
Abstract
Acute kidney injury (AKI) has been a global health epidemic problem with soaring incidence, increased long-term risks for multiple comorbidities and mortality, as well as elevated medical costs. Despite the improvement of patient outcomes following the advancements in preventive and therapeutic strategies, the mortality rates among critically ill patients with AKI remain as high as 40–60 %. The distant organ injury, a direct consequence of deleterious systemic effects, following AKI is an important explanation for this phenomenon. To date, most evidence of remote organ injury in AKI is obtained from animal models. Whereas the observations in humans are from a limited number of participants in a relatively short follow-up period, or just focusing on the cytokine levels rather than clinical solid outcomes. The remote organ injury is caused with four underlying mechanisms: (1) “classical” pattern of acute uremic state; (2) inflammatory nature of the injured kidneys; (3) modulating effect of AKI of the underlying disease process; and (4) healthcare dilemma. While cytokines/chemokines, leukocyte extravasation, oxidative stress, and certain channel dysregulation are the pathways involving in the remote organ damage. In the current review, we summarized the data from experimental studies to clinical outcome studies in the field of organ crosstalk following AKI. Further, the long-term consequences of distant organ-system, including liver, heart, brain, lung, gut, bone, immune system, and malignancy following AKI with temporary dialysis were reviewed and discussed.
Similar content being viewed by others


Introduction
Acute kidney injury (AKI) is a common clinical problem affecting up to 1 % of the general population and 8-15 % of hospitalized patients [1–3], and the incidence is increasing worldwide [4, 5]. Among the critically ill patients, about 50 % develop AKI and 4–15 % have severe AKI needing renal replacement therapy (RRT) support [6, 7]. Besides, AKI was found to be an independent predictor for end-stage renal disease (ESRD) in a large cohort study enrolling 233,803 elderly patients, and the impact of AKI on developing ESRD was even higher than that of previous chronic kidney disease (CKD) (hazard ratio (HR) of AKI alone and CKD alone, comparing with those without AKI or CKD, were 13.0 and 8.4, respectively) [8]. On the other hand, AKI has varied renal recovery rates ranging from 30 % to 70 % in diverse patient types [9].
AKI carries widely-ranged risks of morbidity and mortality in a stepwise manner which increase concurrently with increasing severity and duration of AKI, and even mild temporary AKI is associated with increased morbidity and mortality [8–11]. In addition, the different AKI recovery status might also attribute to mortality and morbidity [9, 10]. Thus AKI has been a global health epidemic problem with soaring incidence, increasing long-term risks for multiple comorbidities and mortality, along with growing healthcare costs [9, 11–13]. Owing to the advancements in preventive and therapeutic strategies, the AKI-associated mortality rates exhibited a significantly declining trend over the decades in both general hospitalized patients [14, 15] and critically ill patients [4]. However, the mortality rates among critically ill patients with AKI remain as high as 40–60 % [7, 16]. Even with survival from the catastrophic AKI events, they sequels of multi-organ damage are disconcerting. One of the possible explanations for this phenomenon is that the RRT, a currently most effective therapy for severe AKI, itself may also carry adverse side effects [17]. Another and perhaps a more important explanation is the distant organ injury, a direct consequence of deleterious systemic effects, following AKI [18, 19]. An increasing body of evidence supports that the extra-renal complications are at least partially responsible for the burden of mortality from AKI [20, 21]. Actually, AKI is often resulted from distant organ injury or systemic illness such as sepsis, and AKI can in turn cause extra-renal organ dysfunction [16, 18]. The term “organ crosstalk” is used to describe “the effects of one dysfunctional organ on the function of another” or “the reciprocal trigger of organ dysfunction of two different organs” [18, 19].
Although the concept of organ crosstalk in AKI is being gradually established, most of the evidence is obtained from animal models [22–24]. The observations in humans are from a limited number of participants in a relatively short follow-up period, [25] or just focusing on the cytokine levels rather than clinical solid outcomes [26]. As such, little is clearly understood on distant organ injury following AKI [18]. The aim of this review is to update the knowledge, from basic aspect to long-term clinical effect, regarding the remote organs consequences following AKI. The organ crosstalk goes from other organs to kidney resulting in AKI will not be covered in this review.
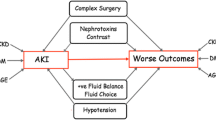
Distant organ consequences following AKI (Fig. 1)
AKI is gradually considered a pan-metabolic, pan-endocrine and pan-organ problem which exerts negative consequences on many organ systems of the body [27–29]. Briefly speaking, the systemic effects are the reflection of a broad common pathology which ultimately causes an ‘augmented’ inflammation and impairment of immunocompetence during AKI [29, 30]. These multifaceted systemic effects could be categorized into four underlying mechanisms: (1) “Classical” pattern of acute uremic state which affects all metabolic and endocrine pathways, causes disruption of electrolyte and volume homeostasis, and further proximate factors have a profound impact on immuno-competence [31–33]. (2) Inflammatory nature of the injured kidneys. Animal studies disclosed that injured kidneys may cause obviously higher inflammatory chemokines expression and renal fibrosis [34] as well as profound iron-mediated oxidative stress by disturbing systemic iron homeostasis [35], while supplement with hepcidin may increase the expression of renal H-ferritine and exhibit renal-protective effect [35]. The association between AKI and infection susceptibility is plausible given that acute kidney insults are known to induce changes in gene regulation, oxidative stress, inflammation, leukocyte trafficking, and apoptosis and to incite systemic and distal organ injury. The inflammatory process might eventually transform into systemic inflammatory reaction mediating distant organ injury [24, 36]. (3) Modulating effect of AKI of the underlying disease process. A great modulating effect on the underlying disease process of other organ-systems would be induced by the disturbed cytokine/chemokine homeostasis in AKI, which may be attributable to the decreased renal clearance and/or increased production of these cytokine/chemokine [34, 35, 37–39]. (4) Healthcare dilemman RRT support is generally considered as necessary for AKI patients with profound biochemical disarrangement or fluid overload [40]. However, RRT itself is proven to carry significant risks for adverse patient outcome owing to the hemodynamic instability and nutrients loss during RRT, as well as reactive oxygen species and inflammatory reaction secondary to the bio-incompatibility of artificial kidney, and the use of unfractionated heparin [17, 30, 41, 42]. The adequate serum level of antibiotics and anticoagulant are also difficult to achieve and maintain in AKI patients with RRT [17], which may disturb infection control or cause complications. Besides, the use of mechanical ventilation and hemodialysis catheters also raise the risk of complications.

Based on the aforementioned mechanisms, several complex pathways are involved in the crosstalk of organs during AKI, causing injury in distant organ-systems including neuromuscular, cardiovascular, pulmonary, gastrointestinal, hepatobiliary, immunologic, hematologic, and metabolic systems [18, 19, 21, 30, 39].
Long-term remote organ consequences following AKI with temporary dialysis
This review focused on the long-term pivotal effects of de novo RRT-requiring AKI on extra-renal organ systems. To avoid the confounding detrimental effects of chronic RRT, which has been proven to result in worse patient outcomes, the following review only covered studies in which the enrolled subjects were limited to those recovered from the most severe form of AKI, i.e. those with transient RRT-requiring AKI (Table 1).
Kidney-heart crosstalk
Most patients with acute decompensated heart failure have underlying renal insufficiency, which, alone or along with acute renal insults, expose the patients to adverse clinical outcomes [43–45]. The effects of cardiac failure on kidney injury may be through hemodynamic-, humoral- and immune-mediated pathways [46–49]. Reversely, AKI may also result in acute cardiac disorder via some mechanisms such as: (1) increased preload secondary to AKI-induced salt and water retention; (2) myocardial damage due to neutrophil trafficking, myocyte apoptosis, endothelial dysfunction, as well as elevated level of inflammatory cytokines (interleukin (IL)-1, IL-6, and tumor necrosis factor (TNF)-α) resulting from increased production and impaired clearance [21, 50–52].
To identify the association of AKI with long-term cardiovascular risk, Wu et al. [12] compared 4,869 patients who recovered from de novo RRT-requiring AKI (recovery-AKI group) and the same number of matched patients (no-AKI group). To make an unbiased estimate of the confounders, propensity score method was used to adjust baseline characteristics which might affect dialysis withdrawal and subsequent patient outcomes. The control group (no-AKI group) was matched with the exposure group (recovery-AKI group) on the basis of age, sex, same calendar year of index hospitalization, and comorbidities before and during index hospitalization. Furthermore, the results were further validated by analysis of a prospectively constructed database.
With a mean follow-up period of 3.31 years, the patients in “recovery-AKI group” had 1.7 times higher risk of coronary events than “no-AKI group”, independent of the effects of subsequent progression to CKD and ESRD. In an adjusted comparison, “RRT-requiring AKI alone” (3.3 times hazard) was associated with even higher long-term coronary events than “diabetes alone” (2.8 times hazard). Furthermore, adjusting for interim coronary events attenuated the association between RRT-requiring AKI and subsequent risk of death, supporting the hypothesis that coronary events are in the causal pathway linking AKI and mortality. The study substantiated the interaction of cardiorenal syndrome type 3, which describes impaired myocardial function by various interconnected pathways in AKI [53]. The association between AKI and subsequent risk for cardiac events were also identified in some other studies [54, 55].
Kidney-brain crosstalk
AKI has neurological complications including dizziness, attention deficits, tremor, seizure, altered mental status, delirium, and even death [21]. Cellular and soluble inflammatory mediators as well as uremic toxins contribute to the neurological symptoms. Animal studies using mice found that AKI may subsequently result in increased vascular permeability, disruption in the blood-brain barrier, increased cerebral proinflammatory cytokines (IL-6, IL-1β, IL-12, keratinocyte-derived chemokine, granulocyte-colony stimulating factor, and glial fibrillary acidic protein), and increased neuronal pyknosis and microgliosis (up-regulation of brain macrophages) [21, 23]. Microgliosis is a hallmark of cerebral inflammation and is implicated in the pathology of neurodegenerative diseases [56]. Alterations in calcium concentrations, water handling and neurotransmitter turnover may also play roles in functional changes in the brain after AKI [21]. Additionally, posterior reversible encephalopathy syndrome (PRES) has been reported in AKI patients with [57] and without hypertension [58]. Hypertension that exceeds the limits of auto-regulation of the brain, immune response and endothelial dysfunction may account for the development of PRES [58]. Reversely, although about one-fourth of hospitalized patients with acute stroke develop AKI, the renal changes secondary to neurological illness is less established [21]. Increased inflammation is observed in renal allografts from brain-dead donors [59].
A study determining the long-term effect of AKI on de novo stroke was carried out with a median follow-up period of 3.36 years [60]. The patients in “recovery-AKI group” (n = 4,315) had 1.3 times elevated risk of developing incident ischemic and hemorrhagic stroke than those in “no-AKI group” (n = 4,315) regardless of progression to subsequent CKD. The risk factors for kidney injury leading to an AKI event may persist and eventually lead to future stroke without a direct causal association with preexisting CKD. AKI may thus amplify the long-term risk of incident stroke and mortality, and the impact is similar to diabetes.
Over the 3 years of follow-up, RRT-requiring AKI is associated with an increased risk of dementia after critical illness [61]. Other independent risk factors include infection, severe sepsis [61], and a prolonged duration of delirium [62]. In this regard, interventions directed at reducing delirium and preserving renal function may mitigate brain injury associated with critical illness.
Kidney-immune system crosstalk
The profound impact on immunocompetence is one of the most important complications of AKI since kidney is an important immunologic organ. AKI can cause short- and long-term, either renal or systemic, immune-modulation. First of all, both T cell population and phenotype alteration within and outside the kidney were observed in animal model after ischemic/reperfusion kidney injury [63, 64], and these changes can last for about three months. Moreover, either ischemia/reperfusion injury itself or protein binding uremic toxin can leads to epigenetic modifications resulting in distinct genomic signatures [36, 65, 66]. In concordance to these findings, our group had also observed an increase in long-term risk of severe sepsis and tuberculosis after RRT-requiring AKI. The adjusted risk of developing severe sepsis prompting hospitalization was approximately two-fold higher among AKI survivors compared to non-AKI patients (incidence rate of 6.84 versus 2.32 per 100 person-years) [67]. Patients who recover from RRT-requiring AKI also had significantly higher incidence of TB than patients without AKI (HR, 3.84; p, 0.001) [68]. Taken together, studies from bench to bedside all showed that AKI alters host immunocompetence even after renal function recovery, and these alterations could affect patient’s long-term outcome.
On the other hand, several studies have shown that certain cytokine or chemokine gene polymorphism are related to the occurrence or severity of AKI. In clinical studies, TNF-α and IL-10 phenotype predict AKI and mortality in hospitalized patients [69, 70], while transforming growth factor (TGF)-β and interferon-γ genotype do not [71]. C-C chemokine receptor 5 knock-out mice showed increased susceptibility to lipopolysaccharide‑induced acute renal injury [72]. It is therefore reasonable to postulate that certain genetic backgrounds would affect the susceptibility to immune derangement, inflammation, sepsis and AKI, whichever happens first.
Kidney-lung crosstalk
Respiratory consequences are the most clinically relevant distant organ injury in AKI, and AKI is also commonly seen in patients with pulmonary inflammation and mechanical ventilation [21, 30]. AKI alters peripheral vascular responses by increasing oxidative stress, likely in the endothelium [73]. As to renal cytokine production, complement activation, toll-like receptor-2, and toll-like receptor 4 signaling contribute to cytokine production after AKI [74, 75]. Experimental studies demonstrated that AKI results in lung injury via following pathways: (1) lung edema, which may be resulted from increased pulmonary vascular permeability and dysregulated ion transport channels; (2) increased cytokines and chemokines related to impaired renal clearance and increased production; and (3) increased leukocyte trafficking with mononuclear phagocyte production. Besides, AKI may express modulatory effects that vary with the severity of lung injury [21, 76].
Following AKI, serum IL-6 increases in the absence of a counter anti-inflammatory response by spleen, and it brings an exuberant proinflammatory response and mediates lung injury via Chemokine (C-X-C motif) ligand 1 production in mice [77, 78]. In clinical studies, inflammatory cytokines, such as IL-6 and/or IL-8, are potential mediators of the distant organ damage from AKI. Serum IL-6 correlates with endothelial dysfunction in human [79], while elevated levels of IL-6 are associated with prolonged ventilator weaning times and increased mortality in patients with AKI and acute lung injury [80].
A study evaluating the long-term risk and outcome of active tuberculosis after AKI was conducted enrolling 2,909 RRT-requiring AKI patients (AKI-group) and 11,636 control individuals (no-AKI group) with a mean follow-up period of 3.6 years [68]. The “AKI-group” had 7.7 times higher risk of active tuberculosis than general population. Comparing with “no-AKI group”, the “recovery-AKI group” had 3.8 times, and “non-recovery AKI group” had 6.4 times elevated risk of getting tuberculosis. Besides, active tuberculosis was associated with 1.3 fold increased risk of long-term all-cause mortality after RRT-requiring AKI. These results raise concerns that the increasing global burden of AKI would also increase the incidence of active tuberculosis. The increased long-term risks for severe sepsis and tuberculosis might be the results of impaired pulmonary and immunologic function implicated by AKI.
Kidney-gut crosstalk
Gut is a newly-found organ which would be remotely injured during AKI. The inflammatory response and hypervolemia related to AKI alter the permeability of mesenteric vascular bed and promote the formation of intestinal edema, which is a hallmark of intestinal failure in sepsis [81]. Gut has been known as an amplifier of systemic inflammatory response syndrome in the setting of shock, gut hypoperfusion [82] and intestinal edema [81] through the mechanisms including increased intestinal permeability, disruption of mucosal integrity, liberation of proinflammatory mediators, translocation of intestinal microorganisms and resultant endotoxinemia. The augmented systemic inflammatory reaction by gut would in turn aggravate AKI, giving rise to a vicious cycle.
Malnutrition and calorie deficit are associated with poor renal outcome and mortality in AKI patients. The condition is moreover complicated by changes in gut mobility, insulin resistance, and hypercatabolic state due to inflammatory mediators and neuroendocrine derangement [83]. Despite the lack of large-scale randomized controlled trials in the AKI population, early enteral nutrition should be used to preserve gut function and possibly to prevent stress ulcer hemorrhage [84, 85]. A recent multicenter, randomized controlled trial showed that early parenteral nutrition to supplement insufficient enteral nutrition does not increase the incidence of AKI, but prolongs the duration of renal replacement therapy [86]. Nutritional requirements should be individualized and frequently reassessed to avoid under- or overfeeding, azotemia, hyperglycemia, hypertriglyceridemia, electrolyte and acid-base imbalance, and fluid overload [85].
After a median follow-up period of 2.33 years, Wu et al. [87] disclosed that “recovery-AKI” was an independent predictor of long-term upper gastrointestinal bleeding, and that upper gastrointestinal bleeding was a significant risk factor of long-term mortality. The reported incidence of upper gastrointestinal hemorrhage following transient RRT-requiring AKI was about one hundred times greater than that of the general population. Peptic ulcers accounted for two-thirds of upper gastrointestinal bleeding episodes following AKI. Although AKI incites inflammation, an “immunoparalysis” state, similar to that ensuing from sepsis and critical illness [88, 89], may follow and render the effects of Helicobacter pylori more pernicious. The long-term incidence of upper gastrointestinal bleeding in patients with “recovery-AKI” (15–20 %) outnumbers the short-term incidence in critically ill patients (1–6 %) [90], suggesting the impact of AKI on the microvascular injury [91] might last long, although a compelling mechanism remains obscure. The high accumulation rates of nonsteroidal anti-inflammatory drugs and anti-platelets use after AKI in this cohort further augmented the possibility of gastrointestinal bleeding. Physicians should be more prudent about the use of ulcerogenic agents in this patient population.
Kidney-bone crosstalk
Wang et al. [92], by using a nationwide population-based cohort study, evaluated the associations between AKI and long-term risk on bone fractures. After a series of selecting and matching process, a “recovery-AKI group” containing 448 patients who developed transient RRT-requiring AKI for less than 90 days and who didn’t have diagnosis of bone fracture, and a “no-AKI group” containing 1,792 propensity score-matched individuals (with 1:4 ratio) without AKI or RRT were identified. Comparing with the “no-AKI group”, those in “recovery-AKI group” had 6.5 folds higher risk of developing bone fracture in a mean follow-up period of 3.9 years. Even after adjustment with other covariates, AKI is still independently associated with higher risk of bone fracture irrespective of subsequent development of ESRD. Long‐term bone fractures may also negatively impact patient mortality.
AKI is thought as a renowned predecessor of CKD [93] because the pathological changes of renal osteodystrophy occur earlier than previously expected CKD stages [94], and dysregulated mineral hormones also occur in AKI. It is plausible that earlier changes in vitamin D metabolites and/or fibroblast growth factor (FGF)-23 levels during AKI are responsible for the subsequent bone structural abnormalities [92]. Besides, some risk factors identified to predict bone fracture in the study, such as peripheral vascular disease and neurologic problems, are also at least partly related to AKI. The results from the study additionally offer an insight into the impact of bone disease [92].
Kidney-hepatic crosstalk
Though the clinical evidence of the association between acute liver injury and AKI is well documented, the mechanisms and pathways between kidney-hepatic crosstalk remains to be investigated [95]. An experimental study showed that hepatic ischemic/reperfusion injury (HIRI) abrupt increases multiple cytoprotective proteins, such as neutrophil gelatinase-associated lipocalin (NGAL), heme oxygenase-1 and hepcidin, inducing a renal cortical “stress response” [96]. Though modest azotemia occurs, the HIRI-induced azotemia appears to a pre-renal state rather than an intrinsic renal damage. Thus, despite clinical evidence of acute liver injury predispose to AKI, it seems plausible that AKI contributes to subsequent liver damage more directly. Growing evidence showed that AKI has significant effect on liver inflammatory response, as well as drug or other nutrient metabolism, and even patient outcomes [19]. Experimental studies showed that AKI results in increased vascular permeability, neutrophil and T-lymphocyte infiltration in the liver [18]. Besides, AKI activates oxidative stress, decreases antioxidants level and upregulate the expression of injury-promoting molecules, leading to apoptosis and tissue damage of hepatocytes [30, 97]. Among the related cytokines, IL-6 is a well-known one induced in AKI and could activate Kuffer cell to further produce other inflammatory cytokines including IL-10 [98]. As to the results of clinical studies, an analysis from a randomized control study found that the occurrence of a subsequent AKI would increase mortality rate from 28 % to 58 % among patients with acute liver injury [99].
Kidney-malignancy
A nationwide population study using 1,000,000 representative database during 2000–2008 was conducted by Chao et al. [100] who identified 623 individuals recovering from RRT-requiring AKI (recovery-AKI group) and 623 patients developing ESRD during follow-up (non-recovery AKI group), along with an age, sex, and diabetes status-matched control group (non-AKI group). After a mean follow-up period of 3.7 years, the standardized incidence ratios of all cancers are higher in both recovery-AKI group (1.21) and non-recovery AKI group (1.31) when using general population as reference. And the incidences of de novo malignancy were gradually increased from “no-AKI group”, “recovery-AKI group”, to “non-recovery AKI group” (2.6, 2.9, and 4.2 per 100 person-year, respectively). Overall speaking digestive tract (4.9 %), Genitourinary tract (3.0 %), and respiratory tract (1.7 %) were the top three sites of de novo cancers occurrence. Comparing with the “recovery-AKI group”, the “no-AKI group” had lower risk (HR, 0.66) while the “non-recovery AKI group” had higher risk (HR, 1.44) of developing malignancy.
This study demonstrates patients with non-recovery AKI developed more genitourinary cancers (5.1 %), while recovery patients developed more respiratory tract cancers (2.2 %) in the long run. The relationship presumably includes viral carcinogenesis, uremic immune suppression, and toxin exposure. The acute or chronic inflammation and the ensuing regeneration processes might carry the possibility of promoting the subsequent uncontrollable proliferation and neoplasm formation [50]. The increase in protein binding uremic toxin during AKI also could lead to epigenetic modification and potentially increases chances of tumor-suppressor gene silencing [66, 101]. This study shows patients requiring even temporary RRT have higher long-term risk of developing cancers, independent of subsequent progression to CKD and ESRD.
Discussion
In the current review, the development of severe AKI requiring RRT is found to have significant impact on long-term morbidities of distant organs. These epidemiological findings in large-scaled population studies echo and add much strength to the proposed underlying mechanisms and involved pathways in organ crosstalk of AKI. Besides, Pickering et al. [102] evaluated trial outcomes using mathematic modeling of serum creatinine (SCr) changes in AKI, and found that the “time of SCr elevation” (duration of AKI) is associated with an efficient outcome-predictive power. These could explain the impact of recovery status on patient outcomes. From the nationwide population studies comparing the effects from AKI with different recovery status (recovery versus non-recovery AKI) [68, 87, 100, 103], the “AKI duration”-dependent effect of long-term distant organ injury from RRT-requiring AKI represent its real impact.
Similar results were also revealed among patients with less severe form of AKI not requiring RRT support, no matter the study focused on diabetic population [104] or not [105]. The findings indicated that the AKI per se, beside RRT, speaks for itself. Recently, a retrospective multicenter study enrolling 447 critically-ill patients from six intensive care units evaluated the impact of duration (transient and persistent AKI) and severity of AKI (stage 3 AKI) on patient outcomes [106]. After adjustment with all confounding factors, “persistent AKI” was found as an independent factor associated with worse hospital survival. However, when “stage 3 AKI” was put into the final multivariate medel, “stage 3 AKI” replaced “persistent AKI” as an independent factor with lower survival. The findings are interesting and may be interpreted that “severity of AKI” is more relevant than “duration of AKI” in influencing patient prognosis.
An episode of AKI is proven to result in prolonged impairment of renal blood flow and clearance even the SCr has apparently returned to baseline [107]. Maladaptive repair after AKI, which is characterized by persistent parenchymal inflammation with increased numbers of myofibroblasts and accumulation of extracellular matrix, may lead to CKD. And the risk factors for the maladaptive repair response include the type and duration of injury [108].
The exact causative association between AKI and the long-term distant organ injury risks is still not clearly recognized [109]. Nonetheless, when the risk factors that had engendered an AKI event may persist [110] and concomitantly or subsequently lead to distant organ damage without direct causal association between the past CKD. Cytokine surge during AKI is at least partly resulted from subsequent impaired filtration and clearance of uremic toxins, and its impact is thought to attribute to the remote damage between kidney and distant organs [18]. Although it is seemingly intuitive that the duration of AKI would be positively associated with remote organ damage, the direct evidence addressing this is lacking.
The findings from aforementioned studies raise the possibility that AKI might trigger a cascade of perturbations which are not completely resolved. And certain non-traditional risk factors, such as impaired endothelial progenitor cells, endothelial dysfunction, inflammatory response, oxidative stress, hyper-homocysteinemia, and thrombogenic factors during AKI, are involved in the he pathogenic mechanisms [111, 112]. These risk factors may play a role in accelerated atherosclerosis in the arteries of both the kidney and remote organs, making AKI a non-modifiable entity. Besides, the RRT hemofiltrate from AKI patients inhibited in vitro neutrophil chemotaxis, oxidative metabolism, and apoptosis, which could favorably affect endothelial evolution [113]. Taken together, AKI, in addition to the traditional cardiovascular equivalent, serves as a “kidney specific” risk factor associated with distant organ injury.
Since AKI is known as a contributing factor to late-stage CKD, it is possible that early kidney changes involving endothelial phenotypic transition may have already taken place during acute events, paving the way toward progressive renal function deterioration. Recently, FGF-23, a novel regulator of mineral metabolism which is markedly elevated in AKI [114], is regarded as an index of subclinical cardiovascular pathology and associated with adverse cardiovascular outcome [115]. Likewise, the expression of NGAL, a marker of renal tubular injury, is also related to increased cardiovascular and all-cause mortality independent of traditional cardiovascular risk factors [116].
Besides the concept of organ crosstalk during AKI that AKI itself could cause a number of systemic vascular endothelial alterations which impact cardiovascular health [109], some possible explanations for the remote organ injury from recoverable AKI are summarized below. First, AKI may serve as a surrogate of other end-organ damages. A recoverable AKI may be a less severe AKI event which itself does not cause damage but merely reflects a sicker patient population who have less renal reserve and more subsequent medical complications. Second, regardless renal recovery status, AKI patients had higher probability to be hospitalized for a longer duration than those without AKI, thus may get higher risks of medical complications [105].
Among the managements of AKI-related remote organ consequences, early identifying and stratifying patient in risk, as well as preventive measures to avoid the occurrence and evolution of AKI are the most important strategy. Over the past decade, many novel biomarkers with important biological function in the pathogenesis of AKI were identified and validated. Generally speaking, the biomarkers of AKI are categorized into three groups, namely, functional biomarkers (such as SCr, cystatin C, α1- or β2-microglobulin), tubular enzymes (such as α-glutathione-S-transferase (α-GST)), and unregulated proteins (such as NGAL, L-type fatty acid-binding protein (L-FABP), kidney injury molecule-1 (KIM-1) and IL-18) [117].
A rapidly elevated urine concentration of NGAL, L-FABP, α-GST, KIM-1, and IL-18 is indicative of AKI, achieving an early detection of AKI about 24 to 48 hours before the rise of SCr level [118]. According to the varied characteristic of individual biomarker along with the concentration change in serum and urine sample, the biomarkers are also valuable in making differential diagnosis of AKI among the critically ill patients [119]. Besides, the elevated level of some biomarkers are of important prognostic value. An early assessment of prognosis may result in better outcomes [119].
Since cytokines and chemokines were thought to play important roles in the organ crosstalk in AKI [18, 19, 21, 30, 39], it is reasonable to consider “removing cytokines/chemokines” as a potential management strategy to preventing remote organ damage following AKI. Although hemofiltration could remove inflammatory cytokines, it does not affect patient mortality rates regardless the amount of applied dosage among the patients with septic shock in which inflammatory mediators contribute to patients outcomes [120]. Actually, standard dialysis membrane could only remove limited amount of cytokines even with high volume hemofiltration [121]. A kind of recently-developed dialysis membranes with moderately larger pore size, called high cutoff membranes, is found to have better effectiveness in removing cytokines than standard membranes and associated with better immunologic function and survival in experimental models of sepsis [17, 122]. Besides, “coupled plasma filtration and adsorption” is found to improve function of immunity and circulating leukocytes in septic shock [123], while “polymycin B hemoperfusion” is suggestive of beneficial effect on arterial pressure, gas exchange, and mortality [124]. However, the evidence exactly focusing on the association between RRT and remote organ consequence is lacking. Further large-scaled, prospective study is warranted to evaluated the association among RRT intervention, cytokines/chemokines/oxidative stress, and remote organs injury, in AKI patients undergoing optimized RRT in a way that the multiple negative effects of the acute uremic state are mitigated.
Conclusion
In conclusion, an increasing body of research demonstrated the organ crosstalk during AKI has significant impact on long-term distant organ-system comorbidities, the impact persist despite subsequent renal function recovery. Recognizing key biomarkers of inflammation as novel therapeutic targets may improve the quality of diagnosis and therapy since cytokines and chemokines play important roles in the distant organ injury during AKI. Besides, optimizing RRT for remove certain cytokines, as well as decreasing inflammatory and acute uremic status may probably be a useful strategy to avoid distant organ injury.
Abbreviations
- AKI:
-
acute kidney injury
- α-GST:
-
α-glutathione-S-transferase
- CKD:
-
chronic kidney disease
- ESRD:
-
end-stage renal disease
- FGF:
-
fibroblast growth factor
- HIRI:
-
hepatic ischemic/reperfusion injury
- HR:
-
hazard ratio
- IL:
-
interleukin
- KIM-1:
-
kidney injury molecule-1
- L-FABP:
-
L-type fatty acid-binding protein
- NGAL:
-
neutrophil gelatinase-associated lipocalin
- PRES:
-
posterior reversible encephalopathy syndrome
- RRT:
-
renal replacement therapy
- SCr:
-
serum creatinine
- TGF:
-
transforming growth factor
References
Waikar SS, Wald R, Chertow GM, Curhan GC, Winkelmayer WC, Liangos O, et al. Validity of international classification of diseases, ninth revision, clinical modification codes for acute renal failure. J Am Soc Nephrol. 2006;17(6):1688–94.
Bagshaw SM, Laupland KB, Doig CJ, Mortis G, Fick GH, Mucenski M, et al. Prognosis for long-term survival and renal recovery in critically ill patients with severe acute renal failure: a population-based study. Crit Care. 2005;9(6):R700–709.
Ali T, Khan I, Simpson W, Prescott G, Townend J, Smith W, et al. Incidence and outcomes in acute kidney injury: a comprehensive population-based study. J Am Soc Nephrol. 2007;18(4):1292–8.
Bagshaw SM, George C, Bellomo R. Changes in the incidence and outcome for early acute kidney injury in a cohort of Australian intensive care units. Crit Care. 2007;11(3):R68.
Cerda J, Lameire N, Eggers P, Pannu N, Uchino S, Wang H, et al. Epidemiology of acute kidney injury. Clin J Am Soc Nephrol. 2008;3(3):881–6.
Hoste EA, Clermont G, Kersten A, Venkataraman R, Angus DC, De Bacquer D, et al. RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis. Crit Care. 2006;10(3):R73.
Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294(7):813–8.
Ishani A, Xue JL, Himmelfarb J, Eggers PW, Kimmel PL, Molitoris BA, et al. Acute kidney injury increases risk of ESRD among elderly. J Am Soc Nephrol. 2009;20(1):223–8.
Pannu N, James M, Hemmelgarn B, Klarenbach S. Association between AKI, recovery of renal function, and long-term outcomes after hospital discharge. Clin J Am Soc Nephrol. 2013;8(2):194–202.
Wu VC, Shiao CC, Chang CH, Huang TM, Lai CF, Lin MC, et al. Long-term outcomes after dialysis-requiring acute kidney injury. Biomed Res Int. 2014;2014:365186.
Wu VC, Huang TM, Lai CF, Shiao CC, Lin YF, Chu TS, et al. Acute-on-chronic kidney injury at hospital discharge is associated with long-term dialysis and mortality. Kidney Int. 2011;80(11):1222–30.
Wu VC, Wu CH, Huang TM, Wang CY, Lai CF, Shiao CC, et al. Long-term risk of coronary events after AKI. J Am Soc Nephrol. 2014;25(3):595–605.
Li PK, Burdmann EA, Mehta RL. World Kidney Day 2013: acute kidney injury-global health alert. Am J Kidney Dis. 2013;61(3):359–63.
Waikar SS, Curhan GC, Wald R, McCarthy EP, Chertow GM. Declining mortality in patients with acute renal failure, 1988 to 2002. J Am Soc Nephrol. 2006;17(4):1143–50.
Xue JL, Daniels F, Star RA, Kimmel PL, Eggers PW, Molitoris BA, et al. Incidence and mortality of acute renal failure in Medicare beneficiaries, 1992 to 2001. J Am Soc Nephrol. 2006;17(4):1135–42.
Mehta RL, Pascual MT, Soroko S, Savage BR, Himmelfarb J, Ikizler TA, et al. Spectrum of acute renal failure in the intensive care unit: the PICARD experience. Kidney Int. 2004;66(4):1613–21.
Ronco C, Ricci Z, De Backer D, Kellum JA, Taccone FS, Joannidis M, et al. Renal replacement therapy in acute kidney injury: controversy and consensus. Crit Care. 2015;19(1):146.
Ologunde R, Zhao H, Lu K, Ma D. Organ cross talk and remote organ damage following acute kidney injury. Int Urol Nephrol. 2014;46(12):2337–45.
Lane K, Dixon JJ, MacPhee IA, Philips BJ. Renohepatic crosstalk: does acute kidney injury cause liver dysfunction? Nephrol Dial Transplant. 2013;28(7):1634–47.
Rabb H, Chamoun F, Hotchkiss J. Molecular mechanisms underlying combined kidney-lung dysfunction during acute renal failure. Contrib Nephrol. 2001;132:41–52.
Grams ME, Rabb H. The distant organ effects of acute kidney injury. Kidney Int. 2012;81(10):942–8.
Klein CL, Hoke TS, Fang WF, Altmann CJ, Douglas IS, Faubel S. Interleukin-6 mediates lung injury following ischemic acute kidney injury or bilateral nephrectomy. Kidney Int. 2008;74(7):901–9.
Liu M, Liang Y, Chigurupati S, Lathia JD, Pletnikov M, Sun Z, et al. Acute kidney injury leads to inflammation and functional changes in the brain. J Am Soc Nephrol. 2008;19(7):1360–70.
Hassoun HT, Grigoryev DN, Lie ML, Liu M, Cheadle C, Tuder RM, et al. Ischemic acute kidney injury induces a distant organ functional and genomic response distinguishable from bilateral nephrectomy. Am J Physiol Renal Physiol. 2007;293(1):F30–40.
Levy EM, Viscoli CM, Horwitz RI. The effect of acute renal failure on mortality. A cohort analysis. JAMA. 1996;275(19):1489–94.
Liangos O, Kolyada A, Tighiouart H, Perianayagam MC, Wald R, Jaber BL. Interleukin-8 and acute kidney injury following cardiopulmonary bypass: a prospective cohort study. Nephron Clin Pract. 2009;113(3):c148–154.
de Mendonca A, Vincent JL, Suter PM, Moreno R, Dearden NM, Antonelli M, et al. Acute renal failure in the ICU: risk factors and outcome evaluated by the SOFA score. Intensive Care Med. 2000;26(7):915–21.
Metnitz PG, Krenn CG, Steltzer H, Lang T, Ploder J, Lenz K, et al. Effect of acute renal failure requiring renal replacement therapy on outcome in critically ill patients. Crit Care Med. 2002;30(9):2051–8.
Kelly KJ. Acute renal failure: much more than a kidney disease. Semin Nephrol. 2006;26(2):105–13.
Druml W. Systemic consequences of acute kidney injury. Curr Opin Crit Care. 2014;20(6):613–9.
Vaara ST, Korhonen AM, Kaukonen KM, Nisula S, Inkinen O, Hoppu S, et al. Fluid overload is associated with an increased risk for 90-day mortality in critically ill patients with renal replacement therapy: data from the prospective FINNAKI study. Crit Care. 2012;16(5):R197.
Silva RC, Landgraf MA, Correa-Costa M, Semedo P, Cenedeze MA, Pacheco-Silva A, et al. Acute kidney injury reduces phagocytic and microbicidal capacities of alveolar macrophages. Cell Physiol Biochem. 2013;31(2-3):179–88.
Mehta RL, Bouchard J, Soroko SB, Ikizler TA, Paganini EP, Chertow GM, et al. Sepsis as a cause and consequence of acute kidney injury: Program to Improve Care in Acute Renal Disease. Intensive Care Med. 2011;37(2):241–8.
Bolisetty S, Zarjou A, Hull TD, Traylor AM, Perianayagam A, Joseph R, et al. Macrophage and epithelial cell H-ferritin expression regulates renal inflammation. Kidney Int. 2015;88(1):95–108.
Scindia Y, Dey P, Thirunagari A, Liping H, Rosin DL, Floris M, et al. Hepcidin mitigates renal ischemia-reperfusion injury by modulating systemic iron homeostasis. J Am Soc Nephrol. 2015;26(11):2800–14.
Grigoryev DN, Liu M, Hassoun HT, Cheadle C, Barnes KC, Rabb H. The local and systemic inflammatory transcriptome after acute kidney injury. J Am Soc Nephrol. 2008;19(3):547–58.
Hoke TS, Douglas IS, Klein CL, He Z, Fang W, Thurman JM, et al. Acute renal failure after bilateral nephrectomy is associated with cytokine-mediated pulmonary injury. J Am Soc Nephrol. 2007;18(1):155–64.
Zager RA, Johnson AC, Lund S, Hanson S. Acute renal failure: determinants and characteristics of the injury-induced hyperinflammatory response. Am J Physiol Renal Physiol. 2006;291(3):F546–556.
Yap SC, Lee HT. Acute kidney injury and extrarenal organ dysfunction: new concepts and experimental evidence. Anesthesiology. 2012;116(5):1139–48.
Bellomo R, Kellum JA, Ronco C. Acute kidney injury. Lancet. 2012;380(9843):756–66.
Elseviers MM, Lins RL, Van der Niepen P, Hoste E, Malbrain ML, Damas P, et al. Renal replacement therapy is an independent risk factor for mortality in critically ill patients with acute kidney injury. Crit Care. 2010;14(6):R221.
Oudemans-van Straaten HM, Kellum JA, Bellomo R. Clinical review: anticoagulation for continuous renal replacement therapy--heparin or citrate? Crit Care. 2011;15(1):202.
Kajimoto K, Sato N, Keida T, Sakata Y, Takano T, Acute Decompensated Heart Failure Syndromes I. Associations of anemia and renal dysfunction with outcomes among patients hospitalized for acute decompensated heart failure with preserved or reduced ejection fraction. Clin J Am Soc Nephrol. 2014;9(11):1912–21.
Marenzi G, Cabiati A, Cosentino N, Assanelli E, Milazzo V, Rubino M, et al. Prognostic significance of serum creatinine and its change patterns in patients with acute coronary syndromes. Am Heart J. 2015;169(3):363–70.
Aronson D, Abassi Z, Allon E, Burger AJ. Fluid loss, venous congestion, and worsening renal function in acute decompensated heart failure. Eur J Heart Fail. 2013;15(6):637–43.
Weinfeld MS, Chertow GM, Stevenson LW. Aggravated renal dysfunction during intensive therapy for advanced chronic heart failure. Am Heart J. 1999;138(2 Pt 1):285–90.
Firth JD, Raine AE, Ledingham JG. Raised venous pressure: a direct cause of renal sodium retention in oedema? Lancet. 1988;1(8593):1033–5.
Ronco C, Haapio M, House AA, Anavekar N, Bellomo R. Cardiorenal syndrome. J Am Coll Cardiol. 2008;52(19):1527–39.
Ljungman S, Laragh JH, Cody RJ. Role of the kidney in congestive heart failure. Relationship of cardiac index to kidney function. Drugs. 1990;39 Suppl 4:10–21. discussion 22-14.
Kelly KJ. Distant effects of experimental renal ischemia/reperfusion injury. J Am Soc Nephrol. 2003;14(6):1549–58.
Bhalodia YS, Sheth NR, Vaghasiya JD, Jivani NP. Homocysteine-dependent endothelial dysfunction induced by renal ischemia/reperfusion injury. J Nephrol. 2011;24(5):631–5.
Kelly KJ, Meehan SM, Colvin RB, Williams WW, Bonventre JV. Protection from toxicant-mediated renal injury in the rat with anti-CD54 antibody. Kidney Int. 1999;56(3):922–31.
Virzi G, Day S, de Cal M, Vescovo G, Ronco C. Heart-kidney crosstalk and role of humoral signaling in critical illness. Crit Care. 2014;18(1):201.
Ko T, Higashitani M, Sato A, Uemura Y, Norimatsu T, Mahara K, et al. Impact of acute kidney injury on early to long-term outcomes in patients who underwent surgery for type a acute aortic dissection. Am J Cardiol. 2015;116(3):463–8.
Mitchell AM, Kline JA, Jones AE, Tumlin JA. Major adverse events one year after acute kidney injury after contrast-enhanced computed tomography. Ann Emerg Med. 2015;66(3):267–274.e4.
Lull ME, Block ML. Microglial activation and chronic neurodegeneration. Neurotherapeutics. 2010;7(4):354–65.
Loh HH, Tan CH. Acute renal failure and posterior reversible encephalopathy syndrome following multiple wasp stings: a case report. Med J Malaysia. 2012;67(1):133–5.
Kim SM, Choi H, Kim Y, Shin J, Jang HR, Lee JE, et al. Posterior reversible encephalopathy syndrome during recovery from acute kidney injury after hepatitis a infection. Case Rep Nephrol Urol. 2012;2(1):33–7.
de Vries DK, Lindeman JH, Ringers J, Reinders ME, Rabelink TJ, Schaapherder AF. Donor brain death predisposes human kidney grafts to a proinflammatory reaction after transplantation. Am J Transplant. 2011;11(5):1064–70.
Wu VC, Wu PC, Wu CH, Huang TM, Chang CH, Tsai PR, et al. The impact of acute kidney injury on the long-term risk of stroke. J Am Heart Assoc 2014, 3(4). doi:10.1161/JAHA.114.000933.
Guerra C, Linde-Zwirble WT, Wunsch H. Risk factors for dementia after critical illness in elderly Medicare beneficiaries. Crit Care. 2012;16(6):R233.
Pandharipande PP, Girard TD, Jackson JC, Morandi A, Thompson JL, Pun BT, et al. Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306–16.
Burne-Taney MJ, Yokota N, Rabb H. Persistent renal and extrarenal immune changes after severe ischemic injury. Kidney Int. 2005;67(3):1002–9.
Ascon M, Ascon DB, Liu M, Cheadle C, Sarkar C, Racusen L, et al. Renal ischemia-reperfusion leads to long term infiltration of activated and effector-memory T lymphocytes. Kidney Int. 2009;75(5):526–35.
Sun CY, Hsu HH, Wu MS. p-Cresol sulfate and indoxyl sulfate induce similar cellular inflammatory gene expressions in cultured proximal renal tubular cells. Nephrol Dial Transplant. 2013;28(1):70–8.
Wu VC, Young GH, Huang PH, Lo SC, Wang KC, Sun CY, et al. In acute kidney injury, indoxyl sulfate impairs human endothelial progenitor cells: modulation by statin. Angiogenesis. 2013;16(3):609–24.
Lai TS, Wang CY, Pan SC, Huang TM, Lin MC, Lai CF, et al. Risk of developing severe sepsis after acute kidney injury: a population-based cohort study. Crit Care. 2013;17(5):R231.
Wu VC, Wang CY, Shiao CC, Chang CH, Huang HY, Huang TM, et al. Increased risk of active tuberculosis following acute kidney injury: a nationwide population-based study. PLoS One. 2013;8(7), e69556.
Dalboni MA, Quinto BM, Grabulosa CC, Narciso R, Monte JC, Durao Jr M, et al. Tumour necrosis factor-alpha plus interleukin-10 low producer phenotype predicts acute kidney injury and death in intensive care unit patients. Clin Exp Immunol. 2013;173(2):242–9.
Susantitaphong P, Perianayagam MC, Tighiouart H, Liangos O, Bonventre JV, Jaber BL. Tumor necrosis factor alpha promoter polymorphism and severity of acute kidney injury. Nephron Clin Pract. 2013;123(1-2):67–73.
Grabulosa CC, Batista MC, Cendoroglo M, Quinto BM, Narciso R, Monte JC, et al. Frequency of TGF- beta and IFN- gamma genotype as risk factors for acute kidney injury and death in intensive care unit patients. BioMed Res Int. 2014;2014:904730.
Lee DH, Park MH, Hwang CJ, Hwang JY, Yoon HS, Yoon DY, et al. CCR5 deficiency increased susceptibility to lipopolysaccharide-induced acute renal injury. Arch Toxicol. 2015 [Epub ahead of print].
Phillips SA, Pechman KR, Leonard EC, Friedrich JL, Bian JT, Beal AG, et al. Increased ANG II sensitivity following recovery from acute kidney injury: role of oxidant stress in skeletal muscle resistance arteries. Am J Physiol Regul Integr Comp Physiol. 2010;298(6):R1682–1691.
Amura CR, Renner B, Lyubchenko T, Faubel S, Simonian PL, Thurman JM. Complement activation and toll-like receptor-2 signaling contribute to cytokine production after renal ischemia/reperfusion. Mol Immunol. 2012;52(3-4):249–57.
Chen J, Hartono JR, John R, Bennett M, Zhou XJ, Wang Y, et al. Early interleukin 6 production by leukocytes during ischemic acute kidney injury is regulated by TLR4. Kidney Int. 2011;80(5):504–15.
Andres-Hernando A, Dursun B, Altmann C, Ahuja N, He Z, Bhargava R, et al. Cytokine production increases and cytokine clearance decreases in mice with bilateral nephrectomy. Nephrol Dial Transplant. 2012;27(12):4339–47.
Ahuja N, Andres-Hernando A, Altmann C, Bhargava R, Bacalja J, Webb RG, et al. Circulating IL-6 mediates lung injury via CXCL1 production after acute kidney injury in mice. Am J Physiol Renal Physiol. 2012;303(6):F864–872.
Andres-Hernando A, Altmann C, Ahuja N, Lanaspa MA, Nemenoff R, He Z, et al. Splenectomy exacerbates lung injury after ischemic acute kidney injury in mice. Am J Physiol Renal Physiol. 2011;301(4):F907–916.
Esteve E, Castro A, Lopez-Bermejo A, Vendrell J, Ricart W, Fernandez-Real JM. Serum interleukin-6 correlates with endothelial dysfunction in healthy men independently of insulin sensitivity. Diabetes Care. 2007;30(4):939–45.
Simmons EM, Himmelfarb J, Sezer MT, Chertow GM, Mehta RL, Paganini EP, et al. Plasma cytokine levels predict mortality in patients with acute renal failure. Kidney Int. 2004;65(4):1357–65.
Lautenschlager I, Dombrowsky H, Frerichs I, Kuchenbecker SC, Bade S, Schultz H, et al. A model of the isolated perfused rat small intestine. Am J Physiol Gastrointest Liver Physiol. 2010;298(2):G304–313.
White LE, Hassoun HT. Inflammatory mechanisms of organ crosstalk during ischemic acute kidney injury. Int J Nephrol. 2012;2012:505197.
Casaer MP, Mesotten D, Schetz MR. Bench-to-bedside review: metabolism and nutrition. Crit Care. 2008;12(4):222.
Hurt RT, Frazier TH, McClave SA, Crittenden NE, Kulisek C, Saad M, et al. Stress prophylaxis in intensive care unit patients and the role of enteral nutrition. JPEN J Parenter Enteral Nutr. 2012;36(6):721–31.
McCarthy MS, Phipps SC. Special nutrition challenges: current approach to acute kidney injury. Nutr Clin Pract. 2014;29(1):56–62.
Gunst J, Vanhorebeek I, Casaer MP, Hermans G, Wouters PJ, Dubois J, et al. Impact of early parenteral nutrition on metabolism and kidney injury. J Am Soc Nephrol. 2013;24(6):995–1005.
Wu PC, Wu CJ, Lin CJ, Wu VC. Long-term risk of upper gastrointestinal hemorrhage after advanced AKI. Clin J Am Soc Nephrol. 2015;10(3):353–62.
Murray CJ, Richards MA, Newton JN, Fenton KA, Anderson HR, Atkinson C, et al. UK health performance: findings of the Global Burden Of Disease Study 2010. Lancet. 2013;381(9871):997–1020.
Sundar KM, Sires M. Sepsis induced immunosuppression: Implications for secondary infections and complications. Indian J Crit Care Med. 2013;17(3):162–9.
Bardou M, Quenot JP, Barkun A. Stress-related mucosal disease in the critically ill patient. Nat Rev Gastroenterol Hepatol. 2015;12(2):98–107.
Cook D, Heyland D, Griffith L, Cook R, Marshall J, Pagliarello J. Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. Crit Care Med. 1999;27(12):2812–7.
Wang WJ, Chao CT, Huang YC, Wang CY, Chang CH, Huang TM, et al. The impact of acute kidney injury with temporary dialysis on the risk of fracture. J Bone Miner Res. 2014;29(3):676–84.
Goldstein SL, Jaber BL, Faubel S, Chawla LS. AKI transition of care: a potential opportunity to detect and prevent CKD. Clin J Am Soc Nephrol. 2013;8(3):476–83.
Hamdy NA, Kanis JA, Beneton MN, Brown CB, Juttmann JR, Jordans JG, et al. Effect of alfacalcidol on natural course of renal bone disease in mild to moderate renal failure. BMJ. 1995;310(6976):358–63.
Francoz C, Glotz D, Moreau R, Durand F. The evaluation of renal function and disease in patients with cirrhosis. J Hepatol. 2010;52(4):605–13.
Zager RA, Johnson AC, Frostad KB. Acute hepatic ischemic-reperfusion injury induces a renal cortical “stress response,” renal “cytoresistance,” and an endotoxin hyperresponsive state. Am J Physiol Renal Physiol. 2014;307(7):F856–868.
Golab F, Kadkhodaee M, Zahmatkesh M, Hedayati M, Arab H, Schuster R, et al. Ischemic and non-ischemic acute kidney injury cause hepatic damage. Kidney Int. 2009;75(8):783–92.
Deng J, Kohda Y, Chiao H, Wang Y, Hu X, Hewitt SM, et al. Interleukin-10 inhibits ischemic and cisplatin-induced acute renal injury. Kidney Int. 2001;60(6):2118–28.
Liu KD, Glidden DV, Eisner MD, Parsons PE, Ware LB, Wheeler A, et al. Predictive and pathogenetic value of plasma biomarkers for acute kidney injury in patients with acute lung injury. Crit Care Med. 2007;35(12):2755–61.
Chao CT, Wang CY, Lai CF, Huang TM, Chen YY, Kao TW, et al. Dialysis-requiring acute kidney injury increases risk of long-term malignancy: a population-based study. J Cancer Res Clin Oncol. 2014;140(4):613–21.
Young GH, Wu VC. KLOTHO methylation is linked to uremic toxins and chronic kidney disease. Kidney Int. 2012;81(7):611–2.
Pickering JW, Frampton CM, Endre ZH. Evaluation of trial outcomes in acute kidney injury by creatinine modeling. Clin J Am Soc Nephrol. 2009;4(11):1705–15.
Lai TS, Wang CY, Pan SC, Huang TM, Lin MC, Lai CF, et al. Risk of developing severe sepsis after acute kidney injury: a population-based cohort study. Crit Care. 2013;17(5):R231.
Coca SG, King Jr JT, Rosenthal RA, Perkal MF, Parikh CR. The duration of postoperative acute kidney injury is an additional parameter predicting long-term survival in diabetic veterans. Kidney Int. 2010;78(9):926–33.
Brown JR, Kramer RS, Coca SG, Parikh CR. Duration of acute kidney injury impacts long-term survival after cardiac surgery. Ann Thorac Surg. 2010;90(4):1142–8.
Perinel S, Vincent F, Lautrette A, Dellamonica J, Mariat C, Zeni F, et al. Transient and persistent acute kidney injury and the risk of hospital mortality in critically Ill patients: results of a multicenter cohort study. Crit Care Med. 2015;43(8):e269–275.
Hall JW, Johnson WJ, Maher FT, Hunt JC. Immediate and long-term prognosis in acute renal failure. Ann Intern Med. 1970;73(4):515–21.
Chawla LS, Kimmel PL. Acute kidney injury and chronic kidney disease: an integrated clinical syndrome. Kidney Int. 2012;82(5):516–24.
Druml W. Acute renal failure is not a “cute” renal failure! Intensive Care Med. 2004;30(10):1886–90.
Rifkin DE, Coca SG, Kalantar-Zadeh K. Does AKI truly lead to CKD? J Am Soc Nephrol. 2012;23(6):979–84.
Bonventre JV. Pathophysiology of AKI: injury and normal and abnormal repair. Contrib Nephrol. 2010;165:9–17.
Sun J, Shannon M, Ando Y, Schnackenberg LK, Khan NA, Portilla D, et al. Serum metabolomic profiles from patients with acute kidney injury: a pilot study. J Chromatogr B Analyt Technol Biomed Life Sci. 2012;893–894:107–13.
Cohen G, Horl WH. Retinol binding protein isolated from acute renal failure patients inhibits polymorphonuclear leucocyte functions. Eur J Clin Invest. 2004;34(11):774–81.
Leaf DE, Wolf M, Stern L. Elevated FGF-23 in a patient with rhabdomyolysis-induced acute kidney injury. Nephrol Dial Transplant. 2010;25(4):1335–7.
Arnlov J, Carlsson AC, Sundstrom J, Ingelsson E, Larsson A, Lind L, et al. Serum FGF23 and risk of cardiovascular events in relation to mineral metabolism and cardiovascular pathology. Clin J Am Soc Nephrol. 2013;8(5):781–6.
Helmersson-Karlqvist J, Larsson A, Carlsson AC, Venge P, Sundstrom J, Ingelsson E, et al. Urinary neutrophil gelatinase-associated lipocalin (NGAL) is associated with mortality in a community-based cohort of older Swedish men. Atherosclerosis. 2013;227(2):408–13.
Charlton JR, Portilla D, Okusa MD. A basic science view of acute kidney injury biomarkers. Nephrol Dial Transplant. 2014;29(7):1301–11.
Doi K, Negishi K, Ishizu T, Katagiri D, Fujita T, Matsubara T, et al. Evaluation of new acute kidney injury biomarkers in a mixed intensive care unit. Crit Care Med. 2011;39(11):2464–9.
McCullough PA, Bouchard J, Waikar SS, Siew ED, Endre ZH, Goldstein SL, et al. Implementation of novel biomarkers in the diagnosis, prognosis, and management of acute kidney injury: executive summary from the tenth consensus conference of the Acute Dialysis Quality Initiative (ADQI). Contrib Nephrol. 2013;182:5–12.
Joannes-Boyau O, Honore PM, Perez P, Bagshaw SM, Grand H, Canivet JL, et al. High-volume versus standard-volume haemofiltration for septic shock patients with acute kidney injury (IVOIRE study): a multicentre randomized controlled trial. Intensive Care Med. 2013;39(9):1535–46.
Lehner GF, Wiedermann CJ, Joannidis M. High-volume hemofiltration in critically ill patients: a systematic review and meta-analysis. Minerva Anestesiol. 2014;80(5):595–609.
Haase M, Bellomo R, Morgera S, Baldwin I, Boyce N. High cut-off point membranes in septic acute renal failure: a systematic review. Int J Artif Organs. 2007;30(12):1031–41.
Ronco C, Brendolan A, Lonnemann G, Bellomo R, Piccinni P, Digito A, et al. A pilot study of coupled plasma filtration with adsorption in septic shock. Crit Care Med. 2002;30(6):1250–5.
Cruz DN, Perazella MA, Bellomo R, de Cal M, Polanco N, Corradi V, et al. Effectiveness of polymyxin B-immobilized fiber column in sepsis: a systematic review. Crit Care. 2007;11(2):R47.
Acknowledgments
This work was supported by the following grants: National Science Council (NSC)-102-2314-B-002-140-MY2, NSC 101-2314-B-002-132-MY3, NSC 101-2314-B-002-085-MY3, NSC100-2314-B-002-119, and NSC-100-2314-B-002-147-MY3; National Taiwan University Hospital (NTUH)-103-082, NTUH-103-S-2467, NTUH-102-CGN03, NTUH-102-S2097, NTUH-101-M1953, and NTUH-100-N1776; and National Health Research Institute (NHRI)-PH-101-SP-09 and NHRI-PH-102-SP-09.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
CCS and VCW conceived the review topic and wrote the manuscript; PCW, TMH, TSL, WSY, CHW and CFL wrote the manuscript; TSC and KDW revised and approved the final version of the manuscript.
Authors’ information
CCS is the chief of renal division and the director of Education and Research center in Saint Mary’s Hospital Luodong, and assistant professor in Saint Mary’s Medicine, Nursing and Management College. PCW is attending physician in renal division of MacKay Memorial Hospital. TMH is attending physician in renal division of National Taiwan University Hospital Yun-Lin Branch. TSL is attending physician in renal division of National Taiwan University Hospital, Bei-Hu Branch. WSY is attending physician in renal division of National Taiwan University Hospital, Hisn-Chu Branch. CHW is attending physician in renal division of Taipei Tzu Chi Hospital. CFL is attending physician in renal division of National Taiwan University Hospital. VCW is the chief executive of National Taiwan University Study group on ARF (NSARF) and attending physician of renal division in National Taiwan University Hospital. TSC is the chief of renal division of National Taiwan University Hospital and professor in National Taiwan University medical college. KDW is attending physician in renal division of National Taiwan University Hospital and professor in National Taiwan University medical college.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Shiao, CC., Wu, PC., Huang, TM. et al. Long-term remote organ consequences following acute kidney injury. Crit Care 19, 438 (2015). https://doi.org/10.1186/s13054-015-1149-5
Published:
DOI: https://doi.org/10.1186/s13054-015-1149-5