
Abstract
Background
Ovarian mucinous carcinoma is a disease that requires unique treatment. But for a long time, guidelines for ovarian serous carcinoma have been used for the treatment of ovarian mucinous carcinoma. This study aimed to construct and validate nomograms for predicting the overall survival (OS) and cancer-specific survival (CSS) in patients with ovarian mucinous adenocarcinoma.
Methods
In this study, patients initially diagnosed with ovarian mucinous adenocarcinoma from 2004 to 2015 were screened from the Surveillance, Epidemiology, and End Results (SEER) database, and divided into the training group and the validation group at a ratio of 7:3. Independent risk factors for OS and CSS were determined by multivariate Cox regression analysis, and nomograms were constructed and validated.
Results
In this study, 1309 patients with ovarian mucinous adenocarcinoma were finally screened and randomly divided into 917 cases in the training group and 392 cases in the validation group according to a 7:3 ratio. Multivariate Cox regression analysis showed that the independent risk factors of OS were age, race, T_stage, N_stage, M_stage, grade, CA125, and chemotherapy. Independent risk factors of CSS were age, race, marital, T_stage, N_stage, M_stage, grade, CA125, and chemotherapy. According to the above results, the nomograms of OS and CSS in ovarian mucinous adenocarcinoma were constructed. In the training group, the C-index of the OS nomogram was 0.845 (95% CI: 0.821–0.869) and the C-index of the CSS nomogram was 0.862 (95%CI: 0.838–0.886). In the validation group, the C-index of the OS nomogram was 0.843 (95% CI: 0.810–0.876) and the C-index of the CSS nomogram was 0.841 (95%CI: 0.806–0.876). The calibration curve showed the consistency between the predicted results and the actual results, indicating the high accuracy of the nomogram.
Conclusion
The nomogram provides 3-year and 5-year OS and CSS predictions for patients with ovarian mucinous adenocarcinoma, which helps clinicians predict the prognosis of patients and formulate appropriate treatment plans.
Similar content being viewed by others

Introduction
Ovarian cancer has the highest mortality rate among gynecologic malignancies [1]. Most ovarian cancer patients present with advanced disease at the time of initial diagnosis [2]. As one of the 10 most common cancers in women, the mortality rate of ovarian cancer is increasing [3]. There are an estimated 21,410 new cases of ovarian cancer and an estimated 13,770 deaths in the United States in 2021 [4]. Ovarian epithelial tumors are the most common histological type of ovarian cancer, which can be classified as benign, borderline, and malignant. The common types of ovarian epithelial tumors are serous tumors, mucinous tumors, ovarian endometrioid tumors, and clear cell tumors. Primary mucinous ovarian carcinoma is relatively rare among ovarian cancers [5]. A careful understanding of its biological characteristics shows that ovarian mucinous carcinoma is a disease that requires unique treatment. But for a long time, guidelines for ovarian serous carcinoma have been used for the treatment of ovarian mucinous carcinoma [6]. Therefore, it is significant to develop a predictive model to predict the prognosis and formulate individualized treatment plans for ovarian mucinous adenocarcinoma.
The nomogram predicts the probability of clinical events by integrating different determinants, which is in line with personalized medicine. Currently, the use of nomograms is also increasing [7]. Wang et al. [8] retrospectively analyzed 172 patients with primary ovarian signet cell carcinoma and constructed 1-year, 3-year, and 5-year OS nomograms, which were helpful for clinicians to assess the prognosis of patients. Wang et al. [9] screened 131,050 patients with epithelial ovarian cancer from the seed database and constructed nomograms of OS and CSS. Compared with the FIGO 2018 staging system, nomograms provided a better predictive effect.
In this study, we constructed and validated 3-year and 5-year OS and CSS nomograms in patients with ovarian mucinous adenocarcinoma based on the Surveillance, Epidemiology, and End Results (SEER) database. Nomograms help clinicians predict patient outcomes and formulate individualized treatment plans.
Material and methods
Patients selection
The Surveillance, Epidemiology, and End Results (SEER) database collects information on the demographics and clinical characteristics of cancer patients from cancer registries covering 47.9% of the U.S. population and publishes cancer incidence and mortality. It is updated once a year and is available to people for free [10]. We extracted relevant data from the SEER database for retrospective analysis by SEER*Stat 8.3.9 software (https://seer.cancer.gov/).
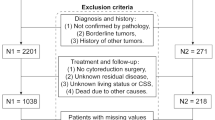
We use the third edition of the International Classification of Diseases Oncology Special Edition (ICD-O-3) to screen for ovarian mucinous adenocarcinoma. ICD-O-3 includes anatomical codes and morphological codes. The inclusion criteria were the pathologically confirmed malignant mucinous adenocarcinoma as the first primary tumor and patients with anatomical codes (C56.9 (ovary)) between 2004 and 2015. The morphological codes were: 8470/3, 8471/3, 8472/3, 8473/3, 8480/3, and 8482/3. Then, we excluded Unknown Race recode(n = 17), Unknown marital status at diagnosis(n = 112), Unknown grade(n = 746), Paired site, but no information concerning laterality(n = 31), and Unknown CA125(n = 542). The flowchart is shown in Fig. 1.

Flowchart for screening patients. A total of 2757 patients initially diagnosed with primary ovarian mucinous adenocarcinoma between 2004 and 2015 were screened through the database, of which 1309 were included in the analysis
Predictors
We download the following data from the database: age, race, marital status, laterality, grade, AJCC TNM stage, CA125, surgery at the primary site, radiation therapy, chemotherapy, survival time, cause of death, and vital status. We included these data in subsequent analyses. This study focused on overall survival (OS) and cancer-specific survival (CSS). OS was defined as the time from diagnosis to death or last follow-up. CSS was defined as the time from diagnosis to death due to ovarian mucinous adenocarcinoma or last follow-up.
Statistic methods
In this study, 1309 patients with ovarian mucinous adenocarcinoma were finally screened and randomly divided into the training group and the validation group according to the ratio of 7:3 by R software (version 4.0.3). Finally, there were 917 cases in the training group and 392 cases in the validation group. We used X-tile software (version 3.6.1) to determine the optimal cut-off point for age (12–57 years, 58–70 years, 71–92 years) (Fig. 2).

Identification of the best cut-off point of age (A, B) through X-tile software
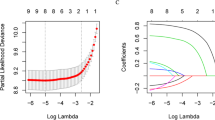
We compared the variables screened in the training group and the validation group by Chi-square test. The p-value> 0.05 indicates that there is no statistical difference between the two groups, in other words, the two groups are comparable. Univariate Cox regression analysis was performed on the variables of the training group to screen out the risk factors related to OS and CSS in ovarian mucinous adenocarcinoma (p < 0.05). We performed multivariate Cox regression analysis of selected risk factors (p < 0.05). According to the risk factors screened by multivariate Cox regression analysis (p < 0.05), we could determine independent risk factors for OS and CSS. Prognostic nomograms of OS and CSS at 3 and 5 years were constructed according to their respective independent risk factors. We evaluated the discriminative ability of the model by the area under the ROC curve (AUC) and the C-index. Their value ranges and meanings were similar. Different ranges of AUC represent different meanings. The model had no predictive ability: AUC = 0.50; low accuracy: 0.50 < AUC ≤ 0.70; moderate accuracy: 0.70 < AUC ≤ 0.90; high accuracy: > 0.90. The C-index evaluated the probability that the predicted result was consistent with the actual observed result. It was used to evaluate the predictive ability of the model. The accuracy of the model was evaluated by the calibration curve, that is, it was used to compare the fit between the predicted situation and the actual situation. Taking the 45°diagonal in the figure as the reference line, the closer the actual probability line is to the reference line, the higher the accuracy of the model will be. The model was internally validated by the validation group, which verified the discriminative ability and accuracy of the model. All statistical analyses were performed with SPSS (version 25.0) and R software (version 4.0.3). A p-value < 0.05 was considered statistically significant.
Results
Demographic and clinical characteristics
A total of 1309 patients with ovarian mucinous adenocarcinoma were included in this study, including 917 (70.1%) in the training group and 392 (29.9%) in the validation group. Most patients were younger (12-57 years, 64.3%), white (80.0%), and married (48.7%) (Table 1). The majority of tumors were unilateral (88.5%), grade II (43.5%), AJCC stage T1 (74.1%), AJCC stage N0 (91.7%) and AJCC stage M0 (91.4%) (Table 1). Blood CA125 was mostly positive (67.6%) (Table 1). The vast majority of patients underwent surgery (99.2%), nearly half underwent chemotherapy (47.1%), and fewer patients underwent radiation therapy (0.9%) (Table 1).
Independent risk factors for OS and CSS in patients with ovarian mucinous adenocarcinoma
Through univariate and multivariate Cox regression analysis on the training group data, the independent risk factors of OS and CSS were screened out. Univariate Cox regression analysis showed that they (age, race, marital, laterality, grade, T_stage, N_stage, M_stage, CA125, surgery, radiation, chemotherapy) were related to OS and CSS (P < 0.05) (Tables 2 and 3). After multivariate Cox regression analysis of the above factors, it could be concluded that the independent risk factors for OS were age, race, T_stage, N_stage, M_stage, grade, CA125, and chemotherapy (Table 2). Independent risk factors of CSS were age, race, marital, T_stage, N_stage, M_stage, grade, CA125, and chemotherapy (Table 3).
Construction of nomograms
The nomogram of OS was constructed according to the independent risk factors (age, race, T_stage, N_stage, M_stage, grade, CA125, and chemotherapy) of OS (Fig. 3). The nomogram of CSS was constructed according to the independent risk factors (age, race, marital, T_stage, N_stage, M_stage, grade, CA125, and chemotherapy) of CSS (Fig. 3).

Nomograms for predicting 3-, and 5-year overall survival (OS) and cancer-specific survival (CSS) in ovarian mucinous adenocarcinoma. A, 3-, and 5-year overall survival; B, 3-, and 5-year cancer-specific survival
Nomogram validation
In the training group, the C-index of the OS nomogram was 0.845 (95% CI: 0.821–0.869) and the C-index of the CSS nomogram was 0.862 (95%CI: 0.838–0.886). The area under the ROC curves for both 3-year and 5-year OS and CSS nomograms was large in the training group (Fig. 4). The above results indicated that the model had a high discriminative ability. The calibration curves of 3-year and 5-year OS and CSS nomograms in the training group were very close to the reference line, indicating that the accuracy of nomograms was relatively high (Fig. 5).

ROC curves in the training (A, B) and validation (E, F) groups for 3-, and 5-year overall survival. ROC curves in the training (C, D) and validation (G, H) groups for 3-, and 5-year cancer-specific survival. ROC, receiver operating characteristic

Calibration curves in the training (A, B) and validation (E, F) groups for 3-, and 5-year overall survival. Calibration curves in the training (C, D) and validation (G, H) groups for 3-, and 5-year cancer-specific survival
In addition, we did an internal validation. In the validation group, the C-index of the OS nomogram was 0.843 (95% CI: 0.810–0.876) and the C-index of the CSS nomogram was 0.841 (95%CI: 0.806–0.876). The area under the ROC curves for both 3-year and 5-year OS and CSS nomograms was large in the validation group (Fig. 4). The above results indicated that the model had a high discriminative ability. The calibration curves of 3-year and 5-year OS and CSS nomograms in the validation group were very close to the reference line, indicating that the accuracy of nomograms was relatively high (Fig. 5).
Kaplan-Meier curves
The KM method first calculates the probability that a patient who has survived a certain period of time will survive the next period (the survival probability) and then multiplies the survival probabilities one by one to obtain the survival rate for the corresponding period. Older age (71–92), black race, grade III, IV, advanced T, N, and M stages, CA125 positive, chemotherapy, and high-risk level were associated with lower overall survival of the tumor (Figs. 6 and 8). Older age (71–92), black race, separated, grade III, IV, advanced T, N, and M stages, CA125 positive, chemotherapy, and high-risk level were associated with lower cancer-specific survival of the tumor (Figs. 7 and 8).

Kaplan-Meier survival curves for overall survival (A, B, C, D, E, F, G, H) in ovarian mucinous adenocarcinoma patients. A, Age; B, Race; C, Grade; D, T_stage; E, M_stage; F, N_stage; G, CA125; H, Chemotherapy

Kaplan-Meier survival curves for cancer-specific survival (A, B, C, D, E, F, G, H, I) in ovarian mucinous adenocarcinoma patients. A, Age; B, Race; C, Marital; D, Grade; E, T_stage; F, M_stage; G, N_stage; H, CA125; I, Chemotherapy

Kaplan-Meier survival curves for the risk-level of overall survival (A) and cancer-specific survival (B) in ovarian mucinous adenocarcinoma patients
Discussion
Recently, nomograms have been used by clinicians to predict the prognosis of various tumors and formulate individualized treatment plans, such as breast cancer, liver cancer, lung cancer, gastric cancer, and cervical cancer [11,12,13,14,15]. Of course, nomograms also have extensive research in predicting the prognosis of patients with ovarian cancer. Chen et al. [16] selected 1541 patients screened from the SEER database who were initially diagnosed with ovarian clear cell carcinoma (OCCC) during 2010–2016 and randomly divided them into the training group (n = 1079) and the validation group (n = 462). The 3-year and 5-year OS and CSS nomograms were constructed and validated, with high predictive and clinical value [16]. Wang et al. [17] screened 9001 cases of epithelial ovarian cancer through the SEER database and randomly divided them into the training group (n = 6301) and the validation group (n = 2700). They constructed and validated 3-year and 5-year OS and CSS nomograms of the disease, which played a role in evaluating prognosis and guiding clinical treatment [17]. Song et al. [18] included 13,403 patients with advanced epithelial ovarian cancer and constructed the early death nomogram of FIGO Stage III and IV epithelial ovarian cancer patients. The internal validation confirmed that the nomogram was highly accurate in predicting premature death and helpful in screening patients with high clinical risk with high practicality [18]. You et al. [19] included 506 eligible patients with postoperative ovarian sex cord-stromal tumor (SCST) from the SEER database. They constructed and validated the OS nomogram, which showed that it was more practical than FIGO staging [19].
As one of the 10 most common cancers in women, the mortality rate of ovarian cancer is increasing [3]. Ovarian mucinous carcinoma is one of the major subtypes of ovarian cancer. A careful understanding of its biological characteristics shows that ovarian mucinous carcinoma is a disease that requires unique treatment. But for a long time, guidelines for ovarian serous carcinoma have been used for the treatment of ovarian mucinous carcinoma [6]. Therefore, it is important to construct a valuable prognostic model to predict the prognosis of ovarian mucinous adenocarcinoma.
In this study, we identified prognostic factors for OS and CSS in the training group by univariate and multivariate Cox regression analysis of the basic information and disease information of patients in the database. Prognostic factors affecting OS were age, race, T_stage, N_stage, M_stage, grade, CA125, chemotherapy. The above factors, together with marital, were prognostic factors for CSS. Based on multivariate Cox regression analysis, we established a prognostic nomogram for OS and CSS in patients with ovarian mucinous adenocarcinoma. In the training group, through the calculation of the C-index, the drawing of the ROC curve and the calibration curve, the results showed that the prognostic model had the higher discriminative ability and higher accuracy. In addition, internal validation was performed by the validation group.
In the nomogram, it could be seen that T_stage played the greatest role in the prognosis prediction, followed by CA125. CA125 is a tumor marker for ovarian cancer. Its sensitivity is related to the stage and histological type of ovarian cancer. It can be used for the early monitoring of disease recurrence and the monitoring of treatment [20]. From the survival curve, we could see that the elderly seemed to have a lower survival rate than the young. Consistent with previous reports, the black race had a lower survival rate than American Indian/AK Native, Asian/Pacific Islander, and white race [21].
In addition, the limitations of this study needed to be noted. Firstly, patients were mainly from the United States, and there was a lack of disease information for patients in other countries, especially Chinese patients with a large population. Secondly, retrospective analysis of the database resulted in selection bias. Finally, the data of surgery, radiation therapy, and chemotherapy in the database only had the results of YES and NO or Unknown and lacked detailed treatment plans.
Conclusion
In conclusion, this study showed that age, race, T_stage, N_stage, M_stage, grade, CA125, and chemotherapy were independent risk factors for OS in patients with ovarian mucinous adenocarcinoma. In addition, age, race, marital, T_stage, N_stage, M_stage, grade, CA125, and chemotherapy were independent risk factors for CSS. This study constructed and validated 3-year and 5-year prognosis nomograms for OS and CSS in patients with ovarian mucinous adenocarcinoma. Nomograms helped clinicians predict the OS and CSS of patients with ovarian mucinous adenocarcinoma and formulate appropriate treatment plans.
Availability of data and materials
The datasets analyzed during the current study are available from the publicly available SEER database.
References
Javadi S, Ganeshan DM, Qayyum A, et al. Ovarian Cancer, the revised FIGO staging system, and the role of imaging. AJR Am J Roentgenol. 2016;206(6):1351–60.
Armstrong DK, Alvarez RD, Bakkum-Gamez JN, et al. Ovarian Cancer, version 2.2020, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2021;19(2):191–226.
Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–32.
Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7–33.
Ledermann JA, Luvero D, Shafer A, et al. Gynecologic Cancer InterGroup (GCIG) consensus review for mucinous ovarian carcinoma. Int J Gynecol Cancer. 2014;24(9 Suppl 3):S14–9.
Morice P, Gouy S, Leary A. Mucinous Ovarian Carcinoma. N Engl J Med. 2019;380(13):1256–66.
Balachandran VP, Gonen M, Smith JJ, et al. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–80.
Wang X, Ke X, Min J. A prognostic nomogram for women with primary ovarian signet-ring cell carcinoma. Ann Transl Med. 2021;9(7):525.
Wang B, Wang S, Ren W. Development and validation of a nomogram to predict survival outcome among epithelial ovarian cancer patients with site-distant metastases: a population-based study. BMC Cancer. 2021;21(1):609.
Overview of the SEER Program. (2021). Available at: https://seer.cancer.gov/about/overview.html (Accessed Aug 2021).
Li N, Feng LW, Li ZN, et al. Construction and validation of a nomogram to predict overall survival in very young female patients with curatively resected breast Cancer. Cancer Manag Res. 2021;13:6181–90.
Ni X, Li D, Dai S, et al. Development and evaluation of nomograms to predict the Cancer-specific mortality and overall mortality of patients with hepatocellular carcinoma. Biomed Res Int. 2021;2021:1658403.
Wang Z, Li H, Liu T, et al. Development and external validation of a nomogram for predicting Cancer-specific survival of non-small cell lung Cancer patients with ipsilateral pleural dissemination. Front Oncol. 2021;11:645486.
Che K, Wang Y, Wu N, et al. Prognostic nomograms based on three lymph node classification Systems for Resected Gastric Adenocarcinoma: a large population-based cohort study and external validation. Ann Surg Oncol. 2021;28(13):8937–49.
Yu W, Huang L, Zhong Z, et al. A nomogram-based risk classification system predicting the overall survival of patients with newly diagnosed stage IVB cervix uteri carcinoma. Front Med (Lausanne). 2021;8:693567.
Chen Q, Wang S, Lang JH. Development and validation of nomograms for predicting overall survival and Cancer-specific survival in patients with ovarian clear cell carcinoma. J Ovarian Res. 2020;13(1):123.
Wang R, Xie G, Shang L, et al. Development and validation of nomograms for epithelial ovarian cancer: a SEER population-based, real-world study. Future Oncol. 2021;17(8):893–906.
Song Z, Zhou Y, Bai X, et al. A practical nomogram to predict early death in advanced epithelial ovarian Cancer. Front Oncol. 2021;11:655826.
You D, Zhang Z, Cao M. Development and validation of a prognostic prediction model for postoperative ovarian sex cord-stromal tumor patients. Med Sci Monit. 2020;26:e925844.
Molina R, Filella X, Jo J, et al. CA 125 in biological fluids. Int J Biol Markers. 1998;13(4):224–30.
Wang W, Liu J, Liu L. Development and validation of a prognostic model for predicting overall survival in patients with bladder Cancer: a SEER-based study. Front Oncol. 2021;11:692728.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
LY, JFY and SZ searched the database and analysis data. LY, YSS, YJL, LGX and JHZ wrote the manuscript text. JYZ reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study received ethical approval from the Ethics Committee of Zhangjiagang TCM Hospital Affiliated to Nanjing University of Chinese Medicine.
Consent for publication
No conflict.
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yang, L., Yu, J., Zhang, S. et al. A prognostic model of patients with ovarian mucinous adenocarcinoma: a population-based analysis. J Ovarian Res 15, 26 (2022). https://doi.org/10.1186/s13048-022-00958-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13048-022-00958-6