
Abstract
Background
The co-occurrence of cardiometabolic diseases (CMDs) is increasingly prevalent and has been associated with an additive risk of dementia in older adults, but the extent to which this risk can be offset by a healthy lifestyle is unknown. We aimed to examine the associations of cardiometabolic multimorbidity and lifestyle with incident dementia and related brain structural changes.
Methods
This prospective study extracted health and lifestyle data from 171 538 UK Biobank participants aged 60 years or older without dementia at baseline between 2006 and 2010 and followed up until July 2021, as well as brain structural data in a nested imaging subsample of 11 972 participants. Cardiometabolic multimorbidity was defined as the presence of two or more CMDs among type 2 diabetes, coronary heart disease, stroke, and hypertension. Lifestyle patterns were determined based on 7 modifiable lifestyle factors including smoking, alcohol consumption, physical activity, diet, sleep duration, sedentary behavior, and social contact.
Results
Over a median follow-up of 12.3 years, 4479 (2.6%) participants developed dementia. The presence of CMDs was dose-dependently associated with an increased risk of dementia. Compared with participants with no CMDs and a favourable lifestyle, those with ≥ 3 CMDs and an unfavourable lifestyle had a five times greater risk of developing dementia (HR 5.33, 95% CI 4.26–6.66). A significant interaction was found between CMD status and lifestyle (Pinteraction=0.001). The absolute difference in incidence rates of dementia per 1000 person years comparing favourable versus unfavourable lifestyle was − 0.65 (95% CI − 1.02 to − 0.27) among participants with no CMDs and − 5.64 (− 8.11 to − 3.17) among participants with ≥ 3 CMDs, corresponding to a HR of 0.71 (0.58–0.88) and 0.42 (0.28–0.63), respectively. In the imaging subsample, a favourable lifestyle was associated with larger total brain, grey matter, and hippocampus volumes across CMD status.
Conclusion
Our findings suggest that adherence to a healthy lifestyle might substantially attenuate dementia risk and adverse brain structural changes associated with cardiometabolic multimorbidity.
Similar content being viewed by others


Background
Type 2 diabetes, coronary heart disease (CHD), and stroke are well-established cardiometabolic risk factors for dementia [1,2,3,4]. With the ageing of the population, the prevalence of cardiometabolic multimorbidity, defined as two or more cardiometabolic diseases (CMDs), is rising rapidly in older adults [5]. Concurrent CMDs have been shown to interact with each other to increase the risk of negative outcomes [6]. Although relevant evidence about dementia is overall sparse, two recent studies have revealed dose-dependent associations between CMDs and dementia incidence or progression [7, 8], indicating that people with cardiometabolic multimorbidity are at high risk of developing dementia and concerted efforts to reduce the risk are imperative.
Because of limited value of pharmacological therapies currently used for treating dementia, directing the focus toward primary prevention strategies has become a high priority. Healthy lifestyle factors, including nonsmoking, moderate alcohol consumption, physical activity, and healthy diet, have been individually associated with a lower risk of dementia [9]. These lifestyle behaviours often cluster in people and may have synergistic effects on dementia risk [10, 11]. Additionally, mounting evidence has emphasised a role for emerging lifestyle factors, such as sleep duration, television viewing time, and social contact [12,13,14]. Since knowledge about lifestyle-related risk factors of dementia is improving, incorporating the emerging factors in overall lifestyle scores will provide more useful information for public health intervention.
Lifestyle modification is a fundamental component for management of CMDs. A recent study reported that engagement in leisure activities and a rich social network conferred a reduced risk of dementia among older adults with CMDs [15]. However, no previous studies have identified whether and the extent to which the increased dementia risk associated with cardiometabolic multimorbidity can be offset by a broad combination of healthy lifestyle factors. Meanwhile, CMDs have been linked to brain damage before the clinical symptoms of cognitive impairment and dementia [16, 17], but the impact of a healthy lifestyle on brain structural changes in patients with CMDs, particularly those with cardiometabolic multimorbidity, remains unclear. Understanding such features could help tailor future interventions for dementia prevention among the high-risk individuals. In this study, we used data from the UK Biobank cohort to examine how a healthy lifestyle, which incorporates conventional and emerging lifestyle factors, affects the associations of cardiometabolic multimorbidity with incident dementia and brain structural measures. We hypothesised that adherence to a healthy lifestyle may counteract the risk of dementia among people with cardiometabolic multimorbidity.
Methods
Study design and population
The UK Biobank is a population-based cohort that recruited more than 500 000 participants aged 40–70 years who attended one of 22 assessment centres across the UK between 2006 and 2010 [18]. Participants completed touch-screen and nurse-led questionnaires, underwent physical measurements, and provided biological samples. A subgroup of participants received brain imaging tests between 2014 and 2020. In this study, analyses were restricted to individuals aged at least 60 years at baseline who had lifestyle information available, because most sporadic dementia occurs in older adults. Participants with prevalent cognitive impairment or dementia at baseline or a history of encephalitis, meningitis, amyotrophic lateral sclerosis, multiple sclerosis, head injury, or central nervous system infection were excluded from analyses. Those with type 1 diabetes or missing data on glycated hemoglobin (HbA1c) were also excluded. Disease diagnoses were based on a combination of self-report and hospital inpatient records.
The UK Biobank study has ethical approval from the North West Multi-Centre Research Ethics Committee (reference 11/NW/0382). All participants provided written informed consent for the study.
Ascertainment of cardiometabolic diseases and multimorbidity
CMDs that included type 2 diabetes, CHD, stroke, and hypertension were ascertained at baseline using self-reported diagnoses and hospital inpatient records (UK Biobank codes are listed in Supplementary Table 1). The algorithms for identification of prevalent diabetes based on self-reported medical history and medications have been previously described [19]. Undiagnosed diabetes was defined as HbA1c ≥ 48.0 mmol/mol (6.5%), in accordance with the American Diabetes Association criteria [20]. Hypertension was defined as previous professional diagnosis, taking blood pressure-lowering medications, systolic blood pressure ≥ 140 mm Hg, or diastolic blood pressure ≥ 90 mm Hg. CMD status was identified for each participant by summing the number of CMDs (diabetes, CHD, stroke, and hypertension) and categorised as no CMDs, 1 CMD, 2 CMDs, or ≥ 3 CMDs.
Healthy lifestyle categories
We considered seven modifiable lifestyle behaviours known to be associated with dementia risk [9], including smoking, physical activity, alcohol consumption, diet, sleep duration, sedentary behaviour, and social contact, to generate a lifestyle score. All lifestyle data were derived from questionnaire responses at baseline. Details of the assessments of individual lifestyle factors can be found in Supplementary Table 2. Given that weight change is a common phenotype during CMD progression and is affected by medical treatment [21], body mass index (BMI) may not serve as a valid measure for weight management to be included in the lifestyle score.
We determined healthy and unhealthy categories for each lifestyle factor using national guidelines if available. Participants scored 1 point for each of healthy lifestyle factors: no current smoking, moderate alcohol consumption (up to 1 drink [14 g] per day for women and up to 2 drinks [28 g] per day for men) [22], regular physical activity (≥ 150 min per week of moderate activity or ≥ 75 min per week of vigorous activity) [23], a healthy diet pattern (adherence to at least 4 of the 7 endorsed dietary habits—consumption of an increased amount of fruits, vegetables, whole grains, fish, and a reduced amount of refined grains, processed and unprocessed meats) [24], adequate sleep duration (7–9 h/day), less sedentary behaviour (< 4 h per day of television viewing time) [25], frequent social contact (at least 2 of the 3 predefined characteristics—living with other people, regular friends or family visits, and engagement in social activities) [26]. The sum of these factors constituted a final lifestyle score ranging from 0 to 7, with higher scores indicating a healthier lifestyle. This lifestyle score has been validated elsewhere [27]. We then categorised the lifestyle patterns as favourable (score 6–7), intermediate (score 4–5), or unfavourable (score 0–3) based on distribution of the lifestyle score. In sensitivity analysis, we constructed a weighted lifestyle score considering the relative risk for each lifestyle factor estimated from the full adjusted model that included all seven lifestyle factors: weighted lifestyle score = (β1× factor1 + β2 × factor2 +…+ β7 × factor7) × (7/sum of the β coefficients).
Dementia diagnosis
Incident dementia was ascertained through linkage to hospital admission records and death registry data. Date and cause of hospital admissions were obtained from the Health Episode Statistics for England and Wales and the Scottish Morbidity Records for Scotland. Information on death was provided by the National Health Service Digital for England and Wales and the National Health Service Central Register for Scotland. Additional cases were retrieved from primary care records. Dementia diagnoses were documented using the International Classification of Diseases (ICD-9 and ICD-10) codes for Alzheimer’s disease, vascular dementia, and other dementia classifications (Supplementary Table 1).
Brain imaging
Brain MRI data including high-resolution, T1-weighted, three-dimensional MPRAGE and T2-weighted FLAIR images were acquired on a standard Siemens Skyra 3T scanner with a 32-channel receive head coil. The imaging data were processed and released as imaging-derived phenotypes. Full details of the imaging protocol and processing pipeline have been previously described [28]. We used imaging summary statistics of volumes of total brain, grey matter, white matter hyperintensity (WMH), and hippocampus. Brain tissue volumes were normalized for head size based on the external surface of the skull [28]. Median absolute deviation was used to exclude extreme outliers [29].
Covariates
Socioeconomic status was derived from the Townsend deprivation index (in quintiles), a composite measure combining information on car ownership, housing, owner occupation, and employment [30]. Ethnicity was self-reported and categorised into white, Asian, black, or other ethnic group. Educational attainment was self-reported and coded as an ordinal variable (college or university degree, A levels/AS levels, O levels/GCSEs, CSEs or equivalent, NVQ/HND/HNC or equivalent, or none of these). Depression was ascertained during a nurse-led interview at baseline. Apolipoprotein E (APOE) haplotypes were extracted from the genetic data and categorised as APOE ε4 carriers (any ε4 allele) and noncarriers. Cognitive function tests (e.g. reaction time test of symbol matching and visual pairs memory test) were completed through a touchscreen tool.
Statistical analysis
Descriptive characteristics of the study population by CMD status were presented as percentage for categorical variables and means with SDs for continuous variables. Follow-up time was calculated from baseline to the date of dementia diagnosis, death, or the censoring date (30 July 2021), whichever occurred first. Cox proportional hazards models with age the time scale were used to estimate hazard ratios (HRs) of incident dementia associated with CMD status (no CMDs, 1 CMD, 2 CMDs, or ≥ 3 CMDs) and lifestyle category (favourable, intermediate, or unfavourable). Apart from overall CMD status, we calculated HRs for mutually exclusive groups according to specific CMDs, compared with the no CMDs group. To test our main hypothesis, we examined the association of the combination of CMD status and lifestyle category (12 categories with no CMDs and favourable lifestyle as reference) with incident dementia. Statistical interaction between CMD status and lifestyle category was tested by fitting an interaction term in the models. All analyses were adjusted for age, sex, ethnicity, education, socioeconomic deprivation, depression, APOE ε4 carrier status, and cognitive performance at baseline. When investigating the individual association with CMD status, models were additionally adjusted for lifestyle category, and vice versa. Missing covariate data were included as a separate category for categorical variables (all missing covariates < 1%). The proportional hazards assumption was checked using Schoenfeld residuals and satisfied. We also examined the association between lifestyle category and incident dementia within each CMD status. Absolute rate differences in dementia incidence across lifestyle categories were estimated, with participants in the unfavourable lifestyle category as the reference group.
Analyses of CMD status and lifestyle category alone or in combination and volumes of total brain, grey matter, WMH, and hippocampus were conducted using linear regression models with each brain measure as the outcome. Due to the positively skewed distribution, WMH volume was log-transformed before modeling. For each brain measure, interaction between CMD status and lifestyle category was tested using Bonferroni correction for multiple testing.
In supplementary analyses, we included additional covariates of total cholesterol, BMI, and HbA1c to examine whether these upstream cardiometabolic risk markers could partly explain the associations between cardiometabolic multimorbidity, lifestyle, and dementia risk. We also evaluated the possible influence of disease treatments by further adjusting for medications for high blood pressure, high cholesterol, and diabetes. Moreover, we used proportional subdistribution hazards regression models to account for the competing risk of death. Further sensitivity analyses were conducted by using imputed data for missing values of lifestyle factors and covariates, redefining low-risk alcohol consumption as no heavy drinking, and excluding dementia cases within the first 3 or 5 years of follow-up. Given the potential differences between participants with and without MRI data, analyses of associations with brain volumes were weighted by the inverse of their probability of being a complete data case. All statistical analyses were performed with SAS, version 9.4 (SAS Institute Inc). A two-sided P value < 0.05 was considered statistically significant.
Results
Population characteristics
Of the 502 505 participants recruited to UK Biobank, 217 489 (43.2%) were aged 60 years or older. After excluding participants with prevalent dementia (n = 236) or type 1 diabetes (n = 1044) at baseline, those with missing data on lifestyle metrics (n = 32 320) or HbA1c (n = 10 470), or those fulfilled any other exclusion criteria (n = 1881), 171 538 participants were included in the analytic sample (Supplementary Fig. 1). The mean age of participants was 64.1 (SD 2.8) years and 88 389 (51.5%) were women. At baseline assessment, 46 368 (27.0%) participants were free of CMDs, and 100 640 (58.7%), 20 918 (12.2%), 3612 (2.1%) had 1, 2, and ≥ 3 CMDs, respectively. Characteristics of the participants by number of CMDs are presented in Table 1. On the basis of lifestyle score comprising seven behaviours, 25 472 (14.9%) participants were classified into the unfavourable lifestyle category, 90 102 (52.5%) into the intermediate lifestyle category, and 55 964 (32.6%) into the favourable lifestyle category. Participants with one or more CMDs had a lower proportion of favourable lifestyle than those with no CMDs.
Independent association of CMDs and lifestyle with dementia risk
Over a median follow-up of 12.3 years (IQR 11.5–13.0 years), 4479 (2.6%) incident cases of all-cause dementia were documented. Type 2 diabetes, CHD, and stroke were individually associated with dementia risk. The presence of concurrent CMDs was dose-dependently associated with an increased risk of dementia, and this association did not change after adjusting for lifestyle factors. Compared with the reference group with no CMDs, the HRs for dementia were 1.07 (95% CI 0.99–1.15), 1.74 (1.58–1.91), and 2.83 (2.46–3.25) for participants with 1, 2, and ≥ 3 CMDs, respectively (Table 2). In terms of lifestyle factors, each one was related to dementia risk with the exception of diet (Supplementary Table 3). There was a monotonic association between the number of healthy lifestyle factors and lower dementia risk (HR 0.89, 95% CI 0.87–0.91 per additional factor) (Supplementary Table 4). In multivariable models that included CMD status, participants with a favourable lifestyle had a HR for dementia of 0.67 (95% CI 0.61–0.73) compared with those who had an unfavourable lifestyle (Table 2).
Association of CMDs and lifestyle with dementia risk
When CMD status and lifestyle profile were combined, the risk of incident dementia increased with an increasing number of CMDs and an increasingly unhealthy lifestyle (Fig. 1). Compared with participants with no CMDs and a favourable lifestyle, those with ≥ 3 CMDs and an unfavourable lifestyle had a 5-fold greater risk of dementia (HR 5.33, 95% CI 4.26–6.66). However, the risk was markedly reduced among participants with ≥ 3 CMDs and a favourable lifestyle (HR 2.32, 1.63–3.33). A significant interaction was observed between CMD status and lifestyle category on dementia (Pinteraction = 0.001). Analyses of the dementia subtypes showed more pronounced results for vascular dementia compared to Alzheimer’s disease (Supplementary Table 5). The association of CMDs and lifestyle with dementia remained consistent in serial sensitivity analyses when using a weighted lifestyle score, redefining low-risk alcohol consumption as no heavy drinking, or excluding dementia cases during the first 3 or 5 years of follow-up (Supplementary Tables 6–8). Considering the competing risk of death and imputing missing data for exposure and covariates yielded similar results (Supplementary Tables 9–10). The HRs did not appreciably change after adjustment for upstream cardiometabolic risk markers and was slightly attenuated after adjustment for medications on metabolic disorders (Supplementary Table 11). Stratified analyses showed that the joint association of CMD status and lifestyle with dementia risk was stronger in APOE ε4 noncarriers than in APOE ε4 carriers (Pinteraction <0.001) (Supplementary Table 12).

Risk of incident dementia according to cardiometabolic disease status and lifestyle category
Cox regression models with age as time scale were adjusted for sex, ethnicity, education, socioeconomic deprivation, depression, APOE ε4 carrier status, and cognitive performance at baseline. The reference group was participants with no CMDs and a favourable lifestyle. Test for interaction between CMD status and lifestyle category was significant (Pinteraction=0.001). CMD: cardiometabolic disease; HR: hazard ratio
Within each CMD status, a favourable lifestyle was associated with a lower risk of developing dementia (Table 3). The HR for dementia comparing favourable lifestyle versus unfavourable lifestyle was 0.71 (95% CI 0.58–0.88) among participants with no CMDs and 0.42 (95% CI 0.28–0.63) among participants with ≥ 3 CMDs, with an absolute difference in incident dementia rates of − 0.65 (95% CI − 1.02 to − 0.27) and − 5.64 (95% CI − 8.11 to − 3.17) per 1000 person-years, respectively. A similar pattern was found for separate conventional and emerging lifestyle score although the HR estimates were less remarkable than the extended score (Supplementary Table 13).
Association of CMDs and lifestyle with brain structural measures
In an imaging subsample of 11 978 participants, cardiometabolic multimorbidity and unfavourable lifestyle were each associated with smaller volumes of total brain, grey matter, and hippocampus and higher WMH load (Supplementary Table 14). When considered jointly, compared with participants who had no CMDs and a favourable lifestyle, participants with ≥ 3 CMDs and an unfavourable lifestyle had 44.6 cm3 lower total brain volume (P = 0.028), 35.0 cm3 lower grey matter volume (P = 0.004), and 506.9 mm3 lower hippocampal volume (P = 0.059); however, the volume reductions were largely mitigated in those with a favourable lifestyle (Fig. 2). We identified no significant interaction between CMD status and lifestyle category on brain structural measures. The results remained similar when the inverse probability weighting method was applied (Supplementary Table 15).

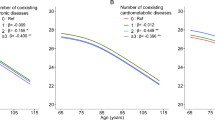
Associations of cardiometabolic disease status and lifestyle category with structural brain volumes
Coefficients for differences in total brain volume (A), grey matter volume (B), WHM volume (C), and hippocampal volume (D) were estimated using linear regression models and adjusted for age, sex, ethnicity, education, socioeconomic deprivation, depression, APOE ε4 carrier status, and cognitive performance at baseline. The reference group was participants with no CMDs and a favourable lifestyle. WMH was log-transformed in the analysis due to its skewed distribution. Interaction between CMD status and lifestyle category: Pinteraction=0.26 for total brain volume, Pinteraction=0.23 for grey matter volume, Pinteraction=0.63 for WMH volume, Pinteraction=0.41 for hippocampal volume. CMD: cardiometabolic disease; WMH: white matter hyperintensity
Discussion
This prospective study provided quantitative data about the interplay between CMD status and lifestyle factors for dementia incidence. Cardiometabolic multimorbidity and overall lifestyle defined by seven lifestyle factors were independently associated with dementia risk. Within any CMD status, a favourable lifestyle was associated with a significantly lower risk of dementia. This association was stronger in participants with cardiometabolic multimorbidity than in those with no or single CMD. The results were corroborated in analyses using brain MRI data for a subcohort. A favourable lifestyle was associated with higher brain volumes, irrespective of CMD status.
Type 2 diabetes, CHD, and stroke are well-recognised risk factors for dementia, with each being associated with up to a two times increased risk of developing dementia [1,2,3]. Despite the fact that cardiometabolic multimorbidity is highly prevalent in people living with dementia [9], few studies have examined the association between multiple cardiometabolic conditions and dementia, and most were limited by small sample size. In the cohort of 2648 older adults from the Swedish National Study on Aging and Care-Kungsholmen (SNAC-K), type 2 diabetes, CHD, and stroke in combination was associated with a HR of 4.76 (95% CI 2.04–11.1) for dementia [15]. A subsequent analysis based on the same cohort reported that individuals with cardiometabolic multimorbidity had nearly twice the risk of cognitive impairment and its progression to dementia compared with those who were CMD-free [7]. Recently, a large study used data from 203 038 UK Biobank participants of European ancestry to investigate the association of stroke, myocardial infarction, and diabetes with dementia risk, and has shown an increase in HRs from 1.94 (95% CI 1.80–2.08) for one CMD to 5.55 (3.39–9.08) for three CMDs [8]. However, type 1 diabetes was not distinguished in this study and undiagnosed diabetes was not considered. In the current study that examined stroke, CHD, hypertension and type 2 diabetes that included both diagnosed and undiagnosed cases, participants with more CMDs had an increasingly higher risk of dementia after accounting for APOE ε4 allele and lifestyle factors; the highest HR (5.61) was observed for participants with four CMDs, suggesting a monotonic, additive relationship between increasing number of CMDs and dementia risk. This finding emphasises the importance of prevention of comorbid CMDs and aggressive intervention actions among patients who already have cardiometabolic multimorbidity to reduce the burden of dementia.
There is considerable evidence that healthy lifestyle factors such as no smoking, moderate alcohol consumption, regular physical exercise, and healthy diet could individually contribute to a lower risk of dementia [9]. Combination of lifestyle factors may interact synergistically and result in stronger associations with dementia risk [10, 11]. However, previous studies have mostly focused on the general population, little is known about the impact of a wide range of lifestyle factors on dementia incidence in people with CMDs. Results from the SNAC-K study showed a reduced risk of dementia associated with high levels of leisure activities and a rich social network in older adults with CMDs [15]. In the present study, we created a lifestyle score incorporating traditional (smoking, alcohol consumption, physical activity, and diet) and emerging lifestyle factors including sleep duration, sedentary behaviour, and social contact. Compared with participants with no CMDs and a favourable lifestyle, we found a five times increased risk of dementia in participants with ≥ 3 CMDs and an unfavourable lifestyle, but the risk was lowered by approximately 68% in those with a favourable lifestyle. Our study adds to the existing knowledge by demonstrating that the increased risk of dementia due to cardiometabolic multimorbidity might be offset by adherence to a healthy lifestyle.
Although favourable lifestyle was associated with a decreased risk of dementia within each CMD status, the risk reductions were more prominent in individuals with cardiometabolic multimorbidity than in those with no CMDs or only one CMD. The results imply that individuals with cardiometabolic multimorbidity might benefit more than others from adopting a healthy lifestyle. Several trials have also shown benefits of multidomain lifestyle interventions on improving cognitive function in older people with an elevated risk of dementia [31,32,33]. Therefore, from a public health perspective, lifestyle modification could be a feasible and effective prevention strategy that is likely to have a significant impact on dementia risk reduction in people with CMDs, particularly those with cardiometabolic multimorbidity.
Total and regional brain volumes are usually recognised as reliable predictors of dementia. For example, total hippocampal volume loss is associated with accelerated memory decline that predicts Alzheimer’s disease and grey matter measures could be used to track Alzheimer’s disease progression [34, 35], while higher WMH load is a major contributor to vascular cognitive impairment [36]. Consistent with previous studies reporting that CMDs were associated with smaller volumes of total brain, grey matter, and hippocampal and higher WMH load [16, 17], our findings showed graded associations between the number of CMDs and widespread negative brain changes. Compared with participants with no CMDs and a favourable lifestyle, the reductions in brain volumes were most significant among individuals with cardiometabolic multimorbidity and an unfavourable lifestyle but were largely attenuated among those who had a favourable lifestyle, suggesting that adherence to a healthy lifestyle might mitigate the deleterious impact of comorbid CMDs on structural brain health.
The mechanisms underpinning the putative protective effect of healthy lifestyle on dementia are not fully understood. Several hypotheses have been proposed involving inhibition of oxidative stress and inflammation, increase of cerebral blood flow, and reduction of amyloid aggregation and neuritic plaques [37], which highlight the role of healthy lifestyle in improving vascular and neurodegenerative pathologies, while cardiometabolic multimorbidity has been shown to cause global cerebrovascular and neurodegenerative processes that contribute to cognitive impairment and dementia [8, 38]. Furthermore, a healthy lifestyle may help patients with CMDs to better cope with medical resources, health behaviours (e.g. adhering to disease treatment, screening for complications), or psychosocial factors [37, 39]. All these aspects presumably favor brain integrity and function, thereby reducing dementia risk.
To our knowledge, this study is the first to examine the association of combined cardiometabolic multimorbidity and lifestyle with dementia incidence. Strengths of this study include use of a large, longitudinal cohort with a long follow up, utilization of comprehensive information to determine an extended lifestyle score combining conventional and emerging factors, and inclusion of data on brain imaging. Some limitations should be discussed. First, lifestyle behaviours were self-reported and misclassification of exposure was inevitable. However, such misclassification errors most likely lead to biased findings toward the null and underestimated the strength of the observed association between lifestyle and dementia risk. Besides, lifestyle metrics were derived from baseline data, and possible changes over time could not be accounted for. Second, UK Biobank participants are more likely to be from less deprived areas and have fewer health conditions such as cardiovascular disease than the general population [40]. Consequently, the effects of cardiometabolic risk and lifestyle could potentially be larger in more representative cohorts due to this selection bias. Third, although the large sample facilitates the investigation of CMD status and lifestyle in combination, certain study groups have low numbers, which might lead to a potential bias. Fourth, the subgroup of individuals with imaging data was generally a little younger, more educated, and less deprived. Therefore, the findings with brain volumes might not be generalised to the whole UK population. However, analyses after weighting by the inverse of probability of attending imaging test yielded similar results. Fifth, because of the observational nature of this study, reverse causality is still possible, even though the results were similar after excluding events occurring in the first 3 or 5 years of follow-up. Given the long preclinical phase before any evident symptoms of dementia, participants who developed dementia might be already in the preclinical phase of the disease or experience brain structural changes. Further prospective studies with a longer follow-up period are essential to validate our findings. Finally, although we adjusted for various potential confounders, residual confounding from unknown or unmeasured factors could not be ruled out.
Conclusion
Our study indicated that cardiometabolic multimorbidity was associated with an increased risk of dementia and reduced brain volumes, while adherence to a healthy lifestyle might attenuate the dementia risk and adverse brain structural changes associated with cardiometabolic multimorbidity. These findings provide strong evidence supporting both clinical guidance and public health initiatives to promote an overall healthy lifestyle to prevent or delay the onset of dementia in people with cardiometabolic multimorbidity.
Data Availability
The data used in this current study are available from the UK Biobank data resources. Permissions are required in order to gain access to the UK Biobank data resources, subject to successful registration and application process. Further information can be found on the UK Biobank website (https://www.ukbiobank.ac.uk/).
Abbreviations
- APOE:
-
apolipoprotein E
- BMI:
-
body mass index
- CHD:
-
coronary heart disease
- CI:
-
confidence interval
- CMD:
-
cardiometabolic disease
- ICD:
-
International Classification of Diseases
- HbA1c:
-
glycated hemoglobin
- HR:
-
hazard ratio
- WMH:
-
white matter hyperintensity
References
Barbiellini Amidei C, Fayosse A, Dumurgier J, et al. Association between age at Diabetes onset and subsequent risk of Dementia. JAMA. 2021;325:1640–9.
Wolters FJ, Segufa RA, Darweesh SKL, et al. Coronary Heart Disease, Heart Failure, and the risk of Dementia: a systematic review and meta-analysis. Alzheimers Dement. 2018;14:1493–504.
Kuźma E, Lourida I, Moore SF, Levine DA, Ukoumunne OC, Llewellyn DJ. Stroke and Dementia risk: a systematic review and meta-analysis. Alzheimers Dement. 2018;14:1416–26.
Cooper C, Sommerlad A, Lyketsos CG, Livingston G. Modifiable predictors of Dementia in mild cognitive impairment: a systematic review and meta-analysis. Am J Psychiatry. 2015;172:323–34.
Glynn LG. Multimorbidity: another key issue for cardiovascular medicine. Lancet. 2009;374:1421–2.
Beard JR, Officer A, de Carvalho IA, et al. The World report on ageing and health: a policy framework for healthy ageing. Lancet. 2016;387:2145–54.
Dove A, Marseglia A, Shang Y, et al. Cardiometabolic multimorbidity accelerates cognitive decline and Dementia progression. Alzheimers Dement. 2022. https://doi.org/10.1002/alz.12708.
Tai XY, Veldsman M, Lyall DM, et al. Cardiometabolic multimorbidity, genetic risk, and Dementia: a prospective cohort study. Lancet Healthy Longev. 2022;3:e428–36.
Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396:413–46.
Lourida I, Hannon E, Littlejohns TJ, et al. Association of lifestyle and genetic risk with incidence of Dementia. JAMA. 2019;322:430–7.
Dhana K, Evans DA, Rajan KB, Bennett DA, Morris MC. Healthy lifestyle and the risk of Alzheimer Dementia: findings from 2 longitudinal studies. Neurology. 2020;95:e374–83.
Lutsey PL, Misialek JR, Mosley TH, et al. Sleep characteristics and risk of Dementia and Alzheimer’s Disease: the Atherosclerosis risk in communities study. Alzheimers Dement. 2018;14:157–66.
Hoang TD, Reis J, Zhu N, et al. Effect of early adult patterns of physical activity and television viewing on midlife cognitive function. JAMA Psychiatry. 2016;73:73–9.
Sommerlad A, Sabia S, Singh-Manoux A, Lewis G, Livingston G. Association of social contact with Dementia and cognition: 28-year follow-up of the Whitehall II cohort study. PLoS Med. 2019;16:e1002862.
Wang Z, Marseglia A, Shang Y, Dintica C, Patrone C, Xu W. Leisure activity and social integration mitigate the risk of Dementia related to cardiometabolic Diseases: a population-based longitudinal study. Alzheimers Dement. 2020;16:316–25.
Cox SR, Lyall DM, Ritchie SJ, et al. Associations between vascular risk factors and brain MRI indices in UK Biobank. Eur Heart J. 2019;40:2290–300.
Shang X, Zhang X, Huang Y, et al. Association of a wide range of individual chronic Diseases and their multimorbidity with brain volumes in the UK Biobank: a cross-sectional study. EClinicalMedicine. 2022;47:101413.
Sudlow C, Gallacher J, Allen N, et al. UK biobank: an open access resource for identifying the causes of a wide range of complex Diseases of middle and old age. PLoS Med. 2015;12:e1001779.
Eastwood SV, Mathur R, Atkinson M, et al. Algorithms for the capture and adjudication of prevalent and incident Diabetes in UK Biobank. PLoS ONE. 2016;11:e0162388.
American Diabetes Association. 2. Classification and diagnosis of Diabetes: standards of Medical Care in Diabetes—2020. Diabetes Care. 2020;43:14–S31.
Tobias DK, Pan A, Jackson CL, et al. Body-mass index and mortality among adults with incident type 2 Diabetes. N Engl J Med. 2014;370:233–44.
Zhang Y, Chen C, Pan X, et al. Associations of healthy lifestyle and socioeconomic status with mortality and incident Cardiovascular Disease: two prospective cohort studies. BMJ. 2021;373:n604.
Lloyd-Jones DM, Hong Y, Labarthe D, American Heart Association Strategic Planning Task Force and Statistics Committee, et al. Defining and setting national goals for cardiovascular health promotion and Disease reduction: the American Heart Association’s strategic impact goal through 2020 and beyond. Circulation. 2010;121:586–613.
Mozaffarian D. Dietary and policy priorities for Cardiovascular Disease, Diabetes, and obesity: a comprehensive review. Circulation. 2016;133:187–225.
Foster HME, Celis-Morales CA, Nicholl BI, et al. The effect of socioeconomic deprivation on the association between an extended measurement of unhealthy lifestyle factors and health outcomes: a prospective analysis of the UK Biobank cohort. Lancet Public Health. 2018;3:e576–85.
Smith RW, Barnes I, Green J, Reeves GK, Beral V, Floud S. Social isolation and risk of Heart Disease and Stroke: analysis of two large UK prospective studies. Lancet Public Health. 2021;6:e232–9.
Han H, Cao Y, Feng C, et al. Association of a healthy lifestyle with all-cause and cause-specific mortality among individuals with type 2 Diabetes: a prospective study in UK Biobank. Diabetes Care. 2022;45:319–29.
Alfaro-Almagro F, Jenkinson M, Bangerter NK, et al. Image processing and quality control for the first 10 000 brain imaging datasets from UK Biobank. NeuroImage. 2018;166:400–24.
Leys C, Ley C, Klein O, et al. Detecting outliers: do not use standard deviation around the mean, use absolute deviation around the median. J Exp Soc Psychol. 2013;49:764–6.
Townsend P, Deprivation. J Soc Policy. 1987;16:125–46.
Ngandu T, Lehtisalo J, Solomon A, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomized controlled trial. Lancet. 2015;385:2255–63.
Andrieu S, Guyonnet S, Coley N, et al. Effect of long-term omega 3 polyunsaturated fatty acid supplementation with or without multidomain intervention on cognitive function in elderly adults with memory complaints (MAPT): a randomised, placebo-controlled trial. Lancet Neurol. 2017;16:377–89.
van Moll EP, Richard E, Eurelings LS, et al. Effectiveness of a 6-year multidomain vascular care intervention to prevent Dementia (preDIVA): a cluster-randomised controlled trial. Lancet. 2016;388:797–805.
Lombardi G, Crescioli G, Cavedo E, et al. Structural magnetic resonance imaging for the early diagnosis of Dementia due to Alzheimer’s Disease in people with mild cognitive impairment. Cochrane Database Syst Rev. 2020;3:CD009628.
Dicks E, Vermunt L, van der Flier WM, Barkhof F, Scheltens P, Tijms BM. Grey Matter network trajectories across the Alzheimer’s Disease continuum and relation to cognition. Brain Commun. 2020;2:fcaa177.
Debette S, Schilling S, Duperron MG, Larsson SC, Markus HS. Clinical significance of magnetic resonance imaging markers of vascular brain injury: a systematic review and meta-analysis. JAMA Neurol. 2019;76:81–94.
Kivipelto M, Mangialasche F, Ngandu T. Lifestyle interventions to prevent cognitive impairment, Dementia and Alzheimer Disease. Nat Rev Neurol. 2018;14:653–66.
Arvanitakis Z, Capuano AW, Leurgans SE, Bennett DA, Schneider JA. Relation of cerebral vessel Disease to Alzheimer’s Disease Dementia and cognitive function in elderly people: a cross-sectional study. Lancet Neurol. 2016;15:934–43.
Santos T, Lovell J, Shiell K, Johnson M, Ibrahim JE. The impact of cognitive impairment in Dementia on self-care domains in Diabetes: a systematic search and narrative review. Diabetes Metab Res Rev. 2018;34:e3013.
Fry A, Littlejohns TJ, Sudlow C, et al. Comparison of sociodemographic and health-related characteristics of UK Biobank participants with those of the general population. Am J Epidemiol. 2017;186:1026–34.
Acknowledgements
The authors thank participants and staff in the UK Biobank for their dedication and contribution to the research.
Funding
This work was funded by the Scientific Research Innovation Fund Project of Wuhan Wuchang Hospital (No. WCYY2022Y03), the Fundamental Research Funds for the Central Universities (No. 2042023kf0040), and Subject Fund of the Central Hospital of Wuhan (No. 2021XK057).
Author information
Authors and Affiliations
Contributions
NH, SX, and HD conceived and designed the study. NH and FT performed the statistical analyses. SX and NH wrote the first draft of the manuscript. SX and HD guaranteed this work and take responsibility for the integrity of the data. All authors contributed to the interpretation of the results and critical revision of the manuscript for important intellectual content and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The UK Biobank has full ethical approval from the North West Multi-Center Research Ethics Committee. All the UK Biobank participants gave written informed consent before data collection.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xiong, S., Hou, N., Tang, F. et al. Association of cardiometabolic multimorbidity and adherence to a healthy lifestyle with incident dementia: a large prospective cohort study. Diabetol Metab Syndr 15, 208 (2023). https://doi.org/10.1186/s13098-023-01186-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-023-01186-8