
Abstract
Background
With the increasing incidence of asymptomatic carriers or milder symptoms, children and adolescents are likely to become a silent source of infection. In view of the efficacy and safety of vaccines in the treatment of novel Coronavirus pneumonia, population-wide vaccination will be an inevitable trend to control the spread of COVID-19. However, there is no survey on the attitudes of Chinese parents of children and adolescents towards their children’s COVID-19 vaccination.
Methods
We used online questionnaires to find out the attitudes of Chinese parents toward their children’s immunization against COVID-19. Logistic regression was used to explore the influencing factors.
Results
A total of 2019 parents participated in the survey. Overall, 74.38% parents said they would actively get vaccinated, 8.90% refused to get vaccinated, 4.60% said they would delay vaccination and 12.12% were still undecided.
Conclusions
In general, Chinese parents have a high desire to be vaccinated against COVID-19, and most parents have a positive attitude towards their children’s vaccination. However, many people still hesitate or even refuse to be vaccinated. Education background, attitudes towards children’s vaccination, children’s age, recent illness and other factors have a certain impact on Chinese parents of children and adolescents towards their children’s COVID-19 vaccination.
Similar content being viewed by others

Introduction
Novel Coronavirus infections pose a serious threat to the health and safety of the public, with over 260 million COVID-19 cases and over 5.21 million deaths worldwide as of December 1, 2021 [1]. COVID-19 has been mostly seen in adults since the outbreak, and children consistently accounted for a small proportion of the total number of coronavirus disease cases in 2019, with pediatric cases accounting for only 2% of the 80,900 COVID-19 cases during the surge in China [2, 3]. Although the majority of pediatric cases of COVID-19 are asymptomatic or mild, with a good prognosis and low mortality, novel coronavirus infection of severe acute respiratory syndrome (SARS) has been reported in children of all age groups [2, 4]. In addition, the disease may progress to multisystem inflammatory syndrome (MTIS), a life-threatening complication of COVID-19 infection [5]. Results of MTIS include myocardial dysfunction, shock, and respiratory failure and require intensive care. Study indicated that 18.4 out of 100,000 children aged 0–4 years and 10.6 out of 100,000 children aged 5–17 years required hospitalization, of which one third required intensive care.
There has recently been increasing evidence that people who are fully vaccinated with the mRNAs (BNT162b2 or mrna-1273) are less likely to develop symptomatic infections and transmit SARS coronavirus 2 (novel coronavirus) to others than those who are not vaccinated [5, 6]. Vaccines tested in young adults over the age of 12 were reported to be safe and effective, including mRNA vaccines produced by Moderna and Pfizer-Biontech [7, 8]. In addition, phase I/II clinical trial results of two inactivated Chinese vaccines produced by Sinovac and Sinopharm showed that the vaccines were well tolerated, safe and could induce humoral reactivity in children and adolescents aged 3–17 years [9]. While vaccinating children and adolescents is seen as key to ending the epidemic, Vaccine Hesitancy (VH) -- the delayed acceptance or refusal of a vaccine despite its availability -- remains a barrier to full population vaccination [5, 10]. Alfieri et al.’s study showed that 33% of parents were hesitant to vaccinate their children against COVID-19 [11]. Separate data from the US showed that 33% of parents said it was very unlikely that their children would be vaccinated against COVID-19 and 12% said they were not sure [12].
As the incidence of asymptomatic carriers is getting higher and higher, the symptoms of patients with COVID-19 infection are getting lighter and lighter, children and adolescents are likely to become a silent source of infection and remain a threat, becoming an important source of sustained transmission [5, 13]. In order for vaccines to be effective in controlling the spread of COVID-19, it is estimated that 67% of the population needs to be vaccinated to achieve herd immunity [11, 14], and a comprehensive push to vaccinate adults, children and adolescents is an inevitable trend in controlling the spread of COVID-19. In addition, for children under the age of 18, such as parents’ behaviors and values tend to have a great impact on their children. This paper mainly explores parents’ attitudes towards COVID-19 vaccination and related influencing factors, so as to provide corresponding guidance for popularizing vaccination for children and adolescents.
Method
Population and sampling
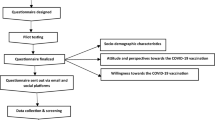
This study was a nation-wide cross-sectional study in China (Fig. 1). The ethics committee of Hangzhou Stomatological Hospital approved all the procedures performed. In November 2021, an anonymous online cross-sectional survey was conducted on Wen Juan network (https://www.wenjuan.com), set by Shanghai Zhongyan Network Technology. It is the largest free online survey platform in China, which can provide questionnaire creation, release, management, collection, and analysis services for enterprises or individuals. Their personal information can be confirmed,authentic,diverse and representative samples can be obtained. Participants are parents of Chinese children and adolescents (< 18 years old). Questionnaires were filled anonymously and 2019 copies were included apart from 131 invalid and wrong questionnaires.

The respondents of our questionnaire came from Eastern Region, Central Region, Western Region, Hong Kong region, Macau region and Taiwan region, China
Questionnaire design
Informed consent had been designed. We set that if the respondent agrees to answer, they can continue to complete the questionnaire. Otherwise they cannot continue.
This questionnaire involved the following aspects (Supplementary File 1):
the twelve basic personal information such as gender, age, family role, level of education, habitual residence, annual household income, the number, gender and age of children, insurance coverage for the children, whether a single parent family and household health care workers or not; and other five aspects of the opinions about the vaccine, for example, “Have you been vaccinated against COVID-19”, “Have your children had a history of other diseases in the last 3 months”, “Have you explained the COVID-19 vaccine to your children”,“What’s your attitude towards children’s vaccination”,“Do you think there are vaccine side effects”. The explanation for the COVID-19 vaccin is for children over the age of 3.
Statistical method
A descriptive statistical analysis was conducted on the social and demographic characteristics of the sample, and the corresponding proportion was calculated accordingly. Parental acceptability of COVID-19 vaccination was used as the dependent variable. A univariate logistic regression model first assessed the significance of the association between each of the background characteristics and the dependent variable. All relationships between the predictor and criterion variables were represented as odds ratios (OR) with 95% confidence intervals. The statistical tests were two-sided, and the effects with p < 0.05 were considered to be statistically significant. All statistical models were constructed using R software version 3.6.0 (R Foundation for Statistical Computing, version 3.6.1; http://www.Rproject.org).
Results
Demographic information
A total of 2019 valid questionnaires, and the basic information of the respondents was summarized in Table 1. Among the respondents, 738 (36.6%) were males, 1281 (63.4%) were females, and 422 (20.9%) were under the age of 30 years. 41.2% had a junior high school degree, 30.4% had a bachelor’s degree, 21.6% had a junior college degree, and the rest 6.8% had a master’s degree or above. In terms of place of residence, 10 parents came from Hong Kong, Macao and Taiwan, 1103 from central China, 139 from western China and 767 from eastern China. As for the annual household income, 26.7% of respondents reported less than 20,000 RMB per year, 22.3% between 20,000 and 50,000 RMB, 31.3% between 50,000 and 150,000 RMB, and 19.7% over 150,000 RMB. A total of 1501 parents of children and adolescents said they would be willing to be vaccinated against COVID-19 and another 518 said they would not. More than 80% of the parents had explained information about COVID-19 vaccine to their children, and more than 90% of the respondents had received COVID-19 vaccine therapy. Most (54.0%) of the children were aged 3–8, and 57.3% of them were boys. Furthermore, most children had health insurance (93.1%), with 10% having commercial insurance, 67.7% having medical insurance and 15.4% having both types of insurances.
Related factors affecting parents’ willingness to vaccinate their children against COVID-19
Several factors were taken into consideration as for parents’ wilingness (Table 2). Gender, age, place of residence, number of children in the family, gender of children, whether a single parent family or not, and whether there was a doctor in the family had no statistical significances(p > 0.05), indicating that these factors had no significant impact on parents’ willingness to vaccinate their children against COVID-19. The children with no history of other diseases (such as cold, fever, diarrhea, etc.) were more likely to be vaccinated than those with other diseases in the last 3 months (OR = 1.29;95%CI 1.24–1.36, p < 0.001). We analyzed parents’ perceptions of their children’s vaccinations. Research showed children and adolescents were less likely to be vaccinated when their parents showed refusal (OR = 0.03;95% CI 0.01–0.04), delay (OR = 0.02; 95% CI 0.01–0.04) and hesitation (OR = 0.04;95% CI 0.03–0.06) respectively comparing with children whose parents maintained positive attitudes. Parents’ perceptions of vaccine side effects also influenced children’s willingness to be vaccinated, with parents feeling that vaccines had no side effects, children were more likely to be vaccinated (OR = 1.51; 95% CI 1.42–1.73, p < 0.001). Besides, when parents were vaccinated against COVID-19, their children were more likely to be vaccinated (OR = 3.29; 95% CI 1.10–9.85, p = 0.033). Compared with uninsured children, insured children were more likely to be vaccinated, especially those with health insurances (OR = 4.00; 95% CI 2.80–5.71, p < 0.001). Children of parents with graduate education or above were also more likely to be vaccinated (OR = 0.58; 95% CI 0.39–0.85, p = 0.005).
The regional distribution of parents’ willingness to vaccinate their children against COVID-19
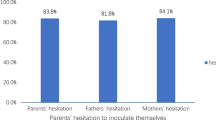
Figure 2 depicted the regional distribution of parents’ willingness to be vaccinated against COVID-19. Overall, 74.38% parents said they would actively get vaccinated for children or adolescents, 8.90% refused to get vaccinated, 4.60% said they would delay vaccination and 12.12% were still undecided. Our results showed that the willingness of parents in central China to be vaccinated was more than 75%. While the hesitation rate of parents in Hong Kong, Macao and Taiwan were 23.08%.

The regional distribution of parents’s willingness to be vaccinated against COVID-19
Discussion
This study contributed to a better understanding of parents’ attitudes towards their children’s COVID-19 vaccination. In this study, 74.38% would actively get vaccinated. Overall, Chinese parents have high willingness to vaccinate children and adolescents against COVID-19. In addition, the study found that 80.19% of parents said they would actively vaccinate their children against COVID-19, 3.37% refused to vaccinate their children, 4.95% said they would delay vaccination, and 11.49% were still hesitant. More and more evidences reveal that vaccination against COVID-19 is currently an important tool to reduce the burden of the COVID-19 epidemic. Rhodes et al. showed parents scored below the midpoint on the willingness to vaccinate their children (M = 3.55, SD = 2.13) [15]. Our research showed that nearly 15% of parents were still refusing to vaccinate their children or are hesitant to do so. Our findings are similar to the survey study from Turkey [16]. Therefore, it is necessary to conduct our questionnaire to encourage and publicize the importance of COVID-19 vaccination, so as to control the COVID-19 epidemic earlier in the world.
There is growing evidence that genetic and viral vector COVID-19 vaccines prevent not only severe disease but also asymptomatic infection [17]. And a study from the United Kingdom found that adults infected 3 weeks after receiving a dose of Pfizer-Biotech or Astrazeneca vaccine were 38 to 49% less likely to pass the virus on to their family contacts than unvaccinated individuals [18]. However, trust in vaccines is still a significant factor influencing vaccination willingness. The main reasons cited by the study for parents’ reluctance to vaccinate their children against COVID-19 included a lack of adequate scientific research (84.8%), concerns about safety and side effects (76.9%), and potential inefficacy of the vaccine due to mutations (36.7%)5. Our research suggests that parents believe the COVID-19 vaccine has no side effects, and that children are more likely to be vaccinated (OR = 1.51; 95% CI 1.42–1.73, p < 0.001). Therefore, access to more positive information about the safety and effectiveness of adolescent COVID-19 vaccines, as well as school COVID-19 vaccination requirements, are the most frequently reported factors that increase the willingness of parents and adolescents to be vaccinated [19, 20]. In addition, Marquez et al. found that 39.2% of parents refused to vaccinate their children against COVID-19, while 27.8% agreed that they would allow their children to be vaccinated against COVID-19 if their doctor recommended it20. Health workers’ advocacy of COVID-19 vaccines is one of the most important sources of reliable vaccine information for the public. Increased clear public communication about the benefits and safety of COVID-19 vaccines for children and adolescents, especially by healthcare professionals, will help increase parents’ confidence in COVID-19 vaccines and their willingness to vaccinate their children against COVID-19. Our result showed their children were more likely to be vaccinated when parents were vaccinated against COVID-19. It’s very critical to educate clear information and transparent communication from public health, governments and leaders about the safety of childhood COVID-19 vaccines [12, 21].
We analyzed the factors that may influence children’s willingness to be vaccinated against COVID-19 and found that gender, age, place of residence, number of children in the household, gender of children, whether it’s a single parent family and whether there is a doctor in the household had no significant influences on the willingness of children and adolescents to be vaccinated against COVID-19. Children who did not get sick were more likely to get vaccinated than those who had other illnesses in the last 3 months. Different from the previous studies, which showed that younger adolescents were more likely to receive COVID-19 vaccination than older adolescents [22], while our study found that older children (13–17 years old) were more likely to be vaccinated against COVID-19. This may be due to China’s implementation of the COVID-19 vaccination program by age, which partially affected the results of the study. Lack of knowledge about COVID-19 and vaccines may increase misunderstandings about COVID-19 vaccines, thereby reduce the willingness of parents to vaccinate children and adolescents.
Parents do have significant effects on their children. On the one hand, studies have found that children and adolescents are less likely to get vaccinated when their parents show signs of rejection, delay, and hesitation. Children were more likely to be vaccinated if their parents felt there were no side effects; and when their parents have been vaccinated against COVID-19, children are more likely to be vaccinated. Our study suggests that parents play a non-negligible and even decisive role in the vaccination of children and adolescents against COVID-19. Parents’ attitudes towards vaccination and their views on vaccines will affect their children’s vaccination willingness. On the other hand, research from Italy shows the lower the education level of the parents, the greater the harm they think the COVID vaccine will do to their children [23]. Our result showed children of parents with graduate education or above were more likely to be vaccinated too. Therefore, it is necessary to raise parents’ awareness of the effectiveness and safety of the vaccine, so as to increase the COVID-19 vaccination rate in children and adolescents.
There did exist some shortcomings in our study. Firstly, we adopted the form of online questionnaire, which was mainly written by parents and indirectly investigated the vaccination intention of children and adolescents. There may be some errors in the data and relevant information to a certain extent. Secondly, the sample size of Hong Kong, Macao and Taiwan was too small,so it’s very necessary to gather more different regions to participate the survey.
Conclusion
In general, Chinese children and adolescents have high desires to be vaccinated against COVID-19, and most parents have positive attitudes towards their children’s vaccination. However, many people still hesitate or even refuse to be vaccinated. From the study, we find that parents’ COVID-19 vaccine behaviors, education backgrounds, attitudes towards children’s vaccination, children’s age, recent illness and other factors have certain impacts on children and adolescents’ willingness to vaccinate against COVID-19.
Availability of data and materials
Availability of data and material at corresponding author.
Abbreviations
- COVID-19:
-
Coronavirus Disease 2019
- SARS:
-
Severe Acute Respiratory Syndrome
- MTIS:
-
Multisystem Inflammatory Syndrome
References
Word Health Organization. Available at: https://www.who.int/data#reports. Accessed 1 Dec 2021
Galindo R, Chow H, Rongkavilit C. COVID-19 in children: clinical manifestations and pharmacologic interventions including vaccine trials. Pediatr Clin N Am. 2021;68(5):961–76. https://doi.org/10.1016/j.pcl.2021.05.004.
Tung Ho CL, Oligbu P, Ojubolamo O, et al. Clinical characteristics of children with COVID-19. AIMS Public Health. 2020;7(2):258–73. https://doi.org/10.1002/ppul.24991.
Kamidani S, Rostad CA, Anderson EJ. COVID-19 vaccine development: a pediatric perspective. Curr Opin Pediatr. 2021;33(1):144–51. https://doi.org/10.1097/MOP.0000000000000978.
Musa S, Dergaa I, Abdulmalik MA, et al. BNT162b2 COVID-19 vaccine hesitancy among parents of 4023 young adolescents (12–15 years) in Qatar. Vaccines (Basel). 2021;9(9):981. https://doi.org/10.3390/vaccines9090981.
Hacisuleyman E, Hale C, Saito Y, et al. Vaccine breakthrough infections with SARS-CoV-2 variants. N Engl J Med. 384(23):2212–8. https://doi.org/10.1056/NEJMoa2105000.
Xue FX. Shen KL (2021) COVID-19 in children and the importance of COVID-19 vaccination. World J Pediatr. 2021;17(5):462–6. https://doi.org/10.1007/s12519-021-00466-5.
Ali K, Berman G, Zhou H, et al. Evaluation of mRNA-1273 SARS-CoV-2 Vaccine in Adolescents.N Engl J Med. 2021;385(24):2241–51. https://doi.org/10.1056/NEJMoa2109522.
Sinopharm. COVID-19 vaccine were approved for emergency use by children aged 3–17 years, 2021. Available at: http://www.sinopharm.com/s/1223-4126-39607.html. Accessed 5 Dec 2021.
MacDonald NE. SAGE working group on vaccine hesitancy. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–4. https://doi.org/10.1016/j.vaccine.2015.04.036.
Alfieri NL, Kusma JD, Heard-Garris N, et al. Parental COVID-19 vaccine hesitancy for children: vulnerability in an urban hotspot. BMC Public Health. 2021;21(1):1662. https://doi.org/10.1186/s12889-021-11725-5.
Szilagyi PG, Shah MD, Delgado JR, et al. Parents’ intentions and perceptions about COVID-19 vaccination for their children: results from a National Survey. Pediatrics. 2021;148(4):e2021052335. https://doi.org/10.1542/peds.2021-052335.
Rubens JH, Akindele NP, Tschudy MM, et al. Acute covid-19 and multisystem inflammatory syndrome in children. BMJ. 2021;372:n385. https://doi.org/10.1136/bmj.n385.
Randolph HE, Barreiro LB. Herd immunity: understanding COVID-19. Immunity. 2020;52(5):737–41. https://doi.org/10.1016/j.immuni.2020.04.012.
Rhodes ME, Sundstrom B, Ritter E, et al. Preparing for a COVID-19 vaccine: a mixed methods study of vaccine hesitant parents. J Health Commun. 2020;25(10):831–7. https://doi.org/10.1080/10810730.2021.1871986.
Çağ Y, Bektemür G, Karabela Ş, et al. Parents’ attitudes toward COVID-19 vaccination and childhood vaccines during the COVID-19 pandemic. Asia Pac J Public Health. 2022;34(2–3):270–2. https://doi.org/10.1177/10105395211058291.
Ladhani SN. Crossing the Rubicon: a fine line between waiting and vaccinating adolescents against COVID-19. J Inf Secur. 2021;83(3):294–7. https://doi.org/10.1016/j.jinf.2021.07.015.
Harris RJ, Hall JA, Zaidi A, et al. Effect of vaccination on household transmission of SARS-CoV-2 in England. N Engl J Med. 2021;385(8):759–60. https://doi.org/10.1056/NEJMc2107717.
Scherer AM, Gedlinske AM, Parker AM, et al. Acceptability of adolescent COVID-19 vaccination among adolescents and parents of adolescents — United States, April 15–23, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(28):997–1003. https://doi.org/10.15585/mmwr.mm7028e1.
Zhang KC, Fang Y, Cao H, et al. Parental acceptability of COVID-19 vaccination for children under the age of 18 years: cross-sectional online survey. JMIR Pediatr Parent. 2020;3(2):e24827. https://doi.org/10.2196/24827.
Bambra C, Riordan R, Ford J, Matthews F. The COVID-19 pandemic and health inequalities. J Epidemiol Community Health. 2020;74(11):964–8. https://doi.org/10.1136/jech-2020-214401.
Cai H, Bai W, Liu S, et al. Attitudes toward COVID-19 vaccines in Chinese adolescents. Front Med (Lausanne). 2021;8:691079. https://doi.org/10.3389/fmed.2021.691079.
Zona S, Partesotti S, Bergomi A, et al. Anti-COVID vaccination for adolescents: a survey on determinants of vaccine parental hesitancy. Vaccines (Basel). 2021;9(11):1309. https://doi.org/10.3390/vaccines9111309.
Acknowledgements
We are grateful to all the medical staf fghting the COVID-19 epidemic at the front line. The work was supported by the Key medical disciplines of Hangzhou.
Funding
This study was supported by Hangzhou Science and Technology Bureau fund (No. 20191203B96;No. 20191203B105); Youth Fund of Zhejiang Academy of Medical Sciences (No. 2019Y009); Medical and Technology Project of Zhejiang Province (No. 2021KY890); Clinical Research Fund of Zhejiang Medical Association (No. 2020ZYC-A13); Hangzhou Health and Family Planning Technology Plan Key Projects (No. 2017ZD02); Zhejiang Medical and Health Science and Technology Plan Project (No. 2019RC245); Hangzhou Agricultural and Social Development Research Active Design Project (No. 20190101A03). Zhejiang Traditional Chinese Medicine Scientific Research Fund Project (No. 2022ZB280).
Author information
Authors and Affiliations
Contributions
L W, W W and C C conceptualized and designed the study, drafted the initial manuscript, designed the data collection instruments, collected data, and reviewed and revised the manuscript. J T and C Wcarried out the statistical analysis and reviewed and revised the manuscript. M Z, Y C and X Z performed the stimulation tests and reviewed and revised the manuscript. M W,Z F and Wq W conceptualized and designed the study and critically reviewed the manuscript for important intellectual content. Wq W conceptualized and designed the study,carried out the statistical analysis, drafted the initial manuscript, coordinated and supervised the data collection, and reviewed and revised the manuscript. All authors contributed to the article and approved the submitted version.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The ethics committee of Hangzhou Stomatological Hospital approved all the procedures performed. Informed consent forms were obtained from all participants. All methods were performed in accordance with the ethical standards as laid down in the Declaration of Helsinki and its later amendments or comparable ethical standards. The confidentiality of the information was maintained, and the data were recorded anonymously throughout the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary file 1.
Original questionnaire data.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, L., Wen, W., Chen, C. et al. Explore the attitudes of children and adolescent parents towards the vaccination of COVID-19 in China. Ital J Pediatr 48, 122 (2022). https://doi.org/10.1186/s13052-022-01321-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13052-022-01321-7