
Abstract
Background
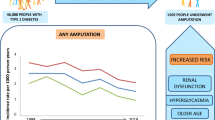
The prevalence of diabetes is rising, and diabetes develops at a younger age in East Asia. Although lower limb amputation negatively affects quality of life and increases the risk of cardiovascular events, little is known about the rates and predictors of amputation among persons with diabetes from young adults to those in the “young-old” category (50–72 y).
Methods
We analyzed data from a nationwide claims database in Japan accumulated from 2008 to 2016 involving 17,288 people with diabetes aged 18–72 y (mean age 50.2 y, HbA1c 7.2%). Amputation occurrence was determined according to information from the claims database. Cox regression model identified variables related to lower limb amputation.
Results
The mean follow-up time was 5.3 years, during which time 16 amputations occurred (0.17/1000 person-years). Multivariate Cox regression analysis showed that age (hazard ratio [HR] 1.09 [95% confidence intervals] 1.02–1.16, p = 0.01) and HbA1c (HR 1.46 [1.17–1.81], p < 0.01) were independently associated with amputations. Compared with those aged < 60 years with HbA1c < 8.0%, the HR for amputation was 27.81 (6.54–118.23) in those aged ≥60 years and HbA1c ≥8.0%.
Conclusions
Age and HbA1c were associated with amputations among diabetic individuals, and the rates of amputation were significantly greater in those ≥60 years old and with HbA1c ≥8.0%.
Similar content being viewed by others


Background
The prevalence of type 2 diabetes is rising in Asia, characterized by onset at a relatively young age and low body mass index (BMI) compared with Western countries [1,2,3]. Diabetes-related complications, including lower-extremity amputation, are a significant cause of increased mortality among people with diabetes and have substantial economic consequences [4,5,6]. Lower limb amputation not only markedly reduces patients’ quality of life [7] but also increases risks of cardiovascular events and death [8, 9]. Gujral et al. reported that the age- and sex-adjusted incidence rate of lower limb amputation for those with diabetes mellitus of Asian ethnic origin was estimated to be 0.34 (95% confidence interval (CI), 0.11–1.07) cases per 1000 person-years compared to 1.42 (1.26–1.59) in Caucasians [10]. However, since diabetes develops at a younger age in East Asia, a study directly exploring this issue among Japanese diabetic individuals from young adults to those in the “young-old” category is needed.
Longer exposure to glycated haemoglobin A1c (HbA1c) levels above target was associated with increased risk of both micro- and macrovascular complications [11, 12]. However, a recent meta-analysis evaluating risk factors for lower extremity amputation in patients with diabetic foot ulcers showed that HbA1c levels do not affect the incidence of amputation [13]. Studies included in that meta-analysis were only on patients with diabetic foot ulcers who had received recent intensive treatment [13], suggesting that the impact of HbA1c on amputation may have been underestimated.
Age is an established independent risk factor for atherosclerosis and macrovascular complications in people with diabetes [14, 15]. However, a meta-analysis showed that age was not related to amputation in diabetic foot ulcer patients [13]. In most studies, the average participants are middle aged or older [10, 16, 17]. Thus, the impact of age on lower limb amputation is not clear among Japanese diabetic individuals ranging from young adults to the “young-old” (50–72 y). Therefore, we aimed to determine the rates of lower limb amputations and risk factors for lower limb amputations in Japanese people with diabetes among young adults to those in the “young-old” category.
Methods
Database
Data were obtained from a nationwide claims database that was provided by JMDC Inc. Details of the database were described previously [15, 18]. Briefly, the JMDC collects claims data from approximately 6,000,000 people who belong to a health insurance provider for company employees and their dependents. This database also has data on annual medical check-ups for some of its participants that include data on blood tests [19].
Study population
People aged 18–72 years who had been followed for at least 3 years between 1 April 2008 and 31 March 2013 were included and followed up to 31 August 2016. For the present study, we examined data on 296,504 individuals. We then excluded 278,831 individuals who did not meet the definition of diabetes and/or required amputation within 1 month of enrollment and/or who had missing data. Finally, this study included 17,288 individuals with diabetes who had at least a 1-year amputation-free period before baseline (Fig. 1). The point of entry to the study was the earliest date for health examination data between 1 April 2008 and 31 March 2013. Mean age and HbA1c value were 50.2 years and 7.2%, respectively.

Flow chart for the extraction of study participants
Definitions
Diabetes was determined by fasting plasma glucose (FPG) ≥7.0 mmol/L or HbA1c ≥6.5% or both without prescription of an antidiabetic drug or with a prescription of an antidiabetic drug regardless of FPG or HbA1c. Blood pressure was measured at all participating facilities in accordance with the guidelines of the Japanese Society of Hypertension [20, 21]. For medical checkups, these guidelines recommended measuring blood pressure twice by the oscillometric method and averaging the results.
Occurrence of amputation was determined according to claims using Diagnosis Procedure Combination (Japanese original codes), the International Classification of Diseases 10th revision (ICD-10) codes and medical procedure data after 1 month of follow-up (Supplemental Table 1). Since we could not completely exclude patients with a past history of lower limb amputation, we used the term “rates of amputation”.
Statistical analysis
Categorical variables were expressed as numerals and percentages. Continuous variables were expressed as the mean ± standard deviations (SD). For comparison between those with and without amputation, χ2 tests were used for the categorical variables. The unpaired Student’s t test or the Mann-Whitney U test based on distribution was used for continuous variables. Cox regression model identified variables related to amputation. First, we conducted a univariate analysis to determine the significant variable for amputation. Then, we performed a multivariate analysis using variables with P < 0.1 in the univariate analysis as covariates. We used categorical variables to clarify the impact of combinations of age and HbA1c on lower limb amputation.
Analyses were performed using SPSS (version 19.0, Chicago, IL, USA). Statistical significance was considered at P < 0.05. The Ethics Committee of the Niigata University approved this study.
Results
Median and maximum follow-up periods were 5.3 and 8.4 years, respectively. During the study period, 16 study participants experienced a new amputation. The rate of amputation was 0.17 per 1000 person-years. Baseline characteristics of those who had or had not experienced amputation during the observational period are summarized in Table 1. Individuals with amputation were significantly older than those without amputation. The levels of HbA1c, systolic blood pressure (SBP), diastolic blood pressure (DBP) and the rate of current smoking were higher in patients with amputation compared to patients without amputation; however, no statistical differences were observed. The percentages of participants aged ≥60 years and with HbA1c ≥8.0% were significantly higher in patients with amputation compared to patients without amputation.
Univariate Cox regression analysis showed that age (hazard ratio [HR] 1.08 [95% confidence intervals] 1.02–1.16, p = 0.01), DBP 5 mmHg increase (HR 0.79 (0.63–0.99), p = 0.04) and HbA1c (HR 1.38 [1.11–1.71], p < 0.01) were independently associated with amputation (Table 2). Multivariate Cox regression analysis showed that age (hazard ratio [HR] 1.09 [1.02–1.16], p < 0.01) and HbA1c (HR 1.46 [1.17–1.81], p < 0.01) were independently associated with amputation (Table 2). Figure 2 shows HRs according to age, HbA1c and their combinations for amputation analyzed by multivariate Cox models. Compared with those aged < 60 years with HbA1c < 8.0%, the HR was 3.77 (1.09–13.04) for those aged ≥60 years with HbA1c < 8.0%, 3.96 (0.93–16.78), for those aged < 60 years with HbA1c ≥8.0% and 27.81 (6.54–118.23) for those aged ≥60 years with HbA1c ≥8.0%.

Hazard ratios for lower limb amputation according to combinations of HbA1c and age. The hazard ratio (HR) for those aged ≥60 years with HbA1c < 8.0% was 3.77 (95% confidence interval (CI) 1.09–13.04) and the HR for those aged < 60 years with HbA1c ≥8.0% was 3.96 (95% CI 0.93–16.78). The HR for those aged ≥60 years with HbA1c ≥8.0% was 27.81 (95% CI 6.54–118.23) compared with those aged < 60 years with HbA1c < 8.0% (reference group). Adjusted for diastolic blood pressure
Discussion
In this study, we found that lower limb amputation frequency was low among young-adults to young-old Japanese people with diabetes. Age and HbA1c were associated with amputation. Compared with persons aged < 60 years and with HbA1c < 8.0%, the risk for amputation was significantly higher among those aged ≥60 years and with HbA1c ≥8.0%.
In USA, the most common causes of limb loss are diabetes with an age-adjusted incidence rate of 2.8 per 1000 person-years in people with diabetes [5]. In Taiwan, the trends for both major and minor lower limb amputation rates were decreased with incidence rates of 1.09 and 0.98 per 1000 person-years, respectively [22]. A recent study conducted in Japan showed that the incidence of diabetic foot ulcers and amputation were 2.9 and 0.47 per 1000 person-years, respectively [16]. In that study, the mean age was 65 years [16], which was much higher than in our study. In our study, the rate of amputation was 0.17 per 1000 person-years, which was extremely low compared to previous studies [16, 22]. These differences reflected differences in characteristics between study participants. For example, the mean age was younger in our study. Older patients may have a longer disease duration, higher number of comorbidities and poorer glycemic control, resulting in a higher incidence of amputation than in younger patients.
Adler et al. showed that there is a substantial increase in the risk of lower limb amputation associated with glycemia in individuals with diabetes [23]. In our multivariate analysis, HbA1c was independently associated with amputation. Interestingly, a recent meta-analysis showed that the HbA1c level does not affect the incidence of amputation in patients with diabetic foot ulcers [13]. Intensive control may decrease the risk of amputation in patients with diabetic foot syndrome [24]. Taken together, glycemic control may help reduce the frequency of lower limb amputations through reducing the development of diabetic foot ulcers, wound progression and progression of neuropathy.
Age plays an important role in atherosclerosis, resulting in an increased risk of cardiovascular disease. No clear association was observed between age and amputation in patients with diabetic foot ulcers [13]. We found that age was independently associated with lower limb amputation, which was consistent with a previous study [25]. Moreover, the risk for amputation was drastically higher among those aged ≥60 years and with HbA1c ≥8.0% compared with patients aged < 60 years and with HbA1c < 8.0% in our study of Japanese with diabetes. However, the sample size for stratified analysis of events was too small to conclude an association between HbA1c and lower limb amputation. Thus, future studies are needed to confirm our findings with an adequate sample size.
Hypertension was associated with both micro- and macro diabetic complications [26, 27]. Although hypertension is approximately twice as frequent in patients with than without diabetes [28], one third of persons with diabetes do not reach target blood pressure values [29]. Therefore, early and sustained blood pressure control is necessary to prevent not only cardiovascular disease but also lower limb amputation in clinical practice.
Our analysis did not show smoking as a significant risk factor for lower limb amputation. However, smoking remains a risk factor for cardiovascular events [30, 31]. Therefore, no conclusion can be drawn regarding the association between smoking and lower limb amputation from our study and future studies that stratify current, past and no smoking are needed.
BMI was not associated with lower limb amputation in this study. Chan et al. showed that the prevalence of obesity was higher in urban than in rural residents in Asia [32]. Generally, lower BMI was associated with increased mortality risk [33]. Unfortunately, we have no data as to whether a study participant resided in a rural or urban area. Another possibility is that our findings reflected an obesity paradox in patients with diabetes [34].
It was noted that men do not examine or look at their feet as often as women do, suggesting a lower level of foot care in men [35]. In our study, only two of the 16 amputations occurred in women. A meta-analysis showed that sex differences existed in the prevalence of glucose tolerance status [36]. However, in our univariate analysis, male sex was not associated with amputation. This may be due to the high proportion of males among both those with and without amputation in our cohort, which was different from both other cohorts and the national level in Japan [12] [37] [38]. Thus, our finding should be interpreted with caution and future studies of adequate populations are necessary to confirm the impact of sex differences on amputation among Japanese young adults to those classified as “young-old”.
This study’s strengths were the large sample size and accurate capture of diabetes diagnoses and lower limb amputation using data from health examinations, medical practice and a claims database. However, several limitations should be addressed. First, the sample size for amputation was too small to establish rates and predictors of amputation. Moreover, we do not have data on diabetic foot ulcers. Unfortunately, ICD-10 codes for diabetic foot ulcer are not commonly used in clinical settings in Japan. Therefore, we cannot accurately identify patients who had diabetic foot ulcers from claims data. Also, we could not distinguish between first, second and subsequent amputations from our database. However, we included patients who had least a 1-year amputation-free period before baseline using claims data. We attempted to distinguish between major and minor amputations. However, the number of amputations was too small to conduct a stratified analysis. Secondly, we have no data on details of smoking status and could not distinguish between never-smokers and former smokers. Thus, our findings should be interpreted with caution in regard to the impact of smoking on amputation. Thirdly, it was not possible to identify participants whose HbA1c, SBP or DBP had either improved or deteriorated during the follow-up period, as these values were measured at only one point in time. Fourth, we could not obtain information on the duration of diabetes, social factors and psychiatric factors that would affect the incidence of amputation. Fifth, the number of lower limb amputations may be underestimated due to coding errors.
Conclusions
Age and HbA1c were associated with amputation. Compared with patients aged < 60 years and with HbA1c < 8.0%, the risk for amputation was much higher among those aged ≥60 years and HbA1c ≥8.0%, suggesting the need for ethnic group-specific strategies to prevent diabetic foot disease.
Availability of data and materials
The data and study materials will not be made available to other researchers for purposes of reproducing the results or replicating the procedure.
Abbreviations
- DBP:
-
Diastolic blood pressure
- FPG:
-
Fasting plasma glucose
- HbA1c:
-
Haemoglobin A1c
- HRs:
-
Hazard ratios
- BMI:
-
Body mass index
- SBP:
-
Systolic blood pressure
- ICD-10:
-
International Classification of Diseases 10th revision
References
Ma RC, Chan JC. Type 2 diabetes in east Asians: similarities and differences with populations in Europe and the United States. Ann N Y Acad Sci. 2013;1281(1):64–91. https://doi.org/10.1111/nyas.12098.
Chan JC. Diabetes and noncommunicable disease: prevent the preventables. Jama. 2013;310(9):916–7. https://doi.org/10.1001/jama.2013.168099.
Hsu WC, Araneta MR, Kanaya AM, Chiang JL, Fujimoto W. BMI cut points to identify at-risk Asian Americans for type 2 diabetes screening. Diabetes Care. 2015;38(1):150–8. https://doi.org/10.2337/dc14-2391.
Graz H, D'Souza VK, Alderson DEC, Graz M. Diabetes-related amputations create considerable public health burden in the UK. Diabetes Res Clin Pract. 2018;135:158–65. https://doi.org/10.1016/j.diabres.2017.10.030.
Gregg EW, Li Y, Wang J, Burrows NR, Ali MK, Rolka D, et al. Changes in diabetes-related complications in the United States, 1990-2010. N Engl J Med. 2014;370(16):1514–23. https://doi.org/10.1056/NEJMoa1310799.
Resnick HE, Carter EA, Sosenko JM, Henly SJ, Fabsitz RR, Ness FK, et al. Incidence of lower-extremity amputation in American Indians: the strong heart study. Diabetes Care. 2004;27(8):1885–91. https://doi.org/10.2337/diacare.27.8.1885.
Hogg FR, Peach G, Price P, Thompson MM, Hinchliffe RJ. Measures of health-related quality of life in diabetes-related foot disease: a systematic review. Diabetologia. 2012;55(3):552–65. https://doi.org/10.1007/s00125-011-2372-5.
Apelqvist J, Larsson J, Agardh CD. Long-term prognosis for diabetic patients with foot ulcers. J Intern Med. 1993;233(6):485–91. https://doi.org/10.1111/j.1365-2796.1993.tb01003.x.
Meshkin DH, Zolper EG, Chang K, Bryant M, Bekeny JC, Evans KK, et al. Long-term mortality after nontraumatic major lower extremity amputation: a systematic review and meta-analysis. J Foot Ankle Surg. 2020. https://doi.org/10.1053/j.jfas.2020.06.027.
Gujral JS, McNally PG, O'Malley BP, Burden AC. Ethnic differences in the incidence of lower extremity amputation secondary to diabetes mellitus. Diabet Med. 1993;10(3):271–4. https://doi.org/10.1111/j.1464-5491.1993.tb00057.x.
van Wijngaarden RPT, Overbeek JA, Heintjes EM, Schubert A, Diels J, Straatman H, et al. Relation between different measures of glycemic exposure and microvascular and macrovascular complications in patients with type 2 diabetes mellitus: an observational cohort study. Diabetes Therap. 2017;8(5):1097–109. https://doi.org/10.1007/s13300-017-0301-4.
Sone H, Tanaka S, Tanaka S, Iimuro S, Oida K, Yamasaki Y, et al. Serum level of triglycerides is a potent risk factor comparable to LDL cholesterol for coronary heart disease in Japanese patients with type 2 diabetes: subanalysis of the Japan diabetes complications study (JDCS). J Clin Endocrinol Metab. 2011;96(11):3448–56. https://doi.org/10.1210/jc.2011-0622.
Lin C, Liu J, Sun H. Risk factors for lower extremity amputation in patients with diabetic foot ulcers: a meta-analysis. PLoS One. 2020;15(9):e0239236. https://doi.org/10.1371/journal.pone.0239236.
Stevens RJ, Kothari V, Adler AI, Stratton IM. The UKPDS risk engine: a model for the risk of coronary heart disease in Type II diabetes (UKPDS 56). Clin Sci (London, England : 1979). 2001;101:671–9.
Fujihara K, Igarashi R, Yamamoto M, Ishizawa M, Matsubayasi Y, Matsunaga S, et al. Impact of glucose tolerance status on the development of coronary artery disease among working-age men. Diabetes Metab. 2017;43(3):261–4. https://doi.org/10.1016/j.diabet.2016.09.001.
Iwase M, Fujii H, Nakamura U, Ohkuma T, Ide H, Jodai-Kitamura T, et al. Incidence of diabetic foot ulcer in Japanese patients with type 2 diabetes mellitus: the Fukuoka diabetes registry. Diabetes Res Clin Pract. 2018;137:183–9. https://doi.org/10.1016/j.diabres.2018.01.020.
Li X, Xiao T, Wang Y, Gu H, Liu Z, Jiang Y, et al. Incidence, risk factors for amputation among patients with diabetic foot ulcer in a Chinese tertiary hospital. Diabetes Res Clin Pract. 2011;93(1):26–30. https://doi.org/10.1016/j.diabres.2011.03.014.
Kimura S, Sato T, Ikeda S, Noda M, Nakayama T. Development of a database of health insurance claims: standardization of disease classifications and anonymous record linkage. J Epidemiol. 2010;20(5):413–9. https://doi.org/10.2188/jea.JE20090066.
JMDC: JMDC. Available at: https://www.jmdc.co.jp/en/jmdc-claims-database. Accessed 1 Nov 2020.
Osawa T, Fujihara K, Harada M, Yamamoto M, Ishizawa M, Suzuki H, et al. Higher pulse pressure predicts initiation of dialysis in Japanese patients with diabetes. Diabetes Metab Res Rev. 2019;35(3):e3120. https://doi.org/10.1002/dmrr.3120.
Yamamoto M, Fujihara K, Ishizawa M, Osawa T, Kaneko M, Ishiguro H, et al. Pulse pressure is a stronger predictor than systolic blood pressure for severe eye diseases in diabetes mellitus. J Am Heart Assoc. 2019;8:e010627.
Lin CW, Armstrong DG, Lin CH, Liu PH, Hung SY, Lee SR, et al. Nationwide trends in the epidemiology of diabetic foot complications and lower-extremity amputation over an 8-year period. BMJ Open Diabetes Res Care. 2019;7(1):e000795. https://doi.org/10.1136/bmjdrc-2019-000795.
Adler AI, Erqou S, Lima TA, Robinson AH. Association between glycated haemoglobin and the risk of lower extremity amputation in patients with diabetes mellitus-review and meta-analysis. Diabetologia. 2010;53(5):840–9. https://doi.org/10.1007/s00125-009-1638-7.
Hasan R, Firwana B, Elraiyah T, Domecq JP, Prutsky G, Nabhan M, et al. A systematic review and meta-analysis of glycemic control for the prevention of diabetic foot syndrome. J Vascular Surg. 2016;63:22S–8S e21–22.
Musa IR, Ahmed MON, Sabir EI, Alsheneber IF, Ibrahim EME, Mohamed GB, et al. Factors associated with amputation among patients with diabetic foot ulcers in a Saudi population. BMC research notes. 2018;11(1):260. https://doi.org/10.1186/s13104-018-3372-z.
Robert T, Rury H, Irene S, Carole C, Valeria F, Susan M, David M, Andrew N, Heather M, Eva K, Charles F, David H, David W, et al. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ (Clinical research ed). 1998;317(7160):703–13. https://doi.org/10.1136/bmj.317.7160.703.
American Diabetes Association. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43:S111–s134.
Sowers JR, Epstein M, Frohlich ED. Diabetes, hypertension, and cardiovascular disease: an update. Hypertension (Dallas, Tex : 1979). 2001;37:1053–9.
Yamada-Harada M, Fujihara K, Osawa T, Yamamoto M, Kaneko M, Kitazawa M, et al. Relationship between number of multiple risk factors and coronary artery Disease risk with and without diabetes mellitus. J Clin Endocrinol Metab. 2019;104(11):5084–90. https://doi.org/10.1210/jc.2019-00168.
Tan CE, Glantz SA. Association between smoke-free legislation and hospitalizations for cardiac, cerebrovascular, and respiratory diseases: a meta-analysis. Circulation. 2012;126(18):2177–83. https://doi.org/10.1161/CIRCULATIONAHA.112.121301.
Ockene IS, Miller NH. Cigarette smoking, cardiovascular disease, and stroke: a statement for healthcare professionals from the American Heart Association. American Heart Association Task Force on Risk Reduction. Circulation. 1997;96(9):3243–7. https://doi.org/10.1161/01.cir.96.9.3243.
Chan JC, Malik V, Jia W, Kadowaki T, Yajnik CS, Yoon KH, et al. Diabetes in Asia: epidemiology, risk factors, and pathophysiology. Jama. 2009;301(20):2129–40. https://doi.org/10.1001/jama.2009.726.
Tanaka S, Tanaka S, Iimuro S, Akanuma Y, Ohashi Y, Yamada N, et al. Body mass index and mortality among Japanese patients with type 2 diabetes: pooled analysis of the Japan diabetes complications study and the Japanese elderly diabetes intervention trial. J Clin Endocrinol Metab. 2014;99(12):E2692–6. https://doi.org/10.1210/jc.2014-1855.
Costanzo P, Cleland JG, Pellicori P, Clark AL, Hepburn D, Kilpatrick ES, et al. The obesity paradox in type 2 diabetes mellitus: relationship of body mass index to prognosis: a cohort study. Ann Intern Med. 2015;162(9):610–8. https://doi.org/10.7326/M14-1551.
de Sonnaville JJ, Colly LP, Wijkel D, Heine RJ. The prevalence and determinants of foot ulceration in type II diabetic patients in a primary health care setting. Diabetes Res Clin Pract. 1997;35(2-3):149–56. https://doi.org/10.1016/S0168-8227(97)01380-6.
Hilawe EH, Yatsuya H, Kawaguchi L, Aoyama A. Differences by sex in the prevalence of diabetes mellitus, impaired fasting glycaemia and impaired glucose tolerance in sub-Saharan Africa: a systematic review and meta-analysis. Bull World Health Organization. 2013;91:671–682d.
Ueki K, Sasako T, Okazaki Y, Kato M, Okahata S, Katsuyama H, et al. J-DOIT3 study group. Effect of an intensified multifactorial intervention on cardiovascular outcomes and mortality in type 2 diabetes (J-DOIT3): an open-label, randomised controlled trial. Lancet Diabetes Endocrinol. 2017;5(12):951–64. https://doi.org/10.1016/S2213-8587(17)30327-3.
Goto A, Noda M, Inoue M, Goto M, Charvat H. Increasing number of people with diabetes in Japan: is this trend real? Intern Med. 2016;55(14):1827–30. https://doi.org/10.2169/internalmedicine.55.6475.
Acknowledgements
The authors thank Mami Haga and Natsuko Tada, Niigata University Faculty of Medicine, for their excellent secretarial assistance.
Funding
This work was supported in part by the Japan Society for the Promotion of Science (18 K17897).
Author information
Authors and Affiliations
Contributions
MK, KF and HS conceived and designed the study and supervised the research. KF, NY and HS acquired the data. MK, TO, MY, MH, MK, YM and TY analyzed and interpreted the data. MK and KF prepared the figures and wrote and revised the manuscript. All authors contributed to drafting the article or revising it critically for important intellectual content and approved the final version to be submitted.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee of the Niigata University approved this study (2015–2410).
Consent for publication
Not applicable.
Competing interests
JMDC, Inc. created a nationwide claims-based database for our group. Although members of this organization participated in preparing this manuscript, they did not contribute to the data analysis or the conclusions made. Thus, we feel that this does not represent a potential conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplemental Table 1.
Definitions of amputation using claims.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kaneko, M., Fujihara, K., Harada, M.Y. et al. Rates and risk factors for amputation in people with diabetes in Japan: a historical cohort study using a nationwide claims database. J Foot Ankle Res 14, 29 (2021). https://doi.org/10.1186/s13047-021-00474-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13047-021-00474-8