
Abstract
Background
Patients with systemic lupus erythematosus (SLE) have substantial unmet medical need. Baricitinib is a Janus kinase (JAK)1 and 2 inhibitor that was shown to have therapeutic benefit in patients with SLE in a phase II clinical trial. The purpose of this study was to evaluate the median change from baseline in conventional serologic biomarkers in subgroups and the overall population of baricitinib-treated patients with SLE, and the SLE Responder Index-4 (SRI-4) response by normalization of anti-dsDNA.
Methods
Data were assessed from the phase II trial I4V-MC-JAHH (NCT02708095). The median change from baseline in anti-dsDNA, IgG, and other conventional serologic markers was evaluated over time in patients who had elevated levels of markers at baseline, and in all patients for IgG. Median change from baseline for baricitinib treatments were compared with placebo. Among patients who were anti-dsDNA positive at baseline, SRI-4 responder rate was compared for those who stayed positive or achieved normal levels by week 24.
Results
Significant decreases of anti-dsDNA antibodies were observed in response to baricitinib 2 mg and 4 mg compared to placebo beginning at weeks 2 (baricitinib 2 mg = − 14.3 IU/mL, placebo = 0.1 IU/mL) and 4 (baricitinib 4 mg = − 17.9 IU/mL, placebo = 0.02 IU/mL), respectively, continuing through week 24 (baricitinib 2 mg = − 29.6 IU/mL, baricitinib 4 mg = − 15.1 IU/mL, placebo=3.0 IU/mL). Significant reductions from baseline of IgG levels were found for baricitinib 4 mg-treated patients compared to placebo at weeks 12 (baricitinib 4 mg = − 0.65 g/L, placebo = 0.09 g/L) and 24 (baricitinib 4 mg = − 0.60 g/L, placebo = − 0.04 g/L). For patients who were anti-dsDNA positive at baseline, no relationship between achieving SRI-4 responder and normalization of anti-dsDNA was observed by week 24.
Conclusions
Baricitinib treatment resulted in a rapid and sustained significant decrease in anti-dsDNA antibodies compared to placebo among those with positive anti-dsDNA antibodies at baseline, as well as a significant decrease in IgG levels in the 4 mg group at weeks 12 and 24. These data suggest that baricitinib may influence B cell activity in SLE. Further studies are needed to evaluate if reductions in anti-dsDNA levels with baricitinib treatment reflect the impact of baricitinib on B cell activity.
Trial registration
Similar content being viewed by others


Background
Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by systemic inflammation, the excessive production of autoantibodies directed at self-antigens, and widespread immune dysregulation [1]. There is evidence that abnormalities in both the innate and adaptive arms of the immune system contribute to disease pathogenesis through a positive feedforward loop, consistent with interferon (IFN) effects [2]. A range of cytokines have been implicated in the etiology of SLE, such as IFNs, B cell activating factor, interleukin (IL)-6, IL-12, IL-17, IL-23, and tumor necrosis factor (TNF) [2, 3]. Dysregulations in cytokine signaling, B cell transcription factors, and B cell-T cell interactions can lead to both the generation of autoreactive B cells and autoantibody production associated with the pathogenesis of SLE [4].
Systemic lupus erythematosus is often characterized by high serological activity, including antibodies against double-stranded DNA (anti-dsDNA). The presence of antibodies that bind to dsDNA have been suggested to contribute to multiple end-organ injuries in SLE [5]. Levels of anti-dsDNA fluctuate with changes in disease activity and, in combination with reduced levels of complement component (C)3 and C4 proteins, are strong indicators of disease flare in patients with SLE [6]. Anti-dsDNA antibodies accompanied by biopsy-proven lupus nephritis (LN) was considered earlier as an independent classification criterion [7] and are also part of the EULAR/ACR 2019 classification for SLE [8, 9] illustrating their key relevance.
The Janus kinase (JAK) family of intracellular, non-receptor tyrosine kinases are important signal transducers associated with many of the key cytokines implicated in immune dysregulation in SLE [1, 10]. Cytokines bind to receptors on the cell membrane and induce phosphorylation of JAKs, and JAKS in turn phosphorylate signal transducer and activator of transcription (STAT) proteins. Phosphorylated STAT proteins then dissociate from the receptor and translocate to the nucleus where they bind to the cytokine response element to activate transcription of specific target genes [11, 12]. Baricitinib is an orally administered, selective, and reversible JAK1/JAK2 inhibitor [13] that has been approved for the treatment of moderate-to-severe active rheumatoid arthritis in adults in over 75 countries including the USA, Japan, and countries in the European Union. Through JAK1/JAK2 inhibition, baricitinib may impact the release of proinflammatory cytokines, such as type I IFNs, IFN-γ, IL-6, IL-12, and IL-23 [10, 14].
In a phase II study of baricitinib in patients with SLE, daily oral baricitinib 4 mg (in addition to standard of care therapy) was superior to placebo with standard of care in improving SLE disease activity at week 24 [14]. However, no significant improvements in least squares (LS) mean change from baseline were observed in the overall population in levels of conventional serologic biomarkers (such as anti-dsDNA antibodies, C3, or C4) for SLE with baricitinib treatment.
The objectives of this analysis were to evaluate the median change from baseline in conventional serologic biomarkers in subgroups (defined in table 1) and in the overall population of baricitinib-treated patients with SLE and to evaluate the SLE Responder Index (SRI-4) response by normalization of anti-dsDNA.
Methods
Trial design
Patient samples were obtained from the double-blind, multicenter, randomized, placebo-controlled, 24-week phase II clinical trial, I4V-MC-JAHH (NCT02708095) [14]. Eligible patients were aged 18 years or older and had a diagnosis of SLE. At baseline, patients were required to have a positive antinuclear antibody or a positive anti-dsDNA, arthritis, or rash (as defined by Systemic Lupus Erythematosus Disease Activity Index-2000 [SLEDAI-2K]) and a clinical SLEDAI-2K score of 4 or greater. Study drug was added to existing stable background standard of care therapy, which could include glucocorticoids up to 20 mg/day of prednisone or equivalent, a single antimalarial, a single immunosuppressant, and/or non-steroidal anti-inflammatory drugs. Tapering of prednisone or equivalent was permitted from baseline to week 16. Active central nervous system lupus or active severe LN was not permitted.
This study was done in accordance with the ethical principles of the Declaration of Helsinki and Good Clinical Practice guidelines. All investigation sites received approval from the appropriate authorized institutional review board or ethics committee. All patients provided written consent before the study-related procedures were done.
Randomization and masking
Patients were allocated (1:1:1) using a computer-generated random sequence to baricitinib 2 mg, baricitinib 4 mg, or placebo. Patients were stratified according to disease activity (SLEDAI-2K score <10 or ≥10), anti-dsDNA status (positive or negative), and region (United States of America [USA], Europe, Asia, or rest of the world). Investigators and patients were masked to allocation.
Outcomes
Autoantibody expression analysis
Serum samples were analyzed for changes from baseline over time for anti-dsDNA, anti-Smith (Sm), immunoglobulin (Ig)G, and anti-cardiolipin (aCL) antibodies IgM, IgG, and IgA, using INOVA QUANTA Lite SC ELISA® (INOVA Diagnostics, San Diego, CA, USA); and changes from baseline over time for antinuclear ribonucleoprotein (anti-RNP), anti-Sjögren’s syndrome-related (SS) antigen A, and anti-SS antigen B using Semi-Quantitative Multiplex Bead Assay; FIDISTM (TheraDiag, Paris, France). Changes from baseline over time for complement C3 and C4 were analyzed using the Siemens BNII Nephelometer TM (Siemens Healthcare Diagnostics, Marburg, Germany). A complete description of baseline requirements and the analysis populations are available in Table 1.
Systemic lupus erythematosus responder rate analysis
Among patients who were anti-dsDNA positive at baseline, SRI-4 responder rate was compared for those who stayed positive or achieved normal levels (<30 IU/mL) by week 24. The SRI-4 response was defined as a reduction of ≥4 points from baseline in SLEDAI-2K score, no new British Isles Lupus Assessment Group (BILAG) A and ≤1 new BILAG B disease activity scores, and no worsening (defined as an increase of ≥0.3 points (10 mm) from baseline) in the Physician’s Global Assessment of Disease Activity.
Patient and public involvement statement
Patients were not involved in the research process.
Statistical analyses
Median changes from baseline for baricitinib 2 mg and baricitinib 4 mg were compared with placebo using a Wilcoxon rank-sum test. In addition, for anti-dsDNA LS mean changes from baseline for baricitinib 2 mg and 4 mg were compared to placebo using mixed-effects model of repeated measures with baseline, region, baseline disease activity (SLEDAI-2K<10 and SLEDAI-2K ≥10), treatment, and treatment-time interaction as variables. Due to the skewness of the laboratory data distribution, evaluating the median change from baseline was more appropriate than the LS mean change from baseline, as the median value is more reflective of the true data. Autoantibody subpopulations used for analysis were based on baseline cut-offs (Table 1). Changes in lab measurements were computed using data from all patients still enrolled in the study at the corresponding time point. For categorical clinical outcomes, such as SRI-4, missing data were imputed using non-responder imputation, and differences between groups were assessed with Fisher’s exact test.
Results
Baseline characteristics and disease activity
Most patients were female with a mean age of 43–45 years with a disease duration of 10–12 years (Table 2). Patients randomized into all three treatment arms had comparable anti-dsDNA, IgG, C3, and C4 at baseline (Table 2).
Median and LS mean change from baseline in anti-dsDNA
In the subgroup of patients with increased anti-dsDNA at baseline, significant decreases in median anti-dsDNA antibody levels were observed for baricitinib 2 mg and baricitinib 4 mg compared with placebo beginning at week 2 (baricitinib 2 mg = − 14.3 IU/mL, placebo = 0.1 IU/mL, p = 0.028) and week 4 (baricitinib 4 mg = − 17.9 IU/mL, placebo = 0.2 IU/mL, p = 0.003) respectively. These decreases were sustained through week 24 (baricitinib 2 mg = − 29.6 IU/mL, baricitinib 4 mg = − 15.1 IU/mL, placebo = 3.0 IU/mL) (Fig. 1a). In the same subgroup, no significant changes were reported in LS mean anti-dsDNA antibody levels in response to baricitinib 2 mg or baricitinib 4 mg compared to placebo at any time point measured (Fig. 1b).

Median (a) and LS mean (b) change from baseline in anti-dsDNA (IU/mL). Data were assessed for significance in patients who were anti-dsDNA positive (≥30 IU/mL) at baseline. *p ≤0.05, **p≤0.01, ***p≤0.001 for BARI vs PBO. BARI, baricitinib; LS mean, least squares mean; PBO, placebo; dsDNA, double-stranded deoxyribonucleic acid
Median change in conventional serologic markers
In the intent-to-treat population, treatment with baricitinib 4 mg resulted in a significant decrease in the median IgG levels compared to placebo from week 12 (baricitinib 4 mg = − 0.65 g/L, placebo = 0.09 g/L, p = 0.004, Fig. 2a) through week 24 (baricitinib 4 mg = − 0.60 g/L, placebo = − 0.04 g/L, p = 0.003, Fig. 2a). A numerical decrease was also observed in response to baricitinib 2 mg.

Median change from baseline in IgG (a), anti-Smith (b), and anti-cardiolipin IgM (c). A Data were assessed for significance in all patients. B Data were assessed for significance in patients with anti-Smith ≥30 IU/mL. C Data were assessed for significance in patients with anti-cardiolipin IgM>12 MPL at baseline. *p ≤ 0.05, **p ≤ 0.01 for BARI vs. PBO. BARI, baricitinib; Ig, immunoglobulin; PBO, placebo; MPL, IgM phospholipid units
In the subgroup of patients with increased anti-Sm at baseline, median anti-Sm levels were numerically decreased in response to baricitinib 4 mg at week 12 compared to placebo (baricitinib 4 mg = − 33.0 IU/mL, placebo = 7.0 IU/mL, Fig. 2b) and a significant difference was reported at week 24 (baricitinib 4 mg = − 63.0 IU/mL, placebo = 22.0 IU/mL, p = 0.017, Fig. 2b). Baricitinib 2 mg did not influence anti-Sm levels compared to placebo.
In the subgroup of patients with increased aCL IgM at baseline, median aCL IgM was significantly decreased by baricitinib 2 mg (− 1.0 U/mL, p = 0.034) and 4 mg (− 2.0 U/mL, p = 0.007) compared to placebo (1.0 U/mL) at week 12 (Fig. 2c). At week 24, baricitinib 4 mg (− 2.50 U/mL) treatment resulted in a sustained statistically significant reduction compared to placebo (2.0 U/mL, p = 0.011, Fig. 2c).
Median change from baseline in other autoantibodies
In the defined subgroups, no significant changes in median values from baseline were observed in aCL IgG, aCL IgA, anti-RNP, or anti-SSA and anti-SSB with baricitinib 2 mg or 4 mg treatment at any timepoint up to week 24 (supplementary material, Fig. S2).
Median change in C3 and C4
In the defined subgroups, no significant differences in median change of C3 and C4 from baseline were observed for baricitinib 2 mg or baricitinib 4 mg treatment at any time point up to week 24 (Fig. 3).

Median change from baseline in C3 (a) and C4 (b). Data were assessed for significance in patients with C3<90 mg/dL, or C4<10 mg/dL at baseline. BARI, baricitinib; C, component; PBO, placebo
Normalization of anti-dsDNA levels and SRI-4 response
The SRI-4 response rate was assessed between patients who remained anti-dsDNA positive post-baseline, and those who achieved normal anti-dsDNA levels. There was no statistically significant difference in SRI-4 responder rate between those who stayed positive, defined as patients with ≥30 IU/mL (N = 143), or those who achieved normalization, defined as patients with <30 IU/mL (N = 17), at any timepoint up to week 24, irrespective of treatment with baricitinib 2 mg, 4 mg, or placebo (Fig. 4).

Normalization (defined by a reduction of anti-dsDNA levels to <30 IU/mL) of anti-dsDNA levels and SRI-4 response. Data were assessed for significance for all patients with anti-dsDNA ≥30 IU/mL at baseline, irrespective of treatment assignment. dsDNA, double-stranded deoxyribonucleic acid; N, number of patients; SLE, systemic lupus erythematosus SRI-4, SLE Responder Index-4
Discussion
The goal of this study was to evaluate the effects of the JAK1/JAK2 inhibitor baricitinib on the median change from baseline in conventional serologic biomarkers in subgroups and the overall population of SLE patients and the SRI-4 response by normalization of anti-dsDNA in a phase II trial.
There are several limitations to the conclusions that can be drawn from this study. While the results support the use of baricitinib in the treatment of SLE, the short timeframe of 24 weeks limits the ability to assess longer-term outcomes. In addition, the small size of the study cohort in this phase II trial is a limiting factor when interpreting the analysis. Data from two larger phase III trials (NCT03616912 and NCT03616964) will further delineate the current findings.
Treatment with baricitinib resulted in a rapid and sustained, statistically significant decrease in anti-dsDNA antibodies compared with placebo in SLE patients positive for anti-dsDNA antibodies at baseline. Treatment with baricitinib 4 mg also resulted in a statistically significant decrease in IgG and aCL IgM levels at weeks 12 and 24 and anti-Sm at week 24 compared with placebo. Increased anti-Sm levels are associated with several clinical symptoms of SLE such as renal, neurologic, and hematologic manifestations [15]. The decrease in anti-Sm seen in this study could represent reduced disease activity but may also reflect decreased immunoglobulin levels. There was no measurable relationship between SRI-4 response rate and anti-dsDNA levels, irrespective of treatment with baricitinib or placebo. This may be due to the limited sample size of the study or may indicate that there is no relationship between anti-dsDNA levels and SRI-4 response rates.
Cytokines such as IL-6, IL-10, IL-12, and IFNs play critical roles in B cell hyperactivity and differentiation, autoantibody production, and the immunopathology of SLE [16,17,18,19]. IL-6, IL-10, and IFNs have been shown to positively correlate with measures of disease activity, such as SLEDAI, and with autoantibody levels in SLE [16, 18, 20,21,22,23]. Recently, microarray analysis on serum samples from this study cohort found that baricitinib 4 mg decreased IL-12p40 and IL-6 (known as a potent stimulator of B cells) at week 12 [24]. Thus, through its inhibition of JAK1/JAK2 signaling, baricitinib may exert downstream effects on B cell activity, thereby mediating its effect on clinical symptoms in SLE [14, 25,26,27].
In the defined patient subgroups, baricitinib treatment combined with standard of care led to significant reductions in autoantibodies including anti-dsDNA, as well as IgG levels. These observed reductions are probably indicative of reduced B cell activity with baricitinib treatment. What is less clear is if this translates into a therapeutic effect or if this is simply an epiphenomenon due to reduced antibody production, as evidenced by decreasing IgG levels.
The titer of anti-dsDNA antibodies is a clinically useful tool to measure disease activity and predict flares in patients with SLE. Anti-dsDNA antibodies can be positive for at least 2 years before a diagnosis of SLE, and an increase in serum levels of anti-dsDNA antibodies is a predictor of symptom flares in patients with SLE [28]. In LN, anti-dsDNA antibodies form immune complexes through interaction with renal antigens and are present in nearly 80% of patients with LN [29]. Stimulating human mesangial cells with anti-dsDNA antibodies promotes the production of proinflammatory cytokines, such as TNF, IL-1β, and IL-6 [30, 31].
Anti-dsDNA can also contribute to LN severity through upregulation of renal fibrosis. Anti-dsDNA IgG isotype can downregulate suppressor of cytokine signaling 1 and activate JAK/STAT 1 signals, which influence the expression of profibrotic genes, such as transforming growth factor beta 1, connective tissue growth factor, and platelet-derived growth factor B [32, 33].
Anti-dsDNA has also been shown to contribute to inflammation of the skin through deposition of an immune complex at the dermoepidermal junction and to contribute to neuropsychiatric complications through cross-reaction with anti-N-methyl-D-aspartate receptor (NMDAR), and NMDARs on neurons, in patients with SLE [34, 35].
In this phase II study, baricitinib 2 mg and 4 mg reduced median anti-dsDNA levels significantly compared to placebo in the subpopulation of patients with high anti-dsDNA at baseline. Given the evidence showing anti-dsDNA involvement in disease activity in SLE, reductions in anti-dsDNA levels with baricitinib treatment could potentially be therapeutic in patients with SLE, a marker of reduced disease activity or the reduction could be merely coincidental, reflecting a decreased antibody production in a non-specific manner. In this study, there was no measurable effect of decreased anti-dsDNA on SRI-4 response rates, irrespective of treatment with baricitinib or placebo. This may have been due to the limited sample size used in this study or may indicate that there is no relationship between anti-dsDNA levels and SRI-4 response rates in the population analyzed. Results presented here should be interpreted with caution, validation by subsequent studies is mandated to evaluate if reductions in anti-dsDNA levels with baricitinib treatment are coincidental or reflect the impact of baricitinib on B cell activity.
Conclusions
As part of the inhibition of cytokine signaling through JAK1 and JAK2 in patients with SLE, the mechanism of action of baricitinib may be mediated partially through the downstream inhibition of autoreactive B cell activation, as manifest by reduction in IgG and autoantibodies including anti-dsDNA.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- aCL:
-
Anti-cardiolipin
- dsDNA:
-
Double-stranded deoxynucleic acid
- anti-RNP:
-
Antinuclear ribonucleoprotein
- BILAG:
-
British Isles lupus assessment group
- C:
-
Component
- IFN:
-
Interferon
- IgG:
-
Immunoglobulin
- IL:
-
Interleukin
- IU:
-
International unit
- JAK:
-
Janus kinase
- LN:
-
Lupus nephritis
- LS:
-
Least squares
- n :
-
Number of patients in a subgroup
- N :
-
Number of patients
- NMDAR:
-
N-methyl-D-aspartate receptor
- SD:
-
Standard deviation
- SLE:
-
Systemic lupus erythematosus
- SLEDAI-2K:
-
SLE Disease Activity Index-2000
- Sm:
-
Smith
- SRI-4:
-
SLE Responder Index-4
- SS:
-
Sjögren’s syndrome-related
- STAT:
-
Signal transducer and activator of transcription
- TNF:
-
Tumor necrosis factor
- USA:
-
United States of America
References
Tsokos GC, Lo MS, Costa Reis P, Sullivan KE. New insights into the immunopathogenesis of systemic lupus erythematosus. Nat Rev Rheumatol. 2016;12(12):716–30.
Wahren-Herlenius M, Dörner T. Immunopathogenic mechanisms of systemic autoimmune disease. Lancet. 2013;382(9894):819–31.
Larosa M, Zen M, Gatto M, Jesus D, Zanatta E, Iaccarino L, et al. IL-12 and IL-23/Th17 axis in systemic lupus erythematosus. Exp Biol Med (Maywood). 2019;244(1):42–51.
Yap DYH, Chan TM. B cell abnormalities in systemic lupus erythematosus and lupus nephritis-role in pathogenesis and effect of immunosuppressive treatments. Int J Mol Sci. 2019;20(24):6231.
Wang X, Xia Y. Anti-double stranded DNA antibodies: origin, pathogenicity, and targeted therapies. Front Immunol. 2019;10:1667.
Giles BM, Boackle SA. Linking complement and anti-dsDNA antibodies in the pathogenesis of systemic lupus erythematosus. Immunol Res. 2013;55(1-3):10–21.
Petri M, Orbai AM, Alarcón GS, Gordon C, Merrill JT, Fortin PR, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012;64(8):2677–86.
Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R, et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheum. 2019;71(9):1400–12.
Johnson SR, Brinks R, Costenbader KH, Daikh D, Mosca M, Ramsey-Goldman R, et al. Performance of the 2019 EULAR/ACR classification criteria for systemic lupus erythematosus in early disease, across sexes and ethnicities. Ann Rheum Dis. 2020;79(10):1333–9.
Schwartz DM, Kanno Y, Villarino A, Ward M, Gadina M, O'Shea JJ. JAK inhibition as a therapeutic strategy for immune and inflammatory diseases. Nat Rev Drug Discov. 2017;16(12):843–62.
O'Shea JJ, Plenge R. JAK and STAT signaling molecules in immunoregulation and immune-mediated disease. Immunity. 2012;36(4):542–50.
Shuai K, Liu B. Regulation of JAK-STAT signalling in the immune system. Nat Rev Immunol. 2003;3(11):900–11.
Fridman JS, Scherle PA, Collins R, Burn TC, Li Y, Li J, et al. Selective inhibition of JAK1 and JAK2 is efficacious in rodent models of arthritis: preclinical characterization of INCB028050. J Immunol. 2010;184(9):5298–307.
Wallace DJ, Furie RA, Tanaka Y, Kalunian KC, Mosca M, Petri MA, et al. Baricitinib for systemic lupus erythematosus: a double-blind, randomised, placebo-controlled, phase 2 trial. Lancet. 2018;392(10143):222–31.
Arroyo-Ávila M, Santiago-Casas Y, McGwin G, Cantor RS, Petri M, Ramsey-Goldman R, et al. Clinical associations of anti-Smith antibodies in PROFILE: a multi-ethnic lupus cohort. Clin Rheumatol. 2015;34(7):1217–23.
Chun HY, Chung JW, Kim HA, Yun JM, Jeon JY, Ye YM, et al. Cytokine IL-6 and IL-10 as biomarkers in systemic lupus erythematosus. J Clin Immunol. 2007;27(5):461–6.
Chasset F, Arnaud L. Targeting interferons and their pathways in systemic lupus erythematosus. Autoimmun Rev. 2018;17(1):44–52.
Lopez de Padilla CM, Niewold TB. The type I interferons: basic concepts and clinical relevance in immune-mediated inflammatory diseases. Gene. 2016;576(1 Pt 1):14–21.
Bengtsson AA, Ronnblom L. Role of interferons in SLE. Best Pract Res Clin Rheumatol. 2017;31(3):415–28.
Linker-Israeli M, Deans RJ, Wallace DJ, Prehn J, Ozeri-Chen T, Klinenberg JR. Elevated levels of endogenous IL-6 in systemic lupus erythematosus. A putative role in pathogenesis. J Immunol. 1991;147(1):117–23.
Stuart RA, Littlewood AJ, Maddison PJ, Hall ND. Elevated serum interleukin-6 levels associated with active disease in systemic connective tissue disorders. Clin Exp Rheumatol. 1995;13(1):17–22.
Houssiau FA, Lefebvre C, Vanden Berghe M, Lambert M, Devogelaer JP, Renauld JC. Serum interleukin 10 titers in systemic lupus erythematosus reflect disease activity. Lupus. 1995;4(5):393–5.
Jin S, Yu C, Yu B. Changes of serum IL-6, IL-10 and TNF-α levels in patients with systemic lupus erythematosus and their clinical value. Am J Transl Res. 2021;13(4):2867–74.
Dörner T, Tanaka Y, Petri MA, Smolen JS, Wallace DJ, Dow ER, et al. Baricitinib-associated changes in global gene expression during a 24-week phase II clinical systemic lupus erythematosus trial implicates a mechanism of action through multiple immune-related pathways. Lupus Sci Med. 2020;7(1):e000424.
Kubo S, Nakayamada S, Tanaka Y. Baricitinib for the treatment of rheumatoid arthritis and systemic lupus erythematosus: a 2019 update. Expert Rev Clin Immunol. 2019;15(7):693–700.
Kubo S, Nakayamada S, Sakata K, Kitanaga Y, Ma X, Lee S, et al. Janus kinase inhibitor baricitinib modulates human innate and adaptive immune system. Front Immunol. 2018;9:1510.
Hoffman W, Lakkis FG, Chalasani G. B Cells, Antibodies, and More. Clin J Am Soc Nephrol. 2016;11(1):137–54.
Pan N, Amigues I, Lyman S, Duculan R, Aziz F, Crow MK, et al. A surge in anti-dsDNA titer predicts a severe lupus flare within six months. Lupus. 2014;23(3):293–8.
Yung S, Chan TM. Mechanisms of kidney injury in lupus nephritis - the role of anti-dsDNA antibodies. Front Immunol. 2015;6:475.
Zhang H, Zhao C, Wang S, Huang Y, Wang H, Zhao J, et al. Anti-dsDNA antibodies induce inflammation via endoplasmic reticulum stress in human mesangial cells. J Transl Med. 2015;13:178.
Yu CL, Sun KH, Tsai CY, Hsieh SC, Yu HS. Anti-dsDNA antibody up-regulates interleukin 6, but not cyclo-oxygenase, gene expression in glomerular mesangial cells: a marker of immune-mediated renal damage? Inflamm Res. 2001;50(1):12–8.
Wang P, Yang J, Tong F, Duan Z, Liu X, Xia L, et al. Anti-double-stranded DNA IgG participates in renal fibrosis through suppressing the suppressor of cytokine signaling 1 signals. Front Immunol. 2017;8:610.
Liang Y, Xu WD, Peng H, Pan HF, Ye DQ. SOCS signaling in autoimmune diseases: molecular mechanisms and therapeutic implications. Eur J Immunol. 2014;44(5):1265–75.
Dong Y, Zhang Y, Xia L, Wang P, Chen J, Xu M, et al. The deposition of anti-DNA IgG contributes to the development of cutaneous lupus erythematosus. Immunol Lett. 2017;191:1–9.
Selmi C, Barin JG, Rose NR. Current trends in autoimmunity and the nervous system. J Autoimmun. 2016;75:20–9.
Acknowledgements
We would like to thank the patients and investigators who participated in the study. Eli Lilly and Company or its representatives provided data, laboratory, and site monitoring services. Writing assistance was provided by Conor McVeigh, PhD, of Eli Lilly and Company. This work has in part been published at the following scientific conference: European League Against Rheumatism (EULAR) 2021 Annual Meeting (Dörner et al., Ann Rheum Dis, volume 80, supplement 1, year 2021, page 588) and ACR convergence 2021 (Dörner T, Van Vollenhaven R, Doria A, Jia B, Fantini D, Terres J, Silk M, de Bono S, Fischer P, Wallace D. Arthritis Rheumatol. 2021; 73 (suppl 10)).
EULAR Abstract Archive (sparx-ip.net)
Dörner T, Van Vollenhaven R, Doria A, Jia B, Fantini D, Terres J, Silk M, de Bono S, Fischer P, Wallace D. Baricitinib Decreases Anti-dsDNA and IgG Antibodies in Adults with Systemic Lupus Erythematosus from a Phase 2 Double-Blind, Randomized, Placebo-Controlled Trial [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 10). https://acrabstracts.org/abstract/baricitinib-decreases-anti-dsdna-and-igg-antibodies-in-adults-with-systemic-lupus-erythematosus-from-a-phase-2-double-blind-randomized-placebo-controlled-trial/. Accessed March 12, 2022.
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was sponsored by Eli Lilly and Company, under license from Incyte Corporation.
The funder of the study had a role in study design, data analysis, data collection, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Author information
Authors and Affiliations
Contributions
TD, RFV, AD, PF, DJW, MS, SB, and JRT contributed to the conception of the work, interpretation of the data, and critical revision of the work. BJ contributed to the data analysis, interpretation of the data, and critical revision of the work. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All studies were approved by the applicable ethical review boards at each participating study site and were conducted in accordance with the principles expressed in the Declaration of Helsinki of 1964 and its subsequent amendments. Written, informed consent was obtained from each patient at study entry before any study procedures took place.
Consent for publication
Not applicable.
Competing interests
TD has received grant support from Chugai, Janssen, Novartis, and Sanofi. He has received consultancy support from AbbVie, Celgene, Eli Lilly and Company, Janssen, Novartis, Roche, Samsung, and UCB, and speaker bureau fees from Eli Lilly and Company and Roche. RFV has received consultancy support from AbbVie, Biotest, BMS, Celgene, Crescendo, Eli Lilly and Company, GSK, Janssen, Merck, Novartis, Pfizer, Roche, UCB, and Vertex. AD has received consultancy support from GSK, Eli Lilly and Company, and Celgene and has speaker bureau fees from GSK, Pfizer, Roche, and Janssen. DJW has received consulting support from Amgen, Eli Lilly and Company, EMD Merck Serono, and Pfizer. BJ, JRT, MS, SB, and PF are employees and shareholders of Eli Lilly and Company.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
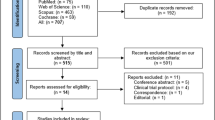
Additional file 1: Figure S1.
Trial profile participant flow chart.
Additional file 2: Figure S2.
Median change from baseline in aCL IgA, aCL IgG, anti-SSA, Anti-SSB, anti-RNP.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

{kind=link}
{kind=link}
Cite this article
Dörner, T., van Vollenhoven, R.F., Doria, A. et al. Baricitinib decreases anti-dsDNA in patients with systemic lupus erythematosus: results from a phase II double-blind, randomized, placebo-controlled trial. Arthritis Res Ther 24, 112 (2022). https://doi.org/10.1186/s13075-022-02794-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13075-022-02794-x