
Abstract
Background
Self-Inflating Resuscitation Bags (SIRB) are common and essential tools in airway management and ventilation. They are often used in resuscitation and emergency anaesthesia outside the operating theatre. There is a common notion that all SIRBs applied with a tight sealed mask will deliver close to 100 % oxygen during spontaneous breathing. The aim of the study was to measure the oxygen delivery of six commonly used SIRBs in a mechanical spontaneous breathing adult in vitro model.
Methods
Three SIRBs of each of the six models were evaluated for oxygen delivery during simulated breathing with an adult mechanical lung. The test was repeated three times per device (54 tests in total). The breathing profile was fixed to a minute volume of 10 L/min, a tidal volume of 500 mL and the SIRBs supplied with an oxygen fresh gas flow of 15 L/min. The fraction of delivered oxygen (FDO2) was measured over a three-minute period. Average FDO2 was calculated and compared at 30, 60 and 90 s.
Results
At 90 s all models had reached a stable FDO2. Average FDO2 at 90 s; Ambu Oval Plus 99,5 %; Ambu Spur II 99,8 %; Intersurgical BVM Resuscitator 76,7 %; Laerdal Silicone 97,3 %; Laerdal The Bag II 94,5 % and the O-Two Smart Bag 39,0 %. All differences in FDO2 were significant apart from the two Ambu models.
Conclusions
In simulated spontaneous breathing, four out of six (by Ambu and Laerdal) Self-Inflating Resuscitation Bags delivered a high fraction of oxygen while two (Intersurgical and O-two) underperformed in oxygen delivery. These large variations confirm results reported in other studies. It is our opinion that underperforming Self-Inflating Resuscitation Bags might pose a serious threat to patients’ health if used in resuscitation and anaesthesia. Manufacturers of Self-Inflating Resuscitation Bags rarely provide information on performance for spontaneous breathing. This poses a challenge to all organizations that need their devices to deliver adequate oxygen during spontaneous breathing.
Similar content being viewed by others

Background
Self-Inflating Resuscitation Bags (SIRBs), also known as Bag-Valve-Mask devices (BVMs) or Manual Resuscitators, are common and essential tools in airway management and ventilation. They are mainly used in resuscitation and emergency anaesthesia outside the Operating Theatre (OT) and Intensive Care Unit (ICU), including the prehospital arena. SIRBs are used for positive pressure ventilation in patients with insufficient breathing but also for preoxygenation of the spontaneously breathing. For patients undergoing anaesthesia with no access to ventilators or anaesthetic machines there are few practical alternatives to a SIRB [1,2,3].
Preoxygenation effectiveness is affected by a compound of several factors including, but not limited to: patient factors (age, anatomy, habitus, pathology, breathing pattern), situational factors (patient position, timing, altitude), operator factors (skills and knowledge) and technical factors (oxygen delivery device characteristics, positive end-expiratory pressure (PEEP), oxygen fresh gas flow rate) [1, 4, 5]. Some of these factors can be optimized by skill, conscious handling and timing, whereas others cannot be changed. The characteristics of the oxygen delivery device are generally fixed to the construction of the specific device.
The fraction of delivered oxygen (FDO2) from a device corresponds to the maximum inhaled fraction of oxygen (FiO2) and subsequently the fraction of alveolar oxygen achieved in a subject [4]. Thus, a low FDO2 directly translates to a suboptimal preoxygenation effect. Clinically, end-tidal oxygen concentration (EtO2) can be used as a measurement that reflects preoxygenation efficacy. Clinical recommendations for preoxygenation in anaesthesia is to target an EtO2 of at least 0.85–0.9 [4,5,6]. EtO2 can never be higher than FDO2 or FiO2; making an FDO2-capability close to 1.0 paramount for achieving a successful preoxygenation.
The gold standard for preoxygenation is a tight sealed mask connected to an anaesthetic machine, with close to an FiO2 of 1.0 [1, 2]. Outside of the OT and ICU the most common devices used for preoxygenation are SIRBs, free-flow oxygen masks, flow-dependent Mapelson systems or high-flow nasal cannulas [1,2,3, 7]. The ability to manually ventilate apnoeic patients and limited oxygen supply typically makes a SIRB the preferred choice [3].
Previous studies comparing different types of devices for preoxygenation in spontaneously breathing adults have come to conflicting results and different conclusions [2, 7,8,9]. There is limited information from manufacturers about their device’s performance for this usage. Despite this, there is a common misconception that all SIRBs applied with a tight sealed mask will deliver close to an FiO2 of 1.0 during spontaneous breathing [10]. Several studies of varying designs in the last 30 years have highlighted that SIRBs differ markedly in their ability to deliver oxygen to the spontaneously breathing adult [10,11,12,13,14].
Our study revisited the research question of FDO2 performance of SIRBs and evaluated six common models on the Scandinavian market. A mechanical lung simulation was used to standardize testing, allowing tests of multiple devices of each model.
The aim of the study was to measure the oxygen delivery of six SIRB models in an adult mechanical spontaneous breathing in vitro model.
Methods
Six models of SIRBs, two reusable and four disposable, were evaluated in a laboratory setting. The characteristics of the different tested SIRBs are presented in Table 1.
Three devices of every model were tested for FDO2 performance. Each device was tested three times, amounting to nine test sequences per model and 54 sequences in total. The test sequence was conducted with a fixed breathing pattern consisting of a sine waveform with a respiratory rate (RR) of 20 per minute, a tidal volume (TV) of 500 mL and an inspiratory/expiratory ratio of 1:2.
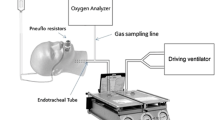
An ASL 5000 mechanical lung simulator (IngMar Medical, Pennsylvania, USA) was used to simulate the spontaneous breathing of an adult. A VT 650 Gas Flow Analyser (Fluke, Washington, USA), used for continuous oxygen sampling, was connected in line between the flow port of the lung machine and the SIRB being tested. A Clear-Guard 3 breathing filter (Intersurgical, Berkshire, UK) was connected between the gas analyser and the SIRB to protect the machines from particle contamination. The oxygen inlet of the SIRB to be tested was connected to 15 L/min of oxygen from a wall outlet and the reservoir and bag filled with oxygen before connection to the breathing circuit. The lung machine was breathing room air through the gas flow analyser before each test until a steady state of FiO2 of 0.21 (+/- 0.001) was achieved. Oxygen sampling was recorded 15 s before the SIRB was connected and went on for 180 s in total with a sampling interval of one second. Before each new model was tested the gas flow analyser was calibrated according to the manufacturer’s instructions and the oxygen wall output flow was calibrated to 15 L/min (+/- 0.01 L/min) with a Defender 510 (MesaLabs, California, USA) dry gas meter.
The start of each breath was manually aligned, and average delivered oxygen concentration was calculated for the nine datasets of each tested model. The means with confidence intervals are presented graphically. ANOVA were used to compare means at 30, 60 and 90 s, including post hoc testing with Bonferroni correction for multiple comparisons. These means were calculated for five seconds (-2 to + 2 s) for each model (total n = 54). Statistical significance was set to p < 0.05.
Results
The FDO2 performance of the different SIRBs are shown in Fig. 1. The differences between models were significant at the predefined times 30, 60 and 90 s and is presented in Table 2.

Delivered oxygen during simulated spontaneous breathing. Mean delivered oxygen for the nine recordings of each model. Error bars represent 95 % CI
Discussion
Four out of six (by Ambu and Laerdal) SIRBs performed well in delivering high and sufficient FDO2. One (Intersurgical) of the disposable devices performed markedly worse than the first four, achieving an FDO2max that is below what is needed to achieve an EtO2 > 0.85 in preoxygenation. The last disposable model (O-Two) performed so poorly that it presents an even greater risk when used for delivering oxygen to a spontaneously breathing patient.
Technical considerations
The two patient valve designs used in the tested models and most other available SIRBs are the duckbill valve and the disc valve (see Figs. 2, 3 and 4). The main reason for variations in FDO2 performance seems to be the presence of an expiratory valve. In our study, as well as in previous studies, the poor FDO2 performance was largely seen in devices with a duckbill design lacking a dedicated disc valve blocking the exhaust port during inspiration (see Fig. 3). This allows for air entrainment through the exhaust port during inspiration, resulting in a mixture of room air and oxygen being delivered to the patient.

The duckbill valve (Laerdal). Drawing is used and modified with permission from www.laerdal.com

The duckbill valve without an expiratory valve (Intersurgical and O-Two). Drawing is used and modified with permission from www.laerdal.com

The disc valve (Ambu). Drawing is used and modified with permission from www.ambu.com
In devices without an expiratory valve, the degree of air entrainment through the exhaust port will mainly depend on the opening pressure and flow resistance of the duckbill valve and the flow resistance of the exhaust port. Though this was not measured in our setup, a higher opening pressure and/or flow resistance of the duckbill valve will likely allow for more air entrainment through the low resistance opening of the exhaust port. If the expiratory valve does not seal properly it can allow for some entrainment of air. This has been shown previously [11] and might explain the smaller variation of FDO2 among the SIRBs with an expiratory valve that we tested.
The other valves in the SIRB add to the complexity (Fig. 5). The flow resistances and opening pressures of these valves determine forward flow pressures and the influence the oxygen fresh gas flow will have on the opening pressure of the patient valve. Increased oxygen fresh gas flow to the SIRB fills the reservoir and generates forward flow, which can lower the opening pressure of the inspiratory valve, resulting in less air entrainment at the patient end. Hence the oxygen fresh gas flow rate becomes more important in devices without a valve on the exhaust port. These factors are probably the main mechanisms behind the performance variation seen among duckbill SIRBs without an expiratory valve.

Cross-section drawing of a generic SIRB with a duckbill valve
Adding a disc valve or a PEEP-valve to the exhaust port will markedly attenuate the entrainment of room air (not reported) and improve performance. This strongly supports that the lack of an expiratory valve is the main cause of the poor performance of some SIRBs. We have not found any explanation as to why some manufacturers have chosen to omit the expiratory valve in their SIRBs.
The disc valve (Fig. 4) on the other hand, has a different design where the inspiratory valve leaflet blocks the exhaust port during inspiration and thus prevents a significant entrainment of room air. To our knowledge there is no study that has shown any significant air entrainment in SIRBs with the disc valve design.
The poorest performer, the O-Two, has an extra flow limiting valve in the neck between the bag and the duckbill valve, in addition to lacking an expiratory valve. The ‘SMART BAG’ feature is proposed to limit high pressures and slow down positive pressure breaths if the bag is squeezed too hard or fast when supplying positive pressure ventilation. Even with this function disabled, as in our tests, it is likely that this valve adds resistance to forward flow, further raising the opening pressure of the duckbill valve during spontaneous breathing.
Previous data also indicates that breathing variables such as TV, RR, breath profile and the peak inspiratory flow rate (PIFR) can affect oxygen delivering capacity [11]. These patient factors interact with the reservoir, casing, valve constructions and oxygen fresh gas flow in a way that is not always predictable.
The oxygen fresh gas flow rate must always exceed the minute volume (MV) to have a theoretical chance of delivering an FDO2 of 1.0. In our test profile, we used a MV of 10 L/min and an oxygen fresh gas flow of 15 L/min to reduce the risk of a mismatch affecting the test results. PIFR can exceed MV by multiple times, making a reservoir mandatory on a SIRB when using an oxygen fresh gas flow rate lower than PIFR. The reservoir size ought to be larger than the TV to sustain a high FDO2. Flush rate oxygen fresh gas flow (30–60 L/min) matching the PIFR can reduce the need for a reservoir but this option is not always available and certainly not in the prehospital environment.
The pros and cons of disposable versus reusable SIRBs were not the focus of our study. It is worth noting though, that we have not found any SIRB performance studies reporting this problem with reusable devices. That said, there are disposable devices that perform just as well or even better than some reusable devices, e.g. Ambu in our study.
Clinical implications
A predictable and constant FDO2 is crucial in supporting or preoxygenating spontaneously breathing critically ill patients. Using a SIRB that delivers a suboptimal oxygen flow in this setting can result in critical hypoxemia. We believe that a SIRB, with a verified oxygen flow, generally is the fall-back option for most operators to resolve many critical situations. This combination of circumstances can result in severe consequences.
The widespread knowledge gap about poor performing SIRBs can also lead to incorrect or conflicting conclusions from research. There are multiple examples where a single model of SIRB was used as a reference device in a comparative study between oxygen delivery devices [7,8,9, 15]. In a study from Robinson et al. [8] the EtO2 during preoxygenation of healthy volunteers were compared between a non-rebreather mask (NRM) and a SIRB (Intersurgical Adult Resuscitator) at an oxygen fresh gas flow of 10 L/min. The results showed that, while neither performed well, they produced comparable levels of EtO2. They concluded that the NRM might be a preferable approach of preoxygenation in that setting. Their choice of the Intersurgical Adult Resuscitator as benchmark was unfortunate and likely affected their results and conclusion. It might also have led to less than ideal practices in some services. Their study highlighted that many clinicians might take for granted that a SIRB with a tight seal mask achieves a near “gold standard” level of preoxygenation.
Strengths and limitations
Mechanical simulations are different from human or animal experiments. This is a limitation, but we believe that our method reliably explores the capacity for oxygen delivery in a SIRB.
Our setup generated highly reproducible recordings with low variability and statistical significance at differences that were below what is clinically relevant. We tested three devices of each model and repeated the recording three times to minimize the impact of a malfunctioning SIRB. There is a limitation in that we used a single breathing profile and one level of oxygen flow. The extensive study by Mills et al. [11] included 27 combinations of breathing profiles and flow rates but our findings are in line with theirs. Additionally, they found large variations of FDO2 related to the different breathing profiles and oxygen flow rates. It is likely that using more challenging breath profiles and more oxygen fresh gas flow levels would have affected the SIRB performance in our study as well.
Recommendations and future directions
We agree with previous researchers and urge manufacturers of underperforming SIRBs to either improve the spontaneous breathing performance or retract them from the market. Since there are both reusable and disposable SIRBs that perform well it is our opinion that a suboptimal SIRB has no place in healthcare today. Furthermore, we encourage all SIRB manufacturers to state their devices’ oxygen delivery performance in clinically relevant breathing scenarios during spontaneous breathing, in addition to positive pressure ventilation.
Further research areas in this field would be to make clinical studies to confirm or refute our findings. Another area would be to develop a SIRB with less imposed work of breathing while still maintaining a high oxygen delivery.
Conclusions
Our study shows that there are Self-Inflating Resuscitation Bags on the market that underperform in oxygen delivery when used for spontaneous breathing. These devices might pose a serious threat to patients’ health if used in resuscitation and anaesthesia. It is our opinion that Self-Inflating Resuscitation Bags that do not provide sufficient oxygen delivery during spontaneous breathing should not be used until further clinical studies prove them safe.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BVM:
-
Bag Valve Mask
- EtO2 :
-
End-tidal Oxygen Concentration
- FDO2 :
-
Fraction of Delivered Oxygen
- FiO2 :
-
Fraction of inspired Oxygen
- MV:
-
Minute Ventilation
- NRM:
-
Non-rebreather mask
- PEEP:
-
Positive End-Expiratory Pressure
- PIFR:
-
Peak Inspiratory Flow Rate
- RR:
-
Respiratory Rate
- SIRB:
-
Self-Inflating Resuscitation Bag
- TV:
-
Tidal Volume
References
Sakles JC. Maintenance of Oxygenation During Rapid Sequence Intubation in the Emergency Department. Acad Emerg Med. 2017;24:1395–404.
Groombridge CJ, Ley E, Miller M, et al. A prospective, randomised trial of pre-oxygenation strategies available in the pre-hospital environment. Anaesthesia. 2017;72:580–4.
Boulton AJ, Mashru A, Lyon R. Oxygenation strategies prior to and during prehospital emergency anaesthesia in UK HEMS practice (PREOXY survey). Scand J Trauma Resusc Emerg Med. 2020;28:99.
Nimmagadda U, Salem MR, Crystal GJ. Preoxygenation. Physiologic Basis, Benefits, and Potential Risks. Anesth Analg. 2017;124:507–17.
Bouroche G, Bourgain JL. Preoxygenation and general anesthesia: a review. Minerva Anestesiol. 2015;81:910–20.
Higgs A, McGrath BA, Goddard C, et al. Guidelines for the management of tracheal intubation in critically ill adults. Br J Anaesth. 2018;120:323–52.
Groombridge C, Chin CW, Hanrahan B, et al. Assessment of Common Preoxygenation Strategies Outside of the Operating Room Environment. Acad Emerg Med. 2016;23:342–6.
Robinson A, Ercole A. Evaluation of the self-inflating bag-valve-mask and non-rebreather mask as preoxygenation devices in volunteers. BMJ Open. 2012;2:e001785.
Pourmand A, Robinson C, Dorwart K, et al. Pre-oxygenation: Implications in emergency airway management. Am J Emerg Med. 2017;35:1177–83.
Chrimes N. Not all bag-valve-mask devices are created equal: beware a possible lower FiO2 during spontaneous ventilation. Anaesth Intensive Care. 2014;42:276.
Mills PJ, Baptiste J, Preston J, et al. Manual resuscitators and spontaneous ventilation-An evaluation. Crit Care Med. 1991;19:1425–31.
Hess D, Hirsch C, Marquis-D’Amico C, et al. Imposed work and oxygen delivery during spontaneous breathing with adult disposable manual ventilators. Anesthesiology. 1994;81:1256–63.
Nimmagadda U, Salem MR, Joseph NJ, et al. Efficacy of Preoxygenation with Tidal Volume Breathing: Comparison of Breathing Systems. Anesthesiology. 2000;93:693–8.
Kwei P, Matzelle S, Wallman D, et al. Inadequate preoxygenation during spontaneous ventilation with single patient use self-inflating resuscitation bags. Anaesth Intensive Care. 2006;34:685–6.
Driver BE, Prekker ME, Kornas RL, et al. Flush Rate Oxygen for Emergency Airway Preoxygenation. Ann Emerg Med. 2017;69:1–6.
Acknowledgements
The Department for Medical Technology, Östersund Hospital for their valuable help in providing test equipment.
Phil Holker for his help with language and proof reading.
The participants and supervisors of SSAI Critical Emergency Medicine program for input and discussions.
The retailers and manufacturers who kindly provided the devices tested.
Funding
The study was funded by the Department of Anaesthesia and Intensive Care, Östersund Hospital, Sweden and the Swedish Heart-Lung Foundation. Funders had no role in the design or conduct of the study. The project was academic with no funding from the industry. Open access funding provided by Umea University.
Author information
Authors and Affiliations
Contributions
SG was the lead investigator, conceived the study and contributed to all aspects of the study. TD contributed to the development of the study design, data interpretation, planning and performing the statistical analyses and critical revision. JJ contributed to the development of the study design and critical revision. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Grauman, S., Johansson, J. & Drevhammar, T. Large variations of oxygen delivery in self-inflating resuscitation bags used for preoxygenation - a mechanical simulation. Scand J Trauma Resusc Emerg Med 29, 98 (2021). https://doi.org/10.1186/s13049-021-00885-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13049-021-00885-3