
Abstract
Background/Objective
Metabolic syndrome (MS) is related to lung dysfunction. However, its impact according to insulin resistance (IR) remains unknown. Therefore, we evaluated whether the relation of MS with lung dysfunction differs by IR.
Subject/Methods
This cross-sectional study included 114,143 Korean adults (mean age, 39.6 years) with health examinations who were divided into three groups: metabolically healthy (MH), MS without IR, and MS with IR. MS was defined as presence of any MS component, including IR estimated by HOMA-IR ≥ 2.5. Adjusted odds ratios (aORs) and 95% confidence intervals (CIs) for lung dysfunction were obtained in MS, MS without IR, and MS with IR groups compared with the MH (reference) group.
Results
The prevalence of MS was 50.7%. The percent predicted forced expiratory volume in 1 s (FEV1%) and forced vital capacity (FVC%) showed statistically significant differences between MS with IR and MH and between MS with IR and MS without IR (all P < 0.001). However, those measures did not vary between MH and MS without IR (P = 1.000 and P = 0.711, respectively). Compared to MH, MS was not at risk for FEV1% < 80% (1.103 (0.993–1.224), P = 0.067) or FVC% < 80% (1.011 (0.901–1.136), P = 0.849). However, MS with IR was clearly associated with FEV1% < 80% (1.374 (1.205–1.566) and FVC% < 80% (1.428 (1.237–1.647) (all p < 0.001), though there was no evident association for MS without IR (FEV1%: 1.078 (0.975–1.192, P = 0.142) and FVC%: 1.000 (0.896–1.116, p = 0.998)).
Conclusion
The association of MS with lung function can be affected by IR. However, longitudinal follow-up studies are required to validate our findings.
Similar content being viewed by others


¶ Jonghoo Lee, Hye Kyeong ParkThese authors contributed equally to this work.
Introduction
Lung dysfunction is associated with frailty, breathlessness, and multimorbidity, including death from all causes and cardiovascular diseases [1,2,3]. As lung dysfunction can occur prior to overt disease manifestation [4], early identification of modifiable risk factors for lung dysfunction is meaningful to reduce various diseases and their complications. Lung function is adversely affected by metabolic syndrome (MS) [5, 6], which comprises modifiable cardio-metabolic abnormalities, including abdominal obesity, hyperglycemia, hypertension, dyslipidemia, and/or insulin resistance (IR) [7, 8]. Furthermore, the extent to which MS affects lung function depends on the numbers [9,10,11,12,13,14,15] and components [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26] that are criteria for MS. Therefore, the role of MS in lung function is an area of active scrutiny, considering the worldwide high prevalence and modifiable precondition of MS-associated major critical health problems [5].
However, there have been variable results on the association between MS and lung function due to multiple concurrent definitions of MS, as suggested by a previous study [27]. IR critically mediates the link between lung dysfunction and MS [5, 22, 24, 28]. However, the label of MS per se does not provide a sensitive approach to identifying IR [29]. Thus, omission of IR as a criterion for MS could increase uncertainty as to MS-related lung effects. Nevertheless, among MS components, IR has not been fully considered in any previous studies. Therefore, we investigated spirometric values in subjects of different metabolic health and IR status to investigate the impact of IR on MS-related lung effects in a large asymptomatic population.
Materials and methods
Study design and population
This cross-sectional study was a part of the Kangbuk Samsung Health Study, which involved Koreans who underwent a comprehensive health examination at the Total Healthcare Center of Kangbuk Samsung Hospital in Seoul and Suwon, Republic of Korea, since January 1, 2002. Most of the examinees were employees and family members of various companies or local governmental organizations. In Republic of Korea, annual or biennial employee health screenings are required by the Industrial Safety and Health Law and are free of charge.
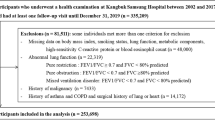
Figure 1 shows the flow chart for inclusion and exclusion of subjects in analyses. This study began with data from 214,551 individuals with health examinations in 2019. From these subjects, inclusion criteria were participants aged 18 years or older with recorded spirometry and metabolic data used to ascertain metabolic health (N = 212,333). Among this cohort, we excluded subjects with missing data for medical history and smoking habits or alcohol consumption (n = 17,759). We additionally excluded participants with a self-reported history and/or those patients currently receiving medication for malignancy (n = 5,698), chronic lung disease or abnormal chest radiograph findings ( n = 28,685), cardiovascular or cerebrovascular disease (n = 3,210), chronic liver disease including positive hepatitis B surface antigen and anti-hepatitis C virus antibody (n = 24,501), chronic renal disease (n = 645), hormonal and musculoskeletal diseases including osteoporosis and thyroid or parathyroid diseases (n = 17,493), and current steroid use (n = 199). However, detailed comorbidities were unavailable (not specified) because the medical history questionnaire only required yes/no responses. As some individuals had more than one exclusion criterion,

Flow diagram of study participants
BA = bronchial asthma; COPD = chronic obstructive pulmonary disease; HBsAg = hepatitis B virus surface antigen; HCV-Ab = hepatitis C virus antibody
114,143 participants were ultimately included in the analysis (Fig. 1).
The study was approved by the Institutional Review Board of Kangbuk Samsung Hospital (KBSMC 2022-03-055), which waived the requirement for informed consent due to the use of de-identified data for analysis purposes. The study protocol conformed to ethical guidelines of the 1975 Declaration of Helsinki and followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Data collection, anthropometric measurements, and laboratory tests
The comprehensive health-screening program assessed demographic, anthropometric, and laboratory data. Standardized self-administered questionnaires were used to ascertain information on demographic characteristics, medical history, medication use, smoking and drinking habits, exercise frequency, and education level. However, detailed comorbidities were unavailable because the medical history questionnaire only required yes/no responses.
Smoking status was classified as nonsmoker, ex-smoker, or current smoker. Alcohol consumption was categorized as none, non-heavy (≤ 20 g/day), or heavy (> 20 g/day). Weekly frequency of moderate physical activity (defined as more than 30 min of activity per day inducing slight breathlessness) was also assessed, and regular exercise was defined as ≥ 3 times/week [30]. Education level was categorized as less than college graduate or college graduate or more [30]. Diabetes mellitus and hypertension were defined as ever diagnosis with these diseases or presently taking related medications.
Physical characteristics and serum biochemical parameters were measured by trained nurses as previously reported [22, 30]. Height and weight were measured with individuals wearing a lightweight hospital gown and bare feet, using automated instruments (InBody 3.0 and Inbody 720, Biospace Co., Seoul, Republic of Korea) that were validated for reproducibility and accuracy of body composition measurements [31] and were calibrated every morning before testing. BMI was calculated by dividing weight (kg) by the square of height (m2). Obesity was defined as BMI ≥ 25 kg/m2 [32]. Blood pressure (BP) was measured with a standard sphygmomanometer after at least 5 min of seated rest. Measurements were performed twice at 5-min intervals and were averaged for analysis.
After at least a 10-h fast, a blood sample was drawn for measurement of liver enzymes, creatinine, lipid profiles, glucose, glycated hemoglobin (HbA1c), insulin, and high-sensitivity C-reactive protein (hsCRP). Serum total cholesterol and triglycerides were determined with an enzymatic colorimetric assay. Low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) were determined through a homogeneous enzymatic colorimetric test. Serum glucose was measured using the hexokinase method on a Cobas Integra 800 apparatus (Roche Diagnostics). HbA1c was measured using an immunoturbidimetric assay with a Cobra Integra 800 automatic analyzer (Roche Diagnostics).
Serum insulin levels were measured using an electrochemiluminescence immunoassay on a Modular Analytics E170 apparatus (Roche Diagnostics, Tokyo, Japan). Serum hs-CRP levels were measured using a nephelometric assay (BNII nephelometer, Dade Behring, Deerfield, IL, USA). The inter- and intra-assay coefficients of variation for quality control specimens were < 5% for the blood variables. IR was assessed using the homeostasis model assessment of insulin resistance (HOMA-IR) equation: fasting blood insulin (µU/ml) × fasting blood glucose (mmol/l)/22.5 [33]. The Laboratory Medicine Department at Kangbuk Samsung Hospital is accredited and participates annually in inspections and surveys by the Korean Association of Quality Assurance for Clinical Laboratories.
Definition of metabolic health and insulin resistance
We selected metabolically healthy subjects using metabolic syndrome components of harmonized criteria [2]. Because risk for health implications of metabolic syndrome such as lung dysfunction [8,9,10,11,12,13, 17] and all-cause or cardiovascular mortality [34] increased incrementally, beginning at 1 risk factor, a very strict definition of metabolic health could be necessary to define the ideally healthy group as a reference to provide a very clear test to determine the effects of MS on lung function impairment that was missed in the previous studies. Therefore, metabolically healthy (MH) was defined as having none of the following metabolic abnormalities [7, 8]: (1) fasting glucose level (FBS) ≥ 100 mg/dL or on medications for diabetes, (2) BP ≥ 130/85 mmHg or on anti-hypertensive drugs, (3) triglyceride (TG) level ≥ 150 mg/dL or on lipid-lowering drugs, (4) high-density lipoprotein cholesterol (HDL-C) < 40 mg/dL in men or < 50 mg/dL in women, and (5) IR defined as HOMA-IR score ≥ 2.5 [35]. In contrast, metabolic syndrome (MS) was defined as having one or more of these metabolic abnormalities. According to these criteria, participants were divided into three groups: MH, MS without IR, and MS with IR.
Lung function measurement
Spirometry was performed according to the American Thoracic Society/European Respiratory Society guidelines [36], using the Vmax22 system (Sensor-Medics, Yorba Linda, CA, USA). Forced expiratory volume in 1s (FEV1) and forced vital capacity (FVC) were obtained under a pre-bronchodilatory setting. The highest FEV1 and FVC values from three or more tests with acceptable curves were used for analyses. The predicted values for FEV1 and FVC were calculated using equations for a representative Korean population sample [37]. The predicted FEV1% (FEV1%) and FVC% (FVC%) were calculated by dividing the measured value (L) by the predicted value (L) and converting the quotient into a percentage. The ratio of FEV1 to FVC (FEV1/FVC) was calculated using the actual measurements. The following criteria were used to determine impaired lung function: FEV1% <80%, FVC% <80%, and FEV1/FVC < 0.7 (obstructive lung function, OLF) [36].
Statistical analyses
Data are expressed as mean ± standard deviation (SD) or median and interquartile range (IQR) for continuous variables and as number (%) for categorical variables. The normality of continuous variables was assessed with the Kolmogorov-Smirnov test. The baseline continuous variables were stratified by metabolic health and IR status and were compared using one-way analysis of variance (ANOVA) or Kruskal-Wallis test. Chi-square test or Fisher’s exact test was used for categorical variables.
Analysis of covariance (ANCOVA) was performed to test differences in mean values of lung function parameters between the three groups divided by metabolic health and IR status after adjusting for age, sex, and continuous variables with P < 0.05 in univariate analyses. Post-hoc analysis was performed using the Bonferroni correction to compare the mean spirometric values between study groups.
All covariates were transformed into categorical variables to analyze the significance of differences between the three groups: high or low and with or without. Differences among the three groups were tested using Chi square or Fisher’s exact test. Multivariate analysis using binary logistic regression was conducted to examine the impact of IR on MS-related lung effects. Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were estimated to determine the risk for lung function impairment in MS, MS without IR, and MS with IR compared with MH (reference). We used three models to progressively adjust for potential confounders: model 1 was adjusted for age, sex, center, smoking status, alcohol intake, regular exercise, and education level; model 2 was adjusted as in model 1 plus for metabolic components of BMI, total cholesterol, low-density lipoprotein cholesterol (LDL-C), and HbA1c; model 3 was adjusted as in model 2 plus for hsCRP and variables with P < 0.05 in univariate analyses. As FVC (L) and FEV1 (L) were strongly correlated (r = 0.942, P < 0.001), they were assessed separately to avoid confounding effects. All tests were two-sided, and P values < 0.05 were considered statistically significant. Data were analyzed using IBM SPSS Statistics 24.0 (IBM Corp., Armonk, NY, USA).
Results
Baseline characteristics of participants
The baseline characteristics of the 114,143 eligible subjects (57.2% male, 39.6 ± 7.8 years), stratified into three groups (MH, MS without IR, and MS with IR) are shown in Table 1. Classification of subjects according to metabolic health and IR status showed that 49.3% were MH, 35.3% were MS without IR, and 15.4% were MS with IR. The prevalence of MS was 50.7%, the mean BMI was 23.6 ± 3.3 kg/m2, and 57.4% of subjects were non-smokers. Of the study population, 2.0% had diabetes and 7.2% were hypertensive. MS groups were older and more likely to be men, to have smoked, and to drink alcohol. Specifically, subjects in the MS with IR group had the worst levels of TG, HDL-C, fasting glucose, HbA1c, insulin, hsCRP, and blood pressure (BP) among the groups (P < 0.001). Also, the values of FEV1, FEV1%, FVC, and FVC% were significantly lower in the MS with IR group than in the other two groups (P < 0.001). However, the MS without IR group included the highest proportion of subjects who exercised regularly.
Lung function among the three groups divided by metabolic health and IR status
Table 2 displays the comparison of lung function parameters between study groups after adjusting for age, sex, center, BMI, smoking (pack-years), alcohol consumption (g/day), moderate physical activity frequency (times/week), systolic BP, glucose, HbA1c, insulin, lipid profiles, liver enzymes, creatinine, and hsCRP. The MS with IR group had the lowest values of FEV1 (L), FEV1%, FVC (L), and FVC% but the highest FEV1/FVC ratio among the three groups (P < 0.001). All spirometric values were significantly different among groups (P < 0.001) except FEV1%, FVC%, and FEV1/FVC ratio between the MH and MS without IR groups.
Comparison of clinical and laboratory parameters among groups stratified by metabolic health and IR status
Table 3 shows the comparison of clinical and laboratory characteristics among the three groups. Subjects in the MH group were younger and less likely to smoke and drink alcohol and more subjects were highly educated. In contrast, the MS with IR group showed significantly worse BMI, hepatic enzymes, lipid profiles, FBS, HbA1c, hs-CRP, insulin, and BP than the other two groups. Moreover, the proportions of subjects with FEV1% <80% and FVC% <80% were significantly higher in the MS with IR group compared to the other groups.
Odds ratios for impaired lung function according to metabolic health and IR status
Multiple logistic regression analysis was performed to determine the effects of MS and IR on lung function impairment (Table 4). After adjusting for only demographic variables of age, sex, center, smoking status, alcohol intake, regular exercise, and education level (model 1), ORs for FEV1% and FVC% (aOR = 1.362 (1.277–1.453) and 1.384 (1.291–1.483), respectively) were significantly higher in MS subjects compared to the MH (reference) group. However, MS was no longer a significant risk for lung dysfunction after adjusting for additional metabolic components of BMI, TC, LDL-C and HbA1c (model 2).
To investigate the effects of these observed associations were mediated by IR in the same way, we estimated aORs for lung dysfunction in the three groups stratified by metabolic health and IR status. According to the fully adjusted logistic regression analysis (model 3), MS with IR was associated with decreased FEV1% and FVC% (aOR = 1.374 (1.205–1.566) and 1.428 (1.237–1.647), respectively), whereas MS without IR was not significantly associated with lung dysfunction. In contrast, the difference in aORs for OLF between groups was consistently not significant.
Discussion
In the current cohort study, the label of MS, defined as presence of any MS component including IR, was not associated with lung dysfunction. In contrast, MS with IR was associated with decreased lung function, but this was not evident for MS without IR. This indicates that IR is a more important determinant for lung dysfunction than is MS. To the best of our knowledge, this study is the first to describe MS-related lung effects using a definition including IR as a criterion and supports the critical effect of IR on lung function.
Recent meta-analysis showed the harmful effects of MS on lung function [6]. However, we demonstrated that the association between MS and lung dysfunction is largely attenuated after adjustment for other metabolic parameters and inflammation markers that are not included in the criteria for MS but are related to lung health [38]. In contrast to previous studies, we used a less-strict definition in an apparently lung disease-free and middle-aged population, which resulted in shifting our subjects with MS to those with a low burden of metabolic abnormalities. These changes seemed to attenuate the effect of MS on lung function and may have contributed to the lack of statistical significance. Our differing results from previous studies may complicate conclusions on whether MS has a negative effect on lung function. However, it may provide a clear test of the association between MS and lung function that was missed in previous studies, because lung dysfunction is related to each metabolic parameter [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26] and their intensity [9,10,11,12,13,14,15]. Therefore, the label of MS may not consistently be optimized to predict lung dysfunction but can be an artifact of the choice of factors used to define altered metabolism related to lung dysfunction.
In contrast, our findings support the role of IR in lung dysfunction and MS. IR is a multifaceted syndrome related to individual MS components [39]. In addition, lung dysfunction has been reported in individuals with IR [22, 23, 25], and impaired lung function predicts the development of IR [40]. Consequently, IR is thought to serve as a “primary link” between lung function impairment and MS [5, 22, 24, 28]. However, concurrent definitions of MS appear to be only modestly successful in identifying IR. Moreover, the greater is the number of MS components present, the higher is the prevalence of IR [29]. The disagreement between MS definition and presence of IR could lead to limitations of concurrent definitions of MS for explanation of MS-related lung dysfunction, especially when using a less strict definition of MS, as in the current study. This could explain our lack of significance in the relationship between MS and lung function and MS-related lung effects according to presence of IR.
Although the precise mechanisms by which IR affects lung function remain unclear, changes in IR-related factors such as free fatty acids (FFA), inflammatory cytokines, mitochondrial dysfunction, and adipokines have been suggested [5, 39, 41]. The increase in FFA reduces glucose utilization and induces abnormal fat metabolism in skeletal muscle. IR also leads to smaller and fewer mitochondria, more of which demonstrate impaired function, which may reduce mitochondrial ATP production and skeletal muscle strength [41]. As forced respiration during spirometry requires respiratory skeletal muscle contraction, IR could mediate a decrease in lung function. Additionally, elevated FFA and hypo-adiponectinemia increase inflammatory cytokines. This could contribute to activation and adhesion of inflammatory cells to the pulmonary capillary endothelium, leading to damage to the airways and a decrease in lung function [5]. Last, hyperinsulinemia could exert a direct negative effect on the airway through airway epithelial damage and airway smooth muscle proliferation [5]. Taken together, these findings indicate IR as an explanatory mechanism leading to lung dysfunction.
Interestingly, we found no association between OLF and MS, regardless of the presence of IR. The reasons for this result are not fully understood. The effect of MS on OLF is controversial, with one study finding a negative correlation [12] and others finding the opposite [18, 20], although most found no association [9,10,11, 14, 16, 22, 24, 28], as in our study. Also, OLF is associated with systemic inflammation [42] but not IR [28]. It seems that the major effect of metabolic derangement is on the lung tissue, with slight effect on airway diameter. Previous studies have also shown an association of OLF with systemic inflammation [42] but not MS [24, 28]. Metabolic derangement could not be associated with OLF, especially in our cohort with median CRP close to the upper normal limit to define systemic inflammation. Moreover, functional debility of the airways might have gone undetected on screening spirometry in our healthy subjects because OLF predominantly reflects obstruction of large airways. These seem to attenuate the relationship between MS and OLF, and careful consideration is required when assessing OLF based on screening spirometry, especially in healthy young and middle-aged subjects.
The current study demonstrates a clear association of modifiable IR with lung dysfunction. Lung dysfunction is associated with respiratory and non-respiratory diseases as well as their risk of mortality [1,2,3]. Therefore, this study has an important strength in that early detection and intervention for IR can reduce mortality risk related to respiratory and other non-respiratory complications. Other strengths of our study are a large sample size, standardized spirometric techniques, and extensive data on potential confounders that increased precision and permitted sufficient statistical power.
However, our study has several limitations. First, a cross-sectional study design tends to incur uncertainty regarding the temporal sequence of exposure–outcome relations. Thus, further longitudinal follow-up studies are needed to validate our findings. Second, our results were obtained from middle-aged asymptomatic and relatively healthy Korean adults. Therefore, our findings cannot be generalized to other demographic populations. In addition, there might be considerable differences in the outcomes based on MS definition [27]. Consequently, the current results should be interpreted cautiously in accordance with racial differences and the criteria used to define MS. Finally, it is possible that some subjects had undetected cardio-metabolic and pulmonary disease because of the questionnaire-based collection of medical histories. This might have altered outcomes, as these subclinical diseases can contribute to lung dysfunction especially among individuals with MS or IR.
In conclusion, the effect of MS on lung function could be altered according to the presence of IR. Therefore, IR is a more important determinant for lung dysfunction than is the label of MS. Our study supports and extends previous findings that IR could be a critical component in mediating the association between MS and lung dysfunction. However, longitudinal follow-up studies and prospective interventional studies are needed to validate our findings.
Data Availability
The data are not publicly available because of institutional review board restrictions (the data were not collected in a way that could be distributed widely). However, the analytical methods are available from the corresponding author upon request.
Abbreviations
- ANCOVA:
-
analysis of covariance
- aOR:
-
adjusted odds ratio
- BMI:
-
body mass index
- BP:
-
blood pressure
- CI:
-
confidence interval
- FBS:
-
fasting glucose level
- FEV1%:
-
percent predicted forced expiratory volume in 1 s
- FFA:
-
free fatty acids
- FVC%:
-
percent predicted forced vital capacity
- HbA1c:
-
glycated hemoglobin
- HDL-C:
-
high-density lipoprotein cholesterol
- HOMA-IR:
-
homeostasis model assessment of insulin resistance
- hsCRP:
-
high-sensitivity C-reactive protein
- IR:
-
insulin resistance
- IQR:
-
interquartile range
- LDL-C:
-
low-density lipoprotein cholesterol
- MH:
-
metabolically healthy
- MS:
-
metabolic syndrome
- OLF:
-
obstructive lung function
- SD:
-
standard deviations
- TC:
-
total cholesterol
- TG:
-
triglycerides
References
Sepulveda-Loyola W, Carnicero JA, Alvarez-Bustos A, Probst VS, Garcia-Garcia FJ, Rodriguez-Manas L. Pulmonary function is associated with frailty, hospitalization and mortality in older people: 5-year follow-up. Heart Lung. 2023;59:88–94.
Higbee DH, Granell R, Davey Smith G, Dodd JW. Prevalence, risk factors, and clinical implications of preserved ratio impaired spirometry: a UK Biobank cohort analysis. Lancet Respir Med. 2022;10(2):149–57.
Ramalho SHR, Shah AM. Lung function and cardiovascular disease: a link. Trends Cardiovasc Med. 2021;31(2):93–8.
Colak Y, Afzal S, Nordestgaard BG, Lange P, Vestbo J. Importance of early COPD in young adults for development of clinical COPD: findings from the Copenhagen General Population Study. Am J Respir Crit Care Med. 2021;203(10):1245–56.
Baffi CW, Wood L, Winnica D, Strollo PJ Jr, Gladwin MT, Que LG, et al. Metabolic syndrome and the lung. Chest. 2016;149(6):1525–34.
Fang NN, Wang ZH, Li SH, Ge YY, Liu X, Sui DX. Pulmonary function in metabolic syndrome: a Meta-analysis. Metab Syndr Relat Disord. 2022;20(10):606–17.
Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640-5.
Primeau V, Coderre L, Karelis AD, Brochu M, Lavoie ME, Messier V, et al. Characterizing the profile of obese patients who are metabolically healthy. Int J Obes (Lond). 2011;35(7):971–81.
Nakajima K, Kubouchi Y, Muneyuki T, Ebata M, Eguchi S, Munakata H. A possible association between suspected restrictive pattern as assessed by ordinary pulmonary function test and the metabolic syndrome. Chest. 2008;134(4):712–8.
Wang F, Tian D, Zhao Y, Li J, Chen X, Zhang Y. High-Density Lipoprotein Cholesterol: A Component of the Metabolic Syndrome with a New Role in Lung Function. 20210602; 2021, Evid Based Complement Alternat Med, p.6615595.
Park BH, Park MS, Chang J, Kim SK, Kang YA, Jung JY, et al. Chronic obstructive pulmonary disease and metabolic syndrome: a nationwide survey in Korea. Int J Tuberc Lung Dis. 2012;16(5):694–700.
Ford ES, Cunningham TJ, Mercado CI. Lung function and metabolic syndrome: findings of National Health and Nutrition Examination Survey 2007–2010. J Diabetes. 2014;6(6):603–13.
Bae MS, Han JH, Kim JH, Kim YJ, Lee KJ, Kwon KY. The relationship between metabolic syndrome and pulmonary function. Korean J Fam Med. 2012;33(2):70–8.
Paek YJ, Jung KS, Hwang YI, Lee KS, Lee DR, Lee JU. Association between low pulmonary function and metabolic risk factors in korean adults: the Korean National Health and Nutrition Survey. Metabolism. 2010;59(9):1300–6.
Chen WL, Wang CC, Wu LW, Kao TW, Chan JY, Chen YJ, et al. Relationship between lung function and metabolic syndrome. PLoS ONE. 2014;9(10):e108989.
Leone N, Courbon D, Thomas F, Bean K, Jego B, Leynaert B, et al. Lung function impairment and metabolic syndrome: the critical role of abdominal obesity. Am J Respir Crit Care Med. 2009;179(6):509–16.
Choi JH, Park S, Shin YH, Kim MY, Lee YJ. Sex differences in the relationship between metabolic syndrome and pulmonary function: the 2007 Korean National Health and Nutrition Examination Survey. Endocr J. 2011;58(6):459–65.
Lam KB, Jordan RE, Jiang CQ, Thomas GN, Miller MR, Zhang WS, et al. Airflow obstruction and metabolic syndrome: the Guangzhou Biobank Cohort Study. Eur Respir J. 2010;35(2):317–23.
Koo HK, Kim DK, Chung HS, Lee CH. Association between metabolic syndrome and rate of lung function decline: a longitudinal analysis. Int J Tuberc Lung Dis. 2013;17(11):1507–14.
Funakoshi Y, Omori H, Mihara S, Marubayashi T, Katoh T. Association between airflow obstruction and the metabolic syndrome or its components in japanese men. Intern Med. 2010;49(19):2093–9.
Yoshimura C, Oga T, Chin K, Takegami M, Takahashi K, Sumi K, et al. Relationships of decreased lung function with metabolic syndrome and obstructive sleep apnea in japanese males. Intern Med. 2012;51(17):2291–7.
Lim SY, Rhee EJ, Sung KC. Metabolic syndrome, insulin resistance and systemic inflammation as risk factors for reduced lung function in korean nonsmoking males. J Korean Med Sci. 2010;25(10):1480–6.
Kim SK, Hur KY, Choi YH, Kim SW, Chung JH, Kim HK, et al. The relationship between lung function and metabolic syndrome in obese and non-obese korean adult males. Korean Diabetes J. 2010;34(4):253–60.
Lin WY, Yao CA, Wang HC, Huang KC. Impaired lung function is associated with obesity and metabolic syndrome in adults. Obes (Silver Spring). 2006;14(9):1654–61.
Kim SK, Bae JC, Baek JH, Jee JH, Hur KY, Lee MK, et al. Decline in lung function rather than baseline lung function is associated with the development of metabolic syndrome: a six-year longitudinal study. PLoS ONE. 2017;12(3):e0174228.
Rogliani P, Curradi G, Mura M, Lauro D, Federici M, Galli A, et al. Metabolic syndrome and risk of pulmonary involvement. Respir Med. 2010;104(1):47–51.
Hinnouho GM, Czernichow S, Dugravot A, Batty GD, Kivimaki M, Singh-Manoux A. Metabolically healthy obesity and risk of mortality: does the definition of metabolic health matter? Diabetes Care. 2013;36(8):2294–300.
Fimognari FL, Pasqualetti P, Moro L, Franco A, Piccirillo G, Pastorelli R, et al. The association between metabolic syndrome and restrictive ventilatory dysfunction in older persons. J Gerontol A Biol Sci Med Sci. 2007;62(7):760–5.
Cheal KL, Abbasi F, Lamendola C, McLaughlin T, Reaven GM, Ford ES. Relationship to insulin resistance of the adult treatment panel III diagnostic criteria for identification of the metabolic syndrome. Diabetes. 2004;53(5):1195–200.
Chang Y, Kim BK, Yun KE, Cho J, Zhang Y, Rampal S, et al. Metabolically-healthy obesity and coronary artery calcification. J Am Coll Cardiol. 2014;63(24):2679–86.
Malavolti M, Mussi C, Poli M, Fantuzzi AL, Salvioli G, Battistini N, et al. Cross-calibration of eight-polar bioelectrical impedance analysis versus dual-energy X-ray absorptiometry for the assessment of total and appendicular body composition in healthy subjects aged 21–82 years. Ann Hum Biol. 2003;30(4):380–91.
Organization WH, Western Pacific Region. The International Association for the Study of Obesity and the International Obesity Task Force. The Asia–Pacific perspective: redefining obesity and its treatment. Sydney, Australia: Health Communications Australia Pty Limited; 2000 Sydney, Australia: Health Communications Australia Pty Limited; 2000.
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–9.
Ho JS, Cannaday JJ, Barlow CE, Mitchell TL, Cooper KH, FitzGerald SJ. Relation of the number of metabolic syndrome risk factors with all-cause and cardiovascular mortality. Am J Cardiol. 2008;102(6):689–92.
Muniyappa R, Lee S, Chen H, Quon MJ. Current approaches for assessing insulin sensitivity and resistance in vivo: advantages, limitations, and appropriate usage. Am J Physiol Endocrinol Metab. 2008;294(1):E15–26.
Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–38.
Choi HS, Park YB, Yoon HK, Lim SY, Kim TH, Park JH, et al. Validation of previous spirometric reference equations and new equations. J Korean Med Sci. 2019;34(47):e304.
Peters U, Suratt BT, Bates JHT, Dixon AE. Beyond BMI: obesity and lung disease. Chest. 2018;153(3):702–9.
Fahed G, Aoun L, Bou Zerdan M, Allam S, Bou Zerdan M, Bouferraa Y et al. Metabolic Syndrome: Updates on Pathophysiology and Management in 2021.Int J Mol Sci. 2022;23(2).
Sagun G, Gedik C, Ekiz E, Karagoz E, Takir M, Oguz A. The relation between insulin resistance and lung function: a cross sectional study. BMC Pulm Med. 2015;15:139.
Abdul-Ghani MA, DeFronzo RA. Pathogenesis of insulin resistance in skeletal muscle. J Biomed Biotechnol. 2010;2010:476279.
Li XF, Wan CQ, Mao YM. Analysis of pathogenesis and drug treatment of chronic obstructive pulmonary disease complicated with cardiovascular disease. Front Med (Lausanne). 2022;9:979959.
Acknowledgements
We would like to thank the staff members of the Kangbuk Samsung Health Study for their hard work, dedication, and continuing support.
Author information
Authors and Affiliations
Contributions
Conception and design: J.-U.S.
Data analysis and interpretation and manuscript writing: J.-U.S., J.L., and H.K.P.
Revision of the manuscript and contribution of intellectual content: J.-U.S., J.L., H.K.P., M.-J.K., S.-Y.H., H.-I.G., and S.Y.L.
Corresponding author
Ethics declarations
Financial support
This work was supported by a 2023 scientific promotion program funded by Jeju National University.
Ethics approval and consent to participate
All procedures performed in the study were in accordance with the 1975 Declaration of Helsinki and its later amendments or comparable ethical standards. This study complies with current research ethics standards and was approved by the Institutional Review Board of Kangbuk Samsung Hospital (KBSMC 2022-03-055), which waived the requirement for informed consent due to the use of de-identified data for analysis purposes.
Consent for publication
Not applicable.
Conflict of interest
The authors have no competing interests to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lee, J., Park, H.K., Kwon, MJ. et al. The impact of insulin resistance on the association between metabolic syndrome and lung function: the Kangbuk Samsung Health Study. Diabetol Metab Syndr 15, 65 (2023). https://doi.org/10.1186/s13098-023-01042-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-023-01042-9