
Abstract
Background
Cardiovascular disease constitutes a major challenge for the health of community-dwelling population, it is essential to delay the development of atherosclerosis. However, long-term prospective studies analyzing the effect of type 2 diabetes (T2D) on central arterial stiffness are lacking, and roles of fasting and postprandial blood glucose (FBG and PBG) in this effect are controversial. Purpose of the current analysis was to investigate the effect of T2D on central arterial stiffness during the 5 years of follow-up, and explore whether both FBG and PBG were determinants of this effect in Chinese community-dwelling population.
Methods
The current analysis involved 898 individuals with carotid-femoral pulse wave velocity (cfPWV) ≤12 m/s. Central arterial stiffness was assessed by standard cfPWV at baseline and follow-up.
Results
Incidence of cfPWV >12 m/s was 21.3% (102 participants). Participants without T2D had an increase of cfPWV with a median of 0.6 m/s, whereas participants with T2D had an increase of cfPWV with a median of 1.2 m/s (p = 0.007). T2D had an independent effect on increased cfPWV in multivariate Logistic regression models (p < 0.05 for all). Elevated levels of both FBG and PBG determined the independent effect on increased cfPWV in multivariate linear regression models (p < 0.05 for all).
Conclusions
Type 2 diabetes had an independent effect on the development of central arterial stiffness in Chinese community-dwelling population. Both FBG and PBG should be responsible for the development of central arterial stiffness and treated as the targets of glycemic control.
Similar content being viewed by others

Background
Type 2 diabetes (T2D) places the individuals at high risk for developing the cardiovascular disease (CVD) [1, 2]. Since T2D and CVD are very common in China, the underlying mechanisms between them have been recognized as a significant public health issue and not been fully elucidated in public health field [3]. Central arterial stiffness may be a significant pathway linking T2D to CVD risk [4]. Central arterial stiffness has been considered as an useful marker of atherosclerosis and a significant determinant of CVD risk [5,6,7]. Several epidemiological studies have reported that central arterial stiffness predicts the mortality and morbidity of CVD [8,9,10,11,12]. Among the noninvasive methods available to assess the central arterial stiffness, carotid-femoral pulse wave velocity (cfPWV) has been accepted as the gold standard due to its reliability and validity [13,14,15,16].
Cardiovascular disease constitutes a major challenge for the health of Chinese community-dwelling population, it is essential to delay the development of atherosclerosis in this population. In previous studies, central arterial stiffness increases after glucose ingestion, and increased blood glucose after glucose ingestion is an independent risk factor for cardiovascular risk [17, 18]. However, there is a lack of long-term prospective studies analyzing the effect of T2D on cfPWV, especially in Chinese community-dwelling population [19]. Moreover, roles of fasting blood glucose (FBG) and postprandial blood glucose (PBG) in this effect are controversial, with some studies emphasizing PBG rather than FBG and other studies concerning FBG but not PBG [20,21,22]. Recent study has suggested that increased cardiovascular risk due to postprandial hyperglycemia might be associated with arterial dysfunction and stiffening, and it is important to examine the effect of FBG and PBG on central arterial stiffness [23]. Purpose of the current analysis was to investigate the effect of T2D on cfPWV during the 5 years of follow-up, and explore whether both FBG and PBG were determinants of this effect in Chinese community-dwelling population.
Methods
Study population
The current analysis recruited 1680 individuals of Han origin aged 18 years or older who voluntarily participated in a large medical check-up program at the health service centers in Beijing from May 2007 to July 2009. In the first stage of sampling, three districts (Fengtai, Shijingshan and Daxing) were selected from 18 districts in Beijing. In the second stage of sampling, four communities were selected from these districts. In the third stage of sampling, participants were selected from these communities. The follow-up visit was performed from February 2013 to September 2013. There were 181 participants lost, and follow-up of 5 years was completed for 1499 participants. Exclusion criteria were cfPWV >12 m/s (451 participants), missing values for variables (127 participants) and death (52 participants). There were 898 participants available for final analysis.
Physical examination
Physical examination was performed by trained physicians. Weight was measured with a digital scale, and height was measured with a wall-mounted measuring tape, with light clothes and no shoes. Body mass index (BMI) was calculated as weight (kg) divided by squared height (m2). Blood pressure was measured in the sedentary position with a standard mercury sphygmomanometer (Yuwell Medical Equipment & Supply Co. Ltd. Jiangsu, China) after a 5-min rest. Adequate-sized cuff, based on arm circumference, was applied around the right arm comfortably placed at heart level [24]. The first and fifth phases of Korotkoff sounds were used as systolic blood pressure (SBP) and diastolic blood pressure (DBP), respectively. SBP and DBP were calculated as the mean of two readings with an interval of at least 1 min. Hypertension was diagnosed with mean SBP ≥140 mmHg, mean DBP ≥90 mmHg, and/or use of anti-hypertensive drugs.
Laboratory analysis
Blood samples were drawn from participants between 8 and 10 a.m. after overnight fasting for at least 12 h, and submitted to our central laboratory. Blood triglycerides (TG), highdensity lipoprotein cholesterol (HDL-c), low-density lipoprotein cholesterol (LDL-c) and FBG were analyzed by qualified technicians blinded to clinical data using enzymatic assays (Hoffman-La Roche Ltd., Basel, Switzerland) on a fully automatic biochemical analyzer (Cobas 6000; Hoffman-La Roche Ltd.). Standard oral glucose tolerance test was performed 2 h after consumption of 75 g glucose to determine the PBG. T2D was diagnosed with FBG ≥7.0 mmol/L, PBG ≥11.1 mmol/L, and/or use of insulin or oral anti-diabetic drugs [25]. High TG was defined as TG ≥2.26 mmol/L (200 mg/dL), low HDL-c as HDL-c <1.04 mmol/L (40 mg/dL), and high LDL-c as LDL-c ≥4.14 mmol/L (160 mg/dL), and/or use of anti-dyslipidemic drugs [26, 27].
Central arterial stiffness assessment
Central arterial stiffness was assessed by automated measurement of cfPWV using Complior Colson device (Créatech, Besançon, France) at baseline and follow-up; the technical characteristics of this device have been described [28]. cfPWV along the artery was measured with two strain-gauge transducers (TY-306 Fukuda pressure-sensitive transducer; Fukuda Denshi Co. Tokyo, Japan) fixed transcutaneously over the course of arteries separated by a known distance; the carotid and femoral arteries (all on the right side) were used. After pulse waveform of sufficient quality was recorded, the digitization process was initiated by the operator, and automatic calculation of the time delay between two upstrokes was started. Measurements were repeated over ten different cardiac cycles, and mean value was used for the final analysis. cfPWV was calculated from the measurement of the pulse transit time and the distance traveled by the pulse between two recording sites (measured on the surface of the body in meters), according to the following formula: cfPWV (m/s) = distance (m)/transit time (s).
Statistical analysis
Continuous variables with normal distribution were presented as mean and standard deviation, whereas continuous variables with skewed distribution were presented as median and interquartile range. Categorical variables were presented as number and percentage. Based on the the diagnostic standard of an increase in cfPWV recommended by the international guideline, groups were determined according to cfPWV >12 or ≤12 m/s at follow-up, and continuous variables were compared between groups using Student’s t test (normal distribution) and Mann–Whitney U test (skewed distribution) [29]. Chi squared test was performed for comparative analysis of categorical variables. Wilcoxon signed-rank test was used to evaluate the change of cfPWV at baseline and follow-up. Pearson and Spearman correlations were used to evaluate the bivariate correlations. Logistic regression analysis was used to evaluate the effect of T2D on cfPWV >12 or ≤12 m/s at follow-up with adjustment for confounding factors (model 1: no adjustment; model 2: adjusted for age ≥60 years and gender; and model 3: adjusted for age ≥60 years, gender, smoker, drinker, obesity, coronary artery disease (CAD), hypertension, high TG, low HDL-c, high LDL-c, anti-hypertensive drugs, anti-dyslipidemic drugs and anti-diabetic drugs). Meanwhile, change of cfPWV was transformed to meet the multinormality assumption, and then linear regression analysis was used to evaluate whether both FBG and PBG were determinants of this effect on change of cfPWV with adjustment for confounding factors (model 1: no adjustment; model 2: adjusted for age and gender; and model 3: adjusted for age, gender, smoker, drinker, body mass index, SBP, DBP, TG, HDL-c, LDL-c, anti-hypertensive drugs, anti-dyslipidemic drugs and anti-diabetic drugs). Statistical analysis was performed using statistical package for the social science (SPSS) software (version 17.0; SPSS Inc. Chicago, IL, USA), with the level of significance set at two sided p < 0.05.
Results
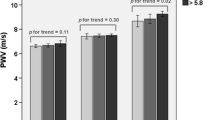
The current analysis had a median age of 53 (range 23–96) years, with 401 males and 497 females. Prevalence of T2D was 11.4% (102 participants) at baseline. Median cfPWV were 9.8 (8.8–10.7) and 10.3 (9.2–11.7) m/s at baseline and follow-up, respectively. Change of cfPWV was 0.7 m/s (p < 0.001 for change) and incidence of cfPWV >12 m/s was 21.3% (191 participants) at follow-up. Participants without T2D had an increase of cfPWV with a median of 0.6 m/s, whereas participants with T2D had an increase of cfPWV with a median of 1.2 m/s (p = 0.007). As presented in Table 1, age, SBP, FBG and PBG levels were significantly higher in participants with cfPWV >12 m/s than those with cfPWV ≤12 m/s (p < 0.05 for all). Percentages of age ≥60, males, CAD, hypertension and T2D in participants with cfPWV >12 m/s were significantly higher than those with cfPWV ≤12 m/s (p < 0.05 for all).
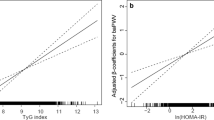
Change of cfPWV had a significant correlation not only with levels of age, DBP, FBG and PBG, but also with percentages of age ≥60, CAD, hypertension, high TG and T2D (p < 0.05 for all; Table 1). T2D had an independent effect on increased cfPWV after adjustment in all three models (p < 0.05 for all; Table 2). Elevated levels of FBG determined the independent effect on increased cfPWV in all three models (p < 0.05 for all; Table 3). When FBG was replaced by PBG, elevated levels of PBG also determined the independent effect on increased cfPWV in all three models (p < 0.05 for all; Table 3).
Discussion
T2D has been proved as a predictor for CVD in previous studies [1, 2]. An individual with T2D is generally considered to have a similar CVD risk as that of an individual without T2D but with myocardial infarction [30]. Central arterial stiffness may be a significant pathway linking T2D to CVD risk. The technical reliability and validity of cfPWV make it feasible for quantifying the central arterial stiffness in a large population. In order to determine the effect of T2D on the development of atherosclerosis in Chinese community-dwelling population, the current analysis investigated the effect of T2D on cfPWV, and explored the roles of FBG and PBG in this effect during the 5 years of follow-up.
The current analysis realized that participants with T2D had significantly higher increase of cfPWV compared with participants without T2D. Previous study has reported that an increase of cfPWV by 1 m/s leads to a 15% higher risk of CVD death, and thus change of cfPWV has significant clinical consequences [11]. Moreover, the current analysis suggested that T2D played an independent effect on central arterial stiffness even after full adjustment, and provided the evidence that central arterial stiffness was a significant and detectable mechanism between T2D and CVD. Corroborating our findings, recent studies have also found the relationship between T2D and cfPWV in other populations [20, 31]. Central arterial stiffness increases after glucose ingestion, and increased blood glucose after glucose ingestion is an independent risk factor for cardiovascular risk [17, 18]. The following pathways appear to be involved in mediating between T2D and cfPWV: firstly, T2D induces the production of reactive oxygen species through activating the oxidative stress [32, 33]; secondly, T2D reduces the nitric oxide of endothelial cells and attenuates the sensitivity of smooth muscle cells to nitric oxide [34]; thirdly, T2D stimulates the release of proinflammatory cytokines and causes the chronic inflammation [33, 35]; fourthly, T2D changes the structure of elastin and collagen in the arterial wall through raised sympathetic activity [36, 37]; finally, elevated levels of advanced glycation end-product alter the significant matrix of molecules in the arterial wall, and result in the pathological changes of arterial wall [38,39,40].
There has been controversial results about the roles of FBG and PBG in the effect of T2D on central arterial stiffness. Some studies have found that individuals with elevated levels of PBG, but not FBG, are significantly associated with central arterial stiffness [19]. However, other studies have reported that elevated levels of FBG rather than PBG are significant risk factor for central arterial stiffness and CVD [20, 21]. Recent study has suggested that increased cardiovascular risk due to postprandial hyperglycemia might be associated with arterial dysfunction and stiffening, and it is important to examine the effect of FBG and PBG on central arterial stiffness [23]. The current analysis confirmed that both FBG and PBG had an independent effect on central arterial stiffness in Chinese community-dwelling population. Fasting hyperglycemia affects vascular function through a series of different mechanisms, and inflammation plays a vital role in its association with vascular stiffness [34]. The mechanism by which postprandial hyperglycemia impairs vascular function is incompletely understood, but one major contributor is decreased bioavailability of nitric oxide caused by oxidative stress [41]. Since both FBG and PBG were independent determinants of central arterial stiffness, clinical doctors should pay attention to both FBG and PBG as the targets of glycemic control, and avoid ignoring either one of FBG and PBG in the development of central arterial stiffness and CVD.
Conclusions
This 5-year prospective analysis demonstrated that T2D had an independent effect on the development of central arterial stiffness in Chinese community-dwelling population. Moreover, both FBG and PBG should be responsible for the development of central arterial stiffness and treated as the targets of glycemic control.
Abbreviations
- T2D:
-
type 2 diabetes
- CVD:
-
cardiovascular disease
- cfPWV:
-
carotid-femoral pulse wave velocity
- FBG:
-
fasting blood glucose
- PBG:
-
ostprandial blood glucose
- SBP:
-
systolic blood pressure
- DBP:
-
diastolic blood pressure
- TG:
-
triglycerides
- HDL-c:
-
highdensity lipoprotein cholesterol
- LDL-c:
-
low-density lipoprotein cholesterol
- CAD:
-
coronary artery disease
References
University of Rochester Medical Center. How diabetes drives atherosclerosis. science daily. 2008. (http://www.sciencedaily.com/releases/2008/03/080313124430.htm).
National Diabetes Education. The link between Diabetes and Cardiovascular Disease. 2007. (http://ndep.nih.gov/media/CVD_FactSheet.pdf).
Yang W, Lu J, Weng J, Jia W, Ji L, Xiao J, Shan Z, Liu J, Tian H, Ji Q, Zhu D, Ge J, Lin L, Chen L, Guo X, Zhao Z, Li Q, Zhou Z, Shan G, He J, China National Diabetes and Metabolic Disorders Study Group. Prevalence of diabetes among men and women in China. N Engl J Med. 2010;362:1090–101.
Stehouwer CD, Henry RM, Ferreira I. Arterial stiffness in diabetes and the metabolic syndrome: a pathway to cardiovascular disease. Diabetologia. 2008;51:527–39.
Arnett DK, Evans GW, Riley WA. Arterial stiffness: a new cardiovascular risk factor? Am J Epidemiol. 1994;140:669–82.
Meaume S, Benetos A, Henry OF, Rudnichi A, Safar ME. Aortic pulse wave velocity predicts cardiovascular mortality in subjects >70 years of age. Arterioscler Thromb Vasc Biol. 2001;21:2046–50.
McLeod AL, Uren NG, Wilkinson IB, Webb DJ, Maxwell SR, Northridge DB, Newby DE. Non-invasive measures of pulse wave velocity correlate with coronary arterial plaque load in humans. J Hypertens. 2004;22:363–8.
Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, Ducimetiere P, Benetos A. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension. 2001;37:1236–41.
Laurent S, Katsahian S, Fassot C, Tropeano AI, Gautier I, Laloux B, Boutouyrie P. Aortic stiffness is an independent predictor of fatal stroke in essential hypertension. Stroke. 2003;34:1203–6.
Mattace-Raso FU, van der Cammen TJ, Hofman A, van Popele NM, Bos ML, Schalekamp MA, Asmar R, Reneman RS, Hoeks AP, Breteler MM, Witteman JC. Arterial stiffness and risk of coronary heart disease and stroke: the Rotterdam Study. Circulation. 2006;113:657–63.
Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;55:1318–27.
Zoungas S, Asmar RP. Arterial stiffness and cardiovascular outcome. Clin Exp Pharmacol Physiol. 2007;34:647–51.
Lehmann ED. Clinical value of aortic pulse-wave velocity measurement. Lancet. 1999;354:528–9.
Munakata M, Ito N, Nunokawa T, Yoshinaga K. Utility of automated brachial ankle pulse wave velocity measurements in hypertensive patients. Am J Hypertens. 2003;16:653–7.
Cruickshank K, Riste L, Anderson SG, Wright JS, Dunn G, Gosling RG. Aortic pulse-wave velocity and its relationship to mortality in diabetes and glucose intolerance: an integrated index of vascular function? Circulation. 2002;106:2085–90.
Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H, European Network for Non-invasive Investigation of Large Arteries. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27:2588–605.
Baynard T, Carhart RL Jr, Weinstock RS, Ploutz-Snyder LL, Kanaley JA. Short-term exercise training improves aerobic capacity with no change in arterial function in obesity. Eur J Appl Physiol. 2009;107:299–308.
Sorkin JD, Muller DC, Fleg JL, Andres R. The relation of fasting and 2-h postchallenge plasma glucose concentrations to mortality: data from the Baltimore Longitudinal Study of aging with a critical review of the literature. Diabetes Care. 2005;28:2626–32.
Li CH, Wu JS, Yang YC, Shih CC, Lu FH, Chang CJ. Increased arterial stiffness in subjects with impaired glucose tolerance and newly diagnosed diabetes but not isolated impaired fasting glucose. J Clin Endocrinol Metab. 2012;97:E658–62.
Lukich E, Matas Z, Boaz M, Shargorodsky M. Increasing derangement of glucose homeostasis is associated with increased arterial stiffness in patients with diabetes, impaired fasting glucose and normal controls. Diabetes Metab Res Rev. 2010;26:365–70.
Kim HK, Kim CH, Kim EH, Bae SJ, Choe J, Park JY, Park SW, Yun YD, Baek SJ, Mok Y, Jee SH. Impaired fasting glucose and risk of cardiovascular disease in Korean men and women: the Korean heart study. Diabetes Care. 2013;36:328–35.
De Angelis L, Millasseau SC, Smith A, Viberti G, Jones RH, Ritter JM, Chowienczyk PJ. Sex differences in age-related stiffening of the aorta in subjects with type 2 diabetes. Hypertension. 2004;44:67–71.
Jacome-Sosa M, Parks EJ, Bruno RS, Tasali E, Lewis GF, Schneeman BO, Rains TM. Postprandial metabolism of macronutrients and cardiometabolic risk: recent developments, emerging concepts, and future directions. Adv Nutr. 2016;7:364–74.
Alvim RO, Freitas SR, Ferreira NE, Santos PC, Cunha RS, Mill JG, Krieger JE, Pereira AC. APOE polymorphism is associated with lipid profile, but not with arterial stiffness in the general population. Lipids Health Dis. 2010;9:128.
Pereira AC, Sposito AC, Mota GF, Cunha RS, Herkenhoff FL, Mill JG, Krieger JE. Endothelial nitric oxide synthase gene variant modulates the relationship between serum cholesterol levels and blood pressure in the general population: new evidence for a direct effect of lipids in arterial blood pressure. Atherosclerosis. 2006;184:193–200.
Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP). expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA. 2001;285:2486–97.
Santos PC, Oliveira TG, Lemos PA, Mill JG, Krieger JE, Pereira AC. MYLIP p. N342S polymorphism is not associated with lipid profile in the Brazilian population. Lipids Health Dis. 2012;11:83.
Asmar R, Benetos A, Topouchian J, Laurent P, Pannier B, Brisac AM, Target R, Levy BI. Assessment of arterial distensibility by automatic pulse wave velocity measurement. Validation and clinical application studies. Hypertension. 1995;26:485–90.
Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, Grassi G, Heagerty AM, Kjeldsen SE, Laurent S, Narkiewicz K, Ruilope L, Rynkiewicz A, Schmieder RE, Boudier HA, Zanchetti A, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Filippatos G, Funck-Brentano C, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL, Erdine S, Kiowski W, Agabiti-Rosei E, Ambrosioni E, Lindholm LH, Viigimaa M, Adamopoulos S, Agabiti-Rosei E, Ambrosioni E, Bertomeu V, Clement D, Erdine S, Farsang C, Gaita D, Lip G, Mallion JM, Manolis AJ, Nilsson PM, O’Brien E, Ponikowski P, Redon J, Ruschitzka F, Tamargo J, van Zwieten P, Waeber B, Williams B, Management of ArterialHypertension of the European Society of Hypertension, European Society of Cardiology. Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European society of hypertension (ESH) and of the European society of cardiology (ESC). J Hypertens. 2007;2007(25):1105–87.
Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998;339:229–34.
Vyssoulis G, Pietri P, Vlachopoulos C, Alexopoulos N, Kyvelou SM, Terentes-Printzios D, Stefanadis C. Early adverse effect of abnormal glucose metabolism on arterial stiffness in drug naive hypertensive patients. Diab Vasc Dis Res. 2012;9:18–24.
Esposito K, Nappo F, Marfella R, Giugliano G, Giugliano F, Ciotola M, Quagliaro L, Ceriello A, Giugliano D. Inflammatory cytokine concentrations are acutely increased by hyperglycemia in humans: role of oxidative stress. Circulation. 2002;106:2067–72.
Muniandy S, Qvist R, Yan GO, Bee CJ, Chu YK, Rayappan AV. The oxidative stress of hyperglycemia and the inflammatory process in endothelial cells. J Med Invest. 2009;56:6–10.
Aronson D. Cross-linking of glycated collagen in the pathogenesis of arterial and myocardial stiffening of aging and diabetes. J Hypertens. 2003;21:3–12.
Mazzone T, Chait A, Plutzky J. Cardiovascular disease risk in type 2 diabetes mellitus: insights from mechanistic studies. Lancet. 2008;371:1800–9.
Cameron JD, Cruickshank JK. Glucose, insulin, diabetes and mechanisms of arterial dysfunction. Clin Exp Pharmacol Physiol. 2007;34:677–82.
Creager MA, Luscher TF, Cosentino F, Beckman JA. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. Circulation. 2003;108:1527–32.
McVeigh GE, Brennan GM, Johnston GD, McDermott BJ, McGrath LT, Henry WR, Andrews JW, Hayes JR. Impaired endothelium-dependent and independent vasodilation in patients with type 2 (non-insulin-dependent) diabetes mellitus. Diabetologia. 1992;35:771–6.
Naka KK, Papathanassiou K, Bechlioulis A, Kazakos N, Pappas K, Tigas S, Makriyiannis D, Tsatsoulis A, Michalis LK. Determinants of vascular function in patients with type 2 diabetes. Cardiovasc Diabetol. 2012;11:127.
Tan KC, Chow WS, Ai VH, Metz C, Bucala R, Lam KS. Advanced glycation end products and endothelial dysfunction in type 2 diabetes. Diabetes Care. 2002;25:1055–9.
Mah E, Bruno RS. Postprandial hyperglycemia on vascular endothelial function: mechanisms and consequences. Nutr Res. 2012;32:727–40.
Authors’ contributions
Conceived and designed the experiments: SF, LL, PY. Performed the experiments: SF, LL, PY. Analyzed the data: SF, WC, LL, PY. Contributed reagents/materials/analysis tools: SF, WC, LL, PY. Wrote the paper: SF, WC, LL, PY. All authors read and approved the final manuscript.
Acknowledgements
We are grateful to all study participants for their participation in the study.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
In attempt to preserve the privacy of patients, clinical data of patients will not be shared; data can be available from authors upon request.
Ethics approval and consent to participate
The study protocol was approved by Ethics Committee of Chinese People’s Liberation Army General Hospital (Beijing, China). Each participant provided written informed consent to be included in the study.
Funding
This work was supported by grants from National Key Basic Research Project (2012CB517503 and 2013CB530804), Health Special Scientific Research Project of Chinese People’s Liberation Army (12BJZ34 and 14BJZ12), and Sanya Medical and Health Science and Technology Innovation Project (2016YW21).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Shihui Fu and Wenji Chen are co-first authors
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Fu, S., Chen, W., Luo, L. et al. Roles of fasting and postprandial blood glucose in the effect of type 2 diabetes on central arterial stiffness: a 5-year prospective community-based analysis. Diabetol Metab Syndr 9, 33 (2017). https://doi.org/10.1186/s13098-017-0231-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-017-0231-3