
Abstract
This study aimed to examine the effects of two high-intensity interval training programs (HIIT) on maximal aerobic velocity (MAV), hematological variations and muscle damage markers in young healthy adults. Twenty-nine male physical education students, aged 20.3 ± 3.3 years, volunteered to participate in this study, and were randomly assigned to a control group (CG, n = 9) or two intervention groups (group 1 or 2). Intervention group 1 (n = 10) exercised at 100% of their MAV (EG100) while group 2 (n = 10) exercised at 110% MAV (EG110). Before and after the eight week training program, blood samples were drawn at rest, before, and after an intermittent exercise. Aspartate aminotransferase (ASAT), alanine aminotransferase (ALAT), C reactive protein (CRP), creatine kinase (CK) concentrations and hematological parameters (white blood cells [WBC], monocytes [MO], lymphocytes [LY], neutrophil [NE]) and lactate dehydrogenase (LDH) were measured. Post-hoc tests showed that MAV was significantly higher in EG110 compared to EG100 after HIIT (p < 0.01, ηp2 = 0.05), whilst ALAT, ASAT, and CPR were significantly lower (p < 0.01; 0.02 < ηp2 < 0.11) in EG110 compared to EG100. Moreover, post-hoc tests indicated that LY decreased significantly (p < 0.001, ηp2 = 0.21) only for EG110. Furthermore, there were significant positive correlations for both EG100 and EG110 between MAV and ALAT (r = 0.66, p = 0.044 and r = 0.64, p = 0.041 respectively), CK (r = 0.67, p = 0.031 and r = 0.86, p = 0.030, respectively), LDH (r = 0.74, p = 0.014, and r = 0.071, p = 0.021, respectively). In addition, there was a significant positive correlation for both, EG100 and EG110 between MAV and LY (r = 0.79, p < 0.01; r = 0.72, p < 0.05, respectively). Concerning the relationship between MAV and NE, there was a significant positive correlation (r = 0.66; p < 0.05) only for EG110. Findings from this study revealed that HIIT at 110% MAV was more efficient to improve MAV and reduce muscle damage. In addition, we observed significant associations between performance improvements (MAV) and markers of muscle damage.
Similar content being viewed by others

Background
It is well-established that acute high intensity physical exercise can have negative effects on inflammatory mediators [1, 2]; concurrently, however, long-term physical training has the potential to enhance performance markers such as maximal aerobic velocity (MAV), improve immune function, and reduce inflammation [3]. Training intensity appears to play a key mediating role in directing the effects of exercise bouts towards biopositive or negative responses. In fact, several studies showed signicant MAV improvements after 3.5 to 7.0 weeks of HIIT [4,5,6]. Recently, Rhibi et al. [5] showed a significant MAV enhancement after 8 weeks of HIIT in male physical education students. Furthermore, the exercise immunology literature is consistent regarding post-exercise cell count increases (leucocytosis, neutrophil [NE], monocytosis [MO], and lymphocytosis [LY]) after a single bout of high-intensity swimming [6, 7] or cross‐country skiing [8]. Brancaccio et al. [9] showed that white blood cells (WBC) increased significantly during high-intensity maximal tasks. There is evidence that physical activity may also alter homocysteine metabolism by increasing protein and/or methyl-group turnover [10]. In fact, Nieman [11] proposed a model of immune response to training named the inverted-U model. In fact, the immune status was gradually improved in response to an increase in physical activity. However, it was decreased in response to high intensity training. Moreover, different studies showed a slight decrease in the immune parameters in response to high intensity training or overtraining programs in athletes [12, 13]. However, no modification was observed in mitogens activity after 60 min of running at 95% of VMA in trained runners. Interestingly, there is also evidence that the leucocytosis induced by intense exercise (90–105% of maximal aerobic velocity [MAV]) could be due to the general increase in muscle damage [14].
It is well-established that prolonged physical exercise results in transient elevations of biochemical markers of muscular damage such as aspartate aminotransferase (AST), alanine aminotransferase (ALT), creatine kinase (CK), and lactate deshydrogenase (LDH) [9]. Previous studies reported a signifcant increase in CRP [15, 16], CK [15,16,17], and LDH [15, 18] after training programs. In fact, Anđelković et al. [15] found that CRP, CK, and LDH concentrations increased after 90 days of soccer training. Silva et al. [16] showed an increase in CRP and CK levels at the end of a soccer season in professional soccer players. In contrast, Requena et al. [19] observed that CK remained unaltered and LDH concentration decreased after the off-season rest period. Gharahdaghi et al. [20] showed a significant reductions in LDH and CK concentration at rest in response to 4 weeks of high-intensity aerobic training.
The literature also suggests that long-term training could affect the different muscle damage markers mentioned above [21]. Thus, it is important to determine the optimal intensity and duration during high-intensity interval training (HIIT) to achieve performance improvements (e.g., MAV) and at the same time to minimize the muscular damage and the potential injury risks [22]. Likewise, exercise intensity is an important factor contributing to sarcolemma disruption, allowing the release of enzymes of damaged muscle into the blood [23]. In recent years, trainers/coaches and athletes have sought contemporary training modes to yield performance improvements and induce optimal adaptation [24]. Indeed, moderate exercise (55–75% MAV) stimulates the immune system and may be somewhat responsible for exercise related reduction in fatigue and illness [25]. However, high intensity exercise (90–100% MAV) induces immunosuppression in the recovery period and may explain the increased risk of infection in athletes [25]. In endurance sports, during the cycles of high training volume and intensity that include consecutive training sessions with little recovery time in between, athletes may experience a temporarily diminished performance concomitant with an immunodepression state [26, 27]. Indeed, stiffness and soreness following a period of exercise are less when the exercise is repeated a week later; the result of adaptation by the muscle [28]. However, none of these studies have examined the variation in muscular damage markers in response to a HIIT exercise program, despite the known efficiency of this training type for performance improvement.
In addition, HIIT protocols enable individuals to maintain sub-maximal (90% MAV at least), maximal (100% MAV), or supra maximal (> 100% MAV) intensities. In this context, Millet et al. [29] showed that the time recorded at 90% of V̇O2max were significantly higher during 30 s IE at 105% V̇O2max than IE at 100% V̇O2max. Ballor and Volovsek [30] showed that increasing exercise intensity (from 90 to 110% MAV) could improve the mean V̇O2 (from 63.5 to 69.6% MAV) measured during IE. In addition, Thevenet et al. [31] showed that no significant difference was found in t90 V̇O2max or t95 V̇O2max values in response to 100% or 110% MAV IE. Indeed, IE at 100–110% MAV did not allow all participants reaching at least 90 or 95% of V̇O2max (only 2 out of 9 tested participants) [31]. Thus, it is plausible that higher exercise intensities might allow a greater improvement in aerobic performance and the fatigue resistance at high intensity effort. However, a high exercise intensity can induce central or peripheral fatigue which could possibly impair sports performance [32]. To our knowledge, there are no published longitudinal data pertaining to the effects of increasing the exercise intensity of intermittent exercise and the resultant muscle damage and hematological responses. Given the lack of research in this area, the aim of the current study was to examine the influence of eight weeks of HIIT, at different intensities (100% MAV vs. 110% MAV), on MAV, muscle damage markers and hematological parameters in young adults. Based on the extant literature [33, 34], we hypothesized that increasing training intensity could lead to better muscular adaptations in order to reduce muscular damage markers after short and intense intermittent exercise, and that any HIIT would yield greater changes than the control group.
Methods
Participants
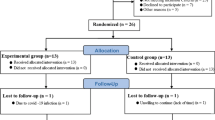
Twenty-nine male physical education students volunteered to participate in this study, and were randomly assigned into three groups: a control group (CG, n = 9; age: 22.0 ± 1.2 years) and two experimental groups (EG). EG100 comprised n = 10 individuals aged 21.4 ± 1.1 years and EG110 included n = 10 participants aged 21.9 ± 1.3 years. More information on the experimental groups will be provided in the next paragraph. Age of participants and their physical characteristics were measured before and after HIIT and are displayed in Table 1. The participants were informed of all the procedures of the experiment including performance of the exercise training protocols and possible risks associated with its administration in accordance with the Helsinki Declaration. Prior to participation, the participants underwent a medical examination and were fully informed about the experimental procedures and signed consent was obtained from the participants. Approval was granted by the Research Ethics Committee of the University of Rennes 2, Rennes, France.
Experimental approach
All subjects visited the laboratory for a familiarization session to get to know the applied experimental set-up (e.g., tests). During this session, anthropometrics (i.e., body height and mass, percentage body fat) were taken. All measurements were performed by the same investigator in accordance with the positions and techniques established by the International Biological Program [35].
Study exclusion criteria comprised any contraindications to maximal exercise testing (e.g., cardiovascular or pulmonary disease), endocrine disorders, and metabolic syndrome symptoms (e.g., hypertension). All participants were healthy, without any injuries during the past six months prior to the start of the study.
Before and after HIIT, all participants performed a maximal graded test [36] to determine their maximal aerobic velocity (MAV). Thereafter, subjects in the EG100 and EG110 groups carried out an intermittent exercise test consisting of repeated 30 s intensive runs at 100% MAV (EG100) or 110% MAV (EG110) (Fig. 1). Between the bouts, a 30 s active recovery was allowed (50% MAV). The runs were repeated until exhaustion. The CG only performed the maximal graded test and the intermittent exercise test before and after HIIT. Participants of both EG100 and EG110 performed another maximal graded test at the mid of the HIIT program (at the 5th week) in order to assess MAV and to update the training speeds for the remaining weeks of the training program. All tests took place in the morning and were performed until full exhaustion on a 400 m outdoor tartan track, at the same time of day, with 48 h of rest between tests. Our study took place in ambient temperatures ranging from 16 to 22 °C and humidity from 50 to 75% with a wind speed < 2 m/s. For each test, the participants were verbally encouraged to run at maximal effort. Testing was stopped if participants could not maintain the required speed or if they stopped the tests due to exhaustion. Before and after the HIIT programs, all tests (maximal graded test and intermittent exercise) were completed within 2 weeks (Fig. 1).

Study design for both experimental groups and control groups and experimental design for blood sampling
Anthropometric measurements
Body mass was measured to the nearest 0.1 kg, with the participants in light clothing and unshod, using an electronic scale (Kern, MFB 150K100). Height was determined to the nearest 0.5 cm with a measuring tape fixed to the wall. All measurements were performed by the same examiner, in accordance with the positions and techniques established by the International Biological Program. Percent body fat was determined using four skinfolds and a Harpenden caliper [37]. The fat free mass was calculated by subtracting the fat mass from the body mass.
Maximal graded test
To determine participants’ MAV, a maximal graded test was performed on a track, in a stadium according to Cazzorla and Léger [36] The initial speed was 8 km h–1 and this was increased by 0.5 km h–1 every minute. The running pace was given by an examiner, equipped with a whistle and a chronometer and made a short sound when the subject had to pass a cone to be able to maintain a constant speed. A longer sound marked the change in the running stage. The velocity at the finally completed stage was determined as MAV. The accuracy of MAV was considered to be equal to the velocity during the previous stage plus 0.5 km h−1 [38].
Intermittent exercise (IE) test
Participants performed, as long as possible, a 30 s run at 100% MAV (EG100) or 110% MAV (EG110) alternating with 30 s active recovery (50% MAV). These tests were carried out on the same track as the maximal graded test. Before each test, we calculated, as a function of the MAV of each subject, the required distance to be covered during the 30 s intensive runs at 100% MAV, 110% MAV, and the 30 s active recovery at 50% MAV. During the recovery period, a longer sound was made at mid-period (15 s) to inform the athletes of the remaining time for the end of recovery and make a U-turn. The distance performed for 30 s at both intensities (100% or 110% MAV) was calculated based on the following equation: Distance = Velocity × time. The 30 s IE was preceded by a standardized warm-up consisting of 10 min continuous jogging, followed by 5 min of the participant’s usual stretching routine, five short bursts of accelerations on the track, and 2 min rest.
High intensity interval training programs
EG100 and EG110 groups participated in the HIIT program three times per week for a total of 8 weeks making up 24 exercise sessions (Table 2). The HIIT sessions were separated by at least 48 h to allow sufficient recovery. All HIIT sessions included three different periods according to the procedures previously described by Rhibi et al. [5, 39]. In brief, the sessions started with a standardized warm-up which consisted of 15 min continuous jogging, followed by 5 min dynamic stretching exercises and 5 short bursts of accelerations on the track. During every training session on the track, there was one subject per lane. All different distances for each athlete (running and recovery intervals) were fixed by the examiner before every exercise session. The subjects began from a standing position, behind a cone. Thereafter, they performed the HIIT session. For these training sessions, the subjects’ pace was provided by an examiner emitting sounds at regular intervals up to the end of the exercise session. During the 30 s recovery period, subjects had to cover a distance determined according to their own MAV. At the end of each HIIT session, subjects cooled down for ~ 5 min by running at low intensity, and performing dynamic stretching. Two members of our laboratory supervised all HIIT sessions. The two intervention groups (EG100 and EG110) performed similar training volumes across the study period. In contrast to EG100 and EG110, CG did not participate in any additional exercise program, but continued their regular compulsory physical education program at the university.
Blood sampling and analysis
Pre and post the intervention period, blood samples were taken before the 30 s intermittent exercise test. All venous blood samples were drawn upon arriving at the laboratory, where a heparinized catheter (Insyte-W, 1.1 mmo.d. × 30 mm) was inserted into an antecubital vein. Subjects then rested quietly, for 20 min. Thereafter, a blood sample (10 mL) was taken to determine resting concentration. Samples were placed in an ice bath and centrifuged immediately. Aliquots of the resulting plasma were stored at − 80 °C until analyzed. Blood was collected in two tubes: the first heparinized tube was used to determine aspartate aminotransferase (ASAT), alanine aminotransferase (ALAT), C reactive protein (CRP), creatine kinase (CK) and lactate dehydrogenase (LDH) concentrations. The second EDTA tube was used to determine hematological parameters (i.e., white blood cells—WBC) and principal derivative subpopulations such as monocytes (MO), lymphocytes (LY) and neutrophil (NE). The ALAT, ASAT, CRP, CK and LDH concentrations were determined using a multiparametric analyzer Konelab 30™ (Thermo Electron Corporation). ALAT and ASAT activities were determined enzymatic method using kinetic method (UV). The intra-assay coefficient of variation for the ALAT and ASAT kit was 1.4 and 1.8%, respectively. CRP activity was determined using an Immunoturbidimetry method. The intra-assay coefficient of variation for the CRP kit was 1.7%. CK activity was determined using UV method (IFCC) by the N-acetyl-cysteine method. The intra-assay coefficient of variation for the CK kit was 1.8%. LDH activity was determined by enzymatic rate method (IFCC). The intra-assay coefficient of variation for the LDH kit was 1.1%. Haematological parameters were generally performed within 3 h in a multichannel automated Hematology Analyzer Sysmex XS-1000i. We measured simultaneously red blood cells, WBC and principal derivative subpopulations such as NE, LY and MO.
Statistical analyses
Data were reported as means and standard deviations (± SD). Normality of data was tested and confirmed for all variables using the Kolmogorov–Smirnov procedure. Levene’s test was used to determine homogeneity of variance. Test–retest reliability for all tests was assessed using intra-class correlation coefficients (ICCs) [40]. The effects of exercise were evaluated using a two-way analysis of variance (ANOVA) with repeated measures (3 groups × 2 times). If group by time interactions turned out to be significant, Bonferroni adjusted post-hoc tests were computed. Greenhouse–Geisser corrections were used when the assumption of sphericity (Mauchly’s test) was violated. Partial eta-squared (ηp2) was calculated to assess the practical significance for all ANOVA outcomes. Values of 0.01–0.059, 0.06–0.13, and ≥ 0.14 were considered as small, intermediate and large effects, respectively [41]. We also calculated predefined contrasts analyses [42] to specifically test the following hypothesis, H1) any HIIT condition would yield greater improvements in the outcome measures than the control group. Accordingly, we compared the control condition vs EG100 and EG110 (coded as − 0.667, 0.333, and 0.333, respectively). This approach yielded a comparison of one (or more) condition(s) vs. the grand mean of the specified contrasts. Indeed, post-hoc analysis, while useful, does not, alone, yield sufficient insight into multiple levels or detailing patterns in response; whereas, contrast analysis allows researchers to test theory-driven expectations directly against empirically derived group or cells means [43, 44]. In addition, we plotted pre-post changes (deltas Δ) of performance measures (MAV) with deltas in hematological variations and muscle damage markers using Pearson’s product moment correlation coefficients (r). Statistical significance was set, a priori¸ at p < 0.05. The statistical analysis was carried out using Statistica Version 13.2 software (StatSoft, France) and R (R Core Team (2018). R: A Language and environment for statistical computing. [Computer software]. Retrieved from https://cran.r-project.org/) using the Car:Anova package (Fox & Weisberg [45]; car: Companion to Applied Regression. [R package]. Retrieved from https://cran.r-project.org/package=car).
Results
An a posteriori power calculation was computed using G*Power (Version 3.1, University of Düsseldorf, Germany) and the primary outcome parameter of this study MAV. As input parameters for G*power, we used the following variables from this study: effect size for MAV group by time interaction (ηp2 = 0.61, equals Cohen’s f = 1.25), alpha error = 0.05, N = 29 total sample size, three groups and two tests. The post hoc power analysis showed an actual power of 0.99.
No testing or training related injuries occurred over the study period, and the attendance rates were 100% for the two exercise groups (e.g., EG100 and EG110). Pre and post test results are outlined in Tables 3 and 4. No significant between-group baseline differences were found for any of the analyzed parameters.
Maximal aerobic velocity (MAV)
A significant main effect of time was observed for MAV performances (F = 84.39; p < 0.001; ηp2 = 0.71; power = 0.99). A significant group × time interaction was found for MAV (F = 18.26; p < 0.001; ηp2 = 0.61; power = 0.99). Post-hoc tests revealed significant (p < 0.001) pre-to-post improvements for MAV performances in EG100 (ηp2 = 0.08, + 5.8%) and EG110 (ηp2 = 0.10, + 8.9%) compared to CG. Post hoc tests revealed also higher MAV performances (p = 0.01; ηp2 = 0.05) in EG110 compared to EG100 after HIIT. A pilot study was recorded to assess the reliability and the sensitivity of this test using 29 participants and showed 0.94 ICC and 95% CI (0.88–0.98).
Muscle damage markers
Significant main effects of time were observed for ALAT (F = 27.21; p < 0.001; ηp2 = 0.68; power = 0.99), ASAT (F = 14.49; p < 0.001; ηp2 = 0.66; power = 0.95), CRP (F = 6.05; p < 0.001; ηp2 = 0.41; power = 0.66), CK (F = 18.31; p < 0.001; ηp2 = 0.82; power = 0.98), and LDH (F = 13.45; p < 0.001; ηp2 = 0.61; power = 0.95). Significant group × time interactions were identified for ALAT (F = 15.54; p = 0.007; ηp2 = 0.16; power = 0.99), ASAT (F = 1.92; p = 0.004; ηp2 = 0.17; power = 0.88), CRP (F = 8.50; p = 0.009; ηp2 = 0.02; power = 6.21), CK (F = 9.28; p = 0.003; ηp2 = 0.08; power = 0.84), and LDH (F = 5.97; p = 0.006; ηp2 = 0.33; power = 0.93). Post hoc tests revealed significant pre-to post decreases (p < 0.001) in both EG100 and EG110 for ALAT (ηp2 = 0.06; ηp2 = 0.16, respectively) and ASAT (ηp2 = 0.05; ηp2 = 0.10, respectively). Post hoc tests revealed that ALAT (p = 0.04; ηp2 = 0.05) and ASAT (p = 0.02; ηp2 = 0.06) were significantly lower in EG110 (ALAT:—3.0 ± 1.6; ASAT: − 2.9 ± 3.7) compared to EG100 (ALAT: − 1.8 ± 0.9; ASAT: − 1.9 ± 1.7) after HIIT. Post hoc tests revealed significant pre-to post decreases for CRP in EG100 (p = 0.03; ηp2 = 0.12; − 12.5%) and EG110 (p = 0.02; ηp2 = 0.02; − 8.6%) and for LDH in EG100 (p = 0.005; ηp2 = 0.19; − 13.1%) and EG110 (p < 0.001; ηp2 = 0.11; − 20%). However, CK decreased only for EG110 (p = 0.01; ηp2 = 0.12, − 15.7%), after HIIT.
A pilot study was recorded to assess the reliability and the sensitivity of this parameters using 29 participants and showed 0.91 ICC and 95% confidence interval (CI) of 0.83–0.95 for ALAT, 0.89 ICC and 95% CI of 0.72–0.96 for ASAT, 0.93 ICC and 95% CI of 0.75–0.98 for CRP, 0.95 ICC and 95% CI of 0.89–0.96 for CK and 0.95 ICC and 95% CI of 0.84–0.98 for LDH.
Contrast analysis (muscle damage)
Contrast analysis indicated that adherence to any HIIT condition (EG100 and EG110) significantly reduced ALAT (Est:2.62, SE:0.51, t(28) = 5.07, p < 0.001) and LDH (Est:32, SE:9.09, t(28) = 3.51, p = 0.001) vs. the control condition. However, contrast analysis highlighted no significant changes for ASAT (Est:1.73, SE:1.06, t(28) = 1.63, p = 0.11), CRP (Est:0.28, SE:0.26, t(28) = 1.08, p = 0.28), and CPK (Est:14.25, SE:14.82, t(28) = 0.96, p = 0.34), for HIIT conditions vs. control.
Hematological parameters
Significant main effects of time were found for WBC (F = 14.92; p < 0.001; ηp2 = 0.82; power = 0.96), NE (F = 24.72; p < 0.001; ηp2 = 0.59; power = 0.99), LY (F = 12.41; p < 0.001; ηp2 = 0.73; power = 0.93), and MO (F = 7.22; p < 0.001; ηp2 = 0.62; power = 0.74). Significant group × time effects were observed for WBC (F = 0.81; p = 0.022; ηp2 = 0.14; power = 0.99), NE (F = 5.49; p = 0.015; ηp2 = 0.15; power = 0.71), LY (F = 8.97; p = 0.002; ηp2 = 0.17; power = 0.83), and MO (F = 5.76; p = 0.004; ηp2 = 0.10; power = 0.63). Post hoc tests revealed significant pre-to post decreases in both EG100 and EG110 for WBC (p = 0.013, p = 0.002, respectively; ηp2 = 0.03, ηp2 = 0.04, respectively; − 5.6%, − 7.0%, respectively), and for NE (p < 0.001; ηp2 = 0.07, ηp2 = 0.05, respectively; − 7.5%, − 9.8%, respectively). However, post hoc tests revealed a significant decrease in LY (p = 0.02; ηp2 = 0.21, − 22.2%) only in EG110 after HIIT.
A pilot study was conducted to assess the reliability and the sensitivity of this parameters using 29 participants, and showed an ICC of 0.97 and 95% CI of 0.91—0.99 for WBC, 0.89 ICC and 95% CI of 0.78—0.94 for NE, 0.87 ICC and 95% CI of 0.69—0.88 for LY and 0.89 ICC and 95% CI of 0.78—0.93 for MO.
Contrast analysis (hematology)
Contrast analysis indicated that any HIIT condition (EG100 and EG110) significantly reduced WBC (Est:0.45, SE:0.11, t(28) = 4.29, p = 0.002) and NE (Est:0.33, SE:0.07, t(28) = 4.68, p < 0.001) vs. the control condition. However, contrast analysis highlighted no significant changes for LY (Est:0.32, SE:0.16, t(28) = 2.03, p = 0.06) and MO (Est:0.06, SE:0.06, t(28) = 1.12, p = 0.27), for HIIT conditions vs. control.
Relationships between deltas in MAV with deltas in hematological parameters and muscle-damage markers
Table 5 illustrates that pre-post changes in MAV correlated with pre-post changes in hematological and muscle-damage markers in the range of 0.40 to 0.79. Significant correlations were found between MAV and ALAT (r = 0.66, p < 0.05), MAV and CK (r = 0.67, p < 0.05), MAV and LDH (r = 0.74, p < 0.05), MAV and LY (r = 0.79, p < 0.01) for EG100. However, there were no significant correlations between MAV and ASAT, CRP and WBC for EG100.
For EG110, significant correlations were found between MAV and ALAT (r = 0.64, p < 0.05), MAV and CK (r = 0.86, p < 0.05), MAV and LDH (r = 0.071, p < 0.05), MAV and LY (r = 0.72, p < 0.01) and MAV and NE (r = 0.66; p < 0.05). However, there were no significant correlations between MAV and ASAT, CRP and WBC for EG110.
Discussion
This study compared the effects of eight weeks of HIIT, at 100% MAV vs. 110% MAV, on performance development (i.e., MAV), muscle damage markers, and hematological parameters in young active men. The main findings of this study were that HIIT at 110% MAV induced higher MAV values compared to 100% MAV. Indeed, HIIT at 110% MAV induced lower ASAT, ALAT, LDH, NE, and LY concentrations than exercising at 100% MAV. There were significant correlations (p < 0.05) between MAV and ASAT, ALAT, LDH, NE, and LY in EG100 and EG110. However, no statistically significant effect of any exercise modality was observed for MO, WBC, CRP, and CK.
Effects of increasing intensity on performance development
Our results showed a significant improvement in aerobic performances after HIIT in both trained groups compared to pre-intervention. Our findings agree with previous results reported in the literature. Indeed, several studies reported significant increases in V̇O2max and MAV after 4 to 7 weeks of a HIIT program [46, 47]. In addition, in our study, MAV performances recorded after HIIT were significantly better in EG110 compared to EG100. These differences seem to be dependent on the intensity of exercise, since EG100 presented smaller improvement in MAV performance compared to EG110 [39], whilst both HIIT conditions yielded significant improvements vs. the control group.
Muscular damages markers variations in response to HIIT
After HIIT training, we found significantly decreased responses compared to pre-intervention in ALAT, ASAT, CRP, and LDH, in both EG100 and EG110 groups. Furthermore, after HIIT, ALAT and ASAT concentrations were significantly lower in EG110 compared to EG100. Furthermore, specific contrast analysis indicated that adherence to any HIIT condition (EG100 and EG110) significantly reduced ALAT and LDH compared to the control condition. This study showed significant positive correlations between pre-post changes in MAV with deltas in ALAT for EG100 (r = 0.66; p < 0.05) and EG110 (r = 0.64; p < 0.05). These findings suggest that high intensity exercise has an impact on selected biochemical markers of muscular damage.
How training programs reduce inflammation and CRP levels is not well defined [48]. However, exercise training related reductions in fat mass have been associated with a larger reduction in CRP [34]. Musa et al. [33] showed significant decreases in high-density lipoprotein (HDL) cholesterol and triglycerides levels after 8 weeks of HIIT, whilst Kessler et al. [49], in their literature review, also reported that HIIT improved HDL cholesterol after a minimum of 8 weeks of HIIT. Physical activity is related to several factors that are independently correlated with lower CRP levels [50]. Moreover, Mauger et al. [51] noted that CRP production was significantly positively correlated with IL-6, and inversely correlated with HDL-C levels. Indeed, CRP metabolism has been linked to liver fat deposition, and therefore altered uptake of triglyceride-rich lipoprotein would be predicted to affect CRP metabolism [52]. Thus, the decrease of CRP observed in the present study could be explained by cholesterol and triglycerides’ concentrations.
After the HIIT program, CK levels were significantly lower in the EG110 group compared to before training. Our results are concordant with those of Baird et al. [53], who showed that, although the mechanism(s) by which CK is cleared from the blood has not been fully elucidated, it is likely that the observed serum CK levels reflect complex interactions associated with energy status and scale of muscle disturbance [53]. In agreement, Brewster et al. [54] showed that higher levels of tissue CK activity may increase the cellular energy and improve muscular contraction. However, it is less clear why physical exercise should result in release of CK into the blood [53]. Moreover, according to Baird et al. [53], when total work time is equalized by inversely varying intensity and duration, the greatest rise in CK levels occurs in the highest-intensity (80% MAV) exercise with the shortest duration (170 repetitions), compared to the session with a longer duration (524 repetitions) and lower intensity exercise (30% MAV). Indeed, these results support the possibility of higher CK levels with increasing exercise intensity.
Main et al. [55] showed that increases in muscle damage could explain the decrease in muscle performance after 8 weeks of endurance training program. Thus, the decrease of muscle damage we observed (i.e., CK) after HIIT, in both EG100 and EG110, could be partly explanatory for the increasing performance. Furthermore, in our study, after HIIT, MAV values were significantly higher in EG110 than EG100. In this study, we observed a significant positive correlation between deltas in MAV with pre-post changes in CK (r = 0.67; r = 0.86; respectively; all p < 0.05) for EG100 and EG110.
Therefore, HIIT seems to improve aerobic performances, by increasing intermittent exercise intensity, without a notable difference in muscular damage markers level. According to Morgan [56], the inflammatory response during exercise is related to the muscular metabolism and the degree of muscular lesion development. Morgan [56] suggested that the subsequent muscular adaptation process involved an increase in the number of sarcomeres in series of muscle fibers after a training program, based on specific repeated running training. Thus, after a HIIT program, compared to before, the decrease of muscular damage markers observed in both groups in the present study could be manifest through muscular adaptations processes. Accordingly, we speculate that the 30 s intermittent exercise with 110% MAV probably lead to non-uniform sarcoma elongation, that could explain muscles adaptations compared to 100% MAV [56]; of course, the veracity of this claim must be addressed in further mechanistic studies.
Our study showed that LDH concentrations were significantly lower in EG110 compared to EG100 after the HIIT program. The LDH decrease in EG110 after HIIT could be mainly attributed to aerobic pathway intervention. Indeed, according to the duration, the human body uses increasingly aerobic pathway to produce a sufficient quantity of ATP for exercise [57]. This action promotes the decrease of LDH activity [58, 59], and can explain the diminution of LDH found in our study after HIIT using 110% MAV. Previous studies have reported a significant increase of LDH in response to acute exercise, such as weightlifting, high intensity exercise, and after maximal graded tests [60, 61]. This increase could be explained by the increase of V̇O2 during exercise, which causes oxidative stress and muscle damage [62]. This study showed significant positive correlations for between MAV and LDH (r = 0.74, r = 0.071, respectively; p < 0.05) for EG100 and EG110.
Hematological parameters variations in response to HIIT
Our study showed that WBC and NE decreased significantly in both EG100 and EG110 after HIIT compared to pre-intervention. However, LY decreased significantly only in the EG110 group after HIIT compared to before. Furthermore, specific contrast analysis indicated that adherence to any HIIT condition (EG100 and EG110) significantly reduced WBC and NE compared to the control condition. There was a significant positive correlation between MAV and and LY (r = 0.79, r = 0.72, respectively; p < 0.01) for EG100 and EG110. The decreases in WBC, NE and LY previously defined after HIIT could be reflective of the "open window" concept [63]. Indeed, in monitoring the changes in humoral and cellular immune parameters following endurance exercise, it has been proposed that this type of exercise can induce a suppression of some immune variables which may make the individuals more susceptible to pathogens [64]. Our results were in accordance with those of Morgado et al. [7], who showed that the cumulative effects of training loads induced an overall reduction of the ability of the immune system to respond after a training program. Kakanis et al. [65] found that intermittent exercise training (at 90% of the subject’s second ventilatory threshold) provoked a temporary reduction in immune function (i.e., respiratory burst response, proliferation). However, Nieman [66] found that moderate intensity (< 3 moderate-to vigorous aerobic session of > 20 min) training program, over 15 weeks (5 sessions / week), induced an increase (+ 20%) in immunoglobulin and a diminution in LY. Likewise, many studies do not indicate changes in immune function past 2 h after the completion of exercise.
Strengths and limitations of the study
The present study represents a novel addition to the literature; indeed, to our knowledge, there are no published data concerning increasing the exercise intensity of intermittent exercise and the resultant muscle damage and hematological responses. We hypothesized that increasing intensity training could lead to better performance development (MAV) in order to reduce muscular damage markers after short and intense intermittent exercise, and that any HIIT would yield greater changes than the control group. Accordingly, these hypotheses were robustly, statistically, addressed using ANOVA and post-hoc testing, including specific contrast analysis. As to this study’s limitations, we acknowledge that a greater sample size would have been preferable, and further work that is appropriately powered is now required. However, we assert that this work represents the first of its’ type, and will provide a platform for further research. While our study focused on measures of aerobic performance, biochemical and hematological parameters to examine the muscular damages, a comparison of muscle soreness and muscular strength could further strengthen and explain our findings.
Practical applications
When coaches prescribe exercise programs, two essential aims are sought; improve performance and avoid injuries. To that end, we suggest the HIIT program based on IE at 110% MAV appears feasible, because it does not induce additional muscle damage compared to the intervention group that performed at 100% MAV. However, based on contrast analysis, it is evident that participating to either HIIT protocols outlined in the present study would elicit significant muscular and hematological improvements.
Conclusions
In conclusion, 8-weeks of HIIT, at both 100% and 110% MAV, had significant positive effects on damage and hematological measures, vs. control. Moreover, training HIIT at a 110% MAV intensity was more efficient for improving MAV with + 9.07 ± 3.38% and reducing damage biomarkers (ALAT, ASAT, CK and LDH), vs. 100% MAV, in physically active young men.
Availability of data and materials
The datasets generated during and analyzed during the current study are not publicly available due to confidential information about the participants but are available from the corresponding author on reasonable request.
Abbreviations
- HIIT:
-
High-intensity interval training programs
- MAV:
-
Maximal aerobic velocity
- V̇O2 :
-
Oxygen consumption
- ASAT:
-
Aspartate aminotransferase
- ALAT:
-
Alanine aminotransferase
- CRP:
-
C reactive protein
- CK:
-
Creatine kinase
- WBC:
-
White blood cells
- MO:
-
Monocytes
- LY:
-
Lymphocytes
- NE:
-
Neutrophil
- LDH:
-
Lactate dehydrogenase
- ANOVA:
-
2-Way analysis of variance
- ES:
-
Effect size
References
Meckel Y, Eliakim A, Seraev M, Zaldivar F, Cooper DM, Sagiv M, et al. The effect of a brief sprint interval exercise on growth factors and inflammatory mediators. J Strength Cond Res. 2009;23:225–30.
Meckel Y, Nemet D, Bar-Sela S, Radom-Aizik S, Cooper DM, Sagiv M, et al. Hormonal and inflammatory responses to different types of sprint interval training. J Strength Cond Res. 2011;25:2161–9.
Walsh NP, Gleeson M, Shephard RJ, Gleeson M, Woods JA, Bishop NC, et al. Position statement. Part one: immune function and exercise. Exerc Immunol Rev. 2011;17:6–63.
Denadai BS, Ortiz MJ, Greco CC, de Mello MT. Interval training at 95% and 100% of the velocity at VO2 max: effects on aerobic physiological indexes and running performance. Appl Physiol Nutr Metab. 2006;31:737–43.
Rhibi F, Zouhal H, Lira FS, Ouerghi N, Prioux J, Besbes S, et al. Inflammatory cytokines and metabolic responses to high-intensity intermittent training: effect of the exercise intensity. Biol Sport. 2021;39:263–72.
Morgado JP, Monteiro CP, Teles J, Reis JF, Matias C, Seixas MT, et al. Immune cell changes in response to a swimming training session during a 24-h recovery period. Appl Physiol Nutr Metab. 2016. https://doi.org/10.1139/apnm-2015-0488.
Morgado JP, Monteiro CP, Matias CN, Reis JF, Teles J, Laires MJ, et al. Long-term swimming training modifies acute immune cell response to a high-intensity session. Eur J Appl Physiol. 2018;118:573–83.
Yamada K, Nakata M, Horimoto N, Saito M, Matsuoka H, Inagaki N. Measurement of glucose uptake and intracellular calcium concentration in single, living pancreatic beta-cells. J Biol Chem. 2000;275:22278–83.
Brancaccio P, Lippi G, Maffulli N. Biochemical markers of muscular damage. Clin Chem Lab Med. 2010;48:757–67.
Joubert LM, Manore MM. Exercise, nutrition, and homocysteine. Int J Sport Nutr Exerc Metab. 2006;16:341–61.
Nieman DC. Immune response to heavy exertion. J Appl Physiol (1985). 1997;82(5):1385–94. https://doi.org/10.1152/jappl.1997.82.5.1385.
Hack V, Strobel G, Weiss M, Weicker H. PMN cell counts and phagocytic activity of highly trained athletes depend on training period. J Appl Physiol (1985). 1994;77(4):1731–5. https://doi.org/10.1152/jappl.1994.77.4.1731.
Gleeson M, McDonald WA, Pyne DB, Cripps AW, Francis JL, Fricker PA, Clancy RL. Salivary IgA levels and infection risk in elite swimmers. Med Sci Sports Exerc. 1999;31(1):67–73. https://doi.org/10.1097/00005768-199901000-00012.
Pyne DB. Exercise-induced muscle damage and inflammation: a review. Aust J Sci Med Sport. 1994;26:49–58.
Anđelković M, Baralić I, Đorđević B, Stevuljević JK, Radivojević N, Dikić N, et al. Hematological and biochemical parameters in elite soccer players during a competitive half season. J Med Biochem. 2015;34:460–6.
Silva JR, Rebelo A, Marques F, Pereira L, Seabra A, Ascensão A, et al. Biochemical impact of soccer: an analysis of hormonal, muscle damage, and redox markers during the season. Appl Physiol Nutr Metab. 2014;39:432–8.
Pimenta E, Coelho D, Capettini LS, Gomes T, Pussieldi G, Ribeiro J, et al. Analysis of creatine kinase and alpha-actin concentrations in soccer pre-season. Rev Brasil de Ciên. 2015. https://doi.org/10.18511/0103-1716/rbcm.v23n4p5-14.
Coppalle S, Rave G, Ben Abderrahman A, Ali A, Salhi I, Zouita S, et al. Relationship of pre-season training load with in-season biochemical markers, injuries and performance in professional soccer players. Front Physiol. 2019;10:409.
Requena B, García I, Suárez-Arrones L, Sáez de Villarreal E, Naranjo Orellana J, Santalla A. Off-season effects on functional performance, body composition, and blood parameters in top-level professional soccer players. J Strength Cond Res. 2017;31:939–46.
Gharahdaghi N, Kordi MR, Shabkhiz F. Acute exercise-induced muscular damage after one month training in soccer players. Ovidius Univ Ann Ser Phys Educ Sport Sci Movement Health. 2013;13:S269–S269.
Saidi K, Abderrahman AB, Hackney AC, Bideau B, Zouita S, Granacher U, et al. Hematology, hormones, inflammation, and muscle damage in elite and professional soccer players: a systematic review with implications for exercise. Sports Med. 2021;51:2607–27.
Proske U, Morgan DL. Muscle damage from eccentric exercise: mechanism, mechanical signs, adaptation and clinical applications. J Physiol. 2001;537(Pt 2):333–45.
Brancaccio P, Maffulli N, Limongelli FM. Creatine kinase monitoring in sport medicine. Br Med Bull. 2007;81–82:209–30.
Del Giacco SR, Scorcu M, Argiolas F, Firinu D, Del Giacco GS. Exercise training, lymphocyte subsets and their cytokines production: experience of an italian professional football team and their impact on allergy. Biomed Res Int. 2014;2014.
Pedersen BK, Hoffman-Goetz L. Exercise and the immune system: regulation, integration, and adaptation. Physiol Rev. 2000;80:1055–81.
Gleeson M. Immune function in sport and exercise. J Appl Physiol. 1985;2007(103):693–9.
Rama L, Teixeira AM, Matos A, Borges G, Henriques A, Gleeson M, et al. Changes in natural killer cell subpopulations over a winter training season in elite swimmers. Eur J Appl Physiol. 2013;113:859–68.
Nosaka K, Clarkson PM. Muscle damage following repeated bouts of high force eccentric exercise. Med Sci Sports Exerc. 1995;27:1263–9.
Millet GP, Libicz S, Borrani F, Fattori P, Bignet F, Candau R. Effects of increased intensity of intermittent training in runners with differing VO2 kinetics. Eur J Appl Physiol. 2003;90:50–7.
Ballor DL, Volovsek AJ. Effect of exercise to rest ratio on plasma lactate concentration at work rates above and below maximum oxygen uptake. Eur J Appl Physiol. 1992;65:365–9.
Thevenet D, Leclair E, Tardieu-Berger M, Berthoin S, Regueme S, Prioux J. Influence of recovery intensity on time spent at maximal oxygen uptake during an intermittent session in young, endurance-trained athletes. J Sports Sci. 2008;26:1313–21.
Buchheit M, Laursen PB. High-intensity interval training, solutions to the programming puzzle: part I: cardiopulmonary emphasis. Sports Med. 2013;43:313–38.
Musa DI, Adeniran SA, Dikko AU, Sayers SP. The effect of a high-intensity interval training program on high-density lipoprotein cholesterol in young men. J Strength Cond Res. 2009;23:587–92.
Swift DL, Johannsen NM, Earnest CP, Blair SN, Church TS. Effect of exercise training modality on C-reactive protein in type 2 diabetes. Med Sci Sports Exerc. 2012;44:1028–34.
Weiner JS, Lourie JA. Human biology: a guide to field methods. Oxford: Published for the International Biological Programme by Blackwell Scientific; 1969.
CAZORLA Georges, Luc Leger. Comment évaluer et développer vos capacités aérobies : épreuve progressive de course navette, épreuve progressive de course sur piste VAMEVAL. 1993.
Durnin JVGA, Womersley J. Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged from 16 to 72 years. Br J Nutr. 1974;32:77–97.
Kuipers H, Verstappen FT, Keizer HA, Geurten P, van Kranenburg G. Variability of aerobic performance in the laboratory and its physiologic correlates. Int J Sports Med. 1985;6:197–201.
Rhibi F, Prioux J, Attia MB, Hackney AC, Zouhal H, Abderrahman AB. Increase interval training intensity improves plasma volume variations and aerobic performances in response to intermittent exercise. Physiol Behav. 2019;199:137–45.
Vincent WJ, Weir JP. Statistics in Kinesiology. 4th ed. Human Kinetics Inc.; 2011.
Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. New York: Routledge; 1988.
Abdi H, Williams LJ. Overview principal component analysis.
Rosnow RL, Rosenthal R. “Some things you learn aren’t so”: cohen’s paradox, asch’s paradigm, and the interpretation of interaction. Psychol Sci. 1995;6:3–9.
Rosnow RL, Rosenthal R. Computing contrasts, effect sizes, and counternulls on other people’s published data: general procedures for research consumers. Psychol Methods. 1996;1:331–40.
Fox J, Weisberg S. Visualizing fit and lack of fit in complex regression models with predictor effect plots and partial residuals. J Stat Softw. 2018;87:1–27.
Ben Abderrahman A, Zouhal H, Chamari K, Thevenet D, de Mullenheim P-Y, Gastinger S, et al. Effects of recovery mode (active vs. passive) on performance during a short high-intensity interval training program: a longitudinal study. Eur J Appl Physiol. 2013;113:1373–83.
Burgomaster KA, Howarth KR, Phillips SM, Rakobowchuk M, MacDonald MJ, McGee SL, et al. Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. J Physiol. 2008;586(Pt 1):151–60.
Dongway AC, Faggad AS, Zaki HY, Abdalla BE. C-reactive protein is associated with low-density lipoprotein cholesterol and obesity in type 2 diabetic sudanese. Diabetes Metab Syndrome Obesity Targets Ther. 2015;8:427–35. https://www.dovepress.com/c-reactive-protein-is-associated-with-low-density-lipoprotein-choleste-peer-reviewed-article-DMSO. Accessed 14 Jan 2021.
Kessler HS, Sisson SB, Short KR. The potential for high-intensity interval training to reduce cardiometabolic disease risk. Sports Med. 2012;42:489–509.
Kasapis C, Thompson PD. The effects of physical activity on serum C-reactive protein and inflammatory markers: a systematic review. J Am Coll Cardiol. 2005;45:1563–9.
Mauger J-F, Lévesque J, Paradis M-E, Bergeron N, Tchernof A, Couture P, et al. Intravascular kinetics of C-reactive protein and their relationships with features of the metabolic syndrome. J Clin Endocrinol Metab. 2008;93:3158–64.
Reinehr T, Stoffel-Wagner B, Roth CL, Andler W. High-sensitive C-reactive protein, tumor necrosis factor alpha, and cardiovascular risk factors before and after weight loss in obese children. Metabolism. 2005;54:1155–61.
Baird MF, Graham SM, Baker JS, Bickerstaff GF. Creatine-kinase- and exercise-related muscle damage implications for muscle performance and recovery. J Nutr Metab. 2012;2012: 960363.
Brewster LM, Mairuhu G, Bindraban NR, Koopmans RP, Clark JF, van Montfrans GA. Creatine kinase activity is associated with blood pressure. Circulation. 2006;114:2034–9.
Main LC, Dawson B, Heel K, Grove JR, Landers GJ, Goodman C. Relationship between inflammatory cytokines and self-report measures of training overload. Res Sports Med. 2010;18:127–39.
Morgan DL. New insights into the behavior of muscle during active lengthening. Biophys J. 1990;57:209–21.
Baker JS, McCormick MC, Robergs RA. Interaction among skeletal muscle metabolic energy systems during intense exercise. J Nutr Metab. 2010;2010.
Farhana A, Lappin SL. Biochemistry, lactate dehydrogenase. StatPearls: StatPearls Publishing; 2020.
Dubouchaud H, Butterfield GE, Wolfel EE, Bergman BC, Brooks GA. Endurance training, expression, and physiology of LDH, MCT1, and MCT4 in human skeletal muscle. Am J Physiol Endocrinol Metab. 2000;278:E571–9.
Ammar A, Chtourou H, Hammouda O, Trabelsi K, Chiboub J, Turki M, et al. Acute and delayed responses of C-reactive protein, malondialdehyde and antioxidant markers after resistance training session in elite weightlifters: effect of time of day. Chronobiol Int. 2015;32:1211–22.
Ceci R, Beltran Valls MR, Duranti G, Dimauro I, Quaranta F, Pittaluga M, et al. Oxidative stress responses to a graded maximal exercise test in older adults following explosive-type resistance training. Redox Biol. 2013;2:65–72.
Hammouda O, Chahed H, Chtourou H, Ferchichi S, Miled A, Souissi N. Morning-to-evening difference of biomarkers of muscle injury and antioxidant status in young trained soccer players. Biol Rhythm Res. 2012;43:431–8.
Gomez-Merino D, Drogou C, Chennaoui M, Tiollier E, Mathieu J, Guezennec CY. Effects of combined stress during intense training on cellular immunity, hormones and respiratory infections. NeuroImmunoModulation. 2005;12:164–72.
Pedersen BK, Bruunsgaard H. How physical exercise influences the establishment of infections. Sports Med. 1995;19:393–400.
Kakanis MW, Peake J, Brenu EW, Simmonds M, Gray B, Hooper SL, et al. The open window of susceptibility to infection after acute exercise in healthy young male elite athletes. Exerc Immunol Rev. 2010;16:119–37.
Nieman DC. Immunonutrition support for athletes. Nutr Rev. 2008;66:310–20.
Acknowledgements
The authors would like to thank all the students from the ISSEP of Ksar Said—Tunisia for their participation, as well as the medical team of the El-Kassab hospital, Manouba-Tunisia.
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors acknowledge the support of the Deutsche Forschungsgemeinschaft (DFG) and Open Access Publishing Fund of the University of Freiburg, Germany.
Author information
Authors and Affiliations
Contributions
FR, ABA, JP and HZ conceived and designed the research. FR and ABA conducted the experiments. FR, CCTC, BB and SB contributed to the analysis of data. FR, ABA, ACH, UG and H.Z. drafted the manuscript and analysed the data. All authors critically revised the manuscript. All authors have read and approve the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The participants were informed of all the procedures of the experiment including performance of the exercise training protocols and possible risks associated with its administration in accordance with the Helsinki Declaration. Prior to participation, the participants underwent a medical examination and were fully informed about the experimental procedures and signed consent was obtained from the participants. We confirmed that that informed consent was obtained from all the participants. Approval was granted by the Research Ethics Committee of the University of Rennes 2, Rennes, France.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Rhibi, F., Abderrahman, A.B., Prioux, J. et al. Effects of different training intensities in high-intensity interval training (HIIT) on maximal aerobic velocity, hematological and muscle-damage markers in healthy young adults. BMC Sports Sci Med Rehabil 14, 158 (2022). https://doi.org/10.1186/s13102-022-00550-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-022-00550-x