
Abstract
Background
Mental health is decreasing among young people in Denmark. Our primary aim is to evaluate the effectiveness of a teacher training programme to teach mindfulness as part of regular classroom teaching in Danish upper secondary schools and schools of health and social care on students’ self-reported mental well-being 6 months from baseline. Secondary aims are (1) to evaluate the effectiveness in a vulnerable subgroup as well as in the total population of students 3 and 6 months from baseline using other outcome measures on mental health and (2) to investigate the facilitators and barriers among teachers to implement mindfulness in schools.
Methods
This pragmatic cluster-randomised two-arm superiority trial includes 30 upper secondary schools, 13 schools of health and social care, 76 teachers, and approximately 1100 students aged 16 to 24 years. Our intervention is multi-level and consists of (a) a teacher training programme and (b) a mindfulness programme delivered to students. Students in control schools receive education as usual. Our primary study population is the total population of students. The primary outcome is changes in the short version of the Warwick-Edinburgh Mental Well-Being Scale (SWEMWBS). We also evaluate the effectiveness in a vulnerable subgroup (the 15% with the lowest SWEMWBS score), as well as in the total population of students 3 and 6 months from baseline using other outcome measures on mental health. Data will be analysed using repeated measurement models taking clusters into account. Facilitators and barriers among teachers to implement mindfulness in schools will be investigated through qualitative focus group interviews.
Discussion
The trial will estimate the effectiveness of a population-based strategy on mental health in Danish young people enrolled in education.
Trial registration
ClinicalTrials.gov NCT04610333. Registered on October 10 2020.
Similar content being viewed by others

Background
Mental health of children and young people is a global public health challenge [1]. The need to focus on the mental health of young people is gaining increasing recognition as the global community looks to achieve the ambitious Sustainable Developmental Goals (SDG), such as SDG 3: “Ensure healthy lives and promote well-being for all at all ages” [2]. Mental health conditions account for a considerable proportion of the global disease burden during youth and are the leading course of disability in young people [3]. In fact, 75% of mental disorders begin before the age of 24 and 50% by the age of 15 [4]. Suicide is one of the three leading causes of death among older adolescents [5]. Therefore, mental health conditions have huge costs for the individuals affected as well as for society as a whole. The total costs related to mental health problems in Europe are estimated to account for more than EUR 600 billion. Among the European countries, Denmark has the highest costs in terms of % of GDP (5.4%) [6].
However, mental health is more than the absence of mental disorders [7]. Mental health is a fundamental component of the World Health Organization’s (WHO) definition of health. It is conceptualised as a state of well-being in which the individual realises her or his own abilities, is able to cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to her or his community [8]. In this positive sense, mental health is the foundation for well-being and effective functioning for an individual and a community [7].
In Denmark, mental health among young people has been decreasing in recent years. Since 2010, the National Health Profile has reported an increase in the proportion of 16–24-year-olds with poor mental health [9]. A high occurrence of stress, anxiety, tension, and loneliness is seen in this age group as well [10].
According to WHO, mental health is a public issue that requires political priority and action. This is to ensure that effective promotion and prevention are established and that stigmatisation and discrimination are broken down [11]. Mental health promotion and disease prevention in young people can benefit young lives in the short and long term. This stage is deemed as one of the optimal timeframes for intervention, given the neuroplasticity evident in adolescence and the opportunity to step in at a time when the majority of mental health conditions and risky behaviours have their onset [5]. WHO recommends population-based psychosocial interventions to promote positive mental health and prevent mental disorders [3]. Likewise, The Lancet Commission on global mental health and sustainable development emphasise the importance of improving mental health for whole populations [12]. Population-based interventions have the highest and most valuable impact at a society level [13]. The reason for this is that most cases of poor mental health occur among the many who are at low or moderate risk, rather than among the few who are at high risk. In addition, population-based interventions have the potential to improve mental health in all young people as well as in high-risk and vulnerable groups without causing stigma [13].
School environment has been identified as an appropriate setting for providing mental health promotion and prevention. Not least because of its broad reach and central role in the lives of young people [14, 15]. O’Conner highlights the importance of providing school teachers with the necessary skills and knowledge to ensure that the school setting is a beneficial environment for promoting mental health [14]. However, there is a lack of evidence-based intervention content. Moreover, many strategies to improve mental health are designed to be used when people are unwell, and therefore lack relevance for those at low risk and for those who are at high risk, but not currently showing symptoms [16].
Since life cannot be lived without challenges and discomfort, training the ability to handle and be with these challenges in an appropriate way is necessary and beneficial for everyone. One way to train this is through the practice of mindfulness. Mindfulness is a method of mental health training that can be used by anyone, regardless of how they feel. Mindfulness has been defined as the awareness that arises from paying attention on purpose in the present moment, non-judgementally, in the service of self-understanding, wisdom, and compassion [17]. Mindfulness-based Stress Reduction (MBSR) is a well-described group-based programme in mindfulness training developed in 1979 by Jon Kabat-Zinn [18]. The programme consists of eight weekly sessions of 2 ½ hours and one all-day session. The sessions have standardised core elements consisting of different mental and psychical mindfulness exercises. Additionally, there are teachings on stress, stress management, and how to apply mindfulness to interpersonal communication and everyday situations [18]. Today, MBSR is an incorporated part of both mental health promotion, prevention, and treatment worldwide. A Campbell Systematic Review based on 101 randomised controlled trials concludes that MBSR has a moderately large positive effect on outcome measures of mental health when compared to inactive controls. The intervention also improves the quality of life, including social function, and personal development like empathy, coping, sense of coherence, and mindfulness. Compared to active controls, MBSR has an additional small positive effect on outcome measures of mental health, depression, stress, and mindfulness [19].
Given the beneficial effects established by MBSR in adults, there has been an increasing interest in implementing similar initiatives for young people. Research in this area is still preliminary, but growing. Dunning et al. conclude the positive effects of mindfulness-based interventions on mental health in children and adolescents [20]. Their meta-analysis is based on 33 randomised controlled trials. However, there is a high degree of variability in intervention contents and target groups, and the meta-analysis emphasises the importance of incorporating scaled-up trials to further evaluate the robustness of mindfulness-based interventions in youth [20].
The Danish Parliament has funded the Danish Center for Mindfulness at Aarhus University to educate upper secondary school teachers and teachers at schools of health and social care to teach mindfulness to students. The Danish Center for Mindfulness has systematically developed a version of MBSR modified for young people called “On Top of Everything”. It is built on the same overall themes and mindfulness exercises as MBSR, but the duration, number of sessions, and focus in the exercises are adapted to young people in a classroom setting.
Aims
Our primary aim is to evaluate the effectiveness of a teacher training programme to teach the mindfulness programme “On Top of Everything” as part of regular classroom teaching in Danish upper secondary schools and schools of health and social care on students’ self-reported mental well-being 6 months from baseline. Secondary aims are (1) to evaluate the effectiveness in a vulnerable subgroup as well as in the total population of students 3 and 6 months from baseline using other outcome measures on mental health and (2) to investigate the facilitators and barriers among teachers to implement mindfulness in schools.
Hypothesis
We hypnotise that young people in the intervention group will improve their mental health during the intervention. We expect to find small effect sizes in the total population of students and higher effect sizes in a vulnerable subgroup [13].
Methods/design
Design
The study is designed as a pragmatic cluster-randomised two-arm superiority trial including 30 upper secondary schools and 13 schools of health and social care across Denmark.
Setting
In Denmark, compulsory education is 10 years (0th to 9th grade). Hereafter, it is up to young people themselves to choose their further education. Two options are included in this research project: upper secondary schools and schools of health and social care. Upper secondary school is an academic youth education programme. It exists in four different forms (HTX, HHX, STX, and HF) which takes 2 to 3 years to complete. The common objective of upper secondary schools is to prepare young people for higher education (e.g. the university) [21]. School of health and social care is a vocational education. It educates social and health care assistants, social and health care workers, and pedagogical assistants over a period of 2 to 4 years. The common objective of schools of health and social care is to educate students on how to take care of people who cannot fend for themselves [22].
Eligibility criteria
We included Danish upper secondary schools and schools of health and social care with no exclusion criteria. To be able to participate, consent from headmasters/headmistresses was essential. Each participating school was allowed to include between 1 and 4 teachers for teacher training. One of the inclusion criteria for students was an age of 16 to 24 years. Students were able to opt out of the trial by not completing questionnaires.
Intervention
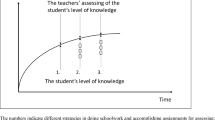
The intervention is a multi-level, multi-component complex intervention. It consists of a teacher training programme and the mindfulness programme “On Top of Everything” delivered to students. Schools were randomised to begin teacher training in 2020 (intervention group) or in 2021 (control group). The timeline for research activities and intervention content is outlined in Fig. 1 [23]. The teacher training proceeds during a period of approximately 1 year and is facilitated by two MBSR instructors from the Danish Center for Mindfulness, Aarhus University (one with a professional background as an upper secondary school teacher and one as a psychologist).

Timeline and description of the research activities and intervention contents in the project
The teacher training programme is based on three parts: First, participation in the MBSR programme, which is delivered in a combination of group-based face-to-face and live online teaching. The aim is to establish a formal mindfulness practice in the teachers. Second, completion of a 4-day residential course including training to teach the “On top of Everything” programme and access to teaching materials. Third, completion of three 2-day supervision seminars on implementation issues and relational competencies based on the work of The Danish Association for Promoting Life Wisdom in Children [24]. The teacher training programme includes information on potential adverse effects associated with mindfulness [25, 26].
The “On Top of Everything” programme consists of 10 well-described, weekly 45–60-min classroom sessions. Each session has a theme and teachers’ notes and body scan, meditation, and yoga recordings.
Public and participant involvement
Teachers and students have been involved in the development of the “On Top of Everything” intervention through pilot tests.
Outcome measures
Outcome measures are described in Table 1. Standard participant demographic information (gender, grade, and family setting) was collected at baseline. The outcome measures were collected at three time points (baseline, 3- and 6-month follow-ups). Information about mindfulness practice was collected at 3- and 6-month follow-ups in the intervention group. Our primary outcome is changes 6 months from baseline in the short version of the Warwick-Edinburgh Mental Well-Being Scale (SWEMWBS) [27] in the total population of students. A range of individual-level secondary outcome measures was chosen based on their ability to explore mental health.
Sample size
We assume a 1-point increase between-group effect in SWEMWBS to be of public health relevance [44, 45]. From another study that analysed the intervention effect on SWEMWBS in a mixed model with three repeated measurements, and where cluster levels of teacher and school were taken into account, we found a within-person SD = 2.4. To detect an effect on 1 score point in SWEMWBS change, SD = 3.5 = SQRT (2) × 2.4 with 80% power, will require 194 participants in each group, 388 participants in total.
Recruitment
We recruited upper secondary schools and schools of health and social care through emails to headmasters/headmistresses, online information meetings, and advertisements on our webpage (www.mindfulness.au.dk) and social media between May 2019 and October 2019. We informed the headmasters/headmistresses as well as interested teachers that schools would be randomised to begin teacher training in 2020 or in 2021. Furthermore, it was obligatory for each teacher to include one class with 15 to 30 students. Due to the logistics of teacher planning, it was not possible to include students before the randomisation of schools.
Randomisation
Sequence generation
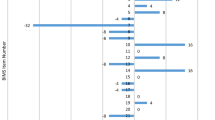
The schools were allocated into intervention or control schools in two runs: one for each type of school. Each school received a random number, and then the schools were sorted according to the number of teachers included in the project (1 or 2–4) and the random number. The schools on the list were then alternately allocated to intervention or control starting with a control. This procedure was used to try to balance the two arms according to the teachers included in the project. The allocation was performed using Microsoft Excel.
Allocation concealment mechanism
The allocation was performed by the third author, who was not involved in the recruitment, implementation, or data collection. The third author received a list of the schools with an anonymous ID concealing the true identity of the schools and whether or not each school had one or more teachers included in the project. The school were then allocated to control or intervention, as described above. After this, the third author received a list with the true identities of the schools; these were then merged onto the schools before the allocations were sent to the second author.
The characteristics of the schools are shown in Table 2.
Blinding
Neither intervention providers nor study participants were blinded.
Data collection and management
Quantitative data were collected and stored using the Research Electronic Data Capture (REDCap) tool hosted by Aarhus University [46]. The included teachers were asked to register the class recruited for the research project, to provide students (including absentees) with online access to the three questionnaires (baseline, 3- and 6-month follow-up), and to arrange a time for students to complete the questionnaires during school hours. Teachers and students received two reminders in case of non-respondence.
We informed the students about the trial and the option to opt out and not completing the questionnaires. Data collection procedures have been pilot-tested and improved several times. Reasons for teachers to opt out of the trial were registered continuously. Furthermore, we registered participation in the teacher training programme and also the teaching of the mindfulness programme. The teachers were asked to report adverse events through their teaching period. Teachers have access to supervision from psychologists and psychiatrists to ensure prevent harm and to take good care of participants who may suffer harm from trial participation.
After implementing the “On Top of Everything” programme, teachers in the intervention group were invited to participate in focus group interviews. The teachers were asked about their experience of implementing mindfulness in their schools and about which facilitators and barriers they encountered through the process.
Statistical methods
Quantitative data will be analysed according to the intention-to-treat principle using a repeated measurement model with the systematic effect: gender, age, class, time (three time points), intervention, interaction between time and intervention, and random effect of school, teacher/class within school, and student within class. Confidence intervals and standard errors will be found by bootstrapping to adjust for possible deviation from the normality of the random effects. Exploring subgroup analysis will be conducted on gender, a vulnerable subgroup (the 15% with the lowest SWEMWBS score), and type of school. To take account of missing data, we will perform four sensitivity analyses representing scenarios with data not missing at random. Missing outcomes will be substituted with the model-based prediction adding or subtracting 0.02 SD in the intervention or control arm.
Qualitative data will be transcribed and analysed based on qualitative content analysis. Each focus group interview will be read and notes will be taken, and themes will be introduced, organised, and related to quotes that are open to interpretation and that continue to an analytic investigation and connection of themes and quotes from all focus group interviews.
Significance and potential impact of the project
This trial will estimate the effectiveness of a population-based strategy on mental health in Danish young people enrolled in education. It will investigate the effectiveness of a mindfulness-based intervention based on the well-described MBSR programme modified to young people by the Danish Center for Mindfulness, Aarhus University. Furthermore, it will investigate facilitators and barriers among teachers to implement mindfulness in schools.
Trial status
In total, 43 schools and 76 teachers consented to participate in the trial (44 teachers from 30 upper secondary schools and 32 teachers from 13 schools of health and social care). Teachers have recruited approximately 1100 students. Three focus group interviews were conducted among teachers in the intervention group after the implementation of the “On Top of Everything” programme.
Teaching of the “On Top of Everything” programme among students in the intervention group took place during the spring semester of 2021. Interviews among teachers took place in June 2021. The last quantitative data (6-month follow-up) were collected among students in the autumn of 2021. We will start cleaning and analysing the data at the beginning of 2023.
Dissemination of knowledge
The results will be submitted for publication in international peer-reviewed journals. The results will also be presented at national and international conferences and scientific meetings. We also attempt to communicate the results in the press and specialist journals, and we will communicate the results at webpages, LinkedIn profiles, and social media (Facebook and Instagram).
Availability of data and materials
The dataset will be available from the second author by reasonable request after publication.
Abbreviations
- BRS:
-
Brief Resilience Scale
- DASS:
-
Depression Anxiety Stress Scale
- EQ:
-
Experiences Questionnaire
- HRQoL:
-
Health-related quality of life
- MBSR:
-
Mindfulness-based stress reduction
- PSS:
-
Perceived Stress Scale
- REDCap:
-
Research Electronic Data Capture
- SDQ:
-
Strengths and Difficulties Questionnaire
- T-ILS:
-
Three-Item Loneliness Scale
- SWEMWBS:
-
Warwick-Edinburgh Mental Well-Being Scale: the short version
- WHO:
-
World Health Organization
- WHO-5:
-
5-Item World Health Organization Well-Being Index
References
Patel V, Flisher AJ, Hetrick S, McGorry P. Mental health of young people: a global public-health challenge. Lancet. 2007;369:1302–13.
Transforming our World. The 2030 agenda for sustainable development. New York: United Nations; 2015.
World Health Organization. Guidelines on mental health promotive and preventive interventions for adolescents. Geneva: World Health Organization; 2020.
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. 2005;62(6):593–602.
World Health Organization. Global Accelerated Action for the Health of Adolescents (AA-HA!). Geneva: World Health Organization; 2017.
Health at a glance: Europe 2018. OECD. 2018.
Promoting mental health. concepts, emerging evidence, practice: summary report. Geneva: World Health Organization; 2004.
World Health Organization. Basic documents. 48th edition. Geneva: World Health Organization; 2014.
Danish Health Authority. Danes’ Health - the National Health Profile 2017. Copenhagen: Danish Health Authority; 2018.
Larsen et al. How are you? 2017 - health profile for region and municipalities (volume 2). The development 2010–2013–2017. Aarhus: DEFACTUM; 2017.
The World Health Report 2001. Mental health: new understanding, new hope. Genéve: World Health Organization; 2001.
Patel V, Saxena S, Lund C, Thornicroft G, Baingana F, Bolton P, et al. The Lancet Commission on global mental health and sustainable development. Lancet Comm. 2018;392:1553–98.
Rose G. Strategy of preventive medicine. New York. Oxford University Press; 1992.
O’Connor CA, Dyson J, Cowdell F, Watson R. Do universal school-based mental health promotion programmes improve the mental health and emotional wellbeing of young people? A literature review J Clin Nurs. 2017;27(3–4):e412–26.
Weare K, Nind M. Mental health promotion and problem prevention in schools: what does the evidence say? Health Promot Int. 2011;26(S1):29–69.
Kuyken W, Nuthall E, Byford S, Crane C, Dalgleish T, Ford T, et al. The effectiveness and cost-effectiveness of a mindfulness training programme in schools compared with normal school provision (MYRIAD): study protocol for a randomised controlled trial. Trials. 2017;18(1):1–17.
Kabat-Zinn J. Meditation is not what you think. New York: Hachette Books; 2018.
Kabat-Zinn J. Full catastrophe living: using the wisdom of your body and mind to face stress, pain and illness. New York: Bantam Books; 1990.
De Vibe M, Fattah S, Dyrdal GM. Tanner-smith EE. Mindfulness-based stress reduction (MBSR) for improving health, quality of life and social functioning in adults: a systematic review and meta-analysis. 2017.
Dunning DL, Griffiths K, Kuyken W, Crane C, Foulkes L, Parker J, et al. Research review: the effects of mindfulness-based interventions on cognition and mental health in children and adolescents – a meta-analysis of randomized controlled trials. J Child Psychol Psychiatry. 2018;60(3).
About the four upper secondary education programmes. [cited 2020 Oct 12]. Available from: https://eng.uvm.dk/upper-secondary-education/national-upper-secondary-education-programmes/the-four-upper-secondary-education-programmes
Danish SOSU-schools. [cited 2020 Oct 12]. Available from: https://sosu.dk/sosu-uddannelsen/
Perera R, Heneghan C, Yudkin P. A graphical method for depicting randomised trials of complex interventions. Br Med J. 2007;334(7585):127–9.
The Danish Association for promoting life wisdom in children. [cited 2020 Sep 30]. Available from: https://bornslivskundskab.dk/eng/
Baer R, Crane C, Miller E, Kuyken W. Doing no harm in mindfulness-based programs: conceptual issues and empirical findings. Clin Psychol Rev. 2019;71:101–14. https://doi.org/10.1016/j.cpr.2019.01.001.
Lindahl JR, Fisher NE, Cooper DJ, Rosen RK, Britton WB. The varieties of contemplative experience: a mixed-methods study of meditation-related challenges in Western Buddhists. PLoS ONE. 2017;12:1–38.
Koushede V, Lasgaard M, Hinrichsen C, Meilstrup C, Nielsen L, Rayce SB, et al. Measuring mental well-being in Denmark: validation of the original and short version of the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS and SWEMWBS) and cross-cultural comparison across four European settings. Psychiatry Res. 2018;2019(271):502–9.
Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, et al. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): development and UK validation. Health Qual Life Outcomes. 2007;5(63):1–13.
Goodman R, Meltzer H, Bailey V. The Strengths and Difficulties Questionnaire: a pilot study on the validity of the self-report version. Int Rev Psychiatry. 2003;15(1–2):173–7.
Goodman A, Goodman R. Strengths and difficulties Questionnaire as a dimensional measure of child mental health. J Am Acad Child Adolesc Psychiatry. 2009;48(4):400–3.
Arnfred J, Svendsen K, Rask C, Jeppesen P, Fensbo L, Houmann T, et al. Danish norms for the strengths and difficulties questionnaire. Dan Med J. 2019;66(6):1–7.
Henry JD, Crawford JR. The short-form version of the Depression Anxiety Stress Scales (DASS-21): construct validity and normative data in a large non-clinical sample. Br J Clin Psychol. 2005;44(2):227–39.
Lovibond SH, Lovebond PF. Manual for the Depression Anxiety Stress Scales (2nd edition). Psychol Found Australa. 1995. p. 42.
Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–96.
Eskildsen A, Dalgaard VL, Nielsen KJ, Andersen JH, Zachariae R, Olsen LR, et al. Cross-cultural adaptation and validation of the Danish consensus version of the 10-item Perceived Stress Scale. Scand J Work Environ Heal. 2015;41(5):486–90.
Smith BW, Dalen J, Wiggins K, Tooley E, Christopher P, Bernard J. The Brief Resilience Scale: assessing the ability to bounce back. Int J Behav Med. 2008;15:194–200.
Windle G, Bennett KM, Noyes J. A methodological review of resilience measurement scales. Health Qual Life Outcomes. 2011;9(8):1–18.
Fresco DM, Moore MT, van Dulmen MHM, Segal ZV, Ma SH, Teasdale JD, et al. Initial psychometric properties of the Experiences Questionnaire: validation of a self-report measure of decentering. Behav Ther. 2007;38(3):234–46.
Kreimeier S, Greiner W. EQ-5D-Y as a health-related quality of life instrument for children and adolescents: the instrument’s characteristics, development, current use, and challenges of developing its value set. Value Heal. 2019;22(1):31–7.
Hughes ME, Waite LJ, Hqwkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys: results from two population-based studies. Res Aging. 2004;26(6):655–72.
Russell D. UCLA Loneliness Scale (version 3): reliability, validity, and factor structure. J Pers Assess. 1996;66(1):20–40.
Åkerstedt T, Hume K, Minors D, Waterhouse J. The meaning of good sleep: a longitudinal study of polysomnography and subjective sleep quality. J Sleep Res. 1994;3:152–8.
Kuyken W, Weare K, Ukoumunne OC, Vicary R, Motton N, Burnett R, et al. Effectiveness of the mindfulness in schools programme: non-randomised controlled feasibility study. Br J Psychiatry. 2013;203(2):126–31.
O’Dea B, Han J, Batterham PJ, Achilles MR, Calear AL, Werner-Seidler A, et al. A randomised controlled trial of a relationship-focussed mobile phone application for improving adolescents’ mental health. J Child Psychol Psychiatry. 2020;61(8):899–913.
Manicavasagar V, Horswood D, Burckhardt R, Lum A, Hadzi-Pavlovic D, Parker G. Feasibility and effectiveness of a web-based positive psychology program for youth mental health: randomized controlled trial. J Med Internet Res. 2014;16(6):1–17.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research Electronic Data Capture (REDCap) - a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inf. 2009;42(2):377–81.
Acknowledgements
We wish to thank all the participating schools, teachers, and students for their support of this research project.
Funding
The Danish Parliament (Case No. 1800332) has funded the development of the teacher training programme, the development of the “On Top of Everything” programme, and the training of the school teachers. The Danish Parliament has no role in the study design, data collection, analysis, interpretation of the data, and writing of the manuscripts.
Author information
Authors and Affiliations
Contributions
LJ and LOF have designed the trial. MF has provided valuable input regarding the trial design and analysis plan, has performed the randomisation, and will supervise the statistical analysis. MSB has contributed to the pilot testing and improvement of the data collection procedures and wrote the first draft of the protocol manuscript. All authors have critically reviewed and contributed to the writing of the protocol. LJ and LOF are responsible for the final datasets and for publishing the results. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Central Denmark Region Committee on Health Research Ethics concluded that the trial should not be treated as a biomedical research project in accordance with the Committee Act § 2, no. 1 and § 14, 1. The research complies with the General Data Protection Regulation (EU) 2016/679 of 27 April 2016 article 6 (1) litra (a) and the Data Protection Act § 10(1). The project is registered at Aarhus University’s record of processing activities under journal no. 2016–051-000001, serial number 1145. Aarhus University hereby confirms that under these conditions, the project is compliant with the EU and national legislation on data protection. The trial is registered at ClinicalTrials.gov Identifier: NCT04610333. Any protocol modifications that might occur will be communicated at Aarhus University’s record of processing activities and at ClinicalTrials.gov. Students will be informed about the option to opt out and not complete the questionnaires.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Beck, M.S., Juul, L., Frydenberg, M. et al. On Top of Everything: a study protocol for a cluster-randomised controlled trial testing a teacher training programme to teach mindfulness among students in Danish upper secondary schools and schools of health and social care. Trials 24, 17 (2023). https://doi.org/10.1186/s13063-022-06920-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-022-06920-7