
Abstract
Background
Considering the heterogenous evidence, a systematic review of the change in anxiety in European children and adolescents associated with the COVID-19 pandemic is lacking. We therefore assessed the change compared with pre-pandemic baselines stratified by gender and age as well as evaluated the impact of country-specific restriction policies.
Methods
A registration on the ‘International Prospective Register of Systematic Reviews’ (PROSPERO) occurred and an a priori protocol was published. We searched six databases (PubMed, Embase, PsycINFO, Cochrane Central Register of Controlled Trials, Web of Science, WHO COVID-19) using a peer-reviewed search string with citation tracking and grey literature screening. Primary outcomes were: (1) general anxiety symptoms; and (2) clinically relevant anxiety rates. We used the Oxford COVID-19 Stringency Index as an indicator of pandemic-related restrictions. Screening of title/abstract and full text as well as assessing risk of bias (using the ‘Risk of Bias in Non-randomized Studies of Exposure’ [ROBINS-E]) and certainty of evidence (using the ‘Grading of Recommendations Assessment, Development and Evaluation’ [GRADE]) was done in duplicate. We pooled data using a random effects model. Reporting is in accordance with the Preferred Reporting Items for Systematic review and Meta-Analysis (PRISMA) statement.
Results
Of 7,422 non-duplicate records, 18 studies with data from 752,532 pre-pandemic and 763,582 pandemic participants met full inclusion criteria. For general anxiety symptoms the total change effect estimate yielded a standardised mean difference (SMD) of 0.34 (95% confidence interval [CI], 0.17–0.51) and for clinically relevant anxiety rates we observed an odds ratio of 1.08 (95%-CI, 0.98–1.19). Increase in general anxiety symptoms was highest in the 11–15 years age group. Effect estimates were higher when pandemic-related restrictions were more stringent (Oxford Stringency Index > 60: SMD, 0.52 [95%-CI, 0.30–0.73]) and when school closures (School Closure Index ≥ 2: SMD, 0.44 [95%-CI, 0.23–0.65]) occurred.
Conclusion
General anxiety symptoms among children and adolescents in Europe increased in a pre/during comparison of the COVID-19 pandemic; particularly for males aged 11–15 years. In periods of stringent pandemic-related restrictions and/or school closures a considerable increase in general anxiety symptoms could be documented.
PROSPERO registration: CRD42022303714.
Similar content being viewed by others


Background
Mental disorders are important causes of disease burden among children and adolescents [1, 2]. Even before the COVID-19 pandemic, the burden of disease study highlighted that anxiety disorders were the most prevalent condition in 2019 among young people in Europe. Among mental health conditions, such disorders represented a leading cause of years lived with disability [2, 3]. In this regard, a link can be drawn between the non-treatment or undertreatment of anxiety disorders in childhood and adolescence and mental illnesses in adulthood, such as anxiety, depression and substance use disorders [4, 5]. Anxiety is generally defined as feelings of concern that appear to have no obvious cause, but are sufficiently persistent and severe to affect daily life [6]. With the onset of the COVID-19 pandemic, the implementation of a broad range of public health and social measures (PHSM) [7] served to exacerbate many determinants of poor mental health. In particular, the environment of children and adolescents has been changed considerably by PHSM, which comprise school and leisure facilities closing, fewer peer interactions, changes in the family system as a result of the requirement to work from home, and quarantine orders [7,8,9]. As already known from previous studies [10,11,12,13], such changes can lead to serious impairments in young people’s mental health. To date, the impact of the COVID-19 pandemic on anxiety has been assessed primarily for the adult population [14,15,16] or its global prevalence for children and adolescents [17,18,19]. Existing European studies with a pre-pandemic baseline showed heterogeneous results [20,21,22,23]. However, a deeper understanding of changes in anxiety symptoms in the young population group is lacking, especially for the European continent.
An up-to-date examination of changes in anxiety symptoms among children and adolescents is therefore imperative and of great public health (PH) relevance in order to counteract suboptimal developments [2]. An analysis of the changes in the European continent means that the lack of an evidence base in the subgroup-stratified summary among children and adolescents can be rectified. It also allows for the use of a quasi-experimental design by analysing the impact of heterogeneous pandemic-related interventions in the European countries. Hence, the aim of this systematic review and meta-analysis is to identify, critically assess, summarise, and determine the certainty of evidence (CoE) regarding the impact of the COVID-19 pandemic on anxiety among children and adolescents in Europe compared with the pre-pandemic baseline. Thereby, it aims to provide information about the relevance of pandemic-related restrictions which will contribute to the analysis and the lessons learned from the immediate restrictions taken to safeguard the population in various European countries.
Methods
This systematic review and meta-analysis is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) [24] statement (Additional file 1: Table S1). Our protocol is registered on the ‘International Prospective Register of Systematic Reviews’ (PROSPERO; CRD42022303714) [25] and was published a priori [26]; any deviations from the original review protocol are presented in Additional file 1: Table S2.
Data sources, search strategy and eligibility criteria
We searched for published articles in six electronic databases (PubMed, Embase, PsycINFO, Cochrane Central Register of Controlled Trials, Web of Science, WHO COVID-19 database [including pre-prints]), up to 18 March, 2022. Additionally, we enlarged our searches by examining previous systematic reviews and meta-analysis on the same topic, checking reference lists in included studies and searching relevant grey literature sources such as reports issued by key organisations and abstracts of relevant conferences up to 16 April, 2022; more information on the screened key organisations and conferences is provided in Additional file 1: Table S3.
We developed the search strategy according to the Population–Exposure–Comparison–Outcome (PECO) [27] scheme and included the following key search terms: children and adolescents (population), COVID-19 (exposure) and anxiety (outcome). The availability of a pre-pandemic baseline (comparison) was assessed manually. The six tailored search strategies can be found in Additional file 1: Table S4. The search strategy was reviewed by a search specialist using the evidence-based checklist ‘Peer Review of Electronic Search Strategies’ (PRESS) [28].
Our pre-defined eligibility criteria were equally defined according to the PECO [27] scheme:
-
Population: Children and adolescents ≤ 19 years, living in the WHO European region [29].
-
Exposure: Participation in survey during the COVID-19 pandemic.
-
Comparison: Pre-pandemic baseline.
-
Primary outcomes: Measurements of general anxiety symptoms or clinically relevant anxiety rates; no secondary outcomes were considered.
We excluded studies undertaken in children and adolescents with pre-existing psychiatric diagnoses. No limits regarding language and effect measurement were applied, however our search strategy was designed and run in English. Publications drawing upon the same study population and measurement time points were included as one item. When measurement time points varied during the COVID-19 pandemic, each measurement time point was considered individually.
Selection process and data extraction
After deduplication, two reviewers (HLW, ID) used the recommended EPPI reviewer software [30] to independently screen first titles and abstracts, and second full texts, in accordance with the above eligibility criteria. Disagreements or uncertainty about eligibility were resolved through discussion. Reasons for exclusion after full text screening were recorded and are reported in a separate table (Additional file 1: Table S5).
Further, two reviewers (HLW, ID) used piloted extraction forms to independently extract data from one third of the published studies and unpublished data requested from study authors. Remaining data extraction was completed by one reviewer (HLW) and verified by the other (ID). Differences in data extraction were discussed and resolved between the two reviewers. Our data extraction forms, in accordance with a former systematic review [31], included the following items: study information (first author, year of publication, country, study type), population and setting (sample size, % female, age of CA), COVID-19 determinants (time point of data measurement), pre-pandemic baseline (time point of data measurement, link between pre-pandemic population and the population during the pandemic) and outcomes (type of outcome, diagnostic instrument, psychometric properties of the diagnostic instrument, symptom reporter). We defined general anxiety symptoms and clinically relevant anxiety rates as primary outcomes. General self-reported measurements of anxiety were summarised as general anxiety symptoms. Since the measurement instruments and scales used varied considerably, the measurement data was standardised to standardised mean difference (SMD) with a 95% confidence interval (CI); this standardisation is also recommended by the Cochrane Handbook [32]. Measurements with a clinical cut-off or with a clinical diagnostic (International Statistical Classification of Diseases and Related Health Problems [ICD]) were summarised as clinically relevant anxiety rates and reported as odds ratio (OR) with a 95% CI. To describe PHSM restrictions in the measurement time frame of the studies and make them comparable, we used the Oxford COVID-19 Stringency Index [8] and the School Closure Index [8] as indicators. The Oxford COVID-19 Stringency Index consists of nine metrics including school closures, workplace closures and stay-at-home requirements. The index ranges from 0 (no restrictions) to 100 (most stringent restrictions) and was validated [8]. In accordance with the COVIDSurg Collaborative [33], we defined three categories: light restrictions (index < 20), moderate lockdowns (index 20–60) and full lockdowns (index > 60). The School Closure Index represents the handling of school closures and is an incorporated measurement in the Oxford COVID-19 Stringency Index, which was considered separately in our analyses. The index ranges from 0 to 3: 0 describes no restrictions; 1 contains recommended closure or all schools open with alterations resulting in significant differences compared with non-COVID-19 operations; 2 involves closure (only some levels or categories, e.g. just high school, or just public schools); and 3 requires closures at all levels [8]. We defined the cut-offs as ‘no or few alterations compared with a pre-COVID-19 situation’ (index < 2) and ‘partial or full school closure’ (index ≥ 2) [31]. We contacted nearly all study authors and asked to provide further unpublished data on age or gender-stratified data.
Risk of Bias assessment
Three reviewers (HLW, LMP, ID) independently assessed the risk of bias (RoB) in teams of two using the ‘Risk of Bias in Non-randomized Studies of Exposure’ (ROBINS-E) instrument [34]. For each study, the seven bias domains and a whole RoB assessment was revealed as either low, some concerns, high RoB, or very high RoB [34].
Data synthesis and statistical analyses
For the meta-analysis, we pooled effect estimates for general anxiety symptoms and clinically relevant anxiety rates in total and analysed different subgroups: gender (female/male), age (11–15, 16–19 years), Oxford Stringency Index (> 60/ ≤ 60) [8] and School Closure Index (≥ 2/ < 2) [8]. We used, where possible, results from adjusted analysis for pooling. If necessary, dichotomous data were transferred to SMD, using the formula recommended by Chinn [35]. Where multiple pre-pandemic measurements were available, the last measurement was used for calculation purposes. We excluded measurements, with combined anxiety/depression scores, from the meta-analysis. Where parent and self-reported data were presented [36], we gave preference to the self-reported data. Furthermore, within the meta-analysis, we grouped the studies according to their RoB rating; low/some concerns (= low) RoB studies and high RoB/very high RoB (= high) RoB studies were summarised both separately and in total. In particular, the pooled effect of the low RoB studies was taken for further interpretation. We used Review Manager 5.4.1 [37] and R Studio 4.2.1 [38] for data entry, statistical analysis, and graph creation. In all meta-analyses, random-effect models and the inverse-variance method with the ‘DerSimonian and Laird’ approach were used.
We investigated heterogeneity by using visual inspection of the forest plots as well as the Chi2 test and I2 index [39]. If I2 > 50%, substantial heterogeneity was presumed. We conducted sensitivity analyses and meta-regression (if ≥ 10 studies per examined variable) to explain substantial heterogeneity [40]. Publication bias was analysed by visually interpreting funnel plots for signs of asymmetry [41] and statistically by calculating the Egger’s test (if ≥ 10 studies) [42].
Certainty of evidence
We assessed the overall CoE for each outcome using the ‘Grading of Recommendations Assessment, Development and Evaluation’ (GRADE) system and presented it along with the main findings of the review in a ‘Summary of findings’ table, based on a transparent format with defined applied criteria (Additional file 1: Table S6) and a generated evidence profile (Additional file 1: Table S7) [43]. The GRADE tool covers five categories for downgrading (RoB, imprecision, inconsistency, indirectness, publication bias) and three categories for upgrading (magnitude of effects, dose–response relationships, impact of residual confounding). The CoE could be rated as high, moderate, low or very low.
Results
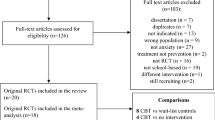
Our electronic search identified 7,420 non-duplicate records from database searches and additional two grey literature publications. Of these, 51 studies entered full-text screening. After a comprehensive screening process, detailed in the PRISMA flow diagram (Additional file 1: Figure S1), we included 18 studies with 22 effect measures, comprising 16 peer-reviewed studies [20, 22, 23, 36, 44,45,46,47,48,49,50,51,52,53,54,55], one report [56], and one pre-print [21]. Reasons for exclusion after full-text screening are described in Additional file 1: Table S5.
Study characteristics
The characteristics of each of the studies that were included are described in Table 1. The total population sample included data from 752,532 pre-pandemic and 763,582 pandemic participants (broken down into general anxiety symptoms: 11,425 pre-pandemic and 13,387 pandemic participants; clinically relevant anxiety rates: 741,107 pre-pandemic and 750,195 pandemic participants). Studies were carried out in a range of countries: four in Germany [21, 44, 45, 56], four in the United Kingdom [22, 23, 36, 55], three in Italy [47,48,49], two in Spain [51, 52], two in Switzerland [53, 54], and one in Israel [46], one in the Netherlands [20], and one in Norway [50], respectively. Most of the studies measured general anxiety symptoms in spring/summer 2020 (14 effect measures) [20,21,22,23, 36, 45,46,47, 49,50,51, 53,54,55], while two effect measurements were conducted in autumn 2020 [21, 22] and three in winter 2020/spring 2021 [21, 51, 52]. Clinically relevant anxiety rates were analysed in four studies [44, 45, 48, 56]. Of the included studies, 17 [20,21,22,23, 36, 44,45,46,47,48,49,50, 52,53,54,55,56] reported data for children and adolescents over the age of 11 and 11 studies [20, 36, 44, 45, 47,48,49, 51, 54,55,56] for children and adolescents under the age of 11. The measurement time point was rated as ‘full lockdown’ (Oxford Stringency Index > 60) in 14 studies [20, 22, 23, 36, 44, 46,47,48,49,50,51,52,53,54] and partial or full school closure occured in 11 studies (School Closure Index ≥ 2) [20,21,22,23, 36, 46,47,48,49, 51, 55]. In addition, 12 studies [20,21,22,23, 36, 44, 45, 47, 49, 53, 55, 56] provided further study data (generally unpublished gender-stratified and age-stratified data). The effect estimates of the 18 studies that were included are summarised in Additional file 1: Table S8. The RoB assessment revealed a ‘some concerns’ rating for six studies [20, 21, 44, 46, 53, 56], a ‘high RoB’ rating for eight studies [22, 23, 36, 45, 47, 50, 51, 55] and a ‘very high RoB’ rating for four studies [48, 49, 52, 54]. Detailed rating information is provided in Additional file 1: Figure S2 (traffic-light plot) and Additional file 1: Figure S3 (weighted-bar plot).
Meta-analysis of general anxiety symptoms
For general anxiety symptoms, 12 studies [20,21,22,23, 36, 45, 46, 48, 49, 52, 53, 55] were pooled and CoE was graded as ‘very low’ (Table 2; further information in Additional file 1: Table S7). In a pooling of four low RoB studies with six measures, a total change of a SMD of 0.34 (95% CI, 0.17 to 0.51, I2 = 96%; Fig. 1) was calculated. Following gender stratification, a SMD of 0.30 (95% CI, 0.12 to 0.49, I2 = 90%; Additional file 1: Figure S4) for females and 0.34 (95% CI, 0.07 to 0.60, I2 = 95%; Additional file 1: Figure S5) for males in low RoB studies was revealed. Age-stratified pooling was possible for the 11–15 years age category with three studies [20, 21, 53] and five effect measures, and for the 16–19 years age category with two studies [20, 21] and four effect measures. For the 11–15 years age category, the total change effect estimate yielded a SMD of 0.39 (95% CI, 0.18 to 0.60, I2 = 93%; Additional file 1: Figure S6). Change effect estimates were also evident for females (SMD, 0.34; 95% CI, 0.19 to 0.49; I2 = 71%; Additional file 1: Figure S7) and males (SMD, 0.45; 95% CI, 0.15 to 0.74; I2 = 93%; Additional file 1: Figure S8). Pooling within the 16–19 years age category revealed a SMD of 0.24 (95% CI, -0.01 to 0.49, I2 = 92%; Additional file 1: Figure S9) in total, a SMD of 0.18 (95% CI, -0.01 to 0.37; I2 = 75%; Additional file 1: Figure S10) for females and a SMD of 0.31 (95% CI, -0.02 to 0.63; I2 = 92%; Additional file 1: Figure S11) for males.

Forest plot of changes in youth general anxiety symptoms comparing before and during COVID-19 pandemic. SE, standard error; SMD, standardized mean differences; RoB, risk of bias; 95%-CI, 95%-confidence interval
To estimate the extent to which the stringency of PHSM has an impact on anxiety symptoms, low RoB studies were pooled by the Oxford COVID-19 Stringency Index (> 60 vs ≤ 60) and the School Closure Index (≥ 2 and < 2). An increase in general anxiety symptoms was observed for the Oxford COVID-19 Stringency Index > 60 (SMD, 0.52; 95% CI, 0.30 to 0.73; I2 = 96%; Fig. 2) and the School Closure Index ≥ 2 (SMD, 0.44; 95% CI, 0.23 to 0.65; I2 = 96%; Fig. 3).

Forest plot of changes in youth general anxiety symptoms comparing Oxford Stringency Index. SE, standard error; SMD, standardized mean differences; SI, stringency index; 95%-CI, 95%-confidence interval

Forest plot of changes in youth general anxiety symptoms comparing School Closure Index. SE, standard error; SMD, standardized mean differences; SL, School Closure Index; 95%-CI, 95%-confidence interval
Meta-analysis of clinically relevant anxiety rates
For clinically relevant anxiety rates, four studies [44, 45, 48, 56] were pooled and CoE was graded as ‘very low’ (Table 2; further information in Additional file 1: Table S7). Total change yielded an OR of 1.08 (95% CI, 0.98 to 1.19, I2 = 82%; Fig. 4) in two low RoB studies [44, 56]. Clinically relevant anxiety rates increased significantly in females in low RoB studies (OR, 1.10 [95% CI, 1.02 to 1.19], I2 = 52%; Additional file 1: Figure S12), but not for males (OR, 1.04 [95% CI, 0.92 to 1.17], I2 = 76%; Additional file 1: Figure S13).

Forest plot of changes in youth clinically relevant anxiety symptoms comparing before and during COVID-19 pandemic. OR, Odds Ratio; RoB, risk of bias; 95%-CI, 95%-confidence interval
Heterogeneity, publication bias and sensitivity analysis
As heterogeneity was substantial in all meta-analyses (I2 > 50%), meta-regression analyses were conducted for the total population, female and male children and adolescents. In every meta-regression analysis, ‘RoB’ and ‘study design’ represent positive covariates (Additional file 1: Tables S9-14). The covariate ‘RoB’ was addressed by the aforementioned stratification of low vs high RoB studies. Effect direction and significance did not change after removing the study with cross-sectional design. Sensitivity analyses (Additional file 1: Table S15) revealed significant differences for study design and effect conversion. However, only one cross-sectional study and one study with converted measurements were included in the analyses. Effect direction and significance did not alter after removing these studies from meta-analyses. Visual analysis of the (contour-enhanced) funnel plots implied asymmetry (Additional file 1: Figures S14–S19), but was discarded by applying Egger’s test (Additional file 1: Table S16).
Discussion
This systematic review and meta-analysis provides insights into the changes in general anxiety symptoms and clinically relevant anxiety rates in European children and adolescents after the onset of the COVID-19 pandemic when compared with the pre-pandemic baseline. We included 18 studies that assessed changes in over 750,000 children and adolescents (for several measurement points) across Europe. The pooled effect estimates of low RoB studies revealed an increase in general anxiety symptoms overall, and particularly for males in the 11–15 years age category. A significant increase in clinically relevant anxiety rates was also observed among female children and adolescents.
Considering the various different restriction policies in European countries, this systematic review and meta-analysis is the first that assessed the association between PHSM and higher general anxiety symptoms. For children above six years of age, school closures have been a major disruptor as these measures radically changed their life [9]. Instead of having social contact five days a week, often for six or eight hours a day with their class, peers and friends, they were homebound and unable to socialise properly. These full or partial school closures affected approximately 105 million pupils and students in Europe [57]. Our meta-analyses revealed particularly high general anxiety symptoms during periods of school closure (SMD, 0.44; 95% CI, 0.23 to 0.65) and other restriction measures (SMD, 0.52; 95% CI, 0.30 to 0.73); these effect increases outlined a potential impact of school closures and PHSM on anxiety symptoms. However, the evidence rating of "very low" have to be considered here; therefore, further reseach is needed. Both effect estimates were higher than in a previous meta-analysis on depression [31]. As social anxiety can be reduced through exposure to social interactions, the non-exposure to social contacts and social challenges in the school environment as a result of PHSM may explain the stronger correlation with the symptomatology. Further research will allow a comparison of the reduction in anxiety symptoms between subgroups and countries following the acute pandemic phase. Our results suggest that the higher association with restrictive measures could lead to a more rapid reduction in symptoms once life returns to normal. Nevertheless, social exclusion of children and adolescents during the pandemic could lead to life-long mental and physical health consequences [3, 58, 59]. However, a clearcut separation of the effects on anxiety due to school closure from those due to other pandemic related restrictions—like worries about (elderly) relatives, fear of long-lasting health effects (long COVID), and also closure of recreational and sports facilities—was not possible. This limitation was already found in a previous review [19]. Therefore, our results must be interpreted indicative regarding the possible drivers for the increased anxiety.
Regarding different subgroups, our analyses first showed strong differences between studies with low and high RoB. While the increase in general anxiety symptoms is clearly evident for studies with a low RoB, the pooling effects of high RoB studies were indistinct and non-significant. The heterogeneous evidence in literature can partly be attributed to the different quality of existing studies; this underlines the importance of strictly assessing the RoB. Second, age-specific analyses found considerably higher effect estimates for children and adolescents aged 11–15 years, in particular among males, but lower and more imprecise estimates for those aged 16–19 years. Taking into account the fact that the risk of anxiety disorders among children aged 10–14 years had already been reported as being high three decades before the COVID-19 pandemic [2], our findings showed that this age group was also more vulnerable to increases during the COVID-19 pandemic. The imprecise results for general anxiety symptoms among males in the 16–19 year age category are in contrast to findings on depression [31]. This underlines the necessity to differentiate between different mental health diagnoses in specific age groups in the COVID-19 pandemic. Third, for clinically relevant anxiety rates, the pooled associations were based on two low RoB studies from Germany and should be interpreted with caution; further empirical evidence is needed here.
This paper has strong implications for both policy and clinical practice. Policy-makers should consider the unintended consequences before imposing PHSM such as school closures on the mental health of children and adolescents. Psychiatrists, psychotherapists and other public health experts for children and adolescents should therefore be included in pandemic crisis task forces [60, 61]. The increase in general anxiety symptoms and the variation between specific groups and countries requires children and adolescents to be closely monitored over the next few years. This monitoring should cover a broad range of age groups, similar to the recommendation of the U.S. Preventive Services Task Force to screen all children and adolescents aged 8–18, regardless of whether they have symptoms [62]. Based on our study, children and adolescents born in 2005 to 2010 (aged 11–15 years in 2020 to 2021) should be monitored henceforth. While our study indicates a strong need for anxiety disorder therapies (like previous research for depression symptoms [31]), these professionals were understaffed even before the pandemic [6]. Policy makers should therefore strengthen availability and capacity of these professional groups.
Screening and adequate diagnoses are important for identifying children and adolescents with anxiety disorders and the need for therapy. The gap between studies measuring general anxiety symptoms and those measuring clinically relevant anxiety rates in our systematic review might indicate a lack of clinical evidence and diagnoses. Parents, teachers, health care professionals and sports trainers should be made aware of risk factors and symptoms of anxiety disorders as well as mental health services. The negative consequences in later life of a failure to address anxiety symptoms on children and adolescents are well documented [3, 58, 59]. Moreover, even before the COVID-19 pandemic, anxiety and depression disorders were two of the top five causes of overall disease burden for children and adolescents in Europe, and suicide was a leading cause of death among 10–19-year-olds in the WHO European region [3]. It is therefore important to implement evidence-based interventions that can help address mental health issues in children. Targeted interventions and longer programmes in particular seemed to be more effective [3]. In addition, protective factors should be communicated and supported; including parent–child dialogue [63], a predictable home environment [64], peer-to-peer social contact [65] and physical activity [66]. Further, increased resilience among child and adolescents could be a predictor of fewer anxiety symptoms [67, 68].
There are several research gaps regarding anxiety symptoms in the COVID-19 pandemic in Europe, including evidence for children aged below 10 years, differentiation by social status or education, and clinically relevant anxiety rates. Generally, there are only a very small number of studies on anxiety with a pre-pandemic baseline in Europe, although no such studies were able to be included for Eastern European countries and hardly any evidence from southern Europe. To improve this, representative longitudinal cohort or panel studies on CA should be conducted in all European countries so as to have a pre-crisis baseline and to monitor changes over time. Such a cohort or panel should include validated anxiety measures for general symptoms and for a clinically relevant cut-off, as well as demographic, socioeconomic and health-related confounders. These criteria are necessary in order to reduce the RoB and to allow subgroup-specific analyses.
Strength and limitations
There are several limitations to this review. First, RoB was high for 12 studies (66% of the studies included), mainly based on bias due to participant selection, missing data and insufficient adjustment of important confounders. This limitation was addressed by downgrading for RoB in GRADE and we stratified our meta-analyses by RoB. Second, the instruments that were used differed greatly in their scales. To unify them, we transformed the effect estimates to SMD or OR. Third, there was a high level of heterogeneity in the meta-analyses (I2 > 50%), which we tried to explain by conducting meta-regression analyses. Fourth, no country pooling and visualisation over time were possible due to the low study quality. There were only a small number of available studies within our strict inclusion criteria with age-group-specific data. Fifth, there is a lack of longitudinal studies. Sixth, more subgroup analyses were not feasible. Seventh, the Oxford Stringency Index [8] and the School Closure Index [8] were used as proxies for PHSM and cannot cover all facets of the COVID-19 pandemic.
The strengths of this review are that it largely follows the methodological guidelines recommended by the Cochrane Handbook for systematic reviews [32], such as systematic search in several databases with a peer-reviewed search strategy and consideration of pre-prints, grey literature, and conference abstracts. In addition, literature screening, data extraction and RoB rating were performed independently and unpublished data was requested from study authors. In addition, the assessment of the RoB and the CoE was conducted using recommended tools. Thus, an assessment of evidence based on high quality studies was possible, allowing contradictory findings from previous studies to be properly interpreted.
Conclusion
This systematic review and meta-analysis showed an increase in general anxiety symptoms among European children and adolescents during the first two years of the COVID-19 pandemics compared with a pre-pandemic baseline. The 11–15 years male age group was particularly affected. Social distancing policies implemented in European countries, and in particular school closures, might be associated with a considerable increase in the effect of general anxiety symptoms. Therefore, school closures should be implemented only with the greatest caution and with consideration of the evidence available regarding the mental health of children and adolescents. At present, the need is huge to monitor anxiety symptoms in children and adolescents on a long-term basis and to identify which of the 105 million children and adolescents in Europe have disorders that require professional management and treatment. Due to long-term consequences of anxiety disorders and the risk of suicidality, those affected have to be clinically addressed through early identification and therapy.
Availability of data and materials
All data are included in the manuscript and appendix.
References
Reiner RC, Olsen HE, Ikeda CT, et al. Diseases, Injuries, and Risk Factors in Child and Adolescent Health, 1990 to 2017: findings From the Global Burden of Diseases, Injuries, and Risk Factors 2017 Study. JAMA Pediatr. 2019;173:e190337. https://doi.org/10.1001/jamapediatrics.2019.0337.
Castelpietra G, Knudsen AKS, Agardh EE, et al. The burden of mental disorders, substance use disorders and self-harm among young people in Europe, 1990–2019: Findings from the Global Burden of Disease Study 2019. Lancet Reg Health Eur. 2022;16:100341. https://doi.org/10.1016/j.lanepe.2022.100341.
Bruckmayer M, Phillips W. Children and mental health: Preventive approaches to anxiety and depression : European platform for investing in children. Luxembourg: Publications Office of the European Union; 2021.
Copeland WE, Angold A, Shanahan L, et al. Longitudinal patterns of anxiety from childhood to adulthood: the Great Smoky Mountains Study. J Am Acad Child Adolesc Psychiatry. 2014;53:21–33. https://doi.org/10.1016/j.jaac.2013.09.017.
Monk NJ, McLeod GFH, Mulder RT, et al. Childhood anxious/withdrawn behaviour and later anxiety disorder: a network outcome analysis of a population cohort. Psychol Med. 2021;1:1–12. https://doi.org/10.1017/S0033291721002889.
Liu J, Chen X, Lewis G. Childhood internalizing behaviour: analysis and implications. J Psychiatr Ment Health Nurs. 2011;18:884–94. https://doi.org/10.1111/j.1365-2850.2011.01743.x.
Rehfuess EA, Movsisyan A, Pfadenhauer LM, et al. Public health and social measures during health emergencies such as the COVID-19 pandemic: an initial framework to conceptualize and classify measures. Influenza Other Respir Viruses. 2023;17:e13110. https://doi.org/10.1111/irv.13110.
Hale T, Angrist N, Goldszmidt R, et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat Hum Behav. 2021;5:529–38. https://doi.org/10.1038/s41562-021-01079-8.
Fegert JM, Vitiello B, Plener PL, et al. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: a narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc Psychiatry Ment Health. 2020;14:20. https://doi.org/10.1186/s13034-020-00329-3.
Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. The Lancet. 2020;395:912–20. https://doi.org/10.1016/S0140-6736(20)30460-8.
Almeida ILdL, Rego JF, Teixeira ACG, et al. Social isolation and its impact on child and adolescent development: a systematic review. Rev Paul Pediatr. 2021;40:e2020385. https://doi.org/10.1590/1984-0462/2022/40/2020385.
Lacey RE, Kumari M, Bartley M. Social isolation in childhood and adult inflammation: evidence from the National Child Development Study. Psychoneuroendocrinology. 2014;50:85–94. https://doi.org/10.1016/j.psyneuen.2014.08.007.
Kratzer S, Pfadenhauer LM, Biallas RL, et al. Unintended consequences of measures implemented in the school setting to contain the COVID-19 pandemic: a scoping review. Cochrane Database Syst Rev. 2022;6:CD15397. https://doi.org/10.1002/14651858.CD015397.
Santomauro DF, Mantilla Herrera AM, Shadid J, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. The Lancet. 2021;398:1700–12. https://doi.org/10.1016/S0140-6736(21)02143-7.
Hajek A, Neumann-Böhme S, Sabat I, et al. Depression and anxiety in later COVID-19 waves across Europe: New evidence from the European COvid Survey (ECOS). Psychiatry Res. 2022;317:114902. https://doi.org/10.1016/j.psychres.2022.114902.
Thompson EJ, Stafford J, Moltrecht B, et al. Psychological distress, depression, anxiety, and life satisfaction following COVID-19 infection: evidence from 11 UK longitudinal population studies. The Lancet Psychiatry. 2022;9:894–906. https://doi.org/10.1016/S2215-0366(22)00307-8.
Racine N, McArthur BA, Cooke JE, et al. Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents During COVID-19: A Meta-analysis. JAMA Pediatr. 2021;175:1142–50. https://doi.org/10.1001/jamapediatrics.2021.2482.
Viner RM, Mytton OT, Bonell C, et al. Susceptibility to SARS-CoV-2 infection among children and adolescents compared with adults: a systematic review and meta-analysis. JAMA Pediatr. 2021;175:143–56. https://doi.org/10.1001/jamapediatrics.2020.4573.
Viner R, Russell S, Saulle R, et al. School closures during social lockdown and mental health, health behaviors, and well-being among children and adolescents during the first COVID-19 wave: a systematic review. JAMA Pediatr. 2022;176:400–9. https://doi.org/10.1001/jamapediatrics.2021.5840.
Luijten MAJ, van Muilekom MM, Teela L, et al. The impact of lockdown during the COVID-19 pandemic on mental and social health of children and adolescents. Qual Life Res. 2021;30:2795–804. https://doi.org/10.1007/s11136-021-02861-x.
Ravens-Sieberer U, Erhart M, Devine J, et al. Child and adolescent mental health during the COVID-19 pandemic: results of the three-wave longitudinal COPSY study. SSRN J. 2022. https://doi.org/10.2139/ssrn.4024489.
Widnall E, Winstone L, Plackett R, et al. Impact of school and peer connectedness on adolescent mental health and well-being outcomes during the COVID-19 pandemic: a longitudinal panel survey. Int J Environ Res Public Health. 2022. https://doi.org/10.3390/ijerph19116768.
Knowles G, Gayer-Anderson C, Turner A, et al. Covid-19, social restrictions, and mental distress among young people: a UK longitudinal, population-based study. J Child Psychol Psychiatry. 2022. https://doi.org/10.1111/jcpp.13586.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:71. https://doi.org/10.1136/bmj.n71.
Ludwig-Walz H, Fegert JM, Bujard M Depression and anxiety among children and adolescents during the COVID-19 pandemic in Europe: A systematic review: PROSPERO 2022. CRD42022303714
Ludwig-Walz H, Dannheim I, Pfadenhauer LM, et al. Anxiety among children and adolescents during the COVID-19 pandemic in Europe: a systematic review protocol. Syst Rev. 2023. https://doi.org/10.1186/s13643-023-02225-1.
Morgan RL, Whaley P, Thayer KA, et al. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ Int. 2018;121:1027–31. https://doi.org/10.1016/j.envint.2018.07.015.
McGowan J, Sampson M, Salzwedel DM, et al. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol. 2016;75:40–6. https://doi.org/10.1016/j.jclinepi.2016.01.021.
WHO Regional Office for Europe (2022) Countries. https://www.euro.who.int/en/countries. Accessed 18 May 2022
Thomas J, Graziosi S, Brunton J et al. (2020) EPPI-Reviewer: advanced software for systematic reviews, maps and evidence synthesis.: EPPI-Centre Software., London: UCL Social Research Institute
Ludwig-Walz H, Dannheim I, Pfadenhauer LM, et al. Increase of depression among children and adolescents after the onset of the COVID-19 pandemic in Europe: a systematic review and meta-analysis. Child Adolesc Psychiatry Ment Health. 2022;16:109. https://doi.org/10.1186/s13034-022-00546-y.
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (ed) (2022) Cochrane Handbook for Systematic Reviews of Interventions: version 6.3. updated February 2022
COVIDSurg Collaborative,. Effect of COVID-19 pandemic lockdowns on planned cancer surgery for 15 tumour types in 61 countries: an international, prospective, cohort study. Lancet Oncol. 2021;22:1507–17. https://doi.org/10.1016/S1470-2045(21)00493-9.
Higgins J, Morgan R, Rooney A, Taylor K, Thayer K, Silva R, Lemeris C, Akl A, Arroyave W, Bateson T, Berkman N, Demers P, Forastiere F, Glenn B, Hróbjartsson A, Kirrane E, LaKind J, Luben T, Lunn R, McAleenan A, McGuinness L, Meerpohl J, Mehta S, Nachman R, Obbagy J, O'Connor A, Radke E, Savović J, Schubauer-Berigan M, Schwingl P, Schunemann H, Shea B, Steenland K, Stewart T, Straif K, Tilling K, Verbeek V, Vermeulen R, Viswanathan M, Zahm S, Sterne J (2022) Risk Of Bias In Non-randomized Studies - of Exposure (ROBINS-E): Launch version. https://www.riskofbias.info/welcome/robins-e-tool
Chinn S. A simple method for converting an odds ratio to effect size for use in meta-analysis. Statist Med. 2000;19:3127–31. https://doi.org/10.1002/1097-0258(20001130)19:22%3C3127:AID-SIM784%3E3.0.CO;2-M.
Wright N, Hill J, Sharp H, et al. Interplay between long-term vulnerability and new risk: Young adolescent and maternal mental health immediately before and during the COVID-19 pandemic. JCPP Adv. 2021;1:e12008. https://doi.org/10.1111/jcv2.12008.
The Cochrane Collaboration (2020) Review Manager (RevMan) [Computer program]
RStudio: Integrated Development Environment for R (2022). RStudio Team, Boston
Higgins JPT, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60. https://doi.org/10.1136/bmj.327.7414.557.
Deeks JJ, Higgins JP, Altman DG (2022) Chapter 10: Analysing data and undertaking meta-analyses. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (ed) Cochrane Handbook for Systematic Reviews of Interventions: version 6.3. updated February 2022
Sterne JAC, Sutton AJ, Ioannidis JPA, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011;343:d4002. https://doi.org/10.1136/bmj.d4002.
Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–34. https://doi.org/10.1136/bmj.315.7109.629.
Schünemann HJ, Cuello C, Akl EA, et al. GRADE guidelines: 18. How ROBINS-I and other tools to assess risk of bias in nonrandomized studies should be used to rate the certainty of a body of evidence. J Clin Epidemiol. 2019;111:105–14. https://doi.org/10.1016/j.jclinepi.2018.01.012.
Kostev K, Weber K, Riedel-Heller S, et al. Increase in depression and anxiety disorder diagnoses during the COVID-19 pandemic in children and adolescents followed in pediatric practices in Germany. Eur Child Adolesc Psychiatry. 2021. https://doi.org/10.1007/s00787-021-01924-1.
Rau L-M, Grothus S, Sommer A, et al. Chronic pain in schoolchildren and its association with psychological wellbeing before and during the COVID-19 pandemic. J Adolesc Health. 2021;69:721–8. https://doi.org/10.1016/j.jadohealth.2021.07.027.
Shoshani A, Kor A. The mental health effects of the COVID-19 pandemic on children and adolescents: risk and protective factors. Psychol Trauma. 2021. https://doi.org/10.1037/tra0001188.
Frigerio A, Nettuno F, Nazzari S. Maternal mood moderates the trajectory of emotional and behavioural problems from pre- to during the COVID-19 lockdown in preschool children. Eur Child Adolesc Psychiatry. 2022. https://doi.org/10.1007/s00787-021-01925-0.
Davico C, Marcotulli D, Lux C, et al. Impact of the COVID-19 pandemic on child and adolescent psychiatric emergencies. J Clin Psychiatry. 2021. https://doi.org/10.4088/JCP.20m13467.
Crescentini C, Feruglio S, Matiz A, et al. Stuck Outside and Inside: An Exploratory Study on the Effects of the COVID-19 Outbreak on Italian Parents and Children’s Internalizing Symptoms. Front Psychol. 2020;11:586074. https://doi.org/10.3389/fpsyg.2020.586074.
Hafstad GS, Sætren SS, Wentzel-Larsen T et al. (2021) Adolescents' symptoms of anxiety and depression before and during the Covid-19 outbreak - A prospective population-based study of teenagers in Norway. Lancet Reg Health Eur 5:100093. https://doi.org/10.1016/j.lanepe.2021.100093
Giménez-Dasí M, Quintanilla L, Fernández-Sánchez M. Longitudinal Effects of the Pandemic and Confinement on the Anxiety Levels of a Sample of Spanish Children in Primary Education. Int J Environ Res Public Health. 2021. https://doi.org/10.3390/ijerph182413063.
Carrillo-Diaz M, Ortega-Martínez AR, Romero-Maroto M, et al. Lockdown impact on lifestyle and its association with oral parafunctional habits and bruxism in a Spanish adolescent population. Int J Paediatr Dent. 2022;32:185–93. https://doi.org/10.1111/ipd.12843.
Ertanir B, Kassis W, Garrote A. Longitudinal Changes in Swiss Adolescent’s Mental Health Outcomes from before and during the COVID-19 Pandemic. Int J Environ Res Public Health. 2021. https://doi.org/10.3390/ijerph182312734.
Borbás R, Fehlbaum LV, Dimanova P, et al. Mental well-being during the first months of Covid-19 in adults and children: behavioral evidence and neural precursors. Sci Rep. 2021;11:17595. https://doi.org/10.1038/s41598-021-96852-0.
Bignardi G, Dalmaijer ES, Anwyl-Irvine AL, et al. Longitudinal increases in childhood depression symptoms during the COVID-19 lockdown. Arch Dis Child. 2020. https://doi.org/10.1136/archdischild-2020-320372.
Witte J, Zeitler A, Hasemann L (2022) Krankenhausversorgung von Kindern und Jugendlichen während der Pandemie: Fokus: Psychische Erkrankungen. Ergebnisse des DAK Kinder und Jugendreports 2022 / Datenbasis: 2019 bis 2021, Bielefeld
United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects 2022, Online Edition; 2022
Lahey BB. Why are children who exhibit psychopathology at high risk for psychopathology and dysfunction in adulthood? JAMA Psychiat. 2015;72:865–6. https://doi.org/10.1001/jamapsychiatry.2015.0798.
Viswanathan M, Wallace I, Middleton JC et al. (2022) Screening for Depression, Anxiety, and Suicide Risk in Children and Adolescents: An Evidence Review for the U.S. Preventive Services Task Force, Rockville (MD)
(2014) Health in All Policies (HiAP) framework for country action. Health Promot Int 29(Suppl 1):19–28. Doi: https://doi.org/10.1093/heapro/dau035
Moradian N, Moallemian M, Delavari F, et al. Interdisciplinary Approaches to COVID-19. Adv Exp Med Biol. 2021;1318:923–36. https://doi.org/10.1007/978-3-030-63761-3_52.
Mangione CM, Barry MJ, Nicholson WK, et al. Screening for Anxiety in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA. 2022;328:1438–44. https://doi.org/10.1001/jama.2022.16936.
Ioffe M, Pittman LD, Kochanova K, et al. Parent-adolescent communication influences on anxious and depressive symptoms in early adolescence. J Youth Adolesc. 2020;49:1716–30. https://doi.org/10.1007/s10964-020-01259-1.
Glynn LM, Davis EP, Luby JL, et al. A predictable home environment may protect child mental health during the COVID-19 pandemic. Neurobiol Stress. 2021;14:100291. https://doi.org/10.1016/j.ynstr.2020.100291.
Espinoza G, Hernandez HL. Adolescent loneliness, stress and depressive symptoms during the COVID-19 pandemic: the protective role of friends. Infant Child Dev. 2022;31:e2305. https://doi.org/10.1002/icd.2305.
Wolf S, Seiffer B, Zeibig J-M, et al. Is physical activity associated with less depression and anxiety during the COVID-19 pandemic? a rapid systematic review. Sports Med. 2021;51:1771–83. https://doi.org/10.1007/s40279-021-01468-z.
McGuinn LA, Rivera NR, Osorio-Valencia E, et al. Changes in depressive and anxiety symptoms during COVID-19 in children from the PROGRESS cohort. Pediatr Res. 2022. https://doi.org/10.1038/s41390-022-02379-z.
Masten AS, Lucke CM, Nelson KM, et al. Resilience in development and psychopathology: multisystem perspectives. Annu Rev Clin Psychol. 2021;17:521–49. https://doi.org/10.1146/annurev-clinpsy-081219-120307.
Birmaher B, Brent DA, Chiappetta L, et al. Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): a replication study. J Am Acad Child Adolesc Psychiatry. 1999;38:1230–6. https://doi.org/10.1097/00004583-199910000-00011.
Chorpita BF, Yim L, Moffitt C, et al. Assessment of symptoms of DSM-IV anxiety and depression in children: a revised child anxiety and depression scale. Behav Res Ther. 2000;38:835–55. https://doi.org/10.1016/s0005-7967(99)00130-8.
Achenbach TM, Rescorla L (2001) Manual for the ASEBA Preschool forms & profiles. Publicaciones de Psicología Aplicada. Serie Menor, núm. 80. ASEBA, Burlington, VT
Achenbach TM, Rescorla L (2001) Manual for the ASEBA school-age forms & profiles: An integrated system of multi-informant assessment. Publicaciones de Psicología Aplicada. Serie Menor, núm. 80. ASEBA, Burlington, VT
Howell CR, Gross HE, Reeve BB, et al. Known-groups validity of the Patient-Reported Outcomes Measurement Information System (PROMIS(®)) in adolescents and young adults with special healthcare needs. Qual Life Res. 2016;25:1815–23. https://doi.org/10.1007/s11136-016-1237-2.
Finbråten HS, Kleppang AL, Steigen AM. Using the Rasch measurement theory to assess the psychometric properties of the Hopkins Symptom Checklist-10 in adolescents. Health Qual Life Outcomes. 2021;19:248. https://doi.org/10.1186/s12955-021-01884-9.
Kleppang AL, Hagquist C. The psychometric properties of the Hopkins Symptom Checklist-10: a Rasch analysis based on adolescent data from Norway. Fam Pract. 2016;33:740–5. https://doi.org/10.1093/fampra/cmw091.
Burks DB (2020) The SENA: an effective clinical evaluation system in the child and adolescent population. https://virtualpsychcentre.com/the-sena-an-effective-clinical-evaluation-system-in-the-child-and-adolescent-population/. Accessed 25 May 2022
Buela-Casal G, Guillén-Riquelme A. Short form of the Spanish adaptation of the State-Trait Anxiety Inventory. Int J Clin Health Psychol. 2017;17:261–8. https://doi.org/10.1016/j.ijchp.2017.07.003.
Walter R, Remschmidt H. Untersuchungen zur Reliabilität, Validität und Faktorenstruktur einer deutschsprachigen Version der Child Behavior Checklist. Z Klin Psychol Psychother. 1999;28:177–84. https://doi.org/10.1026//0084-5345.28.3.177.
Mossman SA, Luft MJ, Schroeder HK, et al. The Generalized Anxiety Disorder 7-item (GAD-7) scale in adolescents with generalized anxiety disorder: signal detection and validation. Ann Clin Psychiatry. 2017;29:227-234A.
White D, Leach C, Sims R, et al. Validation of the Hospital Anxiety and Depression Scale for use with adolescents. Br J Psychiatry. 1999;175:452–4. https://doi.org/10.1192/bjp.175.5.452.
Reardon T, Spence SH, Hesse J, et al. Identifying children with anxiety disorders using brief versions of the Spence Children’s Anxiety Scale for children, parents, and teachers. Psychol Assess. 2018;30:1342–55. https://doi.org/10.1037/pas0000570.
Acknowledgements
We would like to acknowledge Dr Sabrina Schlesinger (Head of Research Group Systematic Reviews; German Diabetes Center) for her peer-review of the search strategy according to the Peer Review of Electronic Search Strategies (PRESS) Evidence-Based Checklist.
Funding
Open Access funding enabled and organized by Projekt DEAL. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
HLW and MB formulated the research question, with clinical feedback from JMF. All authors contributed to the study concept and design. HLW and ID screened titles, abstracts, full text and extracted data. HLW, LMP and ID assessed risk of bias. HLW and LMP conducted the GRADE assessment. HLW and MB prepared the first draft of the manuscript. HLW and ID accessed and verified all data. The corresponding author had final responsibility for deciding to submit for publication. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Dr Lisa M. Pfadenhauer (last five years): Co-author of the Cochrane reviews ‘Measures implemented in the school setting to contain the COVID‐19 pandemic: a rapid scoping review’, ‘Measures implemented in the school setting to contain the COVID‐19 pandemic’ and ‘Unintended consequences of measures implemented in the school setting to contain the COVID‐19 pandemic: a scoping review’. Prof Dr Martin Bujard (last five years): Research funding from European Union and BMBF (German Ministry of Education and Research). Travel grants and honoraria from universities, federal and state parliaments, federal and state ministries, Evangelical-Lutheran Church, Federal Agency for Civic Education. Consultant for BMFSFJ (Federal Ministry of Family, Senior Citizens, Women and Youth). Every grant and every honorarium were declared to the law office of the Federal Institute for Population Research (BiB). Prof Dr Jörg M. Fegert (last five years): Research funding from European Union, BMG (Federal Ministry of Health), BMBF (Federal Ministry of Education and Research), BMFSFJ (Federal Ministry of Family, Senior Citizens, Women and Youth), DFG (German Research Foundation), G-BA Innovation Fund, State Ministries of Baden-Württemberg and Saarland, State Foundation Baden-Württemberg, Porticus Foundation, Evangelical-Lutheran Church in Württemberg. Travel grants, honoraria, sponsorship for conferences and medical educational purposes from APK, Adenauer- and Ebertstiftung, Deutschlandfunk, DFG, DJI, DKSB, Infectopharm, med update, UNICEF, professional associations, universities and federal and state ministries. Consultant for APK, federal and state ministries. No industry-sponsored lecture series, no shareholdings, no participation in pharmaceutical companies. Every grant and every honorarium were declared to the law office of the University Hospital Ulm. No other disclosures were reported.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Additional Tables, Tables S1-S16 and additional Figures, Figures S1-S19.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ludwig-Walz, H., Dannheim, I., Pfadenhauer, L.M. et al. Anxiety increased among children and adolescents during pandemic-related school closures in Europe: a systematic review and meta-analysis. Child Adolesc Psychiatry Ment Health 17, 74 (2023). https://doi.org/10.1186/s13034-023-00612-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13034-023-00612-z