
Abstract
Background
Using extracorporeal membrane oxygenation (ECMO) to provide advanced life support in adult trauma patients remains a controversial issue now. The study was aimed at identifying the independent predictors of hospital mortality in adult trauma patients receiving ECMO for advanced cardiopulmonary dysfunctions.
Methods
This retrospective study enrolled 36 adult trauma patients receiving ECMO due to advanced shock or respiratory failure in a level I trauma center between August 2006 and October 2014. Variables collected for analysis were demographics, serum biomarkers, characteristics of trauma, injury severity score (ISS), damage-control interventions, indications of ECMO, and associated complications. The outcomes were hospital mortality and hemorrhage on ECMO. The multivariate logistic regression method was used to identify the independent prognostic predictors for the outcomes.
Results
The medians of age and ISS were 36 (27–49) years and 29 (19–45). Twenty-three patients received damage-control interventions before ECMO. Among the 36 trauma patients, 14 received ECMO due to shock and 22 for respiratory failure. The complications of ECMO are major hemorrhages (n = 12), acute renal failure requiring hemodialysis (n = 10), and major brain events (n = 7). There were 15 patients died in hospital, and 9 of them were in the shock group.
Conclusions
The severity of trauma and the type of cardiopulmonary dysfunction significantly affected the outcomes of ECMO used for sustaining patients with post-traumatic cardiopulmonary dysfunction. Hemorrhage on ECMO remained a concern while the device was required soon after trauma, although a heparin-minimized protocol was adopted.
Trial registration
This study reported a health care intervention on human participants and was retrospectively registered. The Chang Gung Medical Foundation Institutional Review Board approved the study (no. 201601610B0) on December 12, 2016. All of the data were extracted from December 14, 2016, to March 31, 2017.
Similar content being viewed by others


Background
Trauma is one of the leading causes of death among adults around the world [1]. The most common causes of early death in trauma patients are hemorrhagic shock, cardiopulmonary dysfunction, and severe brain damage. Therefore, controlling active hemorrhages, maintaining arterial oxygenation, and draining pneumothorax or cardiac tamponade are essential techniques in emergency departments to decrease the early mortality rate in trauma patients [2, 3]. For selected trauma patients who are in advanced shock or respiratory failure, extracorporeal membrane oxygenation (ECMO) can be a salvage therapy that bridges these young and previously healthy patients to recovery [4,5,6,7,8,9]. ECMO is a simplified version of heart-lung machine that can replace the cardiopulmonary function temporarily; it simply sucks in deoxygenated blood from the patient’s venous system and pumps oxygenated blood back to the patient [10]. Depending on the destination of the oxygenated blood, ECMO offers two operating configurations. Venoarterial (VA) ECMO bypasses the lungs and returns the oxygenated blood back to the aorta. Therefore, VA-ECMO can raise both the arterial pressure and arterial oxygenation. Instead of bypassing the lungs, venovenous (VV) ECMO returns the oxygenated blood back to the right atrium. This arrangement makes the venous blood to be refreshed by ECMO first then by the native lungs. Therefore, VV-ECMO provides a purely respiratory support without significant disturbances to the cardiopulmonary system. According to a recently published meta-analysis that enrolls 215 patients with ECMO-treated post-traumatic respiratory failure, ECMO shows a rescue rate of 50 to 79% and is considered a useful salvage treatment for post-traumatic respiratory failure [11]. Now ECMO has also become a new attempt to rescue patients with post-traumatic shock and some encouraging experiences are sporadically reported [4, 7, 9]. However, as an extracorporeal circulation, ECMO requires heparinization and thus carries a risk of hemorrhage [10]. According to the Extracorporeal Life Support Organization Registry International Report 2016 [12], the overall incidence of hemorrhage in ECMO-treated adult patients is around 34% (respiratory support) to 43% (cardiac support). The risk of intracranial hemorrhage is around 2–4% in this report. However, the risk of hemorrhage on ECMO should increase while applying this heparin-equipped therapy to patients with a significant trauma-induced coagulopathy (TIC) [13, 14]. The study was aimed at presenting our experience on ECMO used for post-traumatic cardiopulmonary dysfunctions and identifying the independent predictors of hospital mortality.
Methods
Study population
From August 2006 to October 2014, a total of 638 patients received ECMO for hemodynamic (venoarterial mode; n = 489) or pulmonary (VV mode; n = 159) support at Chang Gung Memorial Hospital. Among the 638 patients, 36 adults (age ≥ 20 years) were enrolled in this retrospective study due to post-traumatic shock or post-traumatic respiratory failure. Before the administration of ECMO, all of the patients had received a whole body CT to recognize the major bleeding sites and received essential procedures (surgery or transarterial embolization) to stop active bleeding. After the major bleeding sites were controlled, ECMO would be used to sustain the hemodynamics or ventilation in selected patients with profound shock (systolic arterial pressure < 60 mmHg), severe hypoxemia [PaO2/ FiO2 ratio < 70 mmHg under maximal mechanical ventilation (MV)], or in-hospital cardiac arrest (CA). The institutional review board of our hospital approved the protocol (CGMF IRB no. 201601610B0) and waived the necessity of individual patient consent.
Managements of ECMO
The details of the principles and equipment in our practice of ECMO have been described in previous reports [8, 9, 15, 16]. According to the candidate’s need, the femoral-femoral VA-ECMO (cut-down cannulation) or the femoral-jugular VV-ECMO (percutaneous cannulation) are provided promptly. The ECMO circuit is heparin-bonded and primed with heparin-contained (2500 U/L) normal saline. To balance the thrombotic and hemorrhagic risks on ECMO, two anticoagulant strategies of ECMO are prepared. The heparin- titrated strategy includes a pre-cannulation bolus dose (5000 unit) and a continuous intravenous maintenance dose of heparin to keep a prolonged aPTT (45–55 s) during ECMO. This strategy is applied to patients who develop a need of ECMO after couple days of trauma, since their risk of hemorrhage on ECMO should be similar to general population. In the other hand, the heparin- minimized strategy waives the pre-cannulation dose and delivers the continuous maintenance dose of heparin after 48 h of ECMO. Approaching a near-normal aPTT (< 40 s) is the therapeutic goal in this period to achieve a satisfactory hemostasis. This strategy is applied to the patients who develop a need of ECMO soon after trauma or damage control interventions, since their risk of hemorrhage on ECMO should be increased due to the effects of Trauma-induced coagulopathy (TIC) [14]. During ECMO, the dose of vasopressors and the intensity of MV are gradually down-graded to maintain a normal mean arterial pressure (70–90 mmHg) and arterial oxygenation (PaO2 > 60 mmHg, PaCO2 30-50 mmHg, and SaO2 > 90%). Continuous renal replacement therapy (CRRT) is used to maintain negative fluid balance in patients with a temporary renal failure. While signs of recovery are presented, the support of ECMO is tapered and stopped if possible. For patients hemorrhaging on ECMO, withholding heparin plus blood transfusion (RBC: plasma: platelet about 1:1:3) is often the first step to achieve hemostasis on ECMO. Endoscopic, angiographic or surgical hemostasis was launched with low threshold once the conservative treatment failed or is impossible to stabilize the hemorrhage. Protamine or antifibrinolytic agents would be provided to patients in whom an obvious source of hemorrhage is not found after a series of investigations.
Data collection and outcome measures
We retrospectively reviewed the electronic medical records in each patient and collected their important demographic and clinical data before and during the administration of ECMO. The following variables were collected: age, gender, characteristics of trauma, injury severity score, damage control interventions,, duration of MV before ECMO, MV settings (peak inspiratory pressure, mean airway pressure, positive end-expiratory pressure, FiO2), duration of emergency room (ER) admission to ECMO administration, cardiac arrest and requiring ECMO-assisted cardiopulmonary resuscitation (E-CPR), the latest results of blood tests (arterial blood gas sampling, blood cell counts, creatinine, and total bilirubin) before ECMO, aPTT values before ECMO and during the first, 12th, 24th and 48th hour of ECMO, durations of hospital and ECMO stay, complications (hemorrhage, requiring CRRT, and brain events) of ECMO, and the outcome (survived or death in hospital). The brain events on ECMO included brain hemorrhage and brain infarction. The primary endpoint of this study was death in hospital, and the secondary endpoint was hemorrhage during ECMO.
Statistical analysis
Statistical analyses were performed using SPSS for Windows (Version 15.0, SPSS, Inc., IL, USA). Because the dataset was small, the Mann–Whitney U test was used to conduct univariate comparisons of the independent variables. The Chi-square or Fisher’s exact test was used to compare the categorical variables. The level of statistical significance was set at p < 0 .05. Continuous variables with a p < 0.05 were dichotomized according to the cut-off values. The cut-off values were determined by the receiver operating characteristic curve (ROC) analysis. These dichotomized risk factors were tested by the multivariate logistic regression analysis with backward stepwise selection to identify independent predictors of hospital mortality and hemorrhage on ECMO.
Results
Univariate comparison
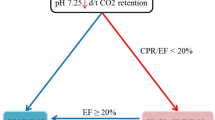
The median age and median ISS of the 36 patients were 36 (27–49) years and 29 (19–45), respectively. Among the 36 patients, 14 received VA-ECMO due to post-traumatic shock and 22 received VV-ECMO due to post-traumatic respiratory failure. In the group of VA-ECMO, eight patients required conventional CPR due to CA before ECMO institution. Three of the 8 patients regained spontaneous circulation after conventional CPR but still received VA-ECMO for the fluctuated hemodynamics. The other 5 patients developed refractory CA and eventually required E-CPR to restore spontaneous circulation. The median ECPR time was 35 (18–55). The causes of CA in the E-CPR group were severe airway obstruction with difficult intubation (n = 2), insufficient drainage of tension pneumothoraces/pneumomediastinum (n = 1), profound acidemia due to exsanguination during damage control surgery (n = 1), and profound sepsis due to intra-abdominal infection (n = 1). The patient with insufficient drainage of tension pneumothoraces/pneumomediastinum suffered from blunt chest injury with severe chest wall deformities, bilateral lung contusions, and pneumothoraces. He was treated with MV and bilateral tube thoracostomies initially and prepared for VV-ECMO implantation later due to his clinical deterioration. Unfortunately, he developed CA before the ECMO team arrived and he could just receive E-CPR with VA-ECMO. Twenty-four patients were weaned off ECMO after a median support of 130 (69–249) hours, and 21 of these patients survived to hospital discharge, including the 2 patients undergoing E-CPR. Figure 1 summarizes the clinical features among patients categorized by the need for ECMO (shock or respiratory failure) and the outcome (died or survived). The information on the mechanisms of trauma and associated therapies in each patient is summarized in Appendices 1 and 2. Twelve patients experienced major hemorrhage (4 intracranial, 5 intra-thoracic, and 3 intra-abdominal) on ECMO. Three patients were found to have significant brain infarctions. Ten patients experienced acute renal failure on ECMO and required CRRT. Table 1 lists the results of univariate comparisons between the survivors and non-survivors. Compared to the survivors, the non- survivors tended to have a higher ISS, post-traumatic shock/CA rather than respiratory failure, and a shorter hospital stay. In the VA-ECMO group, patients requiring E-CPR showed a similar hospital mortality rate when compared with patients receiving VA-ECMO for refractory shock(60% vs.67%; p = 1.0). On the other hand, the only significant difference between the hemorrhagic and the non-hemorrhagic groups was the value of aPTT obtained before ECMO (median aPTT: 52 vs. 33 s; p = 0.01). Table 2 demonstrates the results of univariate comparisons between the patients developing major hemorrhages on ECMO and the patients not. Compared to the non-hemorrhagic patients, the hemorrhagic patients tended to have a longer aPTT before ECMO institution. Figure 2 shows the trends of aPTT on ECMO in the hemorrhagic and non-hemorrhagic groups.

The flowchart of case distribution. CRRT: Continuous renal replacement therapy. ECMO: Extracorporeal membrane oxygenation. ER: Emergency room. ISS: Injury severity score. MV: Mechanical ventilation.VA: Venoarterial. VV: Venovenous

The time courses of the activated partial thromboplastin time during the first 48 h of extracorporeal membrane oxygenation. Median with 25th to 75th interquatile range. * The upper limit of detectable value of aPTT is 120 s
Multivariate comparison
Before entering the multivariate test, the ISS was dichotomized at the point of 35 according to the results of ROC analysis. The sensitivity (Sn), specificity (Sp), positive predictive value (PPV), and negative predictive value (NPV) at this cut-off point for predicting hospital mortality were 67%, 76%, 67%, and 76%, respectively. With the same processing, the aPTT obtained before ECMO was also dichotomized at the point of 40. The Sn, Sp, PPV, and NPV at this cut-off point for predicting hemorrhage on ECMO were 67%, 67%, 59%, and 74%, respectively. Finally, an ISS > 35 and the requirement of VA-ECMO due to a refractory post-traumatic shock/CA were identified to be the independent predictors of hospital mortality of the ECMO-treated trauma patients. With the same method, a pre-ECMO value of aPTT > 40 s was proved to be the independent predictor of hemorrhage on ECMO. The indicators of diagnostic accuracy at this cutoff point were 67% (Sn), 79% (Sp), 62% (PPV), and 83% (NPV), respectively. Table 3 demonstrates the results of multivariate analysis. Table 4 presents the observed and predicted hospital mortalities calculated by the multivariate logistic regression model.
Discussion
This study is aimed at identifying the independent predictors of hospital mortality in adult trauma patients receiving ECMO for advanced cardiopulmonary dysfunctions. Due to the complicated technique and the high resource demand, ECMO is not a routine therapy for advanced cardiopulmonary dysfunctions. However, after experience accumulation, it can become a valuable salvage treatment for advanced cardiopulmonary dysfunctions induced by various etiologies. Based on our experience of handing the coagulopathy in patients requiring postcardiotomy ECMO support [16], we considered that all the surgical or trauma candidates must have their major bleeding sites identified and controlled before the delivery of ECMO. This is the most important selection criterion in our practice [8, 9]. Once ECMO is delivered to a patient with a high risk of hemorrhage, the heparin effect must be minimized even reversed during the support of ECMO [8, 9]. According to the current study, the mortality rates of the ECMO-treated post-traumatic shock and respiratory failure were 64% and 27%, respectively. Compare to our previous publications, the mortality rate of the ECMO-treated post-traumatic shock here was similar to the mortality rate of the ECMO-treated postcardiotomy shock (64% vs. 58%; p = 0.66) [16]. In the other hand, the mortality rate of the ECMO-treated post-traumatic respiratory failure here was lower than the mortality rate of the ECMO-treated non-traumatic respiratory failure (27% vs. 51%; p = 0.05) [17]. Therefore, we thought that ECMO could be a useful life support for advanced post-traumatic cardiopulmonary dysfunctions with a careful patient selection.
In the current study, an ISS > 35 and a refractory post-traumatic shock/CA were found to be independent predictors of hospital mortality in these ECMO-treated trauma patients. The two factors may build a simple classification model for this patient population. According to the Table 3, both the observed and predicted hospital mortality rates were over 80% in patients with the two features. A similar result is found while the classification was applied to a published cohort of 18 adult trauma patients who required ECMO support [4]. Therefore, the patient who has an ISS > 35 and developing a refractory post-traumatic shock/CA should be a suboptimal candidate for ECMO resuscitation, and the decision of enrolling should be made carefully. On the contrary, ECMO seems to be a promising therapeutic option for advanced post-traumatic respiratory failure. Post-traumatic respiratory failure is a common complication seen in patients with blunt chest trauma. Except for pulmonary contusions and transfusion-induced acute lung injury, there are some specific conditions may hinder the work of MV in trauma patients. These conditions include a significant air leak due to pulmonary lacerations, uncoordinated thoracic cage movements due to complex fractures, and restrictive intra-thoracic spaces due to abdominal compartment syndrome. Once thoracotomy is required for hemorrhage control, the associated one-lung ventilation may also bring additional volutrauma to the lungs and increase the risk of advanced respiratory failure after operation. Some of these injuries require surgical repairs but some are improved with lung rest and negative fluid balance. All these can be safely managed by an experienced ECMO team with multidisciplinary expertise [6, 8]. Therefore, if the major bleeding sites are controlled, VV-ECMO is indeed a valuable option to assist these young and previously healthy adults to conquer the temporary respiratory failure and survive.
In this study, twelve of the ECMO-treated trauma patients developed major hemorrhages on ECMO. Nine of the 12 hemorrhagic patients had a prolonged aPTT (> 40 s) before the administration of ECMO. As shown in Fig. 2, ECMO induces an abrupt rise of aPTT in all patients, including the patients treated with the heparin-minimized strategy. Patients with a prolonged aPTT before ECMO institution are quite vulnerable to the anticoagulation effects of heparin and might still lose blood from the oozing wounds due to the difficulty in formatting steady blood clots on ECMO, although the major bleeding sites had been controlled. Reversing the heparin with protamine, mitigating the consumption coagulopathy with blood transfusion, stabilizing the formed blood clots with antifibrinolytic agents, and allowing permissive hypotension are common strategies used to maintain an acceptable output of ECMO before hemostasis is achieved. However, permissive hypotension may inevitably prolong the period of hypoperfusion and jeopardize the survival rate. Therefore, the scale and duration of this hypocoagulation period should be a critical target for intervention while using ECMO to rescue patients with significant TIC. Despite not used in our practice yet, the viscoelastic assay is another valuable technique of coagulation monitoring in this scenario [3, 18].
Regardless of the indications, applying ECMO to patients with traumatic brain injury (TBI) is still a controversial issue. In the current study, four patients developed major ICHs on ECMO. One patient had a re-bleeding TBI, and 3 patients had newly developed ICHs. All of them received ECMO soon after admission, with a median ER-to-ECMO time of 11 h. In the other hand, the TBIs did not re-bleed in the other 3 patients who had a longer ER-to-ECMO time (47, 248 and 295 h, respectively). Therefore, the ER-to-ECMO time seemed to have an effect on re-bleeding from TBIs during ECMO, although a heparin-minimized strategy was adopted. Due to the small sample size, it is impossible to draw any definite conclusion to document the feasibility of delivering ECMO to patients with known TBI. To shorten this knowledge gap, we decided to perform a simple literature review of the case reports focusing on applying ECMO or similar device to patients with TBI. We collected eight English publications from PubMed that were published from 1999 to 2017 [19,20,21,22,23,24,25,26]. The eight studies, enrolling 21 patients with known TBI before ECMO, are summarized in Table 5. The therapeutic purpose is ventilation assistance in seven of the eight studies. The severity of TBI is significant in 19 patients in whom an extraventricular drainage is placed for intracranial decompression and pressure monitoring. Most of the patients have an ER-to-device time > 2 days, and a heparin-free ECMO is provided to patients with an ER-to-device time < 3 days. No TBI re-bleeding occurs, and just one hospital death is reported. According to the above-mentioned findings, ECMO with a heparin-free strategy seems to be safe in patients with minor or drained TBI. However, the summary could be more comprehensive if the therapeutic ranges of aPTT of the “heparin-free” ECMO are available.
The limitations of this study are its retrospective design and the small number of cases involved. The observations were obtained from the ECMO-treated patients only and all of the patients were highly selected by the ECMO team. Further prospective or large-scale retrospective studies are needed to demonstrate the efficacy and safety of ECMO used for post-traumatic cardiopulmonary failure.
Conclusion
The severity of trauma and the type of cardiopulmonary dysfunction significantly affected the outcomes of ECMO used for sustaining adult patients with post-traumatic cardiopulmonary dysfunction. According to our results, ECMO could be a useful salvage therapy for adult patients with post-traumatic cardiopulmonary dysfunctions if they had an ISS less than 35. Hemorrhage on ECMO remained a true concern while the device was required soon after trauma, although a heparin-minimized protocol was adopted.
Abbreviations
- APTT:
-
Activated partial thromboplastin time
- CA:
-
Cardiac arrest
- CRRT:
-
Continuous renal replacement therapy
- ECMO:
-
Extracorporeal membrane oxygenation
- ER:
-
Emergency room
- FiO2:
-
Fraction of inspiratory oxygen
- ICH:
-
Intracranial hemorrhage
- ISS:
-
Injury severity score
- MV:
-
Mechanical ventilation
- PaCO2 :
-
Arterial carbon dioxide tension
- PaO2 :
-
Arterial oxygen tension
- ROC:
-
Receiver operating characteristic
- SaO2 :
-
Arterial oxygen saturation
- SpO2 :
-
Oxyhemoglobin saturation by pulse oximetry
- TBI:
-
Traumatic brain injury
- TIC:
-
Trauma induced coagulopathy
- VA:
-
Venoarterial
- VV:
-
Venovenous
References
Rhee P, Joseph B, Pandit V, Aziz H, Vercruysse G, Kulvatunyou N, et al. Increasing trauma deaths in the United States. Ann Surg. 2014;260:13–21.
Lockey DJ, Lyon RM, Davies GE. Development of a simple algorithm to guide the effective management of traumatic cardiac arrest. Resuscitation. 2013;84:738–42.
Gonzalez E, Moore EE, Moore HB, Chapman MP, Chin TL, Ghasabyan A, et al. Goal-directed Hemostatic resuscitation of trauma-induced Coagulopathy: a pragmatic randomized clinical trial comparing a Viscoelastic assay to conventional coagulation assays. Ann Surg. 2016;263:1051–9.
Bonacchi M, Spina R, Torracchi L, Harmelin G, Sani G, Peris A. Extracorporeal life support in patients with severe trauma: an advanced treatment strategy for refractory clinical settings. J Thorac Cardiovasc Surg. 2013;145:1617–26.
Cordell-Smith JA, Roberts N, Peek GJ, Firmin RK. Traumatic lung injury treated by extracorporeal membrane oxygenation (ECMO). Injury. 2006;37:29–32.
Ried M, Bein T, Philipp A, Muller T, Graf B, Schmid C, et al. Extracorporeal lung support in trauma patients with severe chest injury and acute lung failure: a 10-year institutional experience. Crit Care. 2013;17:R110.
Arlt M, Philipp A, Voelkel S, Rupprecht L, Mueller T, Hilker M, et al. Extracorporeal membrane oxygenation in severe trauma patients with bleeding shock. Resuscitation. 2010;81:804–9.
Wu MY, Lin PJ, Tseng YH, Kao KC, Hsiao HL, Huang CC. Venovenous extracorporeal life support for post-traumatic respiratory distress syndrome in adults: the risk of major hemorrhages. Scand J Trauma Resusc Emerg Med. 2014;22:56.
Tseng YH, Wu TI, Liu YC, Lin PJ, Wu MY. Venoarterial extracorporeal life support in post-traumatic shock and cardiac arrest: lessons learned. Scand J Trauma Resusc Emerg Med. 2014;22:12.
Aberegg SK, Kirkby S, Crowley M. ECMO for respiratory support in adults. In: Gravlee GP, editor. Cardiopulmonary bypass: principles and practice. 3th Ed. Philadephia: Lippincott Willia & Wilkins, a Wolters Kluwer business; 2008. p. 632–46.
Bedeir K, Seethala R, Kelly E. Extracorporeal life support in trauma: worth the risks? J Trauma Acute Care Surg. 2017;82:400–6.
Thiagarajan RR, Barbaro RP, Rycus PT, Mcmullan DM, Conrad SA, Fortenberry JD, et al. Extracorporeal life support organization registry international report 2016. ASAIO J. 2017;63:60–7.
Johansson PI, Stensballe J, Ostrowski SR. Current management of massive hemorrhage in trauma. Scand J Trauma Resusc Emerg Med. 2012;9:47.
Gando S, Sawamura A, Hayakawa M. Trauma, shock, and disseminated intravascular coagulation: lessons from the classical literature. Ann Surg. 2011;254:10–9.
Huang YK, Liu KS, Lu MS, Wu MY, Tsai FC, Lin PJ. Extracorporeal life support in post-traumatic respiratory distress patients. Resuscitation. 2009;80:535–9.
Wu MY, Lin PJ, Lee MY, Tsai FC, Chu JJ, Chang YS, Haung YK, Liu KS. Using extracorporeal life support to resuscitate adult postcardiotomy cardiogenic shock: treatment strategies and predictors of short-term and midterm survival. Resuscitation. 2010;81:1111–6.
Cheng YT, Wu MY, Chang YS, Huang CC, Lin PJ. Developing a simple preinterventional score to predict hospital mortality in adult venovenous extracorporeal membrane oxygenation: a pilot study. Medicine (Baltimore). 2016;95:e4380.
Shere-Wolfe RF, Galvagno SM, Grissom TE. Critical care considerations in the management of the trauma patient following initial resuscitation. Scand J Trauma Resusc Emerg Med. 2012;18:68.
Reynolds HN, Cottingham C, McCunn M, Habashi NM, Scalea TM. Extracorporeal lung support in a patient with traumatic brain injury: the benefit of heparin-bonded circuitry. Perfusion. 1999;14:489–93.
Yen TS, Liu CC, Chen YS, Chao A. Extracorporeal membrane oxygenation resuscitation for traumatic brain injury after decompressive craniotomy. Clin Neurol Neurosurg. 2008;110:295–7.
Messing JA, Agnihothri R, Van Dusen R, Najam F, Dunne JR, Honig JR, et al. Prolonged use of extracorporeal membrane oxygenation as a rescue modality following traumatic brain injury. ASAIO J. 2014;60:597–9.
Muellenbach RM, Kredel M, Kunze E, Kranke P, Kuestermann J, Brack A, et al. Prolonged heparin-free extracorporeal membrane oxygenation in multiple injured acute respiratory distress syndrome patients with traumatic brain injury. J Trauma Acute Care Surg. 2012;72:1444–7.
Munoz-Bendix C, Beseoglu K, Kram R. Extracorporeal decarboxylation in patients with severe traumatic brain injury and ARDS enables effective control of intracranial pressure. Crit Care. 2015;19:381.
Biscotti M, Gannon WD, Abrams D, Agerstrand C, Claassen J, Brodie D, et al. Extracorporeal membrane oxygenation use in patients with traumatic brain injury. Perfusion. 2015;30:407–9.
Zhou R, Liu B, Lin K, Wang R, Qin Z, Liao R, et al. ECMO support for right main bronchial disruption in multiple trauma patient with brain injury--a case report and literature review. Perfusion. 2015;30:403–6.
Robba C, Ortu A, Bilotta F, Lombardo A, Sekhon MS, Gallo F, Matta BF. Extracorporeal membrane oxygenation for adult respiratory distress syndrome in trauma patients: a case series and systematic literature review. J Trauma Acute Care Surg. 2017;82:165–73.
Acknowledgements
We are grateful to all of the members in the Department of Trauma Surgery and the Department of Cardiothoracic Surgery in Chang Gung Memorial Hospital for their feedback on the patient survey.
Funding
This study was supported by no funding.
Availability of data and materials
The data that support the findings of this study are available from Chang Gung Memorial Hospital but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Chang Gung Memorial Hospital.
Author information
Authors and Affiliations
Contributions
WMY and CPL made contributions in study design and manuscript writing. WTI and LPJ made vast contributions in literature review, data collection, and data analysis. WMY made substantial contributions to manuscript composition and was responsible for the final product. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Chang Gung Medical Foundation Institutional Review Board (no. 2016-01610B0) approved the study and waived the requirement for informed consent due to the retrospective nature of this study.
Consent for publication
Not applicable. This study did not contain any individual person’s data in any form (including individual details, image or videos).
Competing interests
The authors declare they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1
Appendix 2
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wu, MY., Chou, PL., Wu, TI. et al. Predictors of hospital mortality in adult trauma patients receiving extracorporeal membrane oxygenation for advanced life support: a retrospective cohort study. Scand J Trauma Resusc Emerg Med 26, 14 (2018). https://doi.org/10.1186/s13049-018-0481-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13049-018-0481-6