
Abstract
Background
Acute abdomen is a medical emergency with a wide spectrum of etiologies. Point-of-care ultrasound (POCUS) can help in early identification and management of the causes. The ACUTE–ABDOMEN protocol was created by the authors to aid in the evaluation of acute abdominal pain using a systematic sonographic approach, integrating the same core ultrasound techniques already in use—into one mnemonic. This mnemonic ACUTE means: A: abdominal aortic aneurysm; C: collapsed inferior vena cava; U: ulcer (perforated viscus); T: trauma (free fluid); E: ectopic pregnancy, followed by ABDOMEN which stands: A: appendicitis; B: biliary tract; D: distended bowel loop; O: obstructive uropathy; Men: testicular torsion/Women: ovarian torsion. The article discusses two cases of abdominal pain the diagnosis and management of which were directed and expedited as a result of using the ACUTE–ABDOMEN protocol. The first case was of a 33-year-old male, who presented with a 3-day history of abdominal pain, vomiting and constipation. Physical exam revealed a soft abdomen with generalized tenderness and normal bowel sounds. Laboratory tests were normal. A bedside ultrasound done using the ACUTE–ABDOMEN protocol showed signs of intussusception. This was confirmed by CT-abdomen. The second case was of a 70-year-old female, a known case of diabetes and hypertension, who presented with a 3-hour history of abdominal pain, vomiting and diarrhea. She had a normal physical exam and laboratory studies. Her symptoms mimicking simple gastroenteritis had improved. However, bedside ultrasound, using the ACUTE–ABDOMEN protocol showed localized free fluid with dilated small bowel loop in right lower quadrant with absent peristalsis. A CT abdomen confirmed a diagnosis of intestinal obstruction. These two cases demonstrate that the usefulness of applying POCUS in a systematic method—like the “ACUTE–ABDOMEN” approach—can aid in patient diagnosis and management.
Case presentation
We are presenting two cases of undifferentiated acute abdomen pain, where ACUTE ABDOMEN sonographic approach was applied and facilitated the accurate patient management and disposition.
Conclusion
ACUTE ABDOMEN sonographic approach in acute abdomen can play an important role in ruling out critical diagnosis, and can guide emergency physician or any critical care physician in patient management.
Similar content being viewed by others



Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
The use of bedside ultrasound by physicians has become increasingly popular in the last two decades, even more so in critically ill patients. In emergency medicine, point of care ultrasound (POCUS) is being used as a diagnostic modality, given its easy accessibility and non-invasive nature. It is used as an adjunct, directing physicians on further testing modalities and treatment plans.
However, there has always been the question of reliability of ultrasound being performed by non-radiologists. In a study involving 651 patients complaining of renal colic, emergency physicians were found to have moderate to high sensitivity for identifying hydronephrosis on POCUS when compared with the consensus interpretation of the same studies by emergency radiologists [1].
Emergency ultrasound is now considered a core skill for emergency physician. American College of Emergency Physicians has introduced Emergency Ultrasound Guidelines that were introduced in 2008 and revisited in 2016, acknowledging that emergency ultrasound is a part of patient assessment within different clinical categories.
Given the time constraint and critical conditions of patients in the emergency, ultrasound approach in the ED should be focused, systemic and specific to patient symptom. Thus, the different protocols for different patient symptom came into practice. These fall under ACEP’s functional clinical category of “symptom or sign-based ultrasound”. To mention a few, FAST ultrasound for the trauma patient, RUSH protocol for the hypotensive patient, and BLUE protocol for the dyspneic patient [2].
Similarly, the ACUTE ABDOMEN protocol [3] was created by the authors to aid in the evaluation of acute abdominal pain using a systematic sonographic approach, integrating the same core ultrasound techniques already in use, into one mnemonic. This novel approach to the patient with abdominal pain systematically assesses the five critical causes—in the first part of the mnemonic “ACUTE” followed by scanning for other surgical causes in the second part of the mnemonic “ABDOMEN”.
The mnemonic ACUTE stands for—A: abdominal aortic aneurysm, C: collapsed inferior vena cava, U: ulcer (perforated viscus), T: trauma (free fluid), E: ectopic pregnancy, followed by ABDOMEN which stands for—A: appendicitis, B: biliary tract, D: distended bowel loop, O: obstructive uropathy, Men: testicular torsion, Women: ovarian torsion.
This might seem quite overwhelming and time consuming for an already busy ER, but if done in the proposed systemic approach, it can, on the contrary, provide pertinent information in a short time. An example of how the ACUTE ABDOMEN protocol directed the patient management is demonstrated in the two cases discussed below.
Case presentation
Case 1
A 33-year-old male of Asian (Pakistani) origin was presented to Rashid Emergency and Trauma Center with a complaint of sudden non-radiating epigastric abdominal pain. The pain was associated with vomiting and constipation for 3 days. There was no chest pain, diarrhea, fever or melena.
The patient had similar presentation in his country 4 years ago and was managed conservatively.
Vital signs were normal. Abdomen was soft with generalized tenderness and normal bowel sounds.
Laboratory studies were normal.
Point of care ultrasound for acute abdomen (ACUTE approach) showed:
-
A: normal aortic diameter
-
C: collapsed IVC > 50%,
-
U: no free air
-
T: localized free fluid with doughnut sign (Fig. 1), and long axis of the segment showed bowel telescoping inside itself with oedematous bowel loop wall (Fig. 2).
Fig. 1 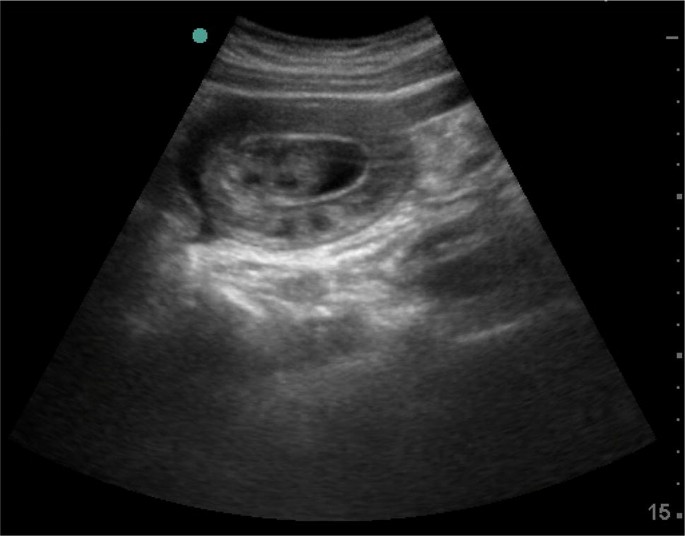
Point of care ultrasound for acute abdomen (ACUTE approach) showed localized free fluid with doughnut sign edematous bowel loop wall
Fig. 2 
Point of care ultrasound for acute abdomen (ACUTE approach) showed bowel telescoping inside itself with edematous bowel loop wall (long axis)


Abdominal X-ray was normal
After ultrasound finding, we decided to perform urgent CT scan of the abdomen which showed the evidence of long segment entero-enteric (jejuno-jejunal) intussusception seen mainly in the left side of the abdomen, with relatively collapsed intussusceptum segment. Mild amount of intraperitoneal free fluid was seen in the jejunal mesentery next to the involved segments as well as in the pelvic peritoneal pouches (Fig. 3).

CT scan abdomen with contrast showed a long segment entero-enteric (jejuno-jejunal) intussusception seen mainly in the left side of the abdomen
Surgical consultation was obtained; however, the patient preferred to continue the medical care in his country.
Case 2
A 70-year-old female diabetic and hypertensive was presented to Rashid Emergency and Trauma Center with generalized abdominal pain for 3 h after food which was associated with vomiting and diarrhea twice. There was no urinary complaint, chest pain or fever.
Vital signs were normal. Abdomen was soft with mild tenderness in the right lower abdomen, without peritonitis clinical sign. Laboratory test was insignificant, except for leukocytosis 17.2·103/μL (3.6–11.0·103/μL) and plasma lactic acid 3.7 mmol/L (0.5–2.2 mmol/L).
Point of care ultrasound for acute abdomen (ACUTE approach) showed:
-
A: normal aortic diameter
-
C: normal IVC
-
U: no free air
-
T: localized free fluid with dilated small bowel loop in right lower quadrant with absent peristalsis (Fig. 4).
Fig. 4 
Point of care ultrasound for acute abdomen showed localized free fluid * with dilated small bowel loop in right lower quadrant with absent peristalsis

CT abdomen showed evidence of significantly dilated small bowel loops in the right side of the lower abdomen and pelvis with a short segment critical stenosis measuring about 2.3 cm. It also showed an evidence suggestive of internal herniation with dilated loops of bowel. Jejunal loops and distal ileum appear collapsed. Free fluid was seen in the abdomen and pelvis (Fig. 5).

CT abdomen with contrast showed dilated small bowel loops in the right side of the lower abdomen and pelvis with a short segment critical stenosis measuring about 2.3 cm
Urgent surgical consultation was obtained and the patient had undergone laparotomy which was conclusive of an omental band adherent to the small bowel mesentery.
About 150 cm proximal to ileo cecal juction producing congestion with punctuate haemorrhages and dilatation of the proximal bowel of about 30 cm. After the band was released; the color of the bowel changed to normal with good peristalsis. No bowel resection was needed.
Patient post-operative course was uneventful, and she was discharged home after 5 days.
Patient symptoms that mimicked simple gastroenteritis had improved, but because of our ultrasound finding that suggested intestinal obstruction, it was decided to perform a CT abdomen. If not for our preliminary ultrasound findings, this patient would have been discharged without further imaging.
Discussion
POCUS approaches have been published in multiple critical care conditions such as Bedside Lung Ultrasound in Emergency (BLUE) protocol in respiratory failure which concluded that lung ultrasound immediately provided the diagnosis of acute respiratory failure in 90.5% of cases. The BLUE protocol focused on lung ultrasound only [4]; however, the RUSH protocol demonstrated that initial integration of bedside ultrasound into the evaluation of the patient with shock results in a more accurate initial diagnosis with an improved patient care plan [5].
In this case series, we presented two cases where ACUTE ABDOMEN played an important role in their management, POCUS can play an important role in acute abdomen, by early recognition and diagnosing critical conditions. Instead of relying only on physical examination which might have very low sensitivity in comparison to ultrasound, for example in physical examination can identify 38% of patients with AAA [6], ultrasound by emergency physician can detect AAA in 93% to 100% of cases, with specificities approaching 100% [7,8,9].
In other pathologies like pneumoperitoneum, X-ray is more frequently used, but ultrasound is superior to upright chest and lateral decubitus X-ray where the sensitivity is 92% versus 78% for X-ray [10].
The two cases presented with undifferentiated acute abdomen, in which bedside ultrasound was started with ACUTE approach after history and physical examination, (Table 1A) [11] showed unexpected finding, which needed further radiological evaluation by CT scan with contrast and early referral to surgical team.
For the second part of the approach, ABDOMEN (Table 1B) [11] usually will be a secondary survey and will focus the assessment with guide of the history and examination.
Conclusions
ACUTE and ABDOMEN sonographic approach in acute abdomen can play an important role in ruling out critical diagnosis, and can guide emergency physician or any critical care physician in patient management.
Further prospective studies are warranted.
Availability of data and materials
Not applicable.
Abbreviations
- POCUS:
-
point of care ultrasound
- BLUE:
-
bedside lung ultrasound in emergency
- RUSH:
-
rapid ultrasound in shock
- AAA:
-
abdominal aortic aneurysm
- IVC:
-
inferior vena cava
References
Pathan S, Mitra B, Mirza S, Momin U, Ahmed Z, Andraous L et al (2018) Emergency physician interpretation of point-of-care ultrasound for identifying and grading of hydronephrosis in renal colic compared with consensus interpretation by emergency radiologists. Acad Emerg Med 25(10):1129–1137
Ultrasound Guidelines: emergency, point-of -care, and clinical ultrasound guidelines in medicine. Acep.org (2019). https://acep.org/patient-care/policy-statements/ultrasound-guidelines-emergency-point-of–care-andclinical-ultrasound-guidelines-in-medicine/. Accessed 14 Mar 2019
Abdominal Pain in ED (2017) Using a novel sonographic approach Maryam Al Ali and Salma Alrajaby Emergency Department, Rashid Hospital, Dubai, United Arab Emirates. Eur J Emerg Med. 24:e1–e15
Lichtenstein D, Mezière G (2008) Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE Protocol. Chest 134(1):117–125
Perera P, Mailhot T, Riley D, Mandavia D (2012) The RUSH Exam 2012: rapid ultrasound in shock in the evaluation of the critically ill patient. Ultrasound Clin 7(2):255–278
Chervu A, Clagett G, Valentine R, Myers S, Rossi P (1995) Role of physical examination in detection of abdominal aortic aneurysms. Surgery 117(4):454–457
Dent B, Kendall RJ, Boyle AA et al (2007) Emergency ultrasound of the abdominal aorta by UK emergency physicians: a prospective cohort study. Emerg Med J 24:547–549
Costantino TG, Bruno EC, Handly N et al (2005) Accuracy of emergency medicine ultrasound in the evaluation of abdominal aortic aneurysm. J Emerg Med 29:455–460
Tayal VS, Graf CD, Gibbs MA (2003) Prospective study of accuracy and outcome of emergency ultrasound for abdominal aortic aneurysm over two years. Acad Emerg Med 10:867–871
Chen S, Yen Z, Wang H, Lin F, Hsu C, Chen W (2002) Ultrasonography is superior to plain radiography in the diagnosis of pneumoperitoneum. Br J Surg 89(3):351–354
Case Report: POCUS to FOCUS–POCUS Journal. Pocusjournal.com (2018). http://pocusjournal.com/article/2018-03-01p15-17/. Accessed 28 Aug 2018
Acknowledgements
None.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
SJ: presentation of the cases, MAA and SA: discussion of the case. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Al Ali, M., Jabbour, S. & Alrajaby, S. ACUTE ABDOMEN systemic sonographic approach to acute abdomen in emergency department: a case series. Ultrasound J 11, 22 (2019). https://doi.org/10.1186/s13089-019-0136-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13089-019-0136-5