
Abstract
Background
Previous studies have reported high prognostic accuracy of circulating neurofilament light (NfL) at 24–72 h after out-of-hospital cardiac arrest (OHCA), but performance at earlier time points and after in-hospital cardiac arrest (IHCA) is less investigated. We aimed to assess plasma NfL during the first 48 h after OHCA and IHCA to predict long-term outcomes.
Methods
Observational multicentre cohort study in adults admitted to intensive care after cardiac arrest. NfL was retrospectively analysed in plasma collected on admission to intensive care, 12 and 48 h after cardiac arrest. The outcome was assessed at two to six months using the Cerebral Performance Category (CPC) scale, where CPC 1–2 was considered a good outcome and CPC 3–5 a poor outcome. Predictive performance was measured with the area under the receiver operating characteristic curve (AUROC).
Results
Of 428 patients, 328 (77%) suffered OHCA and 100 (23%) IHCA. Poor outcome was found in 68% of OHCA and 55% of IHCA patients. The overall prognostic performance of NfL was excellent at 12 and 48 h after OHCA, with AUROCs of 0.93 and 0.97, respectively. The predictive ability was lower after IHCA than OHCA at 12 and 48 h, with AUROCs of 0.81 and 0.86 (p ≤ 0.03). AUROCs on admission were 0.77 and 0.67 after OHCA and IHCA, respectively. At 12 and 48 h after OHCA, high NfL levels predicted poor outcome at 95% specificity with 70 and 89% sensitivity, while low NfL levels predicted good outcome at 95% sensitivity with 71 and 74% specificity and negative predictive values of 86 and 88%.
Conclusions
The prognostic accuracy of NfL for predicting good and poor outcomes is excellent as early as 12 h after OHCA. NfL is less reliable for the prediction of outcome after IHCA.
Similar content being viewed by others
Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Accurate neuroprognostication is essential in patients who remain comatose after cardiac arrest to identify patients who may recover and avoid futile treatment in those who will never awake. Current guidelines recommend multimodal prognostication no earlier than 72 h post-arrest to allow time for recovery and clearance of sedative drugs [1]. Further investigation into markers with early prognostic value in comatose survivors after cardiac arrest may enable earlier multimodal neuroprognostication.
Neurofilament light chain protein (NfL) is a novel biomarker of neuroaxonal injury. Elevated circulating NfL at 24–72 h is highly predictive of poor neurological outcome after out-of-hospital cardiac arrest (OHCA) [2,3,4]. Additionally, low levels of NfL at 24–72 h have been reported to accurately identify patients with good outcome [3, 5]. The prognostic value is low early after ICU admission and the earliest time point when NfL can provide reliable prognostic information is unknown [3, 6]. Previous studies reporting the highest prognostic performance of NfL included only selected cohorts of OHCA [2, 3]. Further studies are needed to validate the predictive value of NfL in heterogeneous cohorts of post-cardiac arrest patients [7].
The current study aimed to investigate the prognostic performance of NfL to predict good and poor outcomes in the first two days after cardiac arrest in an unselected cohort of OHCA and in-hospital cardiac arrest (IHCA) patients. We hypothesised that the predictive performance would be acceptable at 12 h and improve at 48 h due to accumulating brain injury and biomarker kinetics. We also hypothesised that NfL would be a more accurate predictor of outcome after OHCA than IHCA due to differences in patient and clinical characteristics [8, 9].
Methods
Study design and setting
This was a retrospective, multicentre observational study of patients admitted after cardiac arrest to three Intensive Care Units (ICU) in southern Sweden from 2014 to 2018, with no pre-defined study size. The patients were consecutively included in the SWECRIT biobank, aiming to study biomarkers in critically ill patients (ClinicalTrials.gov no. NCT04974775, retrospectively registered July 2021). The study protocol was approved by the Regional Ethical Review Board in Lund, Sweden (registration no. 2014–47 and 2022-02681-01). Written informed consent was obtained from patients who regained mental capacity. The Standards for Reporting Diagnostic accuracy studies (STARD) guidelines were followed [10].
Study population
All patients 18 years or older admitted to intensive care after cardiac arrest were eligible for inclusion. International guidelines on post-resuscitation care were followed, including multimodal neuroprognostication no earlier than 72 h after cardiac arrest for patients who remained unconscious [11]. Blood samples were collected on ICU admission, 12 and 48 h after cardiac arrest. Samples drawn within six hours of the specified time points were included for statistical analysis. Patients with admission samples only (0–6 h after cardiac arrest) were excluded from this study.
Biochemical analyses
All samples were centrifuged, aliquoted, and frozen to −80 °C before storage in the biobank at Region Skane, Sweden (BD-47, SC-1922). The measurements of NfL were performed at the Clinical Neurochemistry Laboratory at the University of Gothenburg in September 2021 by staff blinded to clinical outcomes. Plasma NfL levels were measured using a single-molecule array (Simoa) NfL immunoassay on an HD-X analyser according to instructions from the kit manufacturer (Quanterix, Billerica, MA). Serum neuron-specific enolase (NSE) was analysed by the local laboratory in Region Skane as part of management in clinical practice [12], using a Cobas instrument with electrochemiluminescent immunoassays (Roche Diagnostics, Rotkreuz, Switzerland).
Data sources and outcome
Patient data were collected from the International Cardiac Arrest Registry (INTCAR), the patient administrative system for intensive care units (PASIVA), the Swedish population register, and medical records. Routine electroencephalogram (EEG) was performed when indicated at the treating physician’s discretion. Neurological outcome according to the Cerebral Performance Category (CPC) scale [13] was assessed two to six months post-arrest by personnel (physician or nurse) blinded to NfL levels. We considered CPC 1–2 as good outcome and CPC 3–5 as poor outcome.
Statistical methods
Clinical characteristics are presented as medians and interquartile ranges (IQR) or as counts and percentages. Groups were compared using Mann–Whitney U test, Pearson’s Chi-squared test, or logistic regression. Diagnostic performance was assessed by the area under the receiver operating characteristic curve (AUROC), defined from logistic regression models with and without addition of alternative methods for prediction of outcome. A model with clinical data included age, time to ROSC, witnessed cardiac arrest, bystander CPR (OHCA), shockable rhythm, and administration of adrenaline. The DeLong method was used to compare AUROCs for paired data.
To account for missing data, a multiple imputations approach [14] using the package mice for R was used with the CART method (imputation by classification and regression trees) over N = 20 multiple imputations. Pooled AUROCs were calculated over the imputed datasets using Rubin’s Rules, as implemented in the psfmi package for R.
We assessed partial AUROC (pAUROC) to predict poor outcome at 95–100% specificity. We determined pAUROC to predict a good outcome at 80–95% sensitivity, aiming to be highly predictive and to identify most patients with a good outcome. At the set specificities (95 and 100%) and sensitivities (80 and 95%), we determined cut-offs, positive predictive values (PPV, prediction of poor outcome), and negative predictive values (NPV, prediction of good outcome). We used a bootstrap method implemented in the R package pROC to calculate 95% confidence intervals (CI) and compare paired pAUROCs.
We used logistic regression models separately for OHCA and IHCA to adjust for covariates identified with stepwise backward regression. The backward elimination was continued for as long as the Akaike information criterion (AIC) decreased (R package MASS). We also evaluated differences in the performance of NfL to predict outcome after OHCA and IHCA with an interaction model, testing the interaction between NfL and cardiac arrest setting (OHCA vs IHCA). We tested if the covariates identified in the previous step eliminated the interaction, first using all covariates and finally only the covariates with a significant effect in the interaction model.
To reduce the skewness of the NfL measurements, we used log10-transformed data. Significance was set at p < 0.05. All analyses were performed using R, version 4.1.2 [15].
Results
Study population
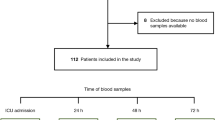
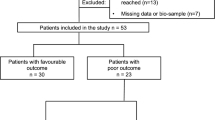
Of 797 patients admitted after cardiac arrest, 617 patients were included in the SWECRIT biobank. After exclusions, 428 patients remained, and of those, 328 (77%) suffered OHCA and 100 (23%) IHCA (Fig. 1). A description of missed and excluded patients is presented in Additional file 1: Table S1. Patient characteristics and outcomes are presented in Table 1 and stratified by outcomes in Additional file 1: Table S2. IHCA compared to OHCA patients were more often females, had more often congestive heart failure, renal disease, diabetes, and cerebrovascular disease, less often a cardiac cause and shockable rhythm, shorter time to ROSC, and on ICU admission higher Glasgow Coma Scale Motor response (GCS-M) and lower lactate (p < 0.05). The mortality at 30 and 180 days were lower and withdrawal of life-sustaining therapy (WLST), WLST due to poor prognosis, and poor neurological outcome were less common after IHCA than OHCA (p < 0.01).

Study flowchart. Long-term outcomes, according to the Cerebral Performance Category (CPC) scale, were dichotomised into good (CPC 1–2) and poor (CPC 3–5) outcomes. ICU intensive care unit, OHCA out-of-hospital cardiac arrest, IHCA in-hospital cardiac arrest
NfL levels were available on admission in 289 OHCA and 83 IHCA patients, at 12 h in 300 OHCA and 87 IHCA patients, and at 48 h in 210 OHCA and 54 IHCA patients. The reasons for missed sampling and time to sampling are presented in Additional file 1: Table S3. In addition, NfL levels were available in 60 samples from 39 OHCA and 13 IHCA patients outside the defined time limits (these data were not used for statistical analyses, but included in Fig. 2).

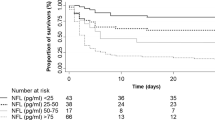
Neurofilament light (NfL) levels over time in OHCA and IHCA patients with good (CPC 1–2) and poor (CPC 3–5) outcomes. The bold lines show the trajectory trend with 95% CI. Each dot represents a sample, and each subtle line a patient. In addition to samples at the defined time points, admission (0–6 h), 12 ± 6 h, and 48 ± 6 h, samples collected outside these time limits (n = 60) were included in this illustration. OHCA out-of-hospital cardiac arrest, IHCA in-hospital cardiac arrest, CPC Cerebral Performance Category
Plasma levels of NfL
NfL levels were higher in patients with poor compared to good outcome at all time points after both OHCA and IHCA, Additional file 1: Fig. S1. The difference remained significant after adjustment for covariates, (p < 0.02 on admission, p < 0.008 at 12 and 48 h) (see Additional file 1: Fig. S2). In patients with a good outcome, NfL median levels were lower after OHCA than IHCA on admission (10 vs. 22 pg/ml, p < 0.001) and at 12 h (11 vs. 25 pg/ml, p = 0.009) but not significantly different at 48 h (21 vs. 36 pg/ml). In patients with poor outcome, NfL levels were lower after OHCA than IHCA on admission (23 vs. 44 pg/ml, p = 0.001), similar at 12 h (96 vs. 100 pg/ml), and higher at 48 h (1425 vs. 541 pg/ml, p = 0.001). The trends of NfL levels over time in all OHCA and IHCA patients with good and poor outcomes are visualised in Fig. 2.
Performance of NfL for prediction of outcomes
The overall prognostic performance of NfL was excellent at 12 and 48 h after OHCA, with AUROCs of 0.93 and 0.97, respectively (p = 0.02) (Fig. 3A). After IHCA, the AUROCs at 12 and 48 h were 0.81 and 0.86, respectively (p = 0.44) (Fig. 3B). The predictive ability was higher after OHCA compared to IHCA at 12 h (p = 0.02) and 48 h (p = 0.03). The performance on admission did not differ significantly between OHCA and IHCA, with AUROCs of 0.77 and 0.67, respectively. In sensitivity analyses where the AUROCs for NfL to predict poor outcome were calculated over multiple imputed datasets in all included patients (n = 617, Fig. 1), the results were overall similar as in the main analyses (Additional file 1: Table S4).

A-B Performance of neurofilament light (NfL) for prediction of neurologic outcomes. Receiver operating characteristic curves (ROC) and the area under the curve (AUROC) of NfL levels measured on admission (0 h), 12 h, and 48 h after OHCA and IHCA for prediction of good (CPC 1–2) versus poor (CPC 3–5) outcomes. OHCA out-of-hospital cardiac arrest, IHCA in-hospital cardiac arrest, CPC Cerebral Performance Category
NfL combined with other data for prognostication
We also tested if NfL provided additional information to other prognostic modalities. The prognostic performance of a model with baseline clinical information increased when adding NfL at 12 h or 48 h after OHCA (from AUROCs 0.86–0.90 for clinical models to 0.96–0.98 for combined models) and after IHCA (from AUROCs 0.72–0.73 to 0.85–0.96) (p < 0.01), but not when adding NfL on admission (Additional file 1: Table S5).
In a subgroup of OHCA patients with EEG data (not analysed in IHCA due to limited data), the prognostic performance of routine EEG (median [IQR] 75 [59-98] h after cardiac arrest) was improved by adding NfL at 12 h (AUROC 0.77 to 0.90, p < 0.001) or 48 h (AUROC 0.74 to 0.97, p < 0.001), but not by NfL on admission (Additional file 1: Table S6).
In a subgroup of OHCA and IHCA patients with available NSE data (sampled at 24 h and 48 h), NfL at 12 h was superior to NSE at 24 h, while NfL at 48 h was superior to NSE at 48 h (p < 0.001 after OHCA, p < 0.05 after IHCA), (Additional file 1: Fig. S3).
Exploring the different prognostic abilities of NfL in OHCA and IHCA
Due to the differences in results for OHCA and IHCA described above, we evaluated an interaction model where NfL and cardiac arrest setting (OHCA or IHCA) showed a significant interaction to predict poor outcome, when using NfL at 12 h (p = 0.003) but not NfL on admission or at 48 h. The interaction at 12 h was eliminated (p = 0.17) by adding the significant covariates age, time to ROSC, cardiac cause, shockable rhythm, and administration of adrenaline to the model (Additional file 1: Table S7).
Plasma NfL for prediction of poor outcome
The performance of NfL to predict the outcome at high specificity (95–100%) assessed with pAUROC was higher after OHCA compared to IHCA at 12 and 48 h (p < 0.04) and similar on admission (Table 2). In OHCA patients, the pAUROC was lower at 12 h than at 48 h (p < 0.001). At 95% specificity, the sensitivity was 70% at 12 h and 89% at 48 h after OHCA.
Plasma NfL for prediction of good outcome
The performance of low NfL levels to predict the outcome at high sensitivity (80–95%) was higher after OHCA compared to IHCA at 12 h and 48 h (p < 0.03) and similar on admission (Table 3). In OHCA patients, there was no significant difference in performance between NfL at 12 h and 48 h. At 95% sensitivity in OHCA at 12 h and 48 h, 71% and 74% of the patients with good outcome (specificity) had NfL levels below the cut-off, corresponding to 86% and 88% correct prediction of good outcome (NPV).
Discussion
This multicentre cohort study investigated the ability of plasma NfL to predict long-term neurological outcome in a heterogeneous population admitted to intensive care after cardiac arrest. NfL at 12 and 48 h after OHCA reliably predicted good and poor neurological outcomes. The predictive ability after IHCA compared to OHCA was lower at 12 and 48 h.
The prognostic performance of NfL at 12 h after OHCA in this study was similar to the accuracy of NfL at 24 and 48 h in two previous studies [2, 4]. One study included an unselected OHCA cohort [4], and the other investigated a selected group of OHCA patients of a presumed cardiac cause [2, 16]. The performance was slightly higher in the COMACARE trial [3, 17], which included a more selected patient group with initial shockable rhythm. The accuracy of any test will depend on the population studied, and the predictive ability will likely improve in highly selected populations of OHCA. Despite the heterogeneous OHCA cohort in this study, the ability of NfL to predict the outcome at 12 and 48 h was excellent, and superior to NSE. This novel finding supports the generalisability of NfL as a useful prognostic tool across the entire spectrum of OHCA patients in the ICU.
In the present study, the prediction of poor outcome at high specificity was better at 48 h compared to 12 h after OHCA. The improved prediction with time likely reflects evolving post-anoxic brain injury but may also be explained by patients not included at 48 h due to prior haemodynamic collapse and circulatory deaths. Although lower than at 48 h, the predictive ability of NfL at 12 h shown here may still be of clinical value.
Low levels of NfL have been shown to predict a good neurological outcome at 24 h after OHCA [3, 5]. In this study, NfL, as early as 12 h after OHCA, had a high ability to predict good outcome. Early prediction of neurological recovery may aid in decision-making, e.g. regarding invasive procedures, and could help avoid inappropriate limitations in care and provide relevant information for relatives. Another potential clinical use of a low 12 h NfL value would be to tailor neuroprotective strategies, e.g. by attempting an early wake up in patients with low NfL. Our results suggest that the prognostic value of EEG is improved by NfL already at 12 h, supporting the prognostic performance of NfL when measured at least 12 h after cardiac arrest. Future studies could explore whether early prediction of outcome may be further strengthened by combining NfL levels at 12 or 24 h with an early (< 24 h) return of a continuous background pattern on EEG [18, 19].
In this study, the predictive performance of NfL on admission to intensive care was low, which is in line with previous studies [3, 6, 20]. In patients with poor outcome, NfL levels increase substantially as post-hypoxic brain injury develops and may reach a steady state between 48 and 72 h [2, 3, 21]. NfL is also known to increase with age, even under normal circumstances [22], and elevated NfL levels can be caused by neurological comorbidity and traumatic brain injury [23,24,25,26,27]. NfL increase caused by other conditions is typically low compared to NfL levels released due to hypoxic brain injury [28,29,30], but in very early prognostication and when low NfL levels are used to predict a good outcome, other causes of NfL elevation may be important to consider.
To our knowledge, NfL has previously not been analysed in an IHCA cohort. The prognostic accuracy of NfL was lower in IHCA compared to OHCA at both 12 and 48 h. However, a significant interaction between the location of arrest and outcome prediction by NfL was only found at 12 h. These results suggest an overall trend for lower predictive ability after IHCA, particularly early after cardiac arrest. IHCA and OHCA patients differ in key parameters that are relevant for prognostication. For example, the time to ROSC was shorter and WLST due to poor prognosis less common after IHCA than OHCA, suggesting a less severe brain injury in IHCA. This is also reflected by the higher level of consciousness on ICU admission after IHCA. When focusing on patients with good outcome, we found that NfL was generally higher in IHCA than OHCA, which may be explained by their higher age and more comorbidities in this cohort [8, 9, 31]. NfL, as a marker of neuroaxonal injury, is not likely to identify patients with poor outcomes due to haemodynamic collapse or other causes of non-neurological death, which may contribute to the lower predictive ability of NfL in IHCA patients. When adjusting our analyses for age, time to ROSC, cardiac cause, shockable rhythm and administration of adrenaline, the difference between IHCA and OHCA in predictive ability of NfL was no longer significant, suggesting that patient and cardiac arrest characteristics may explain the lower predictive value of NfL after IHCA.
Strengths and limitations
Strengths of the present study are the heterogeneous cohort, allowing for more generalisable results, the multicentre design, the large sample size of OHCA patients, and the batch analysis of NfL samples. A limitation of this and other NfL studies is that there is no certified standard for analysis, and both analytical and preanalytical factors may vary, complicating comparisons of NfL levels reported by different studies. Before NfL can be implemented in clinical practice, future studies must establish a standard for analysis and normal values for NfL. This study is also limited by its retrospective design. The data quality depended on the documentation in the patient's medical notes, data on the presumed cause of death was unavailable, and the time to follow-up varied. The sample size of IHCA was small, particularly at 48 h.
Another limitation is that a lack of withdrawal of consent after regaining consciousness in some patients will lead to an underestimation of the proportion of survivors. Differences between included and excluded patients suggest that missing patients were due to early deaths and transfers from the ICU. Prognostication is not performed in clinical practice in patients who die or wake up early, but we cannot exclude that missed inclusions have affected the generalisability of the study.
Conclusion
This study suggests that NfL accurately predicts good and poor neurological outcomes as early as 12 h after cardiac arrest in a heterogeneous group of OHCA patients. The predictive ability of NfL is less reliable after IHCA and needs further investigation.
Availability of protocol and data
The study protocol and the datasets analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AIC:
-
Akaike information criterion
- AUROC:
-
Area under the receiver operating curve
- CI:
-
Confidence interval
- COPD:
-
Chronic obstructive pulmonary disease
- CPC:
-
Cerebral Performance Category
- CPR:
-
Cardiopulmonary resuscitation
- EEG:
-
Electroencephalogram
- ICU:
-
Intensive care unit
- GCS-M:
-
Glasgow Coma Scale Motor response
- IHCA:
-
In-hospital cardiac arrest
- INTCAR:
-
International cardiac arrest registry
- IQR:
-
Interquartile range
- NfL:
-
Neurofilament light chain
- NPV:
-
Negative predictive values
- NSE:
-
Neuron-specific enolase
- OHCA:
-
Out-of-hospital cardiac arrest
- OR:
-
Odds ratio
- PASIVA:
-
Patient administrative system for intensive care units
- pAUROC:
-
Partial area under the receiver operating curve
- PPV:
-
Positive predictive values
- ROSC:
-
Return of spontaneous circulation
- Simoa:
-
Single-molecule array
- STARD:
-
Standards for reporting diagnostic accuracy studies
- WLST:
-
Withdrawal of life-sustaining therapy
References
Nolan JP, Sandroni C, Bottiger BW, Cariou A, Cronberg T, Friberg H, et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care.Intensive Care Med. 2021;47(4):369-421.
Moseby-Knappe M, Mattsson N, Nielsen N, Zetterberg H, Blennow K, Dankiewicz J, et al. Serum neurofilament light chain for prognosis of outcome after cardiac arrest. JAMA Neurol. 2019;76(1):64–71.
Wihersaari L, Ashton NJ, Reinikainen M, Jakkula P, Pettila V, Hastbacka J, et al. Neurofilament light as an outcome predictor after cardiac arrest: a post hoc analysis of the COMACARE trial. Intens Care Med. 2021;47(1):39–48.
Wihersaari L, Reinikainen M, Furlan R, Mandelli A, Vaahersalo J, Kurola J, et al. Neurofilament light compared to neuron-specific enolase as a predictor of unfavourable outcome after out-of-hospital cardiac arrest. Resuscitation. 2022;174:1–8.
Moseby-Knappe M, Mattsson-Carlgren N, Stammet P, Backman S, Blennow K, Dankiewicz J, et al. Serum markers of brain injury can predict good neurological outcome after out-of-hospital cardiac arrest. Intens Care Med. 2021;47(9):984–94.
Adler C, Onur OA, Braumann S, Gramespacher H, Bittner S, Falk S, et al. Absolute serum neurofilament light chain levels and its early kinetics predict brain injury after out-of-hospital cardiac arrest. J Neurol. 2022;269(3):1530–7.
Taccone FS, Nolan JP, Hoedemaekers CWE. Neurofilament to predict post-anoxic neurological outcome: are we ready for the prime time? Intens Care Med. 2021;47(1):77–9.
Hoybye M, Stankovic N, Holmberg M, Christensen HC, Granfeldt A, Andersen LW. In-hospital vs. out-of-hospital cardiac arrest: patient characteristics and survival. Resuscitation. 2021;158:157–65.
Andersson A, Arctaedius I, Cronberg T, Levin H, Nielsen N, Friberg H, et al. In-hospital versus out-of-hospital cardiac arrest: characteristics and outcomes in patients admitted to intensive care after return of spontaneous circulation. Resuscitation. 2022;176:1–8.
Cohen JF, Korevaar DA, Altman DG, Bruns DE, Gatsonis CA, Hooft L, et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: explanation and elaboration. BMJ Open. 2016;6(11): e012799.
Nolan JP, Soar J, Cariou A, Cronberg T, Moulaert VR, Deakin CD, et al. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines for Post-resuscitation Care 2015: Section 5 of the European Resuscitation Council Guidelines for Resuscitation 2015. Resuscitation. 2015;95:202-22.
Lissner Ostlund E, Levin H, Nielsen N, Frigyesi A, Lybeck A. Neuron-specific enolase and long-term neurological outcome after OHCA - a validation study. Resuscitation. 2021;168:206–13.
Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. 1975;1(7905):480–4.
Li P, Stuart EA, Allison DB. Multiple imputation: a flexible tool for handling missing data. JAMA. 2015;314(18):1966–7.
R Core Team. R: a language and environment for statistical computing. Vienna: Foundation for Statistical Computing. 2013.
Nielsen N, Wetterslev J, Al-Subaie N, Andersson B, Bro-Jeppesen J, Bishop G, et al. Target temperature management after out-of-hospital cardiac arrest–a randomized, parallel-group, assessor-blinded clinical trial–rationale and design. Am Heart J. 2012;163(4):541–8.
Jakkula P, Reinikainen M, Hastbacka J, Pettila V, Loisa P, Karlsson S, et al. Targeting low- or high-normal Carbon dioxide, Oxygen, and Mean arterial pressure After Cardiac Arrest and REsuscitation: study protocol for a randomized pilot trial. Trials. 2017;18(1):507.
Hofmeijer J, Beernink TM, Bosch FH, Beishuizen A, Tjepkema-Cloostermans MC, van Putten MJ. Early EEG contributes to multimodal outcome prediction of postanoxic coma. Neurology. 2015;85(2):137–43.
Oh SH, Park KN, Shon YM, Kim YM, Kim HJ, Youn CS, et al. Continuous amplitude-integrated electroencephalographic monitoring is a useful prognostic tool for hypothermia-treated cardiac arrest patients. Circulation. 2015;132(12):1094–103.
Hunziker S, Quinto A, Ramin-Wright M, Becker C, Beck K, Vincent A, et al. Serum neurofilament measurement improves clinical risk scores for outcome prediction after cardiac arrest: results of a prospective study. Crit Care. 2021;25(1):32.
Rana OR, Schroder JW, Baukloh JK, Saygili E, Mischke K, Schiefer J, et al. Neurofilament light chain as an early and sensitive predictor of long-term neurological outcome in patients after cardiac arrest. Int J Cardiol. 2013;168(2):1322–7.
Koini M, Pirpamer L, Hofer E, Buchmann A, Pinter D, Ropele S, et al. Factors influencing serum neurofilament light chain levels in normal aging. Aging (Albany NY). 2021;13(24):25729–38.
Gisslen M, Price RW, Andreasson U, Norgren N, Nilsson S, Hagberg L, et al. Plasma concentration of the neurofilament light protein (NFL) is a biomarker of CNS injury in HIV infection: a cross-sectional study. EBioMedicine. 2016;3:135–40.
De Marchis GM, Katan M, Barro C, Fladt J, Traenka C, Seiffge DJ, et al. Serum neurofilament light chain in patients with acute cerebrovascular events. Eur J Neurol. 2018;25(3):562–8.
Mattsson N, Cullen NC, Andreasson U, Zetterberg H, Blennow K. Association between longitudinal plasma neurofilament light and neurodegeneration in patients with alzheimer disease. JAMA Neurol. 2019;76(7):791–9.
Feneberg E, Oeckl P, Steinacker P, Verde F, Barro C, Van Damme P, et al. Multicenter evaluation of neurofilaments in early symptom onset amyotrophic lateral sclerosis. Neurology. 2018;90(1):e22-30.
Hansson O, Janelidze S, Hall S, Magdalinou N, Lees AJ, Andreasson U, et al. Blood-based NfL: a biomarker for differential diagnosis of parkinsonian disorder. Neurology. 2017;88(10):930–7.
Khalil M, Pirpamer L, Hofer E, Voortman MM, Barro C, Leppert D, et al. Serum neurofilament light levels in normal aging and their association with morphologic brain changes. Nat Commun. 2020;11(1):812.
Ashton NJ, Janelidze S, Al Khleifat A, Leuzy A, van der Ende EL, Karikari TK, et al. A multicentre validation study of the diagnostic value of plasma neurofilament light. Nat Commun. 2021;12(1):3400.
Humaloja J, Ashton NJ, Skrifvars MB. Brain injury biomarkers for predicting outcome after cardiac arrest. Crit Care. 2022;26(1):81.
Mandigers L, Termorshuizen F, de Keizer NF, Gommers D, Dos Reis MD, Rietdijk WJR, et al. A nationwide overview of 1-year mortality in cardiac arrest patients admitted to intensive care units in the Netherlands between 2010 and 2016. Resuscitation. 2020;147:88–94.
Acknowledgements
The authors would like to thank the nursing staff at the ICUs of Skane University Hospital in Malmö and Lund and Helsingborg Hospital for contributing to this study. We are also grateful to the patients who participated.
Funding
Open access funding provided by Lund University. Regional research support, Region Skane; Government funding of clinical research within the Swedish National Health Services (ALF); Biobanking and BioMolecular resources Research Infrastructure (BBMRI, Sweden); Hans-Gabriel and Alice Trolle-Wachtmeister Foundation for Medical Research; Anna-Lisa & Sven-Eric Lundgrens Foundation for medical research; European Union Interreg programme IV A. HZ is a Wallenberg Scholar supported by grants from the Swedish Research Council (#2018-02532), the European Research Council (#681712 and #101053962), Swedish State Support for Clinical Research (#ALFGBG-71320), the Alzheimer Drug Discovery Foundation (ADDF), USA (#201809-2016862), the AD Strategic Fund and the Alzheimer's Association (#ADSF-21-831376-C, #ADSF-21-831381-C and #ADSF-21-831377-C), the Olav Thon Foundation, the Erling-Persson Family Foundation, Stiftelsen för Gamla Tjänarinnor, Hjärnfonden, Sweden (#FO2019-0228), the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No 860197 (MIRIADE), the European Union Joint Programme—Neurodegenerative Disease Research (JPND2021-00694), and the UK Dementia Research Institute at UCL (UKDRI-1003). The funding organisations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
Concept and design were carried out by HF, NMC, HL, AF, and TC. Acquisition or interpretation of data was done by all authors. Biomarker analysis was done by NA, HZ, and KB. Statistical analysis was done by HL and NMC. Draft of the initial manuscript was done by HL, NMC, and AL. Funding was done by HF, AF, NMC, NN, and TC. Supervision was done by NMC, HF, AF, and AL. All authors contributed to the manuscript and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was granted by the Regional Ethical Review Board in Lund, Sweden (registration no. 2014-47 and 2022-02681-01). Written informed consent was obtained from patients who regained mental capacity.
Consent for publication
Not applicable.
Competing interests
HZ has served on scientific advisory boards and as a consultant for Abbvie, Alector, ALZPath, Annexon, Apellis, Artery Therapeutics, AZTherapies, CogRx, Denali, Eisai, Nervgen, Novo Nordisk, Pinteon Therapeutics, Red Abbey Labs, reMYND, Passage Bio, Roche, Samumed, Siemens Healthineers, Triplet Therapeutics, and Wave, has given lectures in symposia sponsored by Cellectricon, Fujirebio, Alzecure, Biogen, and Roche, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program (outside submitted work). KB has served as a consultant, at advisory boards, or at data monitoring committees for Abcam, Axon, Biogen, JOMDD/ Shimadzu. Julius Clinical, Lilly, MagQu, Novartis, Roche Diagnostics, and Siemens Healthineers, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program. The other authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Supplementary tables and figures.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Levin, H., Lybeck, A., Frigyesi, A. et al. Plasma neurofilament light is a predictor of neurological outcome 12 h after cardiac arrest. Crit Care 27, 74 (2023). https://doi.org/10.1186/s13054-023-04355-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-023-04355-3