
Abstract
Background
Despite the fact that Sub-Saharan Africa bears a disproportionate burden of armed conflicts and HIV infection, there has been inadequate synthesis of the impact of armed conflict on HIV treatment outcomes. We summarized the available evidence on the impact of armed conflicts on HIV treatment outcomes in Sub-Saharan Africa from 2002 to 2022.
Methods
We searched four databases; MEDLINE, PubMed, CINHAL, and Scopus. We also explored grey literature sources and reviewed the bibliographies of all articles to identify any additional relevant studies. We included quantitative studies published in English from January 1, 2002 to December 30, 2022 that reported on HIV treatment outcomes for patients receiving antiretroviral therapy (ART) in conflict and post-conflict areas, IDP centers, or refugee camps, and reported on their treatment outcomes from sub-Saharan Africa. Studies published in languages other than English, reporting on non-ART patients and reporting on current or former military populations were excluded. We used EndNote X9 and Covidence to remove duplicates, extracted data using JBI-MAStARI, assessed risk of bias using AHRQ criteria, reported results using PRISMA checklist, and determined Statistical heterogeneity using Cochran Q test and Higgins I2, R- and RevMan-5 software were used for meta-analysis.
Results
The review included 16 studies with participant numbers ranging from 102 to 2572. Lost To Follow-Up (LTFU) percentages varied between 5.4% and 43.5%, virologic non-suppression rates ranged from 25 to 33%, adherence rates were over 88%, and mortality rates were between 4.2% and 13%. A pooled meta-analysis of virologic non-suppression rates from active conflict settings revealed a non-suppression rate of 30% (0.30 (0.26–0.33), I2 = 0.00%, p = 0.000). In contrast, a pooled meta-analysis of predictors of loss to follow-up (LTFU) from post-conflict settings identified a higher odds ratio for females compared to males (1.51 (1.05, 2.17), I2 = 0%, p = 0.03).
Conclusion
The review highlights a lack of research on the relationship between armed conflicts and HIV care outcomes in SSA. The available documents lack quality of designs and data sources, and the depth and diversity of subjects covered.
Similar content being viewed by others

Introduction
Armed conflicts have a negative impact on the health of populations, particularly on HIV patients who require strict adherence to treatment [1,2,3,4,5,6,7]. Providing regular HIV care and ensuring a continuous supply of drugs in conflict zones is difficult [2], leading to increased HIV incidence, prevalence, and related morbidity and mortality[89]. Less than 20% of people in conflict situations receive ART [10], and HIV services are scarce or nonexistent in conflict-affected countries; such as the Central African Republic (CAR), South Sudan, and parts of Yemen [10]. With 1.8 billion people living in conflict-affected areas [11], and 89.3 million people displaced from their homes by the end of 2021[12], researchers need to investigate how war affects HIV treatment.
However, there is a lack of systematic reviews investigating the connection between HIV and conflict, including the impact of armed conflict on HIV treatment outcomes. There were few systematic reviews[913,14,15,16,17] that have paid close attention to HIV prevalence and incidence as a result of armed conflict. None of the systematic reviews assessed the impact of armed conflict on HIV treatment outcomes. Given the importance of HIV treatment in reducing HIV incidence and prevalence, the double burden of HIV and conflict in Sub-Saharan Africa, and the already fragile healthcare system in the region, there is a need for systematic synthesis and exploration of this area of research. This review aims to synthesize the impact of armed conflict on HIV treatment outcomes among HIV patients affected by armed conflicts in SSA, including retention, attrition, LTFU, clinical failure, immunological failure, treatment failure, virological failure, and mortality.
Methods
Study registration
The review was registered in the International Prospective Register for Systematic Reviews (PROSPERO), with the registration number CRD42022361924 and the protocol is published online in BMJ Open [18].
Population and context
The review included individuals in sub-Saharan Africa who received antiretroviral therapy between 2002 and 2022 and were living in conflict-affected, post-conflict, or displacement areas. We selected 2002, as many sub-Saharan African countries introduced HIV care and treatment programs in 2002[19]. The review was limited to sub-Saharan Africa due to the region’s disproportionately high affected by both HIV infection [20] and armed conflicts[1621,22,23,24] (Fig. 1), weak healthcare systems, and lack of clear directives and funding for addressing HIV care in conflict-affected settings.

(Source: UCDP Version 2021)
Number of conflict-affected and conflict incidents in sub-Saharan Africa between 2002 and 2021.
Search strategy and data sources
The search was conducted using three themes: conflict, HIV care, and SSA, and was conducted in four databases. Although the initial plan was to search five databases, access to Web of Sciences was not possible. After seeking advice from our librarian, we chose to exclude Web of Sciences from our search since it had comparable literature content to SCOPUS. Consequently, we searched the remaining four databases, which included MEDLINE, PubMed, CINHAL, and SCOPUS. We also explored grey literature sources and reviewed the bibliographies of all articles to identify any additional relevant studies.
Study selection and eligibility criteria
The study only included quantitative studies conducted in English from January 1, 2002 and December 31, 2022 that focused on HIV patients receiving ART from conflict areas, IDP centers, or refugee camps, and reported on their treatment outcomes. Studies that included both conflict-affected and non-conflict-affected populations were only included if they provided data specifically for the conflict-affected group. Studies published in languages other than English, those that did not mention conflict or provide disaggregated data for conflict-affected populations, studies that involved current or former military populations, studies from countries outside of SSA, studies reporting on African refugees settled outside of SSA, studies published before 2002, and studies reporting on HIV patients not receiving ART were excluded.
Quality assessment
The search results were filtered through a multi-step process that included independent review by two reviewers, evaluation of methodological validity using standardized JBI appraisal instruments [25], and assessment of risk of bias using AHRQ criteria [26]. Disagreements among reviewers were resolved through discussion and consensus but included and extracted data from all relevant documents irrespective of their quality score.
Data extraction
We used EndNote X9 and Covidence to remove duplicates. Data were extracted using the standardized data extraction tool from JBI-MAStARI [27]. The data extracted included specific details about the authors, publication year, country of study, populations, sample size, summary of HIV treatment outcome.
Types of interventions and comparators
The review considered impact of armed conflict on HIV treatment outcomes.
Types of outcome measures
The study focused on HIV care treatment outcomes, including adherence, LTFU, clinical failure, immunological failure, virological failure, and mortality.
Operational definitions
There is no universally accepted definition of armed conflict, as it is an umbrella word for a wide range of ideas and activities, such as conflict, war, violence, terrorism, or catastrophic loss of civilian life, a civil unrest, massive displacement, and violations of human rights and international humanitarian law. While we put the definition of conflict as follows, we would like to remain open to additional definitions by authors.
Armed conflict
Is a situation in which states or other organized parties fight against each other by way of military force. Armed conflicts shall be of international and non-international armed conflicts [28].
Conflict affected areas
Are areas experiencing an armed conflict, and post-conflict regions. The area may be a region, a country, an area within a country, or an area that crosses one or more country boundaries. The impact of conflict may extend beyond the region of conflict to include surrounding areas and those hosting displaced persons. As a result, our definition remains open to the definition of authors.
Conflict -affected populations
Individuals, groups, and communities affected by and remaining in conflict-affected areas, as well as those forcibly displaced from them as refugees and IDPs. Conflict may have an impact on those who host IDPs and refugees. As a result, our definition remains open to author definition.
Internally displaced persons (IDPs)
Those who have been forced or compelled to leave their homes, often due to armed conflict, and who stay within their country’s borders.
Post-conflict
Refers to the period immediately following a conflict, when open combat is over. Nevertheless, despite its linguistic simplicity, the phrase is more challenging to define practically in terms of time, response, transformation, and sustainability. Therefore, our definition remains open to author definition.
Refugees
People who are outside their country of birth due to conflict, war, widespread violence, or feared persecution and who as a result need international protection within the African continent [29].
Data management, analysis and synthesis
The results were reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement [30] and meta regression was done to assess the relationship between armed conflict and HIV treatment outcomes. The Cochran Q test and Higgins I2[31] were used to determine statistical heterogeneity, and the random effect model was used when moderate statistical heterogeneity was detected. A meta-analysis to assess the predictors of LTFU was also conducted. The study used various statistical tools and software for analysis; R- software, STATA, and RevMan-5.
Result
Outcome of the search
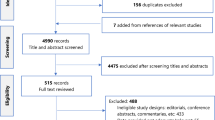
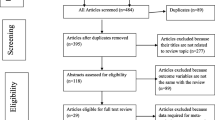
The comprehensive search identified 2487 records; 2332 identified through database searches, and 155 through manual searching of references and websites identified. All the identified 2487 references were exported into EndNote X9, and then into Covidence; 171 in the endnote, and 181 articles in the Covidence duplications were removed. After eliminating duplicates and conducting a comprehensive screening using Covidence was done, and 16 studies were considered eligible for data extraction, with 10 of them providing data for meta-analysis (Fig. 2).

PRISMA flowchart diagram of study selection impact of armed conflict on HIV care outcomes in SSA, 2002–2022
Description of included studies
The research covered in the review spanned from 2007[32] to 2022[33] and had varying follow-up periods, ranging from 4 days [34] to 60 months [35]. The majority of the studies were conducted in Western and Eastern Africa, with a significant number of studies coming from the Democratic Republic of the Congo[323335,36,37], Kenya [38,39,40], and Uganda[344142]. Most of the studies were designed as cohort studies, either retrospective[323538,39,40,4143,44,45] or prospective[3336374246]. The majority of the studies focused on adult populations[33,34,35,36,37394042,43,44], with one study [38] specifically examining children. The studies included patients who were non-IDPs[323335,36,37,384041], non-IDPs & IDPs[3439424445], refugees[4447], or a mix of these groups [43]. Ten studies were carried out in conflict settings[32,33,3436374244,45,46,47], while five took place in post-conflict zones[3538,39,40,41], and one in both [43] (Table 1 and Supplementary Table 1).
Quality assessment—Data aource/Validity/Reliability
Methodological validity of the included studies was evaluated using JBI appraisal instruments. The quality of evidence was rated as high quality (n = 7, 90.91%, n = 5, 81.82%, n = 1, 100%, n = 1, 90%, n = 1, 75%, n = 1, 72.73%) and presented moderate quality. The outcomes of the BJI assessment are shown in supplementary (supplementary Table 2).
Conflict and HIV treatment outcomes
The studies reported various outcomes, with four[33363746] focusing on the relationship between conflict and HIV treatment outcome as the primary outcome, five reporting adherence rates[3234384244], two reporting treatment interruption[3940], nine reporting LTFU[32353638414345,46,47], four reporting immunologic gain[32404243], four looking at the rate of viral non-suppression[37404547], and seven reporting mortality[32333542434647] (Supplementary Table 3).
Adherence
The review found that adherence rates among HIV patients in Sub-Saharan Africa ranged from 88.2%[44] to 99.6%[34]. The studies reported predictors of non-adherence, and non-adherence was associated with being on first-line therapy(OR = 22.22, 95% CI 1.53, 333.33; p = 0.02)[34], and feeling condemned by clinic workers (OR = 22.22, 95%CI 1.53, 333.33; p = 0.02)[34].
Pooled meta-analysis
The pooled adherence rate among HIV patients in conflict-affected SSA regions was 0.06 (0.02–0.12), I2 = 87.12%, p = 0.00, with a significant clinical heterogeneity (Fig. 3).

Pooled meta-analysis of non-adherence rate from active conflict settings among HIV patients who were on ART in SSA from 2002 to 2022
Treatment interruption (TI)
Two studies[3940] conducted in Kenya reported instances of treatment interruption, with the risk of interruption increasing by 71% during post-election violence (95%CI 34, 118, p = 0.001). Male patients (OR = 1.37, 95%CI 1.07, 1.76; p = 0.01), and who traveled more than three hours to the clinic (OR = 1.86, 95%CI 1.28, 2.71; p = 0.001) were found to be at a higher risk of treatment interruption [39]. Treatment interruptions were associated with detectable viral load, with viral loads exceeding 5,000 copies/mL and 10,00060 copies/mL[40].
Lost to follow-up
In active conflict settings, the rate of loss to follow-up (LTFU) ranged from 5.4% (95% CI = 3.2–7.5)[32] to 28.8% (95% CI: 24.9–33.1) [36], while post-conflict areas had a paradoxical level of LTFU ranging from 2.6%[38] to 43.5%[41]. The included studies indicated that factors like educational level [36], place of residence [36], prior experience with antiretroviral therapy (ART) upon enrollment [36], and the World Health Organization (WHO) clinical stage of disease [41] were linked to loss to follow-up (LTFU) among adult patients. Additionally, the study showed that receiving ART reduced the likelihood of complete loss to follow-up among children with HIV in post-crisis Kenya [38].
Pooled meta-analysis
Pooled LTFU rates of 0.16 (0.08–0.28), I2 = 98.55%, p = 0.00 were found in studies from active conflict settings[32364647], (Fig. 4), and 0.16(0.01–0.42), I2 = 99.52%, p = 0.00 post-conflict settings[353841] (Fig. 5).

Pooled meta-analysis of LTFU rate from active conflict settings among HIV patients who were on ART in SSA from 2002 to 2022

Pooled meta-analysis of LTFU rate from post conflict settings among HIV patients who were on ART in SSA from 2002 to 2022
Similarly, a review of studies conducted in post-conflict settings analyzed factors that may predict loss to follow-up (LTFU) in HIV care. The study found that only gender was statistically significant, with a 1.51 (1.05, 2.17), I2 = 0%, P = 0.03 odds ratio for LTFU in females compared to males (Fig. 6).

Meta-analysis of predictors of LTFU in post conflict-settings among HIV patients who were on ART in SSA from 2002 to 2022
Immunologic gain
CD4 gain was reported by four studies[32404243], as a secondary outcome, with changes ranging from 129 mm3[43] to a median of 163 cells/mm3[32] in six months.
Viral non-suppressions
Four studies examined the prevalence of viral non-suppression[37404547], with different thresholds ranging from > 50[4547] to > 1000 copies/mL[4547]. Three studies[374547] investigated predictors of viral non-suppression, with two finding no significant variables and one [37] reporting that being in stage III or IV of the disease (AOR = 1.86, 95% CI 1.01–3.43), and having a high baseline HIV viremia of over 1000 copies/mL(AOR = 3.41, 95% CI 1.64–7.08) were associated with increased risk [37].
Pooled meta-analysis
A pooled-analysis of two studies[4547] from active conflict settings found a pooled non-suppression rate of 30% (0.30(0.26–0.33), I2 = 0.00%, p = 0.000) using a cut-off point of > 1000 copies/mL and a follow-up period of 6–12 months (Fig. 7).

Pooled meta-analysis of virologic non-suppression rate from active conflict settings among HIV patients who were on ART in SSA from 2002 to 2022
Mortality
Seven studies provided information on mortality rates, with five conducted in active conflict settings[3233424647], and one each in post-conflict [35] and both conflict and post-conflict [43] settings. Mortality rates ranged from 3.6% (17/468)[33] to 13.0% (182/1400)[47]. Three studies[334642] examined predictors of mortality namely, socio-demographic variables such as age and sex, as well as clinical variables such as baseline ART status, viral load, CD4 count, WHO clinical stage, and adherence level were reported having associated with lower risk of mortality.
Pooled meta-analysis
A pooled-analysis of five studies from active conflict settings showed a pooled mortality rate of 0.07 (0.04–0.11), I2 = 95.84%, p = 0.00), indicating high clinical heterogeneity (Fig. 8).

Pooled meta-analysis of mortality rate from active conflict settings among HIV patients who were on ART in SSA from 2002 to 2022
Discussion
This systematic review included 16 articles published from 2002 to 2022. To the best of our knowledge, this systematic review is one of the first comprehensive reviews to assess quantitative studies in seeking to address the substantial gaps in current knowledge regarding the impact of armed conflict on HIV care outcomes in SSA.
Despite the anticipated challenges in accessing ART medication and care schedules in conflict settings[163248], such as ARV medications running out, lack of or poor access to health services, a shortage of medical professionals, and an increased burden of other medical priorities, along with the expected negative impact on HIV care outcomes[163249]; the systematic review found lower rates of non-adherence, loss to follow-up, virologic non-suppression, and mortality compared to those reported from politically stable and well-resourced regions in Sub-Saharan Africa[4350,51,52,53,54].
Furthermore, the pattern of unfavourable clinical outcomes among those HIV patients in ART reported in the included studies is driven more strongly by patient level covariates than by the evolution of the surrounding long-term conflict, socioeconomic factors[3539], socioeconomic and clinical factors[33374246], and clinical variables[343640], and these findings correspond to those of previous research in low-income countries, which also found that unfavourable clinical outcomes were associated with patient age, baseline VL, and the status of treatment before enrollment [53]. This suggests that the cause of poor clinical outcomes was likely not to have been related to armed conflict and associated factors.
The inconsistency of the studies with the perceived outcomes reflects the complex interrelationship between conflict and HIV care. Many factors could have contributed to the disparity in perceived HIV care outcomes and conflict. These include, patient commitment and creativity in obtaining treatment[3234383942], as well as education about the benefits of treatment, contribute to positive clinical outcomes. Furthermore, the results of the included studies might have been influenced by information bias, as the impact of conflict-related factors on HIV care was not taken into account. conflict could lead to a range of indirect factors that negatively affect the HIV care outcomes; such as, lack of access to safe drinking water, food insecurity, social unrest, displacement, insecurity, and destruction of livelihoods, psychosocial trauma, and the inability of health systems and other social services[16394855].
Additionally, the studies themselves had limitations, including retrospective design which rely heavily on patient charts which may have missing data and possible information bias, simplistic study (cause and effect) approach, bias in representativeness as majority of the studies were reported from NGOs funded and managed IDP sites, and a focus on adult populations rather than vulnerable groups like children. These non-governmental organizations (NGOs) are concentrated in small, stable areas. They had a small number of patients in them. The studies were also limited by their small geographic scope. The majority of HIV-infected people, however, live in remote villages.
Therefore, the systematic review highlights the limited research on the relationship between armed conflict and HIV care outcomes in Sub-Saharan Africa. Despite high double burden of armed conflicts and HIV infection in Sub-Saharan Africa, the extensive systematic search revealed that there is limited research on the relationship between armed conflict and HIV care outcomes in Sub-Saharan Africa, with only 16 eligible studies found (Fig. 9). This could be due to the belief that providing ART and conducting research during conflict is too difficult [48]. Furthermore, the existing studies focus on a limited geographic scope and adopt a simplistic cause-and-effect approach, failing to capture the complex and contentious relationship between conflict and HIV care outcomes in SSA. Additionally, the available studies failed to consider the conflict related factors, and indirect factors, post conflict settings. Additionally, pediatrics and mothers were also neglected in the available studies. The available studies fall short of addressing the realities of HIV care in conflict settings, and more research is needed to understand the impacts of armed conflicts on HIV care outcomes, especially in sub-Saharan Africa. Therefore, more research is needed to understand the reciprocal relationship between conflict and HIV care outcomes in Sub-Saharan Africa. Details of the recommended research areas are tabled in Table 2.

Mapping conflict events, and locations where studies on the impact of armed conflicts on HIV care outcomes were published, SSA between 2002 and 2021. (source: UCDP Version 21)
Conclusion
This systematic review filled a gap in study on HIV treatment outcomes in conflict zones in Sub-Saharan Africa. However, the review highlights a lack of research on the relationship between armed conflicts and HIV care outcomes in Sub-Saharan Africa. The available documents lack quality of designs and data sources, and depth and diversity of subjects covered; calling further primary studies on a prioritized future research agenda. Furthermore, there were possible limitations to the review, including there might be exclusion of studies not labeled as conflict-related, selection bias due to language limitations (the database search was limited to English), and potential confounding variables of which we are unaware might be present.
Data availability
All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the article.
Abbreviations
- ART:
-
Anti-Retroviral Therapy
- HIV:
-
Human Immuno-Deficiency Virus
- IDP:
-
Internally Displaced People
- LTFU:
-
Lost To Follow-Up
- MoH:
-
Ministry of Health
- NGOs:
-
Non-Governmental Organizations
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)
- SSA:
-
Sub-Saharan Africa
References
MSF. South Sudan: Treating HIV-Positive People Affected by Conflict, 2017.
MSF. HIV/AIDS: continuing against the deadly pandemic 2022 [ https://www.msf.org/hiv-depth.
Abay KA, Abay MH, Berhane G, et al. Access to health services, food, and water during an active conflict: evidence from Ethiopia. PLOS Global Public Health. 2022;2(11):e0001015. https://doi.org/10.1371/journal.pgph.0001015.
Daw MA, Editorial. Armed conflicts; implications, dynamics and impacts on public health care services. Front Public Health. 2022;10:1008883. https://doi.org/10.3389/fpubh.2022.1008883. [published Online First: 2023/02/03].
Niba JO, Ngasa SN, Chang N, et al. Conflict, healthcare and professional perseverance: a qualitative study in a remote hospital in an Anglophone Region of Cameroon. PLOS Global Public Health. 2022;2(11):e0001145. https://doi.org/10.1371/journal.pgph.0001145.
Rammohan A, Mavisakalyan A, Vu L, et al. Exposure to conflicts and the continuum of maternal healthcare: analyses of pooled cross-sectional data for 452,192 women across 49 countries and 82 surveys. PLoS Med. 2021;18(9):e1003690. https://doi.org/10.1371/journal.pmed.1003690.
WHO. Fragile and conflict-affected states, Health and WHO. Switherland: Country Presence Profile Geneva; 2017.
Bala NA, Azman A, Singh PSJ. Exploring Conflict, War and HIV/AIDS on Health of the Internally Displaced Persons living in North Central Nigeria: Research Square, 2021.
Mishra D, O’Laughlin K, Spiegel P. A systematic review evaluating HIV prevalence among conflict-affected populations, 2005–2020. AIDS Rev. 2021;23(3):143–52. https://doi.org/10.24875/AIDSRev.200001311. [published Online First: 2021/07/20].
Ferreyra C. ‘Double victims’ – in conflict zones, people with HIV are twice as vulnerable: OCHA services; [ https://reliefweb.int/report/world/double-victims-conflict-zones-people-hiv-are-twice-vulnerable.
WCPH. Conflict and War: A Dire Threat to Public Health. 2022.
UNHCR. Global Forced Displacemen t2022 [ https://www.unhcr.org/globaltrends/.
Ahmed BH, Giovagnoli MR, Mahad H, et al. Burden of HIV/AIDS infection before and during the civil war in Somalia. East Mediterr Health J. 2010;16(8):907–9. [published Online First: 2011/04/08].
Becker JU, Theodosis C, Kulkarni R. HIV/AIDS, conflict and security in Africa: rethinking relationships. World Hosp Health Serv. 2008;44(4):36–41. [published Online First: 2008/01/01].
Spiegel PB, Bennedsen AR, Claass J, et al. Prevalence of HIV infection in conflict-affected and displaced people in seven sub-saharan African countries: a systematic review. Lancet. 2007;369(9580):2187–95. https://doi.org/10.1016/s0140-6736(07)61015-0. [published Online First: 2007/07/03].
Spiegel PB. HIV/AIDS among conflict-affected and displaced populations: dispelling myths and taking action. Disasters. 2004;28(3):322–39. https://doi.org/10.1111/j.0361-3666.2004.00261.x.
Yucha RE. Understanding how Displacement affects Hiv Prevalence among displaced Populations- A scoping review. Public Health Theses 2019.
Hafte Kahsay K, Hailay G, Paul W. Impact of armed conflicts on HIV treatment outcomes in sub-saharan Africa: protocol for a systematic review and meta-analysis. BMJ open. 2023;13(8):e069308. https://doi.org/10.1136/bmjopen-2022-069308.
UNAIDS HIV Progress Report, 2015.
Tah F, Laith A-R, Direslgn A, et al. Global, regional, and national incidence, prevalence, and mortality of HIV, 1980–2017, and forecasts to 2030, for 195 countries and territories: a systematic analysis for the Global Burden of Diseases, injuries, and risk factors study 2017. Lancet HIV. 2019;6(12):e831–59. https://doi.org/10.1016/s2352-3018(19)30196-1. [published Online First: 2019/08/24].
Hankins CA, Friedman SR, Zafar T, et al. Transmission and prevention of HIV and sexually transmitted infections in war settings: implications for current and future armed conflicts. AIDS. 2002;16(17):2245–52. https://doi.org/10.1097/00002030-200211220-00003. [published Online First: 2002/11/21].
Mills EJ, Singh S, Nelson BD, et al. The impact of conflict on HIV/AIDS in sub-saharan Africa. Int J STD AIDS. 2006;17(11):713–7. https://doi.org/10.1258/095646206778691077. [published Online First: 2006/10/26].
Khaw AJ, Salama P, Burkholder B, et al. HIV risk and prevention in emergency-affected populations: a review. Disasters. 2000;24(3):181–97. https://doi.org/10.1111/1467-7717.00141. [published Online First: 2000/10/12].
P. P. speech delivered to the UN Security Council special session. The Situation in Africa:The Impact of AIDS on Peace and Security, New York, New York, January 10, 2000:p. 1.
Porritt K, Gomersall J, Lockwood C. JBI’s systematic reviews: study selection and critical Appraisal. Am J Nurs. 2014;114:47–52. https://doi.org/10.1097/01.NAJ.0000450430.97383.64.
Viswanathan M, Ansari MT, Berkman ND, et al. AHRQ Methods for Effective Health Care: assessing the risk of Bias of Individual Studies in Systematic Reviews of Health Care Interventions. Methods Guide for Effectiveness and comparative effectiveness reviews. Rockville (MD): Agency for Healthcare Research and Quality (US); 2008. p. 14.
Munn Z, Tufanaru C, Aromataris E. JBI’s systematic reviews: data extraction and synthesis. Am J Nurs. 2014;114:49–54.
(ICRC) ICotRC. How is the Term Armed Conflict Defined in International Humanitarian Law? 2008.
(UNHCR) UHCfR. Persons in need of international protection, June 2017.
Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–41. https://doi.org/10.1016/j.ijsu.2010.02.007. [published Online First: 2010/02/23].
Israel H, Richter RR. A guide to understanding meta-analysis. J Orthop Sports Phys Ther. 2011;41(7):496–504. https://doi.org/10.2519/jospt.2011.3333. [published Online First: 2011/07/05].
Culbert H, Tu D, O’Brien DP, et al. HIV Treatment in a conflict setting: outcomes and experiences from Bukavu, Democratic Republic of the Congo. PLoS Med. 2007;4(5):e129. https://doi.org/10.1371/journal.pmed.0040129.
Buju RT, Akilimali PZ, Tran NT, et al. Determinants of survival of HIV patients receiving Dolutegravir: a prospective cohort study in Conflict-Affected Bunia, Democratic Republic of Congo. Int J Environ Res Public Health. 2022;19(16). https://doi.org/10.3390/ijerph191610220. [published Online First: 2022/08/27].
Garang PG, Odoi RA, Kalyango JN. Adherence to antiretroviral therapy in conflict areas: a study among patients receiving treatment from Lacor Hospital, Uganda. AIDS Patient Care STDs. 2009;23(9):743–7. https://doi.org/10.1089/apc.2009.0073. [published Online First: 2009/08/04].
Akilimali PZ, Musumari PM, Kashala-Abotnes E, et al. Disclosure of HIV status and its impact on the loss in the follow-up of HIV-infected patients on potent anti-retroviral therapy programs in a (post-) conflict setting: a retrospective cohort study from Goma, Democratic Republic of Congo. PLoS ONE. 2017;12(2):e0171407. https://doi.org/10.1371/journal.pone.0171407. [published Online First: 2017/02/09].
Buju RT, Akilimali PZ, Kamangu EN, et al. Incidence and predictors of loss to follow up among patients living with HIV under Dolutegravir in Bunia, Democratic Republic of Congo: a prospective cohort study. Int J Environ Res Public Health. 2022;19(8). https://doi.org/10.3390/ijerph19084631. [published Online First: 2022/04/24].
Buju RT, Akilimali PZ, Kamangu EN, et al. Predictors of viral non-suppression among patients living with HIV under Dolutegravir in Bunia, Democratic Republic of Congo: a prospective cohort study. Int J Environ Res Public Health. 2022;19(3). https://doi.org/10.3390/ijerph19031085. [published Online First: 2022/02/16].
Yoder RB, Nyandiko WM, Vreeman RC, et al. Long-term impact of the Kenya postelection crisis on clinic attendance and medication adherence for HIV-infected children in western Kenya. J Acquir Immune Defic Syndr. 2012;59(2):199–206. https://doi.org/10.1097/QAI.0b013e31823b4448. [published Online First: 2011/10/27].
Pyne-Mercier LD, John-Stewart GC, Richardson BA, et al. The consequences of post-election violence on antiretroviral HIV therapy in Kenya. AIDS Care. 2011;23(5):562–8. https://doi.org/10.1080/09540121.2010.525615. [published Online First: 2011/02/05].
Mann M, Lurie MN, Kimaiyo S, et al. Effects of political conflict-induced treatment interruptions on HIV drug resistance. AIDS Rev. 2013;15(1):15–24. [published Online First: 2013/03/02].
OCERO AA, RETENTION OF HIV POSITIVE PERSONS AT ANTIRETROVIRAL THERAPY. CLINICS IN POST-CONFLICT NORTHERN UGANDA [MASTER OF PUBLIC HEALTH]. UNIVERSITY OF LIMPOPO; 2009.
Kiboneka A, Nyatia RJ, Nabiryo C, et al. Combination antiretroviral therapy in population affected by conflict: outcomes from large cohort in northern Uganda. BMJ (Clinical Res ed). 2009;338:b201. https://doi.org/10.1136/bmj.b201. [published Online First: 2009/02/19].
O’Brien DP, Venis S, Greig J, et al. Provision of antiretroviral treatment in conflict settings: the experience of Médecins sans Frontières. Confl Health. 2010;4(1):12. https://doi.org/10.1186/1752-1505-4-12.
Salami O, Buzu A, Nzeme C. High level of adherence to HAART among refugees and internally displaced persons on HAART in western equatorial region of Southern Sudan: J Int AIDS Soc. 2010;13(Suppl 4):P123. https://doi.org/10.1186/1758-2652-13-S4-P123. eCollection 2010.
Ssonko C, Gonzalez L, Mesic A, et al. Delivering HIV care in challenging operating environments: the MSF experience towards differentiated models of care for settings with multiple basic health care needs. J Int AIDS Soc. 2017;20(Suppl 4):21654. https://doi.org/10.7448/ias.20.5.21654.
Crellen T, Ssonko C, Piening T, et al. What drives mortality among HIV patients in a conflict setting? A prospective cohort study in the Central African Republic. Confl Health. 2019;13(1):52. https://doi.org/10.1186/s13031-019-0236-7.
Ferreyra C, O’Brien D, Alonso B, et al. Provision and continuation of antiretroviral therapy during acute conflict: the experience of MSF in Central African Republic and Yemen. Confl Health. 2018;12(1):30. https://doi.org/10.1186/s13031-018-0161-1.
Ellman T, Culbert H, Torres-Feced V. Treatment of AIDS in conflict-affected settings: a failure of imagination. Lancet (London England). 2005;365(9456):278–80. https://doi.org/10.1016/s0140-6736(05)17802-7. [published Online First: 2005/01/25].
Spiegel P, Sheik M, Gotway-Crawford C, et al. Health programmes and policies associated with decreased mortality in displaced people in postemergency phase camps: a retrospective study. Lancet (London England). 2002;360(9349):1927–34. https://doi.org/10.1016/s0140-6736(02)11915-5. [published Online First: 2002/12/21].
Brinkhof MWG, Pujades-Rodriguez M, Egger M. Mortality of patients lost to Follow-Up in Antiretroviral Treatment programmes in Resource-Limited settings: systematic review and Meta-analysis. PLoS ONE. 2009;4(6):e5790. https://doi.org/10.1371/journal.pone.0005790.
Lutalo T, Gray RH, Wawer M, et al. Survival of HIV-infected treatment-naive individuals with documented dates of seroconversion in Rakai, Uganda. AIDS. 2007;21(Suppl 6):S15–9. https://doi.org/10.1097/01.aids.0000299406.44775.de. [published Online First: 2008/01/11].
Spacek LA, Shihab HM, Kamya MR, et al. Response to antiretroviral therapy in HIV-infected patients attending a public, urban clinic in Kampala, Uganda. Clin Infect Dis. 2006;42(2):252–9. https://doi.org/10.1086/499044. [published Online First: 2005/12/16].
Braitstein P, Brinkhof MW, Dabis F, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet (London England). 2006;367(9513):817–24. https://doi.org/10.1016/s0140-6736(06)68337-2. [published Online First: 2006/03/15].
Griffiths K, Ford N. Provision of antiretroviral care to displaced populations in humanitarian settings: a systematic review. Med Confl Surviv. 2013;29(3):198–215. https://doi.org/10.1080/13623699.2013.813108.
Mills EJ, Nachega JB, Buchan I, et al. Adherence to antiretroviral therapy in sub-saharan Africa and North America: a meta-analysis. JAMA. 2006;296(6):679–90. https://doi.org/10.1001/jama.296.6.679. [published Online First: 2006/08/10].
Acknowledgements
We thank the primary authors of included studies.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
H.K.K performed the search, and employed screening and data extraction with H.A.G independently. All authors have full access to all the data in the study and have final responsibility for the decision to submit for publication. Study concept and design: P.R.W, H.A.G, H.K.K. Acquisition, analysis, or interpretation of data: P.R.W, H.A.G, H.K.K. Drafting of the manuscript: H.K.K. Critical revision of the manuscript for important intellectual content: P.R.W, H.A.G, H.K.K Meta- analysis, and mapping: A.T.G, H.K.K.Study supervision: P.R.W, H.A.G.
Corresponding author
Ethics declarations
Ethical clearance: Ethical clearance was not needed as this is based on published documents.
Consent for publication
Not applicable.
Conflict of interest
The authors declared no conflict of interest.
Disclaimer
The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the US government.
Patient and public involvement
No applicable.
Role of the sponsors
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kebede, H.K., Gesesew, H.A., Gebremedhin, A.T. et al. The impact of armed conflicts on HIV treatment outcomes in Sub-Saharan Africa: a systematic review and meta-analysis. Confl Health 18, 40 (2024). https://doi.org/10.1186/s13031-024-00591-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13031-024-00591-8