
Abstract
Background
Body mass index was intimately associated with islet function, which was affected by various confounding factors. Among all methods of statistical analysis, Mendelian randomization best ruled out bias to find the causal relationship. In the present study, we explored the relationship between 13 East Asian body mass index-related genes reported previously and islet function using the Mendelian randomization method.
Methods
A total of 2892 participants residing in northern China were enrolled. Anthropological information, such as sex, age, drinking status, smoking status, weight, height and blood pressure, was recorded for all participants. Fasting glucose and insulin were detected, and the insulin sensitivity index was calculated. 13 single nucleotide polymorphismss in East Asian body mass index -related genes were analysed with the ABI7900HT system.
Results
Five genetic locus mutations, CDKAL1, MAP2K5, BDNF, FTO and SEC16B, were found to be associated with body mass index and were used to estimate the genetic risk score. We found that the genetic risk score was negatively associated with the insulin sensitivity index. Even after adjusted of confounding factors, the relationship showed statistical significance. A subsequent interaction effect analysis suggested that the negative relationship between the genetic risk score and insulin sensitivity index no longer existed in the nondrinking population, and smokers had a stronger negative relationship than nonsmokers.
Conclusion
We found a negative causal relationship between body mass index-related genetic locus mutations and insulin resistance, which might be increased by acquired lifestyle factors, such as drinking and smoking status.
Similar content being viewed by others

Introduction
Insulin resistance (IR), a metabolic disorder, has been described as an epidemic in the obese population. IR is an important pathomechanism of type 2 diabetes mellitus (T2DM) [1], and it is also a risk factor for cancer [2], Alzheimer’s disease [3], polycystic ovarian syndrome [4], and cardiovascular disease [5]. Eighty percent of obese individuals have IR symptoms, and obesity-induced chronic proinflammation contributes to the development of IR. Previous studies [6, 7] have shown that obesity plays a pivotal role in the development of IR. However, there are some limitations in traditional studies exploring the association between obesity and IR.
Classical research methods, such as cross-sectional studies and case–control studies, have lower credibility in determining causal relationships [8]. These study methods cannot fully control the influence of confounding factors, which may be unknown and cannot be measured [9]. A cohort study is a good method to verify the association between obesity and IR, but this type of study consumes too much time, capital and energy. Experimental research approaches are only carried out in the laboratory and use animals as samples, and the correlation between obesity and IR in humans cannot be observed. Therefore, a new research approach in humans that reflects a causal relationship will provide a greater of awareness of IR for medical care. In addition, the interaction effect is an important method to explore the association between three variables in observational studies. However, disturbance, from an unknown factor or confounding factor, makes the interaction lose its authenticity.
Mendelian randomization (MR) is a new approach to genetic analysis that utilizes genetic loci as instrumental variables to explore the relationship between exposure factors and outcomes [10]. This method makes use of the randomization process of Mendelian laws of genetics to exclude disturbances from unknown factors and confounding factors in observational studies and can better exhibit the causal relationship between exposure factors and outcomes [11]. Simultaneously, MR provides us with a new approach to analyse the interaction effect, i.e., the effect of the exposure factor and covariate on the outcome.
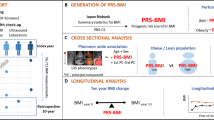
In this study, we examined 13 genetic loci reported by Wen W that were associated with body mass index (BMI) in East Asians [12]. We wanted to verify the causal relationship between BMI and islet function and to explore the effect of the interaction between BMI and other covariates on islet function.
Subjects and methods
Study populations
The study included a total of 2892 participants who lived in the city of Xuzhou, North China, from December 2020 to February 2021. This population in this community has regular physical examinations in Xuzhou Central Hospital. Individuals who met the inclusion criteria and exclusion criteria were recruited for this study. The inclusion criteria were as follows: (1) individuals were ≥ 18 years old and (2) individuals volunteered to participate in the study. The exclusion criteria were as follows: (1) type 1 diabetes mellitus; (2) acute complications from diabetes, such as diabetic ketoacidosis, a hypoglycaemic hypersomnia state, lactic acidosis or hypoglycaemic coma; (3) pregnancy; or (4) heart failure, haematologic disease, liver dysfunction, or steroid use. Because our sample was from the community, some T2DM patients with newly diagnosed were selected into this study inevitably. For controlling the heterogeneity of the participants, on the basis of T2DM diagnostic criteria of the American Diabetes Association [13], the T2DM patients, who were diagnosed less than 3 months, would be included into this study finally. In total, 2268 individuals were included in the present study.
General examinations
All participants were surveyed to collect information on sex, age, drinking status, smoking status, weight, height and blood pressure before the next examination. These covariates were measured by trained medical workers. Sex, age, and whether the subjects had a history of drinking or smoking were acquired by a questionnaire. Participants who “drank alcohol more than five times in 1 year and consumed more than 20 ml of alcohol every time in the past year” were defined as “drinking,” while others were defined as “non-drinking.” Participants who “smoked more than one cigarette per day and maintained this status over 1 year” were defined as “smokers,” and others were defined as “non-smokers.” Weight was recorded to the nearest 0.1 kg when the participants wore light clothing and no coat or shoes. After individuals rested for at least 5 min, systolic pressure and diastolic pressure were measured using a semiautomatic pressure monitor. Biomarker levels, including fasting glucose and fasting insulin, were measured by venous blood sampling. Blood was drawn from every participant after fasting overnight (8 ~ 10 h). BMI was calculated according to the following formula: BMI = weight (kg)/height2 (m). Insulin resistance was evaluated using homeostasis model assessment (HOMA), with the formula as follows: HOMA-IR = fasting glucose (mmol/l) × fasting insulin (mU/l)/22.5 [14]. Beta cell function was evaluated using HOMA-β, with the formula as follows: HOMA-β = [20 × fasting insulin (mU/l)/[fasting glucose (mmol/l)–3.5] [15]. The formula for the insulin sensitivity index was as follows: IAI = 1/[fasting glucose (mmol/l) × fasting insulin (mU/l)] [16].
Genotyping
Thirteen genetic loci related to BMI in East Asians reported by Wang W (PCSK1, GP2, GLPR/QPCTL, PAX6, ADCY3/RBJ, MC4R, GNPDA2, CDKAL1, MAP2K5, BDNF, FTO, SEC16B and TFAP2B) were detected in this study. The detection of all SNPs was performed using TaqMan SNP allelic discrimination on an ABI7900HT system (Applied Biosystems, Foster City, CA). The detected SNP alleles were transformed to numbers according to previous genome-wide association studies. We also analysed the relationship between 13 genetic loci and BMI, and some relationships with BMI in our sample were calculated using the genetic risk score (GRS). This is the first step of MR. Furthermore, the association between the GRS and outcome variables was analysed to verify the relationship between BMI and outcome variables.
Statistical analysis
Data management and analysis were performed using SAS statistical software (Version 9.3; SAS Institute, Inc., Cary, NC, USA). Descriptive statistics revealed the general clinical characteristics of the participants. Linear regression was performed to analyse the association between 13 genetic loci and BMI. Pearson’s correlation and logistic regression were used to examine the relationship between islet function and GRS. All reported P values are two-tailed. The level of statistical significance was set at P < 0.05.
Results
The clinical characteristics of all participants
In the present study, 2268 individuals were included in the final analysis (Table 1). The average age of the participants was 46.40 years, and the average BMI was 24.75 kg/m2. This study had 1105 males and 1163 females. Islet function, which included HOMA-β, HOMAIR and the IAI, was estimated by FPG and Fins. Our sample included 1516 individuals who drank alcohol and 752 nondrinking participants. Smokers made up 48.64% (1103/2268) of the study participants and non-smokers made up 51.46% (1165/2268) of the participants. 31(1.37%) T2DM patients with newly diagnosed less than 3 months were included into this study.
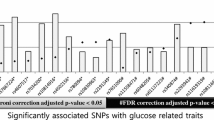
The association between SNPs and BMI
The first step of MR was to verify the association between the SNPs that we detected and BMI. Before analysis, the GRS was calculated according to the number of alleles associated with increased BMI. Table 2 provides this correlation for all participants. In our samples, five SNPs (from CDKAL1, MAP2K5, BDNF, FTO and SEC16B) were related to BMI, and the other genes (PCSK1, GP2, GLPR/QPCTL, PAX6, ADCY3/RBJ, MC4R, GNPDA2 and TFAP2B) were not associated with BMI. Using the five SNPs and their corresponding β values, we estimated the GRS for subsequent analysis. The formula for the GRS is as follows:
where ω is the β value corresponding to the SNP.
GRS was associated with islet function
As shown in Fig. 1, there was a negative correlation between the GRS and the IAI, an index of insulin sensitivity (P < 0.001). The relationship between the GRS and HOMAIR was not significant, and the GRS was also not associated with HOMAβ.

The correlation between genetic risk score and indices of islet function (A a scatter plot with the IAI(× 10) and GRS; B a scatter plot with HOMAβ and the GRS; C: a scatter plot with HOMAIR and the GRS)
Linear regression was conducted to explore the association between the GRS and islet function
Table 3 shows that there was no correlation between GRS and HOMA-IR or HOMA-β in this sample, but the IAI will always be associated with the GRS if BMI is not adjusted. The IAI result verified assumption 3 of MR, that genes act on the outcome only by influencing the exposure.
The measurement data IAI*10 were transformed into two-category data according to the lower quarter value of IAI*10; the value of IAI*10 < 0.16 was set as 1, and the others were set as 0
Figure 2 shows the OR value of the GRS for lower IAI*10 using logistic regression. When the logistic regression equation included the BMI variable, the GRS was not significant in the formula. This result conformed to the assumptions of MR (Fig. 2).

The association between genetic risk score and lower IAI*10 in the study participants
The interaction effect analysis
Drinking status and smoking status modified the association between the GRS and IAI. Figure 3A shows that the IAI*10 for drinking individuals decreased with increasing GRS, but this trend was not observed in the nondrinking participants. Interestingly, data in this figure demonstrate an interaction effect between drinking status and GRS on the IAI*10, with a P value of 0.01. Smoking status also modified this association. Figure 3B shows that there was a stronger negative relationship between GRS and IAI*10 in the smoking population, and this relationship was weak in non-smoking individuals (P = 0.019).

Drinking status and smoking status modified the association between the GRS and IAI
Discussion
In the present study, we performed MR to verify the causal relationship between BMI and islet function and to explore the effect of the interaction between BMI and covariates (lifestyle factors that included drinking status and smoking status) on islet function. Our results show that BMI was a significant reason for decreased insulin sensitivity in Chinese adults, and lifestyle could modify this causal relationship between BMI and islet function.
Our results indicated that there was a causal relationship between BMI and insensibility in Chinese individuals. It’s an important role to demonstrating a causal relationship for scientists, but experiments could not be carried out because of some limitations. For example, some research variables, such as weight, sex, college, and BMI cannot be randomly assigned [17]. If we want to study the effect of those variables on health outcomes, we must eliminate co-occurrences to get closer to understanding the causal relationship. Individual are born with specific genetic variants that are randomly drawn from our parents according to Mendelian principles. This is a naturally occurring phenomenon that offers researchers a chance to randomly manipulate the variables that we cannot manipulate experimentally [18]. This is the basic idea of MR, and three key assumptions should be considered before using MR to study the data. Assumption 1: genes are randomly assigned among the population. In our study, 13 genetic loci were reported in a previous study, and we tested for Hardy–Weinberg equilibrium to determine randomness. All genetic loci were random in our samples. Assumption 2: some genetic loci influence the exposure factor [19]. In the present study, BMI is an exposure factor, and islet function is an outcome. Linear regression was performed to analyse the association between 13 genetic loci and BMI, and five SNPs (CDKAL1, MAP2K5, BDNF, FTO and SEC16B) that impacted BMI levels. Assumption 3: genes act on the outcome only by influencing the exposure. In Table 3, our results show that the GRS influenced insulin sensitivity, but after adjusting for BMI, the effect disappeared. This result indicates that the GRS influenced the IAI*10 via BMI rather than other channels.
BMI is an important index that reflects body obesity. Higher BMI levels (BMI ≥ 28 kg/m2) are a mark of obesity. An obese body has a mass of adipose tissue, which is a large adipose storage and dynamic endocrine organ in humans [20]. Adipose tissue releases free fatty acids, reactive oxygen species, and proinflammatory cytokines such as tumour necrosis factor α, interleukin 6, and interleukin 1 beta). These molecules increase in obesity-activated NF-κB and P38 MAPK signalling to target serine residues of the insulin receptor substrate protein, which are reduced in the liver and muscles. This may be the basic obesity-induced IR mechanism. In five SNPs influencing the GRS, all genes were associated with BMI in previous studies [21, 22]. In addition, some studies found that those SNPs were also directly related to IR. In the present study, we found that those genes were associated with IR via BMI, which may be a highlight of this study.
Daily diet and lifestyle have an essential role in health. Alcohol consumption has been associated with cardiovascular disease [23], effects on cognitive performance [24], and metabolism in numerous studies. Individuals who drank regularly had a higher IR level than individuals who abstained from alcohol, but Takemi et al. published the inverse conclusion in Japanese males [25]. In the present study, we found that drinkers had a lower insulin sensitivity than nondrinking individuals, and drinking status modified the association between BMI and IR. Specifically, the insulin sensitivity of drinkers was reduced with an increasing GRS, but the nondrinking group did not show this trend. There was an interaction effect for the IAI in groups with a different drinking status. Evidence shows that drinking alcohol impairs the liver of drinkers and produces steatohepatitis and fatty liver alcohol, which elevate hepatic IR and reduce hepatic insulin sensitivity [26]. In our questionnaire, we only investigated interviewees’ alcohol consumption in the last year. If an individual had abstained from alcohol for more than 1 year, we recorded this participant as nondrinking. Therefore, our results indicated a health benefit for those who abstained from alcohol for more than 1 year. Smoking is also a bad habit for people. Previous epidemiological studies have indicated that cigarette exposure is a risk factor for developing T2DM [27]. The underlying mechanisms may be that smoking impairs peripheral insulin sensitivity and pancreatic β-cell function [28, 29]. Our result, that smokers had a stronger negative relationship between BMI and insulin sensitivity, agrees with published studies. In the present study, we performed MR to analyse the effect of the interaction between BMI and lifestyle factors on islet function. Compared with conventional statistical methods, MR can substitute genetic loci for the exposure factor to analyse the interaction effect. Stable genetic loci can eliminate disturbance due to other factors. Hence, it is credible that the interaction effect result was from MR.
There are some limitations in this study. Dozens of BMI-associated genes have been reported by previous studies. However, our study only included 13 characteristic East Asian BMI-associated genes. Diet and lifestyle are important factors in IR, but this study only analysed alcohol consumption and smoking status in relation to IR. It should be noted that we found the interaction effect between GRS and drinking (smoking) on IAI, but because of lacking of quantity data of drinking (smoking), we could not perform dose–effect relationship to explore the interaction. According to our results, we reasonably believe that the individuals with higher quantity of smoking (drinking) have a worse IAI. In the further, we will increase the sample to explore the association between lifestyle and islet function.
Conclusion
In summary, we found a causal relationship between BMI and IR, and that BMI was a significant risk factor for IR. This association was genetic, but lifestyle, such as drinking and smoking, could impair insulin sensitivity and increase IR.
Availability of data and materials
All data generated or analyzed during this study are included in this manuscript.
Abbreviations
- BMI:
-
Body mass index
- IR:
-
Insulin resistance
- T2DM:
-
Type 2 diabetes mellitus
- MR:
-
Mendelian randomization
- HOMA:
-
Homeostasis model assessment
- HOMAIR:
-
Homeostasis model assessment insulin resistance
- HOMA-β:
-
Homeostasis model assessment -Beta cell function
- IAI:
-
Insulin sensitivity index
- GRS:
-
Genetic risk score
References
Yaribeygi H, Farrokhi FR, Butler AE, Sahebkar A. Insulin resistance: review of the underlying molecular mechanisms. J Cell Physiol. 2019;234:8152–61.
Amin MN, Hussain MS, Sarwar MS, Rahman Moghal MM, Das A, Hossain MZ, Chowdhury JA, Millat MS, Islam MS. How the association between obesity and inflammation may lead to insulin resistance and cancer. Diabetes Metab Syndr. 2019;13(2):1213–24.
Diehl T, Mullins R, Kapogiannis D. Insulin resistance in Alzheimer’s disease. Transl Res. 2017;183:26–40.
Sahmay S, Aydogan Mathyk B, Sofiyeva N, Atakul N, Azemi A, Erel T. Serum AMH levels and insulin resistance in women with PCOS. Eur J Obstet Gynecol Reprod Biol. 2018;224:159–64.
Abdul-Ghani MA, Jayyousi A, DeFronzo RA, Asaad N, Al-Suwaidi J. Insulin resistance the link between T2DM and CVD: basic mechanisms and clinical implications. Curr Vasc Pharmacol. 2019;17:153–63.
Shimobayashi M, Albert V, Woelnerhanssen B, Frei IC, Weissenberger D, Meyer-Gerspach AC, et al. Insulin resistance causes inflammation in adipose tissue. J Clin Invest. 2018;128:1538–50.
Zhou M, Shao J, Wu CY, Shu L, Dong W, Liu Y, et al. Targeting BCAA catabolism to treat obesity-associated insulin resistance. Diabetes. 2019;68:1730–46.
Sattar N, Preiss D. Reverse causality in cardiovascular epidemiological research: more common than imagined? Circulation. 2017;135:2369–72.
Baumfeld Andre E, Reynolds R, Caubel P, Azoulay L, Dreyer NA. Trial designs using real-world data: the changing landscape of the regulatory approval process. Pharmacoepidemiol Drug Saf. 2020;29:1201–12.
Emdin CA, Khera AV, Kathiresan S. Mendelian randomization. Jama. 2017;318:1925–6.
Lee K, Lim CY. Mendelian randomization analysis in observational epidemiology. J Lipid Atheroscler. 2019;8:67–77.
Wen W, Zheng W, Okada Y, Takeuchi F, Tabara Y, Hwang JY, et al. Meta-analysis of genome-wide association studies in East Asian-ancestry populations identifies four new loci for body mass index. Hum Mol Genet. 2014;23:5492–504.
Meijnikman AS, De Block CEM, Verrijken A, Mertens I, Van Gaal LF. Predicting type 2 diabetes mellitus: a comparison between the FINDRISC score and the metabolic syndrome. Diabetol Metab Syndr. 2018;10:12.
Shashaj B, Luciano R, Contoli B, Morino GS, Spreghini MR, Rustico C, et al. Reference ranges of HOMA-IR in normal-weight and obese young Caucasians. Acta Diabetol. 2016;53:251–60.
Chuengsamarn S, Rattanamongkolgul S, Luechapudiporn R, Phisalaphong C, Jirawatnotai S. Curcumin extract for prevention of type 2 diabetes. Diabetes Care. 2012;35:2121–7.
Wang JZ, Wang H, Zhou HJ, Liu JM, Tang HT, Yang F, et al. Effects of electroacupuncture intervention on expression of hypothalamic PI 3 K and p-PI 3 K proteins in insulin resistance model rats. Zhen ci yan jiu Acupunct Res. 2014;39(46–51):7.
Pourhoseingholi MA, Baghestani AR, Vahedi M. How to control confounding effects by statistical analysis. Gastroenterol Hepatol Bed Bench. 2012;5:79–83.
Riaz H, Khan MS, Siddiqi TJ, Usman MS, Shah N, Goyal A, et al. Association between obesity and cardiovascular outcomes: a systematic review and meta-analysis of mendelian randomization studies. JAMA Netw Open. 2018;1:e183788.
Zheng J, Baird D, Borges MC, Bowden J, Hemani G, Haycock P, et al. Recent developments in mendelian randomization studies. Curr Epidemiol Rep. 2017;4:330–45.
Oikonomou EK, Antoniades C. The role of adipose tissue in cardiovascular health and disease. Nat Rev Cardiol. 2019;16:83–99.
Zhang J, Chi H, Xiao H, Tian X, Wang Y, Yun X, et al. Interleukin 6 (IL-6) and tumor necrosis factor α (TNF-α) single nucleotide polymorphisms (SNPs), inflammation and metabolism in gestational diabetes mellitus in inner Mongolia. Med Sci Monit. 2017;23:4149–57.
Fadaei R, Bagheri N, Heidarian E, Nouri A, Hesari Z, Moradi N, et al. Serum levels of IL-32 in patients with type 2 diabetes mellitus and its relationship with TNF-α and IL-6. Cytokine. 2020;125:154832.
Johnston-Cox H, Mather PJ. Cardiovascular disease and alcohol consumption. Am J Med Sci. 2018;355:409–10.
Gutwinski S, Schreiter S, Priller J, Henssler J, Wiers CE, Heinz A. Drink and think: impact of alcohol on cognitive functions and dementiaevidence of dose-related effects. Pharmacopsychiatry. 2018;51:136–43.
Akahane T, Namisaki T, Kaji K, Moriya K, Kawaratani H, Takaya H, et al. Chronic alcohol consumption is inversely associated with insulin resistance and fatty liver in Japanese males. Nutrients. 2020;12(4):1036.
de la Monte S, Derdak Z, Wands JR. Alcohol, insulin resistance and the liver-brain axis. J Gastroenterol Hepatol. 2012;27(Suppl 2):33–41.
Tong X, Chaudhry Z, Lee CC, Bone RN, Kanojia S, Maddatu J, et al. Cigarette smoke exposure impairs beta-cell function through activation of oxidative stress and ceramide accumulation. Mol Metab. 2020;37:100975.
Godsland IF, Walton C. Insulin resistance and cigarette smoking. Lancet. 1992;340:607.
Arnson Y, Shoenfeld Y, Amital H. Effects of tobacco smoke on immunity, inflammation and autoimmunity. J Autoimmun. 2010;34:J258–65.
Acknowledgements
We acknowledge and thank all participants for their cooperation and sample contributions.
Funding
This work was supported by the Xuzhou Municipal Science and Technology Bureau (KC21208, KC21231).
Author information
Authors and Affiliations
Contributions
XL, HX, YL and MY were drafted this manuscript and collected the sample. XL, WX and HG analyzed the data. JL and HG are responsible for the integrity of the work as a whole. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was reviewed and approved by the ethics committee of the Xuzhou central hospital. The NO. of ethics committee approval is XZXY-LJ-20201110–060.
Consent for publication
Not applicable.
Competing interests
All authors declare that there is no competing interest associated with this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, X., Xu, H., Liu, Y. et al. Lifestyle in adulthood can modify the causal relationship between BMI and islet function: using Mendelian randomization analysis. Diabetol Metab Syndr 14, 55 (2022). https://doi.org/10.1186/s13098-022-00828-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-022-00828-7