM, Vasanthan Rajagopalan DRV. Progressive dual task training for improving physical performance in older adults with impaired balance. Ann Roman Soc Cell Biol 2021:2167–74.
Ruthruff E, Van Selst M, Johnston JC, Remington R. How does practice reduce dual-task interference: Integration, automatization, or just stage-shortening? Psychol Res. 2006;70(2):125–42.
Ghaderi M, Letafatkar A, Almonroeder TG, Keyhani S. Neuromuscular training improves knee proprioception in athletes with a history of anterior cruciate ligament reconstruction: a randomized controlled trial. Clin Biomech. 2020;80:105157.
Lago-Fuentes C, Rey E, Padrón-Cabo A, de Rellán-Guerra AS, Fragueiro-Rodríguez A, García-Núñez J. Effects of core strength training using stable and unstable surfaces on physical fitness and functional performance in professional female futsal players. J Hum Kinet. 2018;65(1):213–24.
Saito A, Okada K, Sasaki M, Wakasa M. Influence of the trunk position on knee kinematics during the single-leg landing: Implications for injury prevention. Sports Biomech. 2020:1–14.
Dingenen B, Staes FF, Santermans L, Steurs L, Eerdekens M, Geentjens J, et al. Are two-dimensional measured frontal plane angles related to three-dimensional measured kinematic profiles during running? Phys Ther Sport. 2018;29:84–92.
Dingenen B, Barton C, Janssen T, Benoit A, Malliaras P. Test-retest reliability of two-dimensional video analysis during running. Phys Ther Sport. 2018;33:40–7.
Paterno MV, Schmitt LC, Ford KR, Rauh MJ, Myer GD, Huang B, et al. Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med. 2010;38(10):1968–78.
Jardim NYV, Bento-Torres NVO, Costa VO, Carvalho JPR, Pontes HTS, Tomás AM, et al. Dual-task exercise to improve cognition and functional capacity of healthy older adults. Front Aging Neurosci. 2021;13:33.
Schnittjer A, Simon JE, Yom J, Grooms DR. The effects of a cognitive dual task on jump-landing movement quality. Int J Sports Med. 2021;42(01):90–5.
Dingenen B, Malfait B, Vanrenterghem J, Robinson MA, Verschueren SM, Staes FF. Can two-dimensional measured peak sagittal plane excursions during drop vertical jumps help identify three-dimensional measured joint moments? Knee. 2015;22(2):73–9.
Dingenen B, Malfait B, Vanrenterghem J, Verschueren SM, Staes FF. The reliability and validity of the measurement of lateral trunk motion in two-dimensional video analysis during unipodal functional screening tests in elite female athletes. Phys Ther Sport. 2014;15(2):117–23.
Ruiz-Pérez I, Elvira JL, Myer GD, Croix MDS, Ayala F. Criterion-related validity of 2-dimensional measures of hip, knee and ankle kinematics during bilateral drop-jump landings. Eur J Hum Mov. 2021;47:100–20.
Cohen J. A power primer. Psychol Bull. 1992;112(1):155.
Falbo S, Condello G, Capranica L, Forte R, Pesce C. Effects of physical-cognitive dual task training on executive function and gait performance in older adults: a randomized controlled trial. BioMed Res Int. 2016;2016:1.
An H-J, Kim J-I, Kim Y-R, Lee K-B, Kim D-J, Yoo K-T, et al. The effect of various dual task training methods with gait on the balance and gait of patients with chronic stroke. J Phys Ther Sci. 2014;26(8):1287–91.
Hein T, Schmeltzpfenning T, Krauss I, Maiwald C, Horstmann T, Grau S. Using the variability of continuous relative phase as a measure to discriminate between healthy and injured runners. Hum Mov Sci. 2012;31(3):683–94.
Sheikhi B, Letafatkar A, Thomas AC, Ford KR. Altered trunk and lower extremity movement coordination after neuromuscular training with and without external focus instruction: a randomized controlled trial. BMC Sports Sci Med Rehabil. 2021;13(1):1–9.
Fong C-M, Blackburn JT, Norcross MF, McGrath M, Padua DA. Ankle-dorsiflexion range of motion and landing biomechanics. J Athl Train. 2011;46(1):5–10.
Myer GD, Ford KR, Hewett TE. Rationale and clinical techniques for anterior cruciate ligament injury prevention among female athletes. J Athl Train. 2004;39(4):352.
Herrington L. The effects of 4 weeks of jump training on landing knee valgus and crossover hop performance in female basketball players. J Strength Cond Res. 2010;24(12):3427–32.
Aerts I, Cumps E, Verhagen E, Wuyts B, Van De Gucht S, Meeusen R. The effect of a 3-month prevention program on the jump-landing technique in basketball: a randomized controlled trial. J Sport Rehabil. 2015;24(1):21–30.
Myer GD, Ford KR, McLean SG, Hewett TE. The effects of plyometric versus dynamic stabilization and balance training on lower extremity biomechanics. Am J Sports Med. 2006;34(3):445–55.
Gokeler A, Benjaminse A, Hewett TE, Paterno MV, Ford KR, Otten E, et al. Feedback techniques to target functional deficits following anterior cruciate ligament reconstruction: implications for motor control and reduction of second injury risk. Sports Med. 2013;43(11):1065–74.
Fitts PM. Perceptual-motor skill learning. In: Categories of human learning. Elsevier; 1964. p. 243–85. https://doi.org/10.1016/B978-1-4832-3145-7.50016-9.
Wulf G. Attentional focus and motor learning: a review of 15 years. Int Rev Sport Exerc Psychol. 2013;6(1):77–104.
Wollesen B, Janssen TI, Müller H, Voelcker-Rehage C. Effects of cognitive-motor dual task training on cognitive and physical performance in healthy children and adolescents: a scoping review. Acta Physiol. 2022;224:103498.
Jaiswal S, Rishi P, Sen S. Efficacy of dual task training on ankle stability in chronic ankle sprain. 2022.
Cakir BA, Turkkan M, Ozer O. Effects of adding cognitive motor coordination exercise to soccer training vs. soccer training alone on physical fitness of prepubescent boys. Int J Appl Exerc Physiol. 2020;9(6):234–42.
Sasaki S, Tsuda E, Yamamoto Y, Maeda S, Kimura Y, Fujita Y, et al. Core-muscle training and neuromuscular control of the lower limb and trunk. J Athl Train. 2019;54(9):959–69.
Jeong J, Choi D-H, Shin CS. Core strength training can alter neuromuscular and biomechanical risk factors for anterior cruciate ligament injury. Am J Sports Med. 2021;49(1):183–92.
Acknowledgements
The authors would like to thank all the athletes for participation in this study.
Funding
None.
Author information
Authors and Affiliations
Contributions
Each author has contributed individually and significantly to the development of the manuscript. MHG, AA, MHN contributed to the original idea, study design, and protocol, the conception of the work, conducting the study,and revising the drafting and editing of the article. MHG, and MHN contributed to the conception of the work, writing, and editing of this article. All authors read and approved the final version of the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of the Sports Sciences Research Institute with ID number (IR.SSRI.REC.1400.1071). The participants were informed about the details of the study and provided written informed consent before study enrolment. Informed consent was obtained from all the participants, and procedures were conducted according to the Declaration of Helsinki.
Consent for publication
Informed consent was obtained from all individuals or their legal guardians to publish identifying images in an online open access publication.
Competing interests
The authors declare no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hamoongard, M., Hadadnezhad, M. & Abbasi, A. Effect of combining eight weeks of neuromuscular training with dual cognitive tasks on landing mechanics in futsal players with knee ligament dominance defect: a randomized controlled trial. BMC Sports Sci Med Rehabil 14, 196 (2022). https://doi.org/10.1186/s13102-022-00593-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-022-00593-0