
Abstract
Background
We assessed the effects of gender, in association with a four-week small-sided games (SSGs) training program, during Ramadan intermitting fasting (RIF) on changes in psychometric and physiological markers in professional male and female basketball players.
Methods
Twenty-four professional basketball players from the first Tunisian (Tunisia) division participated in this study. The players were dichotomized by sex (males [GM = 12]; females [GF = 12]). Both groups completed a 4 weeks SSGs training program with 3 sessions per week. Psychometric (e.g., quality of sleep, fatigue, stress, and delayed onset of muscle soreness [DOMS]) and physiological parameters (e.g., heart rate frequency, blood lactate) were measured during the first week (baseline) and at the end of RIF (post-test).
Results
Post hoc tests showed a significant increase in stress levels in both groups (GM [− 81.11%; p < 0.001, d = 0.33, small]; GF [− 36,53%; p = 0.001, d = 0.25, small]). Concerning physiological parameters, ANCOVA revealed significantly lower heart rates in favor of GM at post-test (1.70%, d = 0.38, small, p = 0.002).
Conclusions
Our results showed that SSGs training at the end of the RIF negatively impacted psychometric parameters of male and female basketball players. It can be concluded that there are sex-mediated effects of training during RIF in basketball players, and this should be considered by researchers and practitioners when programing training during RIF.
Similar content being viewed by others


Background
The demands of team sports in general, and basketball in particular, are determined by the interaction between physical, perceptual, mental, and technical-tactical aspects [1,2,3]. In this context, previous studies have suggested that small-sided games (SSGs) are a particularly relevant training strategy in basketball, since they can simultaneously promote the development of physical, physiological, and technical-tactical aspects required in competition [4,5,6,7,8,9].
However, studies involving cognitive effects of SSGs in basketball players are rare. To the authors’ knowledge, there are only two studies available in the literature so far [4, 10]. Moreover, previous investigations have demonstrated how increased mental demands can worsen perceived exertion [11, 12] and, importantly, physical [12, 13] and technical performance [11, 12] of team sport players. Furthermore, several studies have reported that psychometric disturbances affect sport performance [14, 15]. Thus, researchers have recommended using different scales to investigate recovery, perceived exertion, and well-being to monitor the physiological and psychometric status of players [8, 9, 16]. Indeed, these scales are effective in detecting early signs of tiredness and monitoring well-being to allow for optimization of training to achieve high-level performance [9, 16]. Previous studies have reported that the total quality recovery (TQR) scale is a valid tool that can be used to assess recovery state between training sessions [14, 17, 18]. In this context, Brink et al. [19] reported that TQR did not predict submaximal HR and was not associated with maximum shuttle race test performance. Moreover, Freitas et al. [17] reported that eleven days of an intense training load induced a significant decrease in TQR in volleyball players; whilst Osiecki et al. [18] showed that TQR was not related to the rating of perceived exertion (RPE), but was strongly associated with recovery state and biomarkers for muscle damage in professional soccer players. In addition, Selmi et al. [9] indicated that RPE in SSGs was not influenced by TQR or variability in well-being indices.
Of importance, training sessions, preparation phases, and basketball national and international tournaments can span the month of Ramadan intermitting fasting (RIF), which forces Muslim basketball players to fast, whilst concomitantly maintaining good performances and to continue training at the prescribed load or the intensity of their training [20,21,22]. Previous studies have revealed important physiological and cognitive RIF impacts in athletes, and basketball players in particular, because of the required abstention of food and water for a period exceeding 28 consecutive days [19,20,21,22,23]. In this context, Brini et al. [20] have shown for basketball and Baklouti et al. [23] for soccer that SSGs are common drills used by coaches for training during RIF, since SSGs allow maintenance and development of aerobic fitness in a practical way and lead to a greater motivation especially during RIF.
Moreover, male and female basketball players may respond differently to SSGs training during RIF for instance due to the menstrual cycle. In fact, females are obliged to interrupt their fasting state during the period of menstruation for religious reasons. Furthermore, there is a limited number of studies in the literature that examined the effects of sex during SSGs in basketball, where such studies have been limited to physiological effects in which male players induces a significant higher average heart rate and blood lactate concentration (during 4vs.4 SSG) in comparison with female players [24]. Moreover, research on the effects of sex on sport performances during RIF is scarce, and of the minimal available literature, results are unclear between sexes, perhaps owing to menstruation in females, which alters the observance of RIF during such days [25]. Thus, it would be interesting to control those parameters and to investigate the sex-mediated effects in association with SSGs training during RIF.
To the best of our knowledge, no previous study has investigated the effects of sex, in association with SSGs training, during RIF on psychometric and physiological markers in professional male and female basketball players. Accordingly, we sought to explore the sex-mediated effects of SSGs during RIF on well-being indices (e.g., including perceived ratings of sleep, fatigue, stress, and DOMS), TQR and physiological responses (e.g., heart rate frequency, blood lactate). Considering the previous literature [21, 23, 26], we hypothesized that: 1) psychometric and physiological parameters would be negatively affected by RIF in both sexes; and 2) it would be a sex-mediated effects in association with SSGs training during RIF.
Methods
Participants
Twenty-four professional basketball players from the first Tunisian division (Tunisia) participated in this study (Table 1). The players were assigned, according to their sex, to two groups (males [GM = 12]; females [GF = 12]), where each group included 3 guards, 3 shooting guards, 2 small forwards, 2 forwards, and 2 centers. The inclusion criteria for study participation were 1) participation in at least 90% of the training sessions; 2) Muslims who were fasting during Ramadan; and 3) having good health (no pain or injury reported); 4) and not taking any medications or other drugs; 5) for the female group, the menstrual cycle is longer than 28 days which starts at the beginning of Ramadan. The study was conducted during the competitive season and was approved by the Clinical Research Ethics Committee of the High Institute of Sports and Physical Education of Kef, University of Jendouba, Kef, Tunisia (approval No. 9/2018) and the protocol was conducted in accordance with the Declaration of Helsinki. All participants provided their written informed consent to participate in the study.
Study design and experimental procedure
Players were familiarized with all experimental procedures before the start of the study. To minimize any effects of diurnal variations, the training sessions were conducted at the same time of day. Players were instructed to wear the same footwear during all test sessions.
Overall, the study lasted 5 weeks and was conducted during the 2018/2019 in-season. The experimental period started with the beginning of the month of Ramadan in May 2019 and lasted until June 2019. During the Ramadan period, participants exercised five times per week between 5:30 and 7:00 pm and completed one game per week on the weekend. GM and GF completed a 4 weeks SSGs training (see details below) with a frequency of three sessions per week (Monday, Wednesday and Friday) over the course of the study period. No additional exercises or strength and conditioning sessions were conducted by any of the experimental groups.
Training sessions for both groups started with a 15-min warm-up program consisting of 5 min of low-intensity running, 5 min of dynamic stretching, and 5 min of skipping exercises [27], followed by technical and tactical drills based on basic basketball movements (i.e., offensive, ready stance, running, change of direction, linear sprint, stopping, pivoting, and jumping exercises), specific basketball movements (triple threat position, pivot, face up or one- and two-phase stop), basketball technique fundamentals (dribbling, passing, and shooting), basic defensive movements (defensive stance, defensive slide, denial defense, and box-out) and a simulated game at the end of every session [27], which were identical for both groups. Both groups completed the same training volume (~ 90 min per session) over the course of the study (Table 2).
Small-sided games training program
SSGs were performed on half-court (14 × 15 m) (35 m2 per player) at the beginning of the training session. The duration of each SSG was 12 min. The defensive strategy allowed was player-to-player only. The training regimes consisted of three 4-min bouts interspersed by 2 min of passive recovery, the court size and the duration of 3 vs. 3 SSGs were strictly controlled, as reported in previous studies [12, 28]. The players were asked to perform at maximum effort during the games.
Two coaches were positioned around the perimeter of the court to encourage the players and to provide new balls when necessary to allow for continuous play and to maintain the game pace during the SSGs sessions (Table 3).
Training load monitoring
To determine whether the players’ global training load remained constant throughout the study, the session rating of perceived exertion (RPE) training score was taken after each session. About 30-min after training, players were asked to rate the global intensity of the entire workout session using the category ratio-10 RPE scale according to the methods described by Foster [29]. A daily training load was created by multiplying the training duration (minutes) by the session RPE. The weekly training load was determined by summing the daily training loads for each athlete during each week.
Anthropometrics and fitness measurements
Body mass (kg) was measured with an electronic scale (Pharo 200 Analytic, Germany) and height (m) with a portable stadiometer (Seca, Maresten, UK). Maximal oxygen consumption (VO2max) was estimated using the 20-m shuttle run test, according to the Léger and Gadoury equation [30].
Psychometric markers
Fifteen minutes before the warm-up, each player was asked to complete ratings of well-being indices (quality of sleep, fatigue, stress, and DOMS) considering the timeline from the last SSGs training session until the moment of the new training session. Players rated each index using a scale from 1 to 7 points, where 1 indicated “very, very low” (fatigue, stress, and DOMS) or “good” (quality of sleep) and 7 indicated “very, very high” (fatigue, stress, and DOMS) or “bad” (quality of sleep) [8]. The sum of these 4 scores was used to calculate the HI. A higher HI score indicates a more negative state of well-being. After each player completed the well-being indices, recovery state was evaluated using the TQR scale [9]. The TQR scale ranges from 6 to 20, where 6 indicates “very, very poor recovery” and 20 indicates “very, very good recovery.” This scale has been used in previous studies as an indicator of athletes’ perceived recovery [9]. Immediately at the end of each SSG, RPE was evaluated using the Borg CR-10 scale [29] to assess subjective training intensity.
Physiological measures
HR was continuously monitored throughout the training intervention by HR monitors (Polar Team Sport System; Polar-Electro OY, Kempele, Finland) and was recorded at 5-s intervals. To reduce HR recording error, all players were regularly asked to check their HR monitors during SSGs. The mean HR for each bout was calculated from continuous HR data. The resulting mean HRs for each SSG were further averaged to obtain the overall mean HR (HRmean).
Blood samples for the determination of blood lactate concentration ([Lac]) were collected 3 min after training in the absence of an active recovery [31]. Blood samples, taken from the fingertip of the index finger, were analyzed by a validated portable analyzer (Lactate Pro, Arkray, Japan) [31].
Statistical analyses
All the data were expressed as Mean ± SD. The Shapiro Wilk test identified all variables as normally distributed. Baseline between group differences were computed using t-tests for independent samples. If statistically significant between group baseline differences were found, analysis of covariance (ANCOVA) with group as between-subject comparator (GM and GF) was performed, and baseline data as a covariate [32]. In addition, group-specific repeated-measures analyses of variance (time: pre, post) were applied to evaluate within-group pre-to-post performance. Effect sizes (ESs) were calculated by converting partial eta-squared to Cohen’s d. Effect sizes were classified as small (0 ≤ d ≤ 0.50), medium (0.50 ≤ d ≤ 0.80), and large (d ≥ 0.80) [33]. The significance level was set at p ≤ 0.05, a priori. All analyses were performed using Statistical Package for Social Sciences (SPSS) version 20.0 (SPSS, Inc., Chicago, IL).
Results
All players from both groups completed the study, according to the previously described methodology. Training load remained constant throughout the study, and no injuries were reported. During the four weeks intervention period, adherence rates were 96.5% for GM and 95.8% for GF. The average playing time per game was 29.4 ± 1.8 min for GM and 29.2 ± 1.5 min for GF. No statistically significant between group differences were observed for these measures.
ANCOVA was carried out for psychometric and physiological markers, because there was a significant difference for baseline values between the two groups, except for stress levels, TQR and Lac.
Psychometric markers
Table 4 presents baseline data for psychometric markers. ANCOVA revealed no significant effect of group for any measure of psychometric markers at post-test (sleep [d = 0.005, small, p = 0.742]; fatigue [d = 0.019, small, p = 0.526]; DOMS [d = 0.011, small, p = 0.636]; HI [d = 0.013, p = 0.606]; RPE [d = 0.029, small, p = 0.438]). However, significant pre-to-post-test increases were found for those parameters in both groups, except for RPE where there was a pre-to-post-test increase for GM, only (sleep: GM [d = 0.93, large, p < 0.001] and GF [d = 0.86, large, p < 0.001]; fatigue: GM [d = 0.89, large, p < 0.001] and GF [d = 0.71, p < 0.001]; DOMS: GM [d = 0.90, large, p < 0.001] and GF [d = 0.86, large, p < 0.001]; HI: GM [d = 0.95, large, p < 0.001] and GF [d = 0.90, large, p < 0.001]; RPE: GM [d = 0.72, medium, p < 0.001] and GF [d = 0.28, small, p = 0.061]).
Concerning stress levels and TQR, ANOVA revealed a significant main effect of time ([p < 0.001, d = 0.82, large]; [p < 0.001, d = 0.90, large] respectively) and a significant group x time interaction only for stress levels (p = 0.014, d = 0.44, small). Bonferroni corrected post hoc tests showed a significant increase in stress levels for both groups (GM [− 81.11%; p < 0.001, d = 0.33, small]; GF [− 36.53%; p = 0.001, d = 0.25, small]).
Physiological measures
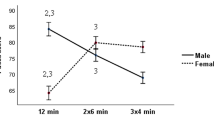
Table 4 presents baseline data for physiological markers. ANCOVA revealed significantly lower HR in favor of males at post-test (1.70%, d = 0.38, small, p = 0.002). Moreover, significant pre-to-post-test changes for HR were found for both groups (GM [2.30%, d = 0.67, medium, p < 0.001] and GF [1.96%, d = 0.82, large, p < 0.001]) (Fig. 1). Concerning Lac, ANOVA revealed only a significant main effect of group (p = 0.031, d = 0.36, small).

Variation of heart rates mean during Ramadan for male, female groups. Legend. HR: heart rates; GM: male group; GF: female group
Discussion
This study investigated the sex-mediated effects of SSGs training during Ramadan on psychometric status (quality of recovery and well-being indices) and physiological responses (HR, blood lactate) in professional male and female basketball players. The main findings of our study indicated that psychometric parameters (i.e., well-being indices) were negatively impacted as a result of RIF for both groups, and that SSGs training elicited a higher HR for female professional basketball players, at the end of RIF. Additionally, players maintained a high training load during the period of the study (2000 AU for GM and 1800 AU for GF) in order to sustain competitive fitness and muscle mass. Our values were similar to these reported in Italian soccer players (1900 AU) (in-season) but lower than overreached rugby league players [34].
Blood lactate concentration did not significantly change throughout RIF for both groups. These results indicated that the participating players maintained similar metabolic conditions for each SSGs session. Moreover, no significant sex-mediated effects were found, which could be explained by the fact that blood lactate concentration is affected not only by the lactate diffusion into the blood but also by the blood volume into which it diffuses; indeed, because women have a smaller total blood volume (4.0 to 4.5 l) than men (5.0 to 6.0 l), a smaller amount of lactate would be required to produce a similar blood lactate concentration [35].
We found that HR significantly decreased at the end of Ramadan for both groups in comparison with the first week. Accordingly, Al Suwaidi et al. [36] explained this decrease by the association of fasting with catecholamine inhibition and reduced venous return, causing a decrease in the sympathetic tone, which leads to a decrease in blood pressure, HR, and cardiac output. Moreover, our results showed that the male group had a significantly lower HR in comparison with the female group. These values could be explained by the recovery capacity of our participants between bouts. In fact, it has been reported that male players have a quicker recovery ability than the female players. Sex-related differences might also be a result of the males’ having a 5–30% greater VO2max and having lower body fat percentage than their female counterparts [37].
Concerning RPE scores, we recorded a higher value at the end of RIF. Our findings could be explained by the increased muscle fatigue during the RIF. This increase is concordant with previous research that reported an increased sensation of fatigue during RIF [26]. Indeed, decrements in physical function can lead to an increase in perceived exertion, an earlier onset of fatigue, and, thus, an increased risk of injury or illness [38].
In this study, psychometric markers, such as stress levels, DOMS, HI, TQR, were negatively affected at the fourth week in comparison with the beginning of RIF for both groups. These results could putatively be explained by the changes in the daily habits of players during Ramadan [35]. In fact, players tend to prepare for the period of fasting during Ramadan by rising earlier and eating a meal before sunrise [35]. Resultantly, players tend to be impacted by partial sleep deprivation, which can affect the higher cognitive centers of the central nervous system which negatively affect mental and athletic performances [35, 39, 40]. Furthermore, the reduction in mental activity has been posited as one of the main reasons for performance decrements [12, 26]. In addition, fatigue has been shown to reduce muscle glycogen depletion and/or alter neurotransmitter activity that could, in turn, negatively influence cognition and motor skill performance [41].
Limitations
Although we present a novel addition to the literature, our study has some limitations that warrant consideration. Firstly, the small sample size, which reduces our statistical power; however, this study merely presents preliminary work, and was not designed to be powered as a randomized controlled trial. Secondly, time-motion variables were not included (i.e., distance covered, sprint number, and run at high intensity), which would have provided a further level of fidelity to our study. Third, only a 3 vs. 3 SSG format was used; thus, changing duration, pitch size, recovery period, number of players, etc., may provide further information or yield differing responses. Finally, the period within the year when Ramadan occurred must be considered; indeed, future studies may have different results by investigating the month of Ramadan under different climatic circumstances.
Conclusions
Our results showed that SSGs training, at the end of RIF, negatively affected psychometric parameters of males and females, in particular in HI, which indicates a more negative state of well-being. Moreover, a significantly higher HR recorded in favor of female professional basketball players. Thus, it can be concluded that there are sex-mediated effects of training during RIF in professional basketball players, and this information should be considered by both researchers and practitioners when programing training during RIF.
Practical applications
-
Higher stress levels, fatigue, and DOMS, were recorded at the end of RIF, which may negatively affect technical aspects and physical performance in basketball.
-
Total quality of recovery decreased by the end of Ramadan which was accompanied by a decrease on sleep quality.
-
Provision of a sufficient recovery during the RIF is recommended to help avoid performance deterioration and overtraining.
Availability of data and materials
The datasets generated during and analyzed during the current study are not publicly available due to confidential information about the participants but are available from the corresponding author on reasonable request.
Abbreviations
- DOMS:
-
Delayed onset of muscle soreness
- TQR:
-
Total quality recovery
- RIF:
-
Ramadan intermitting fasting
- ANCOVA:
-
Analysis of covariance
- RPE:
-
Rating of perceived exertion
- HI:
-
Hooper index
- HR:
-
Heart rate
- Lac:
-
Lactate concentration
- BMI:
-
Body mass index
References
Conte D, Favero TG, Lupo C, Francioni FM, Capranica L, Tessitore A. Time-motion analysis of Italian elite women's basketball games: individual and team analyses. J Strength Cond Res. 2015;29(1):144–50. https://doi.org/10.1519/JSC.0000000000000633.
Marcelino PR, Aoki MS, Arruda A, Freitas CG, Mendez-Villanueva A, Moreira A. Does small sided-gamesʼ court area influence metabolic, perceptual, and physical performance parameters of young elite basketball players? Biol Sport. 2016;33:37–42.
Torres-Ronda L, Ric A, Llabres-Torres, I de Las Heras B, & Schelling, IDAX. Position-dependent cardiovascular response and time-motion analysis during training drills and friendly matches in elite male basketball players. J Strength Cond Res. 2016;30(1):60–70. https://doi.org/10.1519/JSC.0000000000001043.
Clemente FM, Sanches R, Moleiro CF, Gomes M, Lima R. Technical performance and perceived exertion variations between small-sided basketball games in Under-14 and Under-16 competitive levels. J Hum Kinetics. 2020;71(1):179–89. https://doi.org/10.2478/hukin-2019-0082.
McCormick BT, Hannon JC, Newton M, Shultz B, Miller N, Young W. Comparison of physical activity in small-sided basketball games versus full-sided games. Int J Sports Sci Coach. 2012;7(4):689–98. https://doi.org/10.1260/1747-9541.7.4.689.
Olthof SBH, Frencken WGP, Lemmink KAPM. The older, the wider: on-field tactical behavior of elite-standard youth soccer players in small-sided games. Hum Mov Sci. 2015;41:92–102. https://doi.org/10.1016/j.humov.2015.02.004.
Piñar MI, Cárdenas D, Alarcón F, Escobar R, Torre E. Participation of mini basketball players during small-sided competitions. Rev Psic Del Dep. 2009;18:445–9.
Sampaio J, Abrantes C, Leite N. Power, heart rate and perceived exertion responses to 3x3 and 4x4 basketball small-sided games. Rev Psic Del Dep. 2009;18:463–7.
Selmi O, Gonçalves B, Ouergui I, Sampaio J, Bouassida A. Influence of well-being variables and recovery state in physical enjoyment of professional soccer players during small-sided games. Res Sports Med. 2018;26(2):199–210. https://doi.org/10.1080/15438627.2018.1431540.
Sansone P, Tessitore A, Lukonaitiene I, Paulauskas H, Tschan H, Conte D. Technical-tactical profile, perceived exertion, mental demands and enjoyment of different tactical tasks and training regimes in basketball small-sided games. Biol Sport. 2020;37(1):15–23. https://doi.org/10.5114/biolsport.2020.89937.
Badin OO, Smith MR, Conte D, Coutts AJ. Mental fatigue: impairment of technical performance in small-sided soccer games. Int J Sports Physiol Perf. 2016;11(8):1100–5. https://doi.org/10.1123/ijspp.2015-0710.
Smith MR, Coutts AJ, Merlini M, Deprez D, Lenoir M, Marcora SM. Mental fatigue impairs soccer-specifec physical and technical performance. Med Sci Sports Exerc. 2016;48(2):267–76. https://doi.org/10.1249/MSS.0000000000000762.
Conte D, Favero TG, Niederhausen M, Capranica L, Tessitore A. Effect of different number of players and training regimes on physiological and technical demands of ball-drills in basketball. J Sports Sci. 2016;34(8):780–6. https://doi.org/10.1080/02640414.2015.1069384.
Coutinho D, Gonçalves B, Travassos B, Wong DP, Coutts AJ, Sampaio JE. Mental fatigue and spatial references impair soccer players’ physical and tactical performances. Front Psychol. 2017;8:1645. https://doi.org/10.3389/fpsyg.2017.01645.
Halouani J, Chtourou H, Gabbett T, Chaouachi A, Chamari K. Small-sided games in team sports training: a brief review. J Strength Cond Res. 2014;28(12):3594–618. https://doi.org/10.1519/JSC.0000000000000564.
Hooper SL, Mackinnon LT. Monitoring overtraining in athletes: recommendations. Sports Med. 1995;20(5):321–7. https://doi.org/10.2165/00007256-199520050-00003.
Freitas VH, Nakamura FY, Miloski B, Samulski D, Bara-Filho MG. Sensitivity of physiological and psychological markers to training load intensification in volleyball players. J Sports Sci Med. 2014;13(3):571–9.
Osiecki R, Rubio G, Coelho RL, et al. The total quality recovery scale (TQR) as a proxy for determining athletes’recovery state after a professional soccer match. J Exerc Physiol. 2015;18:27–32.
Brink MS, Nederhof E, Visscher C, Schmikli SL, Lemmink KA. Monitoring load, recovery, and performance in young elite soccer players. J Strength Cond Res. 2010;24(3):597–603. https://doi.org/10.1519/JSC.0b013e3181c4d38b.
Brini S, Marzouki H, Castagna C, Bouassida A. Effects of a four-week small-sided game and repeated Sprint ability training during and after Ramadan on aerobic and anaerobic capacities in senior basketball players. Ann Appl Sport Sci. 2018;6(3):7–13.
Brini S, Marzouki H, Ouerghi N, Ouergui I, Castagna C, Bouassida A. Effects of Ramadan observance combined with two training programs on plasma lipids and testosterone/cortisol ratio in male senior basketball players. Med Sport. 2019;72:47–58.
Brini S, Ouerghi N, Bouassida A. Small sided games vs repeated sprint effects on agility in fasting basketball players. Rev Bras Med Esporte. 2020;26(3):248–52. https://doi.org/10.1590/1517-869220202603213948.
Baklouti H, Rejeb N, Aloui A, Jaafar H, Ammar A, Chtourou H, et al. Short versus long small-sided game training during Ramadan in soccer players. Phys Therapy Sport. 2017;24:20–5. https://doi.org/10.1016/j.ptsp.2016.10.002.
Zdeněk R. The effects of sex and changes of game rules on the intensity of inner loads during small-sided games in four on four basketball. J Educ Health and Sport. 2016;6(13):169–73.
Singh R, Hwa OC, Roy J, Jin CW, Ismail SM, Lan MF, et al. Subjective perception of sports performance, training, sleep and dietary patterns of Malaysian junior Muslim athletes during Ramadan intermittent fasting. Asian J Sports Med. 2011;2(3):167–76. https://doi.org/10.5812/asjsm.34750.
Chtourou H, Hammouda O, Souissi H, Chamari K, Chaouachi A, Souissi N. The effect of Ramadan fasting on physical performances, mood state and perceived exertion in young footballers. Asian J of Sports Med. 2011;2(3):177–85.
Brini S, Ben Abderrahman A, Boullosa D, Hackney AC, Zagatto AM, Castagna C, et al. Effects of a 12-week change-of-direction sprints training program on selected physical and physiological parameters in professional basketball male players. Int J Environ Res Public Health. 2020 Nov 6;17(21):8214. https://doi.org/10.3390/ijerph17218214.
Klusemann MJ, Pyne DB, Foster C, Drinkwater EJ. Optimising technical skills and physical loading in small-sided basketball games. J Sports Sci. 2012;30(14):1463–71. https://doi.org/10.1080/02640414.2012.712714.
Foster C. Monitoring training in athletes with reference to overtraining syndrome. Med Sci Sports Exerc. 1998;30(7):1164–8. https://doi.org/10.1097/00005768-199807000-00023.
Léger L, And C Gadoury. Validity of the 20 m shuttle run test with 1 min stages to predict VO2max in adults. Can J Sports Sci 1988; 6: 93–101, The multistage 20 metre shuttle run test for aerobic fitness, 2, DOI: https://doi.org/10.1080/02640418808729800.
Hirvonen J, Rehunen S, Rusko H, Harkonen M. Breakdown of high-energy phosphate compounds and lactate accumulation during short supramaximal exercise. Eur J Appl Physiol Occup Physiol. 1978;56:253–9.
Vickers AJ, Altman DG. Statistics notes: Analysing controlled trials with baseline and follow up measurements. BMJ. 2001;323(7321):1123–4. https://doi.org/10.1136/bmj.323.7321.1123.
Cohen J. Eta-squared and partial eta-squared in fixed factor ANOVA designs. Educ Psychol Meas. 1937;33:107–12.
Coutts AJ, Reaburn P, Piva TJ, Rowsell GJ. Monitoring for overreaching in rugby league players. Eur J Appl Physiol. 2007;99(3):313–24. https://doi.org/10.1007/s00421-006-0345-z.
Vaquera A, Suárez-Iglesias D, Guiu X, Barroso R, Thomas G, Renfree A. Physiological responses to and athlete and coach perceptions of exertion during small-sided basketball games. J Streng Cond Res. 2018;32(10):2949–53. https://doi.org/10.1519/JSC.0000000000002012.
Al Suwaidi J, Bener A, Gehani AA, et al. Does the circadian pattern for acute cardiac events presentation vary with fasting? J Postgrad Med. 2006;52:30–4.
McArdle WD, Foglia GF, Patti AV. Telemetered cardiac response to selected running events. J Appl Physiol. 1981;23(4):566–70.
Leiper JB, Watson P, Evans G, Dvorak J. Intensity of a training session during Ramadan in fasting and non-fasting Tunisian youth football players. J Sports Sci. 2008;26:71–9.
Bonnet MH. Sleep, performance and mood after the energy-expenditure equivalent of 40 hours of sleep deprivation. Psycho physiol. 1980;17(1):56–63. https://doi.org/10.1111/j.1469-8986.1980.tb02460.x.
Souissi N, Sesboüé B, Gauthier A, Larue J, Davenne D. Effects of one night’s sleep deprivation on anaerobic performance the following day. Eur J Appl Physiol. 2003;89(3):359–66. https://doi.org/10.1007/s00421-003-0793-7.
Davis JM. Nutrition, neurotransmitters and central nervous system fatigue. Nut sport. 2000. p. 171–84. https://onlinelibrary.wiley.com/doi/pdf/10.1002/9780470693766.ch12.
Acknowledgments
The authors would like to acknowledge with considerable gratitude all those who volunteered to take part in this study.
Funding
The authors acknowledge the support of the Deutsche Forschungsgemeinschaft (DFG) and Open Access Publishing Fund of the University of Potsdam, Germany. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Conceptualization, S.B. and H.Z.; methodology, S.B., H.Z., U.G. and A.H.; software, A.A.; validation, U.G; C. C, A.H.; formal analysis, S.B. and S.Z; investigation, S.B.; data curation, S.B.; A. A and C.C., writing-original draft preparation, S.B. and A. H writing-review and editing, A.H. and C.C.; U.G. supervision, H.Z. and U.G.;. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Clinical Research Ethics Committee of the High Institute of Sports and Physical Education of Kef, University of Jendouba, Kef, Tunisia (approval No. 9/2018) and the protocol was conducted in accordance with the Declaration of Helsinki. All participants provided their written informed consent to participate in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that the research was conducted without any commercial or financial relationships, and declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Brini, S., Abderrahman, A.B., Clark, C.C.T. et al. Sex-specific effects of small-sided games in basketball on psychometric and physiological markers during Ramadan intermittent fasting: a pilot study. BMC Sports Sci Med Rehabil 13, 56 (2021). https://doi.org/10.1186/s13102-021-00285-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13102-021-00285-1