
Abstract
Background
Juvenile idiopathic arthritis (JIA) is the most common chronic rheumatic disease in children, causing significant morbidity. Despite the dramatic improvement in treatment, many patients do not achieve complete remission, and biomarkers for subclinical disease, flares, and response to treatment are lacking. Neutrophils and neutrophil extracellular traps (NETs) play key roles in the pathogenesis of autoimmune and inflammatory conditions. In this study, we characterized neutrophil enzyme activity and NETs formation in oligoarticular and polyarticular JIA and explored their association with disease activity.
Methods
Neutrophils from 6 healthy controls and 7 patients with oligoarticular and polyarticular JIA were freshly isolated at time of diagnosis and after glucocorticoid intra-articular injection. Enzymatic activity of neutrophil granular enzymes was monitored by colorimetry and PMA-activated NETs formation was assessed using fluorescent microscopy.
Results
In this pilot and feasibility study, we revealed that NETs were significantly increased in oligoarticular JIA patients at time of diagnosis compared to healthy controls. Anti-inflammatory treatment using intra-articular steroid injection normalized NETs formation in these patients. Correlation between NETs formation and clinical Juvenile Activity Disease Activity Score-10 (cJADAS-10) was linear and significant (P = 0.007) in oligo but not in poly JIA patients.
Conclusions
This is the first study exploring the link of NETs formation with oligo and poly JIA activity. We demonstrated a statistically significant linear correlation between cJADAS-10 and NETs formation in oligo but not in poly JIA patients. Hence, we suggest that NETs may reflect clinical disease activity in JIA, and may serve as a putative biomarker. Further work is needed to validate these initial results and determine the dynamics of NETs formation in JIA.
Similar content being viewed by others


Background
Juvenile idiopathic arthritis (JIA) is the most common chronic rheumatic disease in children and can cause significant morbidity, including joint damage and impaired growth [1]. JIA is categorized into distinct subclasses [2], with oligoarticular (oligo) JIA and polyarticular (poly) JIA being the most prevalent [3,4,5]. Apart from the number of inflamed joints during the first 6 months of disease, some mechanistic and immunologic overlaps exist between these two JIA subtypes. Consistently, there is growing consensus that among positive Anti-Nuclear Antibody (ANA) patients, oligo JIA and rheumatoid factor (RF)-negative poly JIA share many clinical characteristics and may represent a continuum of a single disease entity rather than distinct diseases [6, 7]. Despite the dramatic improvement in the disease treatment by the inclusion of biological therapy, many patients still do not achieve complete remission. Furthermore, biomarkers are needed to improve the goal of “treat to target” in JIA. These markers can assist in the detection of subclinical disease, response to therapy, and prediction of flares.
Neutrophils, the most abundant leukocyte in the circulating blood, represent the first line of defense within the innate immune system [8]. Neutrophils protect the host by several mechanisms including phagocytosis, the release of cytotoxic molecules, and the formation of neutrophil extracellular traps (NETs) [9]. NETs are extruded by activated neutrophils and are composed of DNA fibers, histones, and antimicrobial proteins such as neutrophil elastase (NE) and myeloperoxidase (MPO). NETs trap extracellular pathogens and hence protect organisms from infections [10, 11]. However, in recent years it was demonstrated that NETs are also formed in non-infectious conditions [12] including inflammatory and autoimmune diseases such as systemic lupus erythematosus (SLE) [13,14,15], rheumatoid arthritis (RA) [16, 17], anti-neutrophil cytoplasmic antibodies-associated vasculitis [18, 19] and inflammatory bowel disease (IBD) [20]. NETs formation has been intensively studied in adult rheumatic diseases and has been proposed to be involved in both its initiation and progression. In RA, increased NETs formation was shown to be associated with increased disease activity and is therefore considered a new biomarker for monitoring disease activity, possibly allowing for early preventive treatment intervention [17]. The role of NETs in pediatric-onset rheumatic diseases in general and in JIA, in particular, has not been adequately addressed [21,22,23]. Studies in JIA showed a correlation between disease activity and S100A8/A9 proteins, which are primarily present in the cytoplasm of neutrophils and monocytes [24]. S100A12, a marker for neutrophil activation, was also found to be present in the serum and synovial fluid (SF) of JIA patients [23].
Recent study exploring the presence of NET-associated markers in JIA has found that the number of citrullinated histone H3 + neutrophils was higher in the peripheral blood of patients with JIA than in healthy donors, implying an increased NETs formation in JIA. Additionally, they also observed elevated levels of NET-associated products including NE, LL37 (cathelicidin antimicrobial peptide), and cell-free DNA-histone complexes in the same JIA cohort [25].
Understanding the role of neutrophils in JIA can potentially facilitate the detection of subclinical disease and the prediction of disease course. In this study, we aimed to characterize neutrophil enzymes’ activity and NETs formation in oligoarticular and polyarticular JIA and specifically explore its association with JIA disease activity.
Methods
Study population
This is a single-center prospective study conducted at Dana Children’s Hospital of Tel Aviv Medical Center, Tel Aviv, Israel. All parents signed an informed consent form in accordance with the Declaration of Helsinki, Institutional Review Board, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel 0502–19-TLV.
The source for this cohort is a larger cohort of 22 children with JIA aged 1–18 years, recruited in the pediatric rheumatology clinic of Dana Dwek Children’s Hospital between 2/2020 and 2/2021. Inclusion criteria for the larger cohort were a diagnosis of JIA by the International League of Associations for Rheumatology criteria (ILAR) criteria [2], with longitudinal data collection including clinical data and blood samples.
For this study, we included only 7 children from the larger cohort, who were those with a diagnosis of oligo- or RF − poly-JIA who had samples from both time of diagnosis and from the time of first follow-up visit after the initiation of the anti-inflammatory treatment, that included intra-articular steroid injection for all patients, and methotrexate initiated at time of the steroid injection in most of the poly-JIA patients. Patients with systemic-onset JIA and RF + poly JIA were excluded from the analysis, as well as patients who were already being treated with anti-inflammatory medications at the time of the recruitment, including NSAIDS and steroids.
In addition, blood samples were obtained from 6 healthy volunteers, aged 1–18, who were hospitalized for elective surgery and were used as controls. These participants had no chronic or inter-current inflammatory disease and did not take any medications.
For JIA patients, all study visits included physical examination for joint count (0–10 active joints), physician’s global assessment (PhGA) of disease activity on a visual analog scale (VAS) (0–10 cm), and parent/patient-reported global assessment (PGA) of well-being, assessed by a parent if the child was ≤ 9 years old (VAS 0–10 cm). A blood sample was drawn on each visit and included white blood cells (WBC), absolute neutrophilic count (ANC), absolute lymphocytic count (ALC), and C-reactive protein (CRP). Antibody profile from the time of diagnosis included anti-nuclear antibody detected by indirect immunofluorescence assay (ANA-IFA), RF, and anti-cyclic citrullinated peptide (anti-CCP). The clinical JADAS-10 (cJADAS-10) was calculated from the sum of the number of active joints, PhGA, and PGA. The Juvenile Activity Disease Activity Score-10 (JADAS-10) was calculated from the sum of the active joint count, PhGA, PGA, and normalized CRP to a scale of 0–10 [26]. In addition to routine laboratory testing, a blood sample was collected for neutrophil isolation to monitor NE and MPO activity, as well as the percentage of NETs forming neutrophils following PMA activation. Correlation between the disease activity score cJADAS10 or NETs formation and the following metrics were assessed: NE activity, MPO activity, and NETs formation.
Materials
Phosphate buffered saline (PBS) was obtained from Biological Industries. Ethylenediamine tetra-acetic acid (EDTA), bovine serum albumin (BSA), glucose, phorbol 12-myristate 13-acetate (PMA), and Triton X-100 were all purchased from Sigma-Aldrich (MO, USA). Poly-L-lysine solution (0.01%) and buffered 4% paraformaldehyde solution were acquired from Merck (NJ, USA).
Whole blood collection and neutrophil isolation
Human peripheral blood samples (2–5 mL) in EDTA-coated vacutainer tubes (Greiner Bio-One, Austria) were obtained from all participants at each time point. Fresh blood was processed within 60 min of withdrawal. Neutrophils were isolated using EasySep Direct Human Neutrophil isolation kit (StemCell Technologies Inc., Canada), based on immunomagnetic negative selection, according to the manufacturer’s instructions. The number of isolated neutrophils was quantified using Beckman coulter DxH800 (Beckman Coulter Inc., CA, USA), and the final concentration was adjusted to 107/ml in RPMI.
Neutrophil elastase enzymatic activity
105 neutrophils were lysed in 0.2% Triton X-100 solution and incubated with 500 µM chromogenic peptide elastase substrate (Calbiochem, CA, USA) for 90 min at 37 °C. Enzymatic activity was measured by an iMark Microplate Absorbance Reader (Bio-Rad, CA, USA) at 415 nm. A calibration curve was set up by using various amounts of purified NE (Athens Research & Technology, GA, USA). Purified NE was used as a positive control, and a specific NE inhibitor IV (Calbiochem, CA, USA) together with the purified enzyme were used as a negative control for each experiment. NE activity was calculated for 106 neutrophils.
Myeloperoxidase enzymatic activity
105 neutrophils were lysed in 0.2% Triton X-100 solution and incubated with 0.1 mg/ml O-phenylenediamine (Sigma-Aldrich, MO, USA) and 1 mM H2O2 (Sigma-Aldrich) for 20 min at room temperature. Enzymatic activity was measured by an iMark Microplate Absorbance Reader (Bio-Rad, CA, USA) at 450 nm. A calibration curve was set up by using various amounts of purified MPO (Athens Research & Technology, GA, USA). Purified MPO was used as a positive control, and 4-aminobenzoic acid hydrazide (Cayman Chemicals, MI, USA), a specific MPO inhibitor, together with the purified enzyme were used as a negative control for each experiment. MPO activity was calculated for 106 neutrophils.
Neutrophil activation and immunofluorescent staining
Neutrophils were seeded on coverslips coated with poly-L-lysine and activated by 100 nM PMA for 3 h at 37 °C. Subsequently, cells were fixed using a 4% paraformaldehyde solution. Neutrophils were labeled with Sytox Green (Thermo Fischer Scientific, MA, USA) and Hoechst 33,342 (Sigma-Aldrich, MO, USA). Imaging was performed on an LSM700 Laser Scanning Confocal Fluorescence microscope (Zeiss). In each sample, 3 regions of interest containing 100–200 cells were evaluated for NETs formation manually. Non-NETting neutrophils were defined as those with compact DNA stained with both nuclear dyes. NETing neutrophils were defined as those having diffuse DNA stained only with Sytox green.
Statistical analysis
GraphPad Prism version 5 (GraphPad Software Inc., CA, USA) was used for statistical analysis. Student t-test or one-way ANOVA test with Bonferroni post hoc test was used to calculate differences. Statistical tests for comparison were two-tailed, and *P < 0.05 was considered significant. The data are presented as mean ± standard error of mean.
Results
Patients demographics and clinical characteristics
Seven patients who fulfilled the inclusion criteria were included in the analysis, with a median age of 3 years (range 2–14) and 71% female. 57% of the patients were diagnosed with oligo JIA (n = 4) and 43% of the patients with poly JIA (n = 3, Table 1). All oligo JIA patients in the cohort were females, with a median age of 4.5 years old (range 3–11). The poly JIA group included 2 males and 1 female, with a median age of 3 years old (range 2–14). In addition, a total of 6 healthy controls were recruited, with a median age of 7.5 years (range 1–16) all male. All patients but one patient with oligo JIA tested positive for ANA with immunofluorescence (IF). Intra-articular steroid injection (IASI) with triamcinolone hexacetonide (THA) was the first-line treatment for all patients in the cohort, given at the time of diagnosis, with a steroid dose of 1 mg/kg of knees, 0.5 mg/kg for other large joints and 0.3 mg/kg for small joints as accepted. Two of the 3 poly JIA patients were initially treated with systemic methotrexate (MTX) in addition to the intra-articular steroid injections. The median time from the time of disease diagnosis (i.e., first intra-articular steroid injection; sample 1) to the first follow-up after the intra-articular joint injection with steroids (sample 2) was 83 days (ranging 70–124). Further clinical and laboratory characteristics at the time of diagnosis and at the first follow-up after the steroid injections are described in Table 2, including the number of active joints, CRP, cJADAS10, NETs, NE, and MPO (Table 2).
Correlation between NETs formation and disease activity score is statistically significant in oligo JIA patients
In the oligo JIA patients, all the clinical and laboratory parameters decreased following intra-articular steroid injection (Fig. 1A–I). However, only PhGA, cJADAS-10, and JADAS-10 exhibited a statistically significant decline (Fig. 1C, E, F). NE activity (Fig. 2A) and NETs formation (Fig. 2C, D–F) were increased in oligo JIA patients at the time of diagnosis (oJIA-D) compared to the healthy controls (HC). However, only the elevation of NETs formation was statistically significant. Following intra-articular steroid injection, NE activity (Fig. 2A) and NETs formation (Fig. 2C) both showed a decrease. NE activity reduced from 10.4 mU ± 2.8 to 8.2 mU ± 2.8, while NETs formation declined from 68.9% ± 13.4% to 39.4% ± 7.0%, a comparable level to that of the healthy controls, whose NETs formation was 36.7% ± 3.7% (P = 0.72). Furthermore, NETs formation exhibited a statistically significant linear correlation with cJADAS-10 (p = 0.007) (Fig. 2I). There was no statistically significant correlation between NE, MPO activity, and cJADAS (Fig. 2G and H). Additionally, we calculated the correlation of all clinical and laboratory parameters with NETs formation and found a statistically significant correlation with PGA, PhGA, and JADAS10-CRP (Table 3).

Oligoarticular JIA patient characteristics at diagnosis and first follow-up after treatment. Clinical and laboratory parameters and calculated disease activity scores at diagnosis and following steroid injection of 4 oligo JIA patients. A Number of active joints, B PGA, C PhGA, D CRP, E cJADAS10, F JADAS10-CRP; cell counts of G white blood cells, H neutrophils, I lymphocytes. PhGA, cJADAS10, and JADAS10-CRP significantly decreased after treatment compared to diagnosis (*P < 0.05, **P < 0.01)

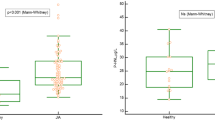
Neutrophil granular enzyme activities and NETs formation among oligo JIA patients. A NE activity, B MPO activity, and C percentage of NETs formation of oligo JIA patients (N = 4) compared to pediatric healthy controls (HC) (N = 6). NE activity and NETs were increased compared to healthy controls at diagnosis and decreased after anti-inflammatory treatment, only the difference between HC and oJIA at diagnosis was statistically significant. Representative immunofluorescent staining demonstrating NETs formation of D healthy control; E oligo JIA patient at diagnosis; F oligo JIA patient after anti-inflammatory treatment. Oligo JIA patients at diagnosis exhibit a significant increase in NETs formation in comparison to healthy control. Following anti-inflammatory treatment NETs formation in oligo JIA patients decreased. White arrows represent NETing neutrophils. G NE activity and H MPO activity showed no correlation with cJADAS. I NETs formation exhibited a statistically significant linear correlation with cJADAS10 (**P = 0.007)
NETs formation does not correlate with disease activity score in polyarticular JIA patients
In the poly JIA patients, all the clinical parameters including the number of active joints, PGA, PhGA, and CRP values showed a minor, non-significant decrease following anti-inflammatory treatment initiation (Fig. 3A–F). White blood cell counts did not change (Fig. 3G–I). NE activity (Fig. 4A) and NETs formation were measured at the same level in poly JIA patients as in the healthy controls at the time of diagnosis and have increased after treatment (Fig. 4C, D–F). MPO activity showed a lower level compared to healthy controls at diagnosis and has mildly reduced after treatment (Fig. 4B). Neither of the neutrophil-related parameters exhibited a correlation with clinical disease activity score cJADAS-10 (Fig. 4G–I). Furthermore, none of the other clinical characteristics showed a correlation with NETs formation (Table 4).

Polyarticular JIA patient characteristics at diagnosis and following treatment. Clinical and laboratory parameters and calculated disease activity scores at diagnosis and following steroid injection of 3 poly JIA patients. A Number of active joints, B PGA, C PhGA, D CRP, E cJADAS10, F JADAS10-CRP, cell counts of G white blood cells, H neutrophils, and I lymphocytes. None of the clinical and laboratory parameters changed significantly following treatment

Neutrophil granular enzyme activities and NETs formation among poly JIA patients. A NE activity, B MPO activity, and C percentage of NETs formation of poly JIA patients (N = 3) compared to pediatric healthy controls (HC) (N = 6). NE activity and NETs were similar to HC at diagnosis and increased after anti-inflammatory treatment. MPO activity was decreased in JIA patients at diagnosis in comparison to HC and did not significantly change following treatment. All of the described parameters did not change significantly between the groups. Representative immunofluorescent staining demonstrating NETs formation of D healthy control; E poly JIA patient at diagnosis; and F poly JIA patient after anti-inflammatory treatment. Poly JIA patient at diagnosis exhibits similar NETs formation as healthy control. Following anti-inflammatory treatment, NETs formation in the poly JIA patient increased. White arrows represent NETing neutrophils. None of the parameters including G NE activity, H MPO activity, and I NETs formation exhibited a correlation with cJADAS
Influence of clinical characteristics on NETs formation and NE activity
We performed further analysis on the entire cohort at diagnosis as one group to gain more information concerning the influencing factors on NETs and NE activity and to evaluate the feasibility as biomarkers. Due to the sample size of the patient population, which is a limiting factor, a bivariate analysis in the form of linear regression was performed between NETs formation and NE activity and clinical characteristics including sex, age at JIA onset, ANA positivity, and number of active joints (Table 5 and Fig. 5). No significant correlation was shown, likely due to the low sample size. The best correlations were found between NETs release and the number of active joints with R2 = 0.518 and P = 0.11 (Fig. 5A) as well as NE activity with the age at JIA onset and number of active joints (R2 = 0.159 and 0.163 respectively and P = 0.37 in both cases) (Fig. 5B, D).

Linear regression analysis of NETs release and NE activity with clinical characteristics of JIA patients. Red circles represent oligo JIA patients; black circles represent poly JIA patients on the graphs. Low evidence of correlation was shown with all clinical characteristics analyzed. Changes in NETs release and NE activity might be influenced by the number of clinical characteristics like the number of active joints (A, B) and age at JIA onset (C, D)
Discussion
In the last decade, neutrophils and NETs formation have received a lot of attention as their role in non-infectious conditions was revealed, including in the pathogenesis of autoimmune and inflammatory diseases [9]. JIA has long been established as an autoimmune disease, triggered by aberrant recognition of autoantigens by T-cells. However, system biology approaches investigating JIA have proposed the complex interaction between innate and adaptive immunity [27]. Moreover, recent data suggest an important role for neutrophils in JIA pathogenesis [28, 29].
In this prospective inception cohort, we explored NETs formation and the enzymatic activity of neutrophil granular enzymes NE and MPO in children with oligoarticular and polyarticular JIA in addition to standard clinical parameters including white blood cell counts, CRP levels, and disease activity scores. We also addressed the correlation of JIA disease activity scores (JADAS) with NETs formation and NE and MPO activity as potential biomarkers for JIA.
In our pilot study, we found that oligo JIA patients showed significantly increased NETs compared to healthy controls at the time of diagnosis. Moreover, neutrophil function, specifically NETs formation, correlated with the disease activity following the steroid injection. Following the treatment with intra-articular steroid injection, NETs formation showed a decreasing trend in comparison to samples at diagnosis, though not significant likely due to the small sample size (N (oligo JIA) = 4 and N (control) = 6). In the case of poly JIA patients, the NETs at time of diagnosis were not necessarily high, and no correlation was found between neutrophil function and disease activity. These differences may again relate to the small sample size of the cohort, as there is little data in the literature to support the difference that we demonstrated in the neutrophil parameters between oligo and poly JIA. However, it is possible that the pathogenesis of the two is different.
There is limited data in the literature on the role of neutrophils and their function in oligo and poly JIA. A recent study reported the presence of both phenotypically and functionally altered neutrophils in the inflamed joint in oligoarticular JIA [28]. Neutrophils in the synovial fluid were activated, had an aged phenotype, had gained monocyte-like features, and had impaired phagocytic capacity. The impairment in phagocytosis and oxidative burst was associated with the phenotype shift. Another study showed that neutrophils from synovial fluid of JIA patients display a hyperactivated phenotype [29]. Overall, the data from the literature supports neutrophil activation during the active state of JIA, though how treatments affect neutrophil function is not conclusive.
Once treating children with JIA, frequent and timely assessment of their clinical response to therapy and disease activity is crucial in a goal to receive clinically inactive disease or low disease activity. The main assessment currently used in JIA, the composite disease activity score, was developed in 2009 and was named Juvenile Arthritis Disease Activity Score (JADAS) [30]. Because inflammatory markers are not always obtained or available at a visit, and their efficacy is often debated, a three-variable version of the JADAS that does not include the acute-phase reactant, termed the clinical JADAS (cJADAS), has been proposed [31]. Though these markers help to follow up disease progression and evaluate treatment effectiveness, the components of PGA and PhGA are rather subjective. There are attempts to develop more specific laboratory biomarkers, such as serum proteins, the neutrophil activation marker S100A12, and the phagocyte activation marker myeloid-related proteins 8 and 14 heterocomplexes (MRP8/14), which were found to be more specific in predicting response to methotrexate and JIA flare than other clinical and laboratory data [32, 33]. It was also revealed that neutrophils in children with JIA are primed to release granular proteins without relation to medical treatment, whereas signs of increased turnover and sequestration of neutrophils are reduced by treatment [34]. However, none of these laboratory markers was implemented in common clinical practice and, therefore, there is a need for the search of putative biomarkers for timely assessment of JIA. In this respect, the finding that NETs formation declines after treatment, coupled with a decreased cJADAS-10 score in oligo JIA might point to a potential biomarker for disease activity.
There are several limitations to our study. Most notably, the size of the cohort is smaller than expected, mainly due to the exclusion of many patients who had no sample from the time of diagnosis. In addition, the method used for neutrophil isolation required fresh blood, which has limited the study to be a single-center study. However, this is a pilot report and we are aiming to increase the cohort for our future reports. In addition, blood samples were used for the study but we did not examine synovial samples, which would potentially provide another perspective to the results.
Conclusions
In conclusion, this is the first study exploring the link between NETs formation and JIA activity. We demonstrated a statistically significant linear correlation between NETs formation and cJADAS-10 in oligo but not in poly JIA patients. Hence, we suggest that NETs formation might play a role in JIA activity and may serve as a putative biomarker. This is a pilot study and more data and in-depth understanding is needed to validate these initial results.
Availability of data and materials
The authors confirm that the data supporting the findings of this study are available within the article. The raw data was generated in the Tel Aviv Sourasky Medical Center and is available on request from the corresponding author.
Abbreviations
- JIA:
-
Juvenile idiopathic arthritis
- Oligo:
-
Oligoarticular
- Poly:
-
Polyarticular
- ANA:
-
Anti-nuclear antibody
- RF:
-
Rheumatoid factor
- NETs:
-
Neutrophil extracellular traps
- NE:
-
Neutrophil elastase
- MPO:
-
Myeloperoxidase
- SLE:
-
Systemic lupus erythematosus
- RA:
-
Rheumatoid arthritis
- IBD:
-
Inflammatory bowel disease
- SF:
-
Synovial fluid
- ILAR:
-
International League of Associations for Rheumatology
- PhGA:
-
Physician’s global assessment
- VAS:
-
Visual analog scale
- PGA:
-
Parent/patient-reported global assessment
- WBC:
-
White blood cells
- ANC:
-
Absolute neutrophilic count
- ALC:
-
Absolute lymphocytic count
- CRP:
-
C-reactive protein
- IFA:
-
Indirect immunofluorescence assay
- Anti-CCP:
-
Anti-cyclic citrullinated peptide
- JADAS-10:
-
Juvenile Activity Disease Activity Score-10
- PBS:
-
Phosphate buffered saline
- EDTA:
-
Ethylenediamine tetra-acetic acid
- BSA:
-
Bovine serum albumin
- IASI:
-
Intra-articular steroid injection
- THA:
-
Triamcinolone hexacetonide
- MTX:
-
Methotrexate
References
Padeh S, Pinhas-Hamiel O, Zimmermann-Sloutskis D, Berkun Y. Children with oligoarticular juvenile idiopathic arthritis are at considerable risk for growth retardation. J Pediatr. 2011;159(5):832-837.e2. https://doi.org/10.1016/J.JPEDS.2011.04.012.
International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001 - PubMed. Accessed February 13, 2022. https://pubmed-ncbi-nlm-nih-gov.ezlibrary.technion.ac.il/14760812/.
Oen KG, Cheang M. Epidemiology of chronic arthritis in childhood. Semin Arthritis Rheum. 1996;26(3):575–91. https://doi.org/10.1016/S0049-0172(96)80009-6.
Gare BA, Fasth A. Epidemiology of juvenile chronic arthritis in southwestern Sweden: a 5- year prospective population study. Pediatrics. 1992;90(6):950–8. https://doi.org/10.1542/peds.90.6.950.
Epidemiology of juvenile chronic arthritis in northern Norway: a ten-year retrospective study - PubMed. Accessed February 21, 2022. https://pubmed.ncbi.nlm.nih.gov/9543575/.
Ravelli A, Varnier GC, Oliveira S, et al. Antinuclear antibody-positive patients should be grouped as a separate category in the classification of juvenile idiopathic arthritis. Arthritis Rheum. 2011;63(1):267–75. https://doi.org/10.1002/art.30076.
Ravelli A, Felici E, Magni-Manzoni S, et al. Patients with antinuclear antibody-positive juvenile idiopathic arthritis constitute a homogeneous subgroup irrespective of the course of joint disease. Arthritis Rheum. 2005;52(3):826–32. https://doi.org/10.1002/ART.20945.
Kobayashi SD, DeLeo FR. Role of neutrophils in innate immunity: a systems biology-level approach. Wiley Interdiscip Rev Syst Biol Med. 2009;1(3):309–33. https://doi.org/10.1002/WSBM.32.
Mayadas TN, Cullere X, Lowell CA. The multifaceted functions of neutrophils. Annu Rev Pathol. 2014;9:181–218. https://doi.org/10.1146/ANNUREV-PATHOL-020712-164023.
Brinkmann V, Reichard U, Goosmann C, et al. Neutrophil extracellular traps kill bacteria. Science. 2004;303(5663):1532–5. https://doi.org/10.1126/SCIENCE.1092385.
Sollberger G, Tilley DO, Zychlinsky A. Neutrophil extracellular traps: the biology of chromatin externalization. Dev Cell. 2018;44(5):542–53. https://doi.org/10.1016/J.DEVCEL.2018.01.019.
Jorch SK, Kubes P. An emerging role for neutrophil extracellular traps in noninfectious disease. Nat Med. 2017;23(3):279–87. https://doi.org/10.1038/NM.4294.
O’neil LJ, Kaplan MJ, Carmona-Rivera C. The role of neutrophils and neutrophil extracellular traps in vascular damage in systemic lupus erythematosus. J Clin Med. 2019;8(9):1325. https://doi.org/10.3390/JCM8091325.
Villanueva E, Yalavarthi S, Berthier CC, et al. Netting neutrophils induce endothelial damage, infiltrate tissues, and expose immunostimulatory molecules in systemic lupus erythematosus. J Immunol. 2011;187(1):538–52. https://doi.org/10.4049/JIMMUNOL.1100450.
Garcia-Romo GS, Caielli S, Vega B, et al. Netting neutrophils are major inducers of type I IFN production in pediatric systemic lupus erythematosus. Sci Transl Med. 2011;3(73). https://doi.org/10.1126/SCITRANSLMED.3001201/SUPPL_FILE/3-73RA20_SM.PDF.
Khandpur R, Carmona-Rivera C, Vivekanandan-Giri A, et al. NETs are a source of citrullinated autoantigens and stimulate inflammatory responses in rheumatoid arthritis. Sci Transl Med. 2013;5(178):178ra40-178ra40. https://doi.org/10.1126/scitranslmed.3005580.
Bach M, Moon J, Moore R, Pan T, Nelson JL, Lood C. A Neutrophil Activation Biomarker Panel in Prognosis and Monitoring of Patients with Rheumatoid Arthritis. Arthritis Rheumatology. Published online July 28, 2019:art.41062. https://doi.org/10.1002/art.41062.
Hattanda F, Nakazawa D, Watanabe-Kusunoki K, et al. The presence of anti-neutrophil extracellular trap antibody in patients with microscopic polyangiitis. Rheumatology. 2019;58(7):1293–8. https://doi.org/10.1093/rheumatology/kez089.
Söderberg D, Segelmark M. Neutrophil extracellular traps in ANCA-Associated vasculitis. Front Immunol. 2016;7:256. https://doi.org/10.3389/fimmu.2016.00256.
Drury B, Hardisty G, Gray RD, Ho GT. Neutrophil extracellular traps in inflammatory bowel disease: pathogenic mechanisms and clinical translation. Cell Mol Gastroenterol Hepatol. 2021;12(1):321–33. https://doi.org/10.1016/J.JCMGH.2021.03.002.
Giaglis S, Hahn S, Hasler P. “The net outcome”: are neutrophil extracellular traps of any relevance to the pathophysiology of autoimmune disorders in childhood?. Front Pediatr. 2016;4(SEP). https://doi.org/10.3389/FPED.2016.00097.
Duvvuri B, Pachman LM, Morgan G, et al. Neutrophil Extracellular Traps in Tissue and Periphery in Juvenile Dermatomyositis. Arthritis Rheum. Published online August 12, 2019:art.41078. https://doi.org/10.1002/art.41078.
Foell D, Wittkowski H, Hammerschmidt I, et al. Monitoring neutrophil activation in juvenile rheumatoid arthritis by S100A12 serum concentrations. Arthritis Rheum. 2004;50(4):1286–95. https://doi.org/10.1002/art.20125.
Foell D, Roth J. Proinflammatory S100 proteins in arthritis and autoimmune disease. Arthritis Rheum. 2004;50(12):3762–71. https://doi.org/10.1002/ART.20631.
Parackova Z, Zentsova I, Malcova H, Cebecauerova D, Sediva A, Horvath R. Increased histone citrullination in juvenile idiopathic arthritis. Front Med (Lausanne). 2022;9:971121. https://doi.org/10.3389/FMED.2022.971121.
Consolaro A, Giancane G, Schiappapietra B, et al. Clinical outcome measures in juvenile idiopathic arthritis. Pediatr Rheumatol Online J. 2016;14(1):23. https://doi.org/10.1186/S12969-016-0085-5.
Jarvis JN, Jiang K, Petty HR, Centola M. Neutrophils: the forgotten cell in JIA disease pathogenesis. Pediatr Rheumatol Online J. 2007;5:13. https://doi.org/10.1186/1546-0096-5-13.
Arve-Butler S, Schmidt T, Mossberg A, et al. Synovial fluid neutrophils in oligoarticular juvenile idiopathic arthritis have an altered phenotype and impaired effector functions. Arthritis Res Ther. 2021;23(1):109. https://doi.org/10.1186/S13075-021-02483-1.
Metzemaekers M, Malengier-Devlies B, Yu K, et al. Synovial fluid neutrophils from patients with juvenile idiopathic arthritis display a hyperactivated phenotype. Arthritis Rheumatol. 2021;73(5):875–84. https://doi.org/10.1002/ART.41605.
Consolaro A, Ruperto N, Bazso A, et al. Development and validation of a composite disease activity score for juvenile idiopathic arthritis. Arthritis Rheum. 2009;61(5):658–66. https://doi.org/10.1002/ART.24516.
Consolaro A, Negro G, Chiara Gallo M, et al. Defining criteria for disease activity states in nonsystemic juvenile idiopathic arthritis based on a three-variable juvenile arthritis disease activity score. Arthritis Care Res (Hoboken). 2014;66(11):1703–9. https://doi.org/10.1002/ACR.22393.
Gerss J, Roth J, Holzinger D, et al. Phagocyte-specific S100 proteins and high-sensitivity C reactive protein as biomarkers for a risk-adapted treatment to maintain remission in juvenile idiopathic arthritis: a comparative study. Ann Rheum Dis. 2012;71(12):1991–7. https://doi.org/10.1136/annrheumdis-2012-201329.
Moncrieffe H, Ursu S, Holzinger D, et al. A subgroup of juvenile idiopathic arthritis patients who respond well to methotrexate are identified by the serum biomarker MRP8/14 protein. Rheumatology (Oxford). 2013;52(8):1467–76. https://doi.org/10.1093/rheumatology/ket152.
Backlund M, Venge P, Berntson L. A cross-sectional cohort study of the activity and turnover of neutrophil granulocytes in juvenile idiopathic arthritis. Pediatr Rheumatol Online J. 2021;19(1):102. https://doi.org/10.1186/S12969-021-00600-7.
Acknowledgements
We would like to thank Dr. Pamela Weiss for critically reviewing the manuscript. This study was partially funded by the Kahn Foundation Orion Program for physician scientist for YB.
Funding
This research was partially funded by the Kahn Foundation for Yoav Binenbaum as a recipient of the Orion Grant for physician scientist in the Tel Aviv Medical Center. The funding body had no role in the study design, data collection, analysis, and interpretation of the data or writing of the manuscript.
Author information
Authors and Affiliations
Contributions
MHB, YB, SB, and RE conceived and designed the work. MHB and YBS enrolled patients and SB, AS, and VF performed the experiment. SB performed the statistical analysis. MHB, SB, GS, RS, YB, and RE wrote the manuscript. All authors contributed to the article, critically revised the manuscript, and approved the submitted version. All contributors to this study are listed as co-authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study involving human participants was reviewed and approved by Institutional Review Board, Sourasky Medical Center Tel Aviv, 0502–19-TLV. All participants’ parents provided their written informed consent to participate in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Heshin-Bekenstein, M., Baron, S., Schulert, G. et al. Neutrophils extracellular traps formation may serve as a biomarker for disease activity in oligoarticular juvenile idiopathic arthritis: a pilot study. Arthritis Res Ther 25, 135 (2023). https://doi.org/10.1186/s13075-023-03104-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13075-023-03104-9