
Abstract
Background
Allergic rhinitis (AR) and allergic asthma are caused by an IgE-mediated inflammatory reaction. Probiotics may exert anti-inflammatory and immune-modulatory activity. Thus, this study aimed at investigating whether a Bifidobacteria mixture could be able to relieve nasal symptoms, and affect quality of life (QoL) in children with AR and intermittent asthma due to Parietaria allergy.
Materials and methods
The present study was conducted as placebo-controlled, double-blinded, and randomized. Globally, 40 children (18 males; mean age 9 ± 2.2 years) were enrolled. They were treated with probiotics or placebo: 1 sachet/day for 4 weeks. AR symptoms, and QoL were assessed at baseline and after treatment. Use of rescue medications, such as cetirizine syrup and salbutamol spray, was also permitted and recorded.
Results
Children treated with probiotic mixture achieved a significant improvement of symptoms (p < 0.005), and QoL ((p < 0.001). Placebo group had worsening of symptoms (p < 0.005) and QoL (p < 0.001). The use of rescue medications was overlapping in the two groups. The intergroup analysis showed that probiotic mixture was significantly superior than placebo for all parameters.
Conclusions
The current study demonstrated that a Bifidobacteria mixture was able of significantly improving AR symptoms and QoL in children with pollen-induced AR and intermittent asthma.
Clinical trial registration
ClinicalTrials.gov ID NCT02807064.
Similar content being viewed by others

Background
Seasonal allergic rhinitis (SAR) is common in children and is characterized by typical symptoms and nasal inflammation after pollen exposure [1, 2]. Anyhow, allergic asthma is characterized by airway inflammation and bronchial hyperreactivity; asthma symptoms are also triggered by allergen inhalation [3]. Actually, allergy is defined by a functional defect of allergen-specific T regulatory cells allowing T helper 2 (Th2) cells polarization [4]. Th2 cells produce interleukins, including IL-4, IL-5, and IL-13, that drive allergic inflammation. Moreover, allergic rhinitis affects quality of life (QoL) in children [5], and is the main risk factor for asthma onset and worsening and is a common co-morbidity in asthmatics [6]. Patients with Parietaria allergy may present AR associated with asthma.
Allergy prevalence has dramatically worldwide increased over the past decades and the hygiene hypothesis suggested that reduced exposure to microbial agents could increase the risk of allergic diseases [7]. This theory has been recently revisited emphasizing the role of microbiota dysbiosis promoting impaired immunological tolerance to allergens [8].
The main medications for allergy are antihistamines, bronchodilators, and corticosteroids, which are effective, but may have adverse events. For this reason, many people prefer to use also non-pharmacological medicine. In this regard, increasing attention has been paid to probiotics. Probiotic is a life microorganism able to give healthy effects on the host [9]. Probiotics may exert many immune-modulatory and anti-inflammatory effects [10, 11]. So, many attempts of restoring enteric microbiota with probiotic supplementation were performed in allergic disorders [12, 13]. In this regard, Lactobacilli were able to reduce allergic symptoms and improve QoL also in children [14]. There is evidence that probiotics promote the production of some cytokines, including IL-10, TGF-β, IL-12, and IFN-γ, that regulate the immune response and damp allergic inflammation [15–19].
Bifidobacteria were also extensively evaluated. B. breve reduced negative effects induced by antibiotics and restored enteric microbiota [20–23]; it also improved symptoms of atopic dermatitis [24]. B longum BB536 is widely used in dairy industry because of its anti-infective activity [25]. B longum BB536 treatment in SAR patients significantly reduced nasal symptoms and Th2-polarized immune response [26]. B infantis M-63 is commonly used in formula. However, Bifidobacteria colonization depends on age of subjects and specific strain [27, 28].
Recently, it has been demonstrated that a Bifidobacteria mixture, containing B longum BB536 (3x109 CFU), B infantis M-63 (1x109 CFU), and B breve M-16 V (1x109 CFU), has several biological characteristics, including in vitro compatibility, stability over time, and optimal doses, able to suggest its clinical use [29]. So, this mixture has been marketed as medical device I class. Therefore, the aim of the current randomized, double-blind, placebo-controlled study was to evaluate the effects of this Bifidobacteria mixture in children with SAR and intermittent asthma. The primary outcome was the effect on AR symptoms, secondary outcome was effects on QoL.
Methods
The present study was conducted as prospective, double-blind, placebo-controlled, and randomized. Globally, 40 children (18 males; mean age 9 ± 2.2 years) were enrolled. They attended the Department of Woman, Child and General and Specialized Surgery of the Second University of Naples, as suffering from SAR and well controlled asthma. AR and asthma diagnosis were performed, according to GINA and criteria [3, 30]. In particular, allergy was defined if symptom history was consistent with documented sensitization, such as positive skin prick test, to Parietaria allergen, i.e. allergic symptoms had to occur only during the Parietaria pollen season. AR diagnosis was done on the basis of typical symptoms occurring during Parietaria pollen season. Asthma diagnosis was performed considering typical symptoms and functional assessment.
Inclusion criteria were: i) age range between 4–17 years, ii) diagnosis of SAR and intermittent asthma due to Parietaria officinalis pollen, iii) presence of AR symptoms, including nasal itching, sneezing, watery rhinorrhea, nasal obstruction, and itchy eyes, since at least two weeks, documented by a run-in period, iv) well controlled asthma, such as symptoms requiring short acting β2-agonist ≤ 2 times/month, and v) written informed consent signed by parents. Exclusion criteria were: i) concomitant respiratory infections, ii) chronic illnesses, iii) continuous use of medications (antihistamines and corticosteroids) in the last 2 weeks, and iv) not well controlled asthma.
Patients were randomly (1:1 ratio) subdivided in two groups: placebo-treated (Group A) and actively-treated (Group B). Active medication was an oral supplementation containing Bifidobacteria mixture, B longum BB536 (3x109 CFU), B infantis M-63 (1x109 CFU), and B breve M-16 V (1x109 CFU) as powder in 3 mg sachet. Placebo was an inert excipient as powder. Patients were instructed to assume 1 sachet diluted in little tepid water or milk in the morning for 8 weeks. Cetirizine syrup (1 drop/3Kg/bw) and salbutamol spray (200 mcg/puff) were permitted as rescue medication during both run-in and treatment periods; the symptomatic use was recorded on a diary card. About cetirizine, it was calculated the number of days when it was assumed. About salbutamol, the number of puff was considered.
Adverse events were registered. The study was performed during the Parietaria pollen season. The study protocol was approved by the Ethics Committee of the Second University of Naples. The study was registered at ClinicalTrials.gov ID NCT02807064.
The study was conducted during the 2015 spring.
Children were evaluated at baseline (T0) and at the end of the treatment (T1).
Nasal symptoms (nasal itching, sneezing, rhinorrhea, nasal obstruction, and itchy eyes) were scored using a four-point scale (0 = no symptom; 1 = mild; 2 = moderate; 3 = severe) and the sum was calculated as total symptom score (TSS).
QoL was assessed by the Mini Rhinoconjunctivitis quality of life questionnaire [31].
Lung function was assessed by spirometry at baseline
The sample size was calculated by log-rank test with power at 90% and α error at 5%: 20 subjects per arm were considered sufficient. Randomization was performed per blocks following the Wichmann-Hill model.
Data were reported as medians and interquartile ranges (IQR) and standard deviation. The Mann–Whitney test was used as a non-parametric counter-part, paired data were compared using the Wilcoxon test. A P-value less than 0.05 was considered statistically significant. A statistical software program (StatSoft Italia s.r.l. 2005. Statistica, Vigonza, Italy) was used for all the analyses.
Results
All children completed the study; both treatments were well tolerated and there were no clinically relevant side effects in children of both groups. The adherence to treatments was >90% in both groups.
There was no significant difference between groups at baseline, including baseline lung function (normal in all subjects) so the two groups were homogeneous.
Symptoms
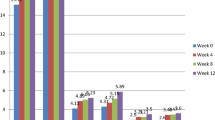
TSS significantly (p < 0.005) increased in Group A (T0 = 8.4 ± 2; T1 = 11 ± 1.3); whereas significantly decreased in Group B (T0 = 9.3 ± 2.1; T1 = 3.5 ± 1.7), as reported in Fig. 1. The intergroup comparison showed that there was a significant difference (p < 0.005) at T1.

Total symptom scores in patients treated with Placebo (Group A) or Bifidobacteria mixture (Group B) at baseline (T0) and after treatement (T1). Data are expressed as medians, IQR, and standard deviations
Quality of life
The only item that significantly changed in both groups during the study was the practical problems. It significantly (p < 0.001) increased in Group A (T0 = 32.4 ± 8.9; T1 = 47.5 ± 7.1); whereas significantly (p < 0.001) decreased in Group B (T0 = 37.6 ± 8.4; T1 = 11.9 ± 5.2), as reported in Fig. 2. The intergroup comparison showed that there was a significant difference (p < 0.001) at T1.

QoL = practical problems item in patients treated with Placebo (Group A) or Bifidobacteria mixture (Group B) at baseline (T0) and after treatement (T1). Data are expressed as medians, IQR, and standard deviations
Rescue medication
Cetirizine use was overlapping in two groups (33 ± 7 days in Group A and 31 ± 8 days in Group B). Salbutamol use was also overlapping in the two groups (22 ± 4 puffs in Group A and 19 ± 7 puffs in Group B).
Discussion
The rationale for using probiotics in allergic disorders is robust and is based on the concept that the balance between immunologic tolerance and inflammation is regulated by crosstalk between intestinal microbiota and innate and adaptive immune response [32]. In particular, the main targets of probiotics are: dendritic cells, epithelial cells, T regulatory cells, effector lymphocytes, natural killer cells, and B cells. Probiotics modulate allergic response mainly by stimulating Th1 pathway and restoring T regs. So, probiotics may effectively modulate the impaired immune response in allergic subjects.
Bifidobacteria are Gram-positive anaerobic bacteria and are ubiquitous and endosymbiotic inhabitant of the digestive tract. As they have beneficial effects on human health, are commonly used in the production of probiotics products. However, probiotics to be fruitfully and safely used should be respond to a series of requisites. In this regard, it has been performed an in vitro study to assess the use of B longum BB536, B infantis M-63, and B breve M-16 V in combination as food supplement [29]. Growth compatibility, resistance to antimicrobial agents, resistance to gastric acidity, bile salt hydrolysis, and adhesion to the human epithelial cells were examined. This study showed that these strains had reliable characteristics confirming their probiotic belonging. A further in vitro study examined the effects of this Bifidobacteria mixture on dendritic cells functionality from children with inflammatory bowel disease [33]. It was demonstrated that Bifodobacteria improved the antigen uptake and processing exerted by dendritic cells from children with Crohn’s disease, but there was no relevant effect in children with ulcerative colitis or functional gastrointestinal disorders. The authors concluded that this immunological effect could damp the impairment of intestinal innate immunity and reduce uncontrolled microbial overgrowth. An in vivo confirmatory study has been recently published [34]. This study explored the possibility that the Bifidobacteria mixture could improve abdominal pain and quality of life in children with irritable bowel syndrome and functional dyspepsia. Actually, this compound achieved the expected outcomes.
On the basis of this background, we tested the hypothesis that this Bifidobacteria mixture could positively affect AR symptoms and QoL in children with SAR and intermittent and well-controlled asthma. Really, the present study showed that a Bifidobacteria mixture was significantly effective in reducing nasal symptoms and in improving QoL in children with SAR and intermittent asthma.
A possible explanation of these findings could be dependent on the modulatory activity on innate immunity. It seems plausible that Bifidobacteria may orient the immune response toward a physiological Th1-polarized immune response and may restore a Treg pathway able to reducing allergic inflammation. Consequently, symptoms diminished.
Probiotics may be able to affect immune response and consequently allergic disorders. This matter is up-to-date in the prevention and treatment of respiratory disorders [12]. Two recent meta-analysis pointed out the role of probiotics in the management of allergic rhinitis and prevention of upper respiratory infection [13, 35].
It is to note that the effectiveness of probiotics is usually specific for each single strain. In this regard, there is a body of evidence that Lactobacillus acidophilus NCFM and Bifidobacterium lactis BL-04 exert different anti-inflammatory effects and modulate allergic reaction, diminishing the Th2-polarization, promoting Th1 proliferation, and restoring the defective Treg function [36–38]. Therefore, these strains have been fruitfully used in the treatment of pollen-induced allergic rhinitis [39]. Moreover, probiotics may be also effective in the treatment of food allergy [40] as well as gastric infection [41].
So, our findings are substantially consistent with these previous reports.
Noteworthy, the current compound significantly improved QoL item concerning the practical problems strictly closed to nasal symptom severity. Thus, this outcome underlines the effectiveness of this compound. However, a placebo effect could be not excluded a priori.
On the other hand, the main limitation of this study is the limited number of enrolled patients. So, it should be considered as preliminary experience that should be possibly confirmed by a multicenter trial enrolling larger population of allergic children.
Conclusion
The current study demonstrated that a Bifidobacteria mixture was able of significantly improving AR symptoms and QoL in children with pollen-induced AR and intermittent asthma.
References
Settipane RA, Schwindt C. Chapter 15: Allergic rhinitis. Am J Rhinol Allergy. 2013;27 Suppl 1:S52–5.
Dondi A, Tripodi S, Panetta V, Asero R, DiRienzo-Businco A, Bianchi A, et al. Italian Pediatric Allergy Network (I-PAN). Pollen-induced allergic rhinitis in 1360 Italian children: comorbidities and determinants of severity. Pediatr Allergy Immunol. 2013;24:742–51.
Global Initiative for Asthma. GINA guidelines. Global strategy for Asthma Management and Prevention. Available at: htpp://www.ginasthma.org/. Accessed July 2016.
Alroqi FJ, Chatila TA. T Regulatory Cell Biology in Health and Disease. Curr Allergy Asthma Rep. 2016;16:27.
Miraglia Del Giudice M, Marseglia A, Leonardi S, La Rosa M, Salpietro C, et al. Allergic rhinitis and quality of life in children. Int J Immunopathol Pharmacol. 2011;24:25–8.
Barberi S, Bernardo L, Bellasio M, Ferrara F, Tosi S, Ciprandi G. Nose-bronchi link: does an asthma march exist?. J Biol Regul Homeost Agents. 2015;29:941–3.
Strachan DP. Hay fever, hygiene, and household size. BMJ. 1989;18:1259–60.
Liu AH. Revisiting the hygiene hypothesis for allergy and asthma. J Allergy Clin Immunol. 2015;136:860–5.
Gilliland SE, Morelli L, Reid G. Health and nutritional properties of probiotics in food including powder milk with live lactic acid bacteria. In: Proceedings from the FAO/WHO Expert Consultation. Cordoba, Argentina: FAO. Food and Nutrition. 2001. paper 85.
Vliagoftis H, Kouranos VS, Betsi GI, Falagas ME. Probiotics for the treatment of allergic rhinitis and asthma: systematic review of randomized controlled trials. Ann Allergy Asthma Immunol. 2008;101:570–9.
Lin W-Y, Lin-Shien F, Lin H-K, Shen C-Y, Chen Y-J. Evaluation of the Effect of Lactobacillus paracasei in Children with Perennial Allergic Rhinitis: A 12-week, Double-blind, Randomized, Placebo-controlled Study. Pediatr Neonatol. 2013;20:S1875–9572.
West CE. Probiotics for allergy prevention. Benef Microbes. 2016;7:171–9.
Zajac AE, Adams AS, Turner JH. A systematic review and meta-analysis of probiotics for the treatment of allergic rhinitis. Int Forum Allergy Rhinol. 2015;5:524–32.
Giovannini M, Agostoni C, Riva E, Salvini F, Ruscitto A, Zuccotti GV, et al. A randomized prospective double blind controlled trial on effects of long-term consumption of fermented milk containing Lactobacillus casei in pre-school children with allergic asthma and/or rhinitis. Pediatr Res. 2007;62:215–20.
Miraglia del Giudice M, Leonardi S, Ciprandi G, Galdo F, Gubitosi A, La Rosa M, et al. Probiotics in childhood: allergic illness and respiratory infections. J Clin Gastroenterol. 2012;46:S69–72.
Das RR, Singh M, Shafiq N. Probiotics in treatment of allergic rhinitis. World Allergy Organ J. 2010;3:239–44.
Lue KH, Sun HL, Lu KH, Ku MS, Sheu JN, Chan CH, et al. A trial of adding Lactobacillus johnsonii EM1 to levocetirizine for treatment of perennial allergic rhinitis in children aged 7e12 years. Int J Pediatr Otorhinolaryngol. 2012;76:994–1001.
Chen YS, Jan RL, Lin YL, Chen HH, Wang JY. Randomized placebo-controlled trial of Lactobacillus on asthmatic children with allergic rhinitis. Pediatr Pulmonol. 2010;45:1111–20.
Miraglia Del Giudice M, Maiello N, Decimo F, Fusco N, D’ Agostino B, Sullo N, et al. Airways allergic inflammation and L. reuterii treatment in asthmatic children. J Biol Regul Homeost Agents. 2012;26:35–40.
Bin-Nun A, Bromiker R, Wilschanski M, Kaplan M, Rudensky B, Caplan M, et al. Oral probiotics prevent necrotizing enterocolitis in very low birth weight neonates. J Pediatr. 2005;147:192–6.
Lin HC, Su BH, Chen AC, Lin TW, Tsai CH, Yeh TF, et al. Oral probiotics reduce the incidence and severity of necrotizing enterocolitis in very low birth weight infants. Pediatrics. 2005;115:1–4.
Akiyama K, Shimada M, Ishizeki S, Takigawa I, Imura S, Yamauchi K, et al. Effects of oral administration of Bifidobacterium on the change of intestinal microflora induced by antibiotic therapy in extremely low birth weight infants. J Jpn Pediatr Soc. 1995;99:1436–41.
Satoh Y, Shinohara K, Umezaki H, Shoji H, Satoh H, Ohtsuka Y, et al. Bifidobacteria prevents necrotizing enterocolitis and infection in preterm infants. Int J Probiotics Prebiotics. 2007;2:149–54.
Hattori K, Yamamoto A, Sasai M, Taniuchi S, Kojima T, Kobayashi Y, et al. Effects of administration of bifidobacteria on fecal microflora and clinical symptoms in infants with atopic dermatitis. Jpn J Allergol. 2003;52:20–30.
Namba K, Hatano M, Yaeshima T, Takase M, Suzuki K. Effects of Bifidobacterium longum BB536 administration on influenza infection, influenza vaccine antibody titer, and cell-mediated immunity in the elderly. Biosci Biotechnol Biochem. 2010;74:939–45.
Xiao JZ, Kondo S, Yanagisawa N, Takahashi N, Odamaki T, Iwabuchi N, et al. Probiotics in the treatment of Japanese cedar pollinosis: a double-blind placebo- controlled trial. Clin Exp Allergy. 2006;36:1425–35.
Yaeshima T, Fujisawa T, Mitsuoka T. Bifidobacterium species ex pressing phenotypical similarity to Bifidobacterium adolescentis isolated from the feces of human adults. Bifidobact Microflora. 1992;11:25–32.
Mackie RI, Sghir A, Gaskins HR. Developmental microbial ecology of the neonatal gastrointestinal tract. Am J Clin Nutr. 1999;69:S1035–45.
Toscano M, De Vecchi E, Gabrieli A, Zuccotti GV, Drago L. Probiotic characteristics and in vitro compatibility of a combination of bifidobacterium breve M-16V, Bifidobacterium longum subsp. Infantis M-63 and Bifidobacterium longum subsp. Longum BB536. Ann Microbiol. 2015;65:1079–86.
Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 Update (in collaboration with the World Health Organization, GA2LEN and AllerGen). Allergy. 2008;63 Suppl 86:8–160.
Juniper EF, Thompson AK, Ferrie PJ, Roberts JN. Development and validation of the Mini Rhinoconjunctivitis quality of life questionnaire. Clin Exp Allergy. 2000;30:132–40.
Frei R, Akdis M, O’Mahony L. Prebiotics, probiotics, synbiotocs, and the immune system: experimental data and clinical evidence. Curr Opin Gastroenterol. 2015;31:153–8.
Strisciuglio C, Miele E, Giugliano FP, Vitale S, Andreozzi M, Vitale A, et al. Bifidobacteria enhance antigen sampling and processing by dendritic cells in pediatric inflammatory bowel disease. Inflamm Bowel Dis. 2015;21:1491–8.
Giannetti E, Maglione M, Alessandrella A, Strisciuglio C, De Giovanni D, Campanozzi A, et al. A Mixture of 3 Bifidobacteria Decreases Abdominal Pain and Improves the Quality of Life in Children With Irritable Bowel Syndrome: A Multicenter, Randomized, Double-Blind, Placebo-Controlled, Crossover Trial. J Clin Gastroenterol. 2016 (in press).
Hao Q, Dong BR, Wu T. Probiotics for preventing acute upper respiratory tract infections (Review). Cochrane Database Syst Rev. 2015;2:CD006895.
Foligne E, Nutten S, Grangette C, et al. Correlation between in vitro and in vivo immunomodulatory properties of lactic acid bacteria. World J Gastroenterol. 2007;13:236–43.
Lammers KM, Brigidi P, Vitali B, et al. Immunomodulatory effects of probiotic bacteria DNA: IL-1 and IL-10 response in human peripheral blood mononuclear cells. FEMS Immunol Med Microbiol. 2003;38:165–72.
Zoumpopoulou G, Tsakalidou E, Dewulf J, et al. Differential crosstalk between epithelial cells, dendritic cells and bacteria. Int J Food Micro. 2009;131:40–51.
Ouwehand AC, Nermes M, Collado MC, et al. Specific probiotics alleviate allergic rhinitis during the birch pollen season. World J Gastroenterol. 2009;15:3261–8.
Castellazzi AM, Valsecchi C, Caimmi S, Licari A, Marseglia A, Leoni MC, et al. Probiotics and food allergy. Ital J Pediatr. 2013;29(39):47.
Lionetti E, Francavilla R, Castellazzi AM, Arrigo T, Labò E, Leonardi S, et al. Probiotics and Helicobacter pylori infection in children. J Biol Regul Homeost Agents. 2012;26(1 Suppl):S69–76.
Acknowledgement
Not applicable.
Funding
The study had no sponsorship.
Availability of data and materials
Please contact authors for data requests.
Authors’ contribution
MMdG designed the study, CI collected linical data, MC analyzed the results, NM revised the paper, FD collected clinical data, GC wrote the paper. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The Ethics Committee of the Seconf University of Naples approved the study and the patients’ consent.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Miraglia Del Giudice, M., Indolfi, C., Capasso, M. et al. Bifidobacterium mixture (B longum BB536, B infantis M-63, B breve M-16V) treatment in children with seasonal allergic rhinitis and intermittent asthma. Ital J Pediatr 43, 25 (2017). https://doi.org/10.1186/s13052-017-0340-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13052-017-0340-5