
Abstract
Background
Volunteer community health workers are increasingly being engaged in Nigeria, through the World Health Organization’s task sharing strategy. This strategy aims to address gaps in human resources for health, including inequitable distribution of health workers. Recent conflicts in rural and fragile border communities in northcentral Nigeria create challenges for volunteer community health workers to meet their community's increasing health needs. This study aimed to explore the perception of volunteers involved in task sharing to understand factors affecting performance and delivery in such contexts.
Methods
This was a qualitative study conducted in fragile border communities in north central Nigeria. Eighteen audio recorded, semi-structured interviews with volunteers and supervisors were performed. Their perceptions on how task sharing and allocation of tasks affect performance and delivery were elucidated. The transactional social framework was applied during the thematic analysis process to generate an explanatory account of the research data, which was analysed using NVivo software.
Results
Promotive and preventive tasks were shared among the predominantly agrarian respondents. There was a structured task allocation process that linked the community with the health system and mainly cordial relationships were in place. However, there were barriers related to ethnoreligious crises and current conflict, timing of task allocations, gender inequities in volunteerism, shortage of commodities, inadequate incentives, dwindling community support and negative attitudes of some volunteers.
Conclusion
The perception of task sharing was mainly positive, despite the challenges, especially the current conflict. In this fragile context, reconsideration of non-seasonal task allocations within improved community-driven selection and security systems should be encouraged. Supportive supervision and providing adequate and timely renumeration will also be beneficial in this fragile setting.
Similar content being viewed by others

Background
Africa has 25% of the global disease burden, but only 4% of the health workforce [1, 2]. In Nigeria, there is an average of 30 doctors per 100,000 population, and this varies within geopolitical zones (GPZ), with the lowest ratios in the northwest and northeast (4:100,000). The ratio is 9 doctors per 10,000 population in the northcentral geoplolitical zone [3]. The ratio for nurses and midwives is 100 and 68 per 100,000 population respectively, and again lowest in the northwest at 21 per 100,000 [4]. These human resources for health (HRH) are also inequitably distributed, with rural areas facing the largest shortages. Yet 50.48% of Nigeria’s population live in the rural areas [5], where the health needs are greater and the poverty index is worse [4, 6]. These geopolitical differences and health challenges are exacerbated by the ongoing conflicts in these areas.
In low and middle-income countries, task sharing is a solution to these HRH inadequacies; whereby less professionally qualified volunteer or paid community health workers (CHWs) are engaged to bridge the health system and poor rural communities [7, 8]. In Nigeria, the CHW programme was established and linked to the principles of primary healthcare following the Alma Ata Declaration, which is key to task shifting and community participation [9, 10]. According to the World Health Organization (WHO 2010), “task shifting is a process whereby specific tasks are appropriately moved from more professional health workers to those with shorter training and fewer qualifications” [11]. It is often used interchangeably with task sharing, which is structured around a team and needs-based approach to rationally distribute tasks among health workers [12]. Nigeria developed a National Task Sharing Policy that was implemented in 2014, to address the gaps in essential healthcare services [3]. The process involved consultations with individuals and organizations within and outside the health sector [12].
Community healthcare worker performance frameworks
The vision for CHWs laid out in the Alma Alta Declaration has not been fully realised; yet CHWs are instrumental in the delivery of health services, particularly rural and remote regions of the country. There are several frameworks aimed at supporting and improving CHWs’ performance in relation to the communities and health systems in which they work. For example, the 5-spice model [13] developed by Partners in Health, a Boston-based non-government organization (NGO) consists of five components: supervision, partners, incentives, choice and education within the healthcare system and community [13]. Whilst the logic model analyses optimal CHW performance as a function of good quality programming, within robust health systems and communities, it also explores how these actors interplay between inputs, outputs and outcomes that promote good performance [14].
Another framework is the transactional process social framework developed by Kok and colleagues [15]. This framework analyses the holistic interaction of the context, community, and health system that CHWs and their supervisors interact within. Supervision is a key hardware component of the transactional framework. The software components include their interests, relationships and power dynamics that exist in the contexts and systems they work in [8, 15]. The interplay of this environment, the economy and health policies form the power relationships and dynamics that shape the motivation of CHWs to deliver their services. This broad, analytical transactional framework is based on existing models [13, 16, 17] and findings that have been used by others to validate the framework to support improvement of healthcare services through policy development [15, 16, 18]. These frameworks can also be employed in fragile and conflict affected contexts, although the evidence base related to their application is weak [19].
Community health workers in conflict affected and fragile contexts
There is need to better understand the influence of conflict, crisis and insecurity on volunteer CHWs’ motivation, experiences, the roles they perform and the relevance of existing performance models within these contexts. Over the last decade (2001–2021), the political crisis related to ‘indigene’ rights and political representation in the Plateau State capital, Jos has developed into a protracted communal conflict affecting most parts of the State and neighbouring communities [20]. Bassa, in Plateau State (northecentral GPZ) shares boundaries with Bauchi (northeast GPZ) and Kaduna (northwest GPZ) States [21], which have experienced similar conflicts. Furthermore, the resurgence of conflicts with pastoral communities has affected the area, threatening the security of volunteer workers and activities [21]. In border and fragile settings, the process of sharing or allocation, as transactional activities, could be complicated by heightened tensions due to stronger ethic and religious differences, that in turn affect motivations or views about the role. Therefore, this study aimed to explore the perceptions, experience, and performance of CHWs in the context of task sharing within communities in Bassa, Plateau State in Northcentral Nigeria and potentially to illuminate workforce dynamics in similar situations where regions experience conflict.
Methods
Volunteer CHWs and their supervisors’ experiences were best understood through the naturalistic lens of qualitative research [22], which is based on evidence grounded in the views of participants. We employed semi-structured interviews to understand CHW and facility heads’ views and experiences on performing their tasks and roles within a conflict affected area. Participants were drawn from six primary healthcare (PHC) centres across five rural communities of Bassa (Fig. 1). These communities have experienced recent ethnoreligious crises and share borders with two States that have also experienced such challenges. The study was conducted between April to September 2019.

Source: Lekwot, Etal 2015
Map showing Plateau and surrounding states [25].
Participant characteristics
A pool of CHWs who reside in the community and provide volunteer services and the facility heads that allocate tasks to them was created [20] with the focal person at the health department of the local government area. Members of this pool were invited to participate in the study through phone calls. They were purposively and independently picked based on fulfilment of the study criteria of volunteering for at least a year and diversity in educational level and years of experience. Following informed consent processes, a total of 18 interviews including two facility heads, two assistant facility heads and 14 volunteer CHWs, were conducted by the lead researcher. After this point, there were recurring issues in the interviews, data saturation was likely to have been reached.
Data collection
All participants agreed to come to the secretariat, which was a safe space where they said they felt comfortable commenting or criticising the system. The topic guides, which were translated into the local dialect and back translated into English had previously been piloted [23, 24]. The topic guides explored the following areas: tasks allocated, support, motivations, challenges faced, and current crises faced. Detailed explanation of keeping all information confidential, anonymising the information, and having separate interviews for the two groups (CHWs and their supervisors) helped to minimise any discomfort. It was explained to all participants that they were under no obligation to answer any questions which made them uncomfortable, or that they felt were too sensitive. A comprehensive security assessment was conducted with the Plateau State Ministry of Health, focal person and facility heads of the study area to ensure that the participants and researcher were safe. Thereafter, participants were contacted by phone and invited to be interviewed.
Quality control/trustworthiness
The lead researcher was open about her positionality as a medical doctor, which helped to ensure that participants were aware of her background knowledge and the limitations of the health systems. The “bracketing off” method, which recognises the influence of positionality on the research process and outcomes [26] was deployed and use of a reflexive diary to document decisions taken, information around the iterative coding process, and emerging themes. At the end of each interview, the answers participants provided were summarised back to participants to check shared meaning through member checking [27]. A periodic audit trail, and discussion of the research process, was also conducted with co-authors at the Liverpool School of Tropical Medicine.
Data analysis
The transcribed interviews were analysed inductively, using the framework approach and NVivo 12 software [22, 28, 29]. It provided a rigorous, but flexible basis for elucidating themes [29]. This allowed for situating findings within a larger discourse and making inferences of links between themes. The transactional framework was used to supoprt the production of an explanatory account of the research data based on emerging themes. It clearly shows the relationship between the health system, CHW performance and the factors that influence these within a much wider context.
Results
To protect participant and location identity, pseudonyms were used (Table 1).
Three key themes emerged from our analysis given the inducive approach taken. (1) narratives on how the health system works (including sub themes on the selection and role of CHWs and the role of supervisors and role allocation) (2) barriers to task sharing (including barriers to performancebarriers associated with community and household conflict, the farming season and system hindrances); and (3) enablers including intrinsic motivation and community development.
Theme 1: The community health system in context: how the health system works
Selection and the role of CHWs
Study participants (CHWs and facility heads) described how CHWs are selected by communities, with the involvement of relevant community stakeholders such as men, women, youth, and religious leaders. This selection is normally completed in collaboration with the existing health system and specifically the community head. However, a participant mentioned how selection processes, especially within border states, have been influenced by ethnoreligious crises.” You know we will have to put our own in these locations…” (Male, CHW Supervisor, 15+ years of experience). The CHWs selected are generally dependent on the type of community and nature of the tasks.This is because communities have ther various health needs and sociocultural norms and recently the ethnoreligious crises have further narrowed the scope of CHWs that are selected. However, those of a certain ethnic and religious group are selected, whilst certain groups are left out of the selection process, due to fragile circumstances associated with the inclusion of non-indigenes who do not belong to the predominant religious group in that community.
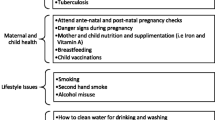
The range of tasks performed by all CHWs were mainly promotive and preventive and none had purely curative or rehabilitative roles. Health promotion tasks included awareness creation including school-based deworming, mosquito net distributions, immunizations (especially polio). “I tell the district head about the distributions and he calls the community members to inform them…” (Male, CHW, 15+ years of experience). Some also focused on personal and environmental sanitation. Preventive tasks included distributing medicines, nets distributions, immunizations and very rarely (in one participant), school eye screening. There was more priority placed on communicable diseases control.
Most participants described that gender intersects with other characteristics to shape selection processes or perceptions of the role of CHWs. However, one participant stated that lower literacy levels among females and their domestic demands limit their selection as volunteers.
“Yes, sometimes they pick equally, but sometimes we the males are more compared to the females. Sometimes you get to see that the woman is pregnant or has a newborn and sometimes lacking a cook for her children, so that alone leaves her restricted.” (Male CHW, 5- < 10 years of experience).
Another participant gave reasons for more male selections “…because when we were distributing Mectizan…it is the males who read in the past and most women are not literate…” (Male, CHW, 15+ years of experience).
The role of supervisors and task allocation
Supervisors are trained on tasks which they cascade to CHWs so they can do their roles which as outlined above are mainly focused on prevention and promotion of communicable diseases such as malaria, schistosomiasis, soil transmitted helminths and polio. Supportive supervision strctures were limited, and attitudes were mixed with some seeing supervision as either absent or punitive, for example “When we commence the work, we are with our supervisors…. If we make a mistake, they point it out, …” (Male, CHW, 15+ years of experience).
“I have never had any supervisor come to see my work since I started volunteering.” (Female, CHW, 15+ years of experience).
The task allocation process begins with training of the supervisors by the local government staff, and the supervisors then train the CHWs. The state implementers are responsible for this above the LGA level. Tasks are then collectively allocated to the CHWs by the supervisors, who rarely provide supportive supervision. Reports are then initially written by the CHWs and sometimes reviewed by supervisors and submitted, which is a rare, shared task amongst CHWs.
“I also encourage the teachers to send timely reports because if they do so, their work is complete. I also inquire that the report has been sent.” (Male CHW, 10 < 15 years of experience).
The task allocation process is clearly structured in terms of selection of volunteers, preparing them and their supervisors for the tasks, which further links the community with the health system. The views on its effectiveness were mixed.
Theme 2: Barriers and enablers to task sharing
Barriers toperformance
This theme looked at circumstances, physical and intangible barriers that limit effective task performance and allocations. Sub themes emerged around community and household conflict, the farming season and system hindrances.
Community and household conflict
Facility heads and CHWs were both faced with barriers in allocating and undertaking tasks in areas affected by conflict. A participant described the decline in community participation in health activities due to conflict stating that “but when we started this thing in 2007 to 2010 the community have been supporting but now the community are not supporting at all from the crises we experience, especially due to ethnic and religious differences.” (Female, CHW Supervisor, 15+ years of experience).
Barriers to CHWs participation in conflicted affected areas included personal choices and attitudes, ethnoreligious background and trust. The quote below summarizes the common perceptions regarding trust that may be exacerbated by ethno- religious viewpoint and linked to national legislation and the right to voluntary decisions.“Sometimes during polio, if we get to … communities and say “Asalam alakum” (the Muslim greeting), …, they tell us to stay outside and sometimes they say they will not give their children…” (Male, CHW, 5– < 10 years of experience).
All participants proferred solutions to overcoming challenges without being prompted. For example, when medicines are administered in communities by the CHWs and refusals from the community occur, the CHWs discuss the reasons why these medicines are necessary to promote healthy individuals and communities. If communities still refuse to take the medicines, despite explanations of benefits of doing so by the CHWs (which appeared to be a common experience), the focal person and the district head are informed.
At the household level, a participant linked barriers in his participation to his gendered role within his family. He highlighted their dissatisfaction with him abandoning family needs for the community, which was seen as not providing much gain. Another participant also shared similar views regarding this. “…Challenges may come from your wife or children saying you have refused to do what will help the home, but something that is not beneficial.” (Male, CHW, 10 < 15 years of experience). This was a recurring challenge from family members, and amplified in contexts of poverty.
Timing of task allocation
Some participants mentioned the rainy season as being a hindrance to them and coinciding with peak periods of medicines and net distributions, leading to community inaccessibiliy, increased attrition rates and negatively affecting farmwork. This was linked to the broader economic challenges they face.
“… Sometimes I don’t go to the farm… and when distributing drugs I can’t go to the farm except I give money to people that will go to farm for me,…” (Male CHW Supervisor, 10 < 15 years of experience).
This contributed to CHW attrition as emphasised by a participant; “Some have stopped because of this.” (Male, CHW, 5– < 10 years of experience). The majority of CHWs suggested the need for a change in timing of campaign based activities to support them to fulfil their role in this task shifting activity.
Financial and logistical limitations
The financial remunerations increased over the years and CHWs were paid in cash ($6.30 naira equivalent; 3500 per task allocation round) in 2018. However, this has currently changed to bank payments which has resulted in delayed or no payments to the CHWs, as most of them do not have bank accounts. Those who have them, travel to urban areas where the banks are, which can bring additional security challenges. They spend transportation costs and are left with little, as bank charges are deducted. A facility head mentioned this and how the current dwindling support led to attrition.
“…,CDDs what they are giving them the community is not supporting them thinking that the NGOs are supporting them, but the NGOs is only the transport allowance that they are giving them…” (Female, CHW Supervisor, 15+ years of experience).
A participant mentioned scarcity of commodities as a major system challenge. This also affected his own household as he forfeited his net for a community member, showing some of the sacrifices CHWs make. …“I was given 100 nets… I initially kept one for myself, but an elderly man said he did not get one, so I gave him my own…” (Male, CHW, 15+ years of experience).
Logistic challenges related to transportation and financing were also mentioned by most participants. Some of them incurred out of pocket spending, as a result. Additionally, a robust system for logistics does not exist. “When we distributed nets, we used my brother’s motorcycle and went house to house using our own money. We did not receive any money for that…” (Male, CHW, 10– < 15 years of experience).
The need for more structured and stable incentivisation was a clear theme and a common view amongst both supervisors and CHWs.
Enablers
Intrinsic motivation
Clear strong themes here included the intrinsic motivation among CHWs to volunteer and attributing most of their rewards to blessings from God, despite the often unsafe contexts that they work in. A participant expressed this as, “…I am happy to do this because of the recognition I get in the community. Some think I am a health worker, and this makes me happy…, I am well respected.” (Male,CHW, 15+ years of experience). Support from supervisors motivated them the most, despite the challenges they faced by living and working in conflict contexts.
A participant emphatically mentioned that “I am happy that you came because if we are doing this work and are being called and asked questions like this, it is good… This has not been done here since I started.” (Female, CHW Supervisor, 0 < 5 years of experience). This emphasises how CHWs (unlike in many contexts) have not participated in research, and have limited opportunities to share their expereinces and the challenges they face in these fragile contexts.
Community development
Partner support through financial support and the provision of medicines, bed nets among other commodities that CHWs distribute to their communities, was a powerful sentiment enabling most volunteers. A CHW had this to say…” the medicines are donated to us from the foreign nations. They told us the value in foreign currency and if we are to convert it to our own, it will be a lot of money…” (Male, CHW, 5– < 10 years of experience).
Discussion
Our study illuminates how CHW performance is a transactional social process shaped by context, system and intervention hard and software [8, 15]. We adapt Kok et al.’s model (2017) in Fig. 2 below to illustrate how community health systems in the the context of fragile border regions, (where there are ethnic and religious differences) in Nigeria are in turn shaped by interests, relationships and power dynamics that exist in the contexts and systems. These shape selection of CHWs, their role allocation, the supervision process and the barriers and enablers they face in their day to day work.

Illustration of key discussion points in relation to Kok et al.’s (2017) transactional framework process (adapted by authors)
System software and hardware: power, values, norms, trust and selection of volunteers; task allcoation and supervision
Volunteer selection
All participants agreed on the need for a transparent selection process that promotes gender equity, ability and that community participation supports CHWs. However, some role and literacy related gender and ethinic/relgious inequalities in selection emerged confirming studies in other contexts. In Nigeria, there were “silent” concerns about a truly transparent selection process due to security concerns, [30]. Furthermore, as reflected in studies elsewhere (Afghanistan) community leader “dominance” in the selection process could introduce bias in selection [31].
Task allocation
According to the WHO, the starting point for an effective design of CHW programmes is a sound situation analysis of population needs, health system necessities and resource allocation [32]. This may explain the focus of supporting partners and the mainly promotive and preventive tasks that CHWs are trained on and expected to undertake; and is also in accordance with national guidelines [3, 4]. The focus on tasks which are promotive and preventive, including community sensitization, mobilization and medicines distributions is in line with Perry et al.’s, [33] analysis of CHWs core tasks. In all 36 states in Nigeria and the Federal Capital Territory, one of the priority areas is combatting malaria [3], hence most CHWs performed these tasks, and others linked to national priorities.
Supervision, power and decision making: linking volunteer CHWs and the health system
The presence of some supportive supervision and cordial working relationship among participants emerged from the analysis. Community support was invaluable, as they were familiar with each other and the trust, values and community norms that they share. However, there were mixed views, on supervision and the gaps in the supervision process was mainly around attitudes of the CHWs to the allocated tasks.CHWs perceived that they are not fully involved in decision making, which they felt was made for them by their supervisors.
These findings differ from other studies [2, 24]. In a Mozambiquan study, CHWs felt that supervision was more fault finding than supportive. The supervisors also had no training and felt the workload of providing clinical facility-based services and community supervision was challenging [8, 34]. Again in a sysematic review, the need for a balance between the community and health facility was emphasised [35]. In a study conducted in Mkuranga District of Tanzania, the community were unaware of the CHWs [36], showing a gap in the link between and within all components of the transactional framework [37]. In our study, supervision as a key hardware component of the transactional framework [38], shaped CHWs on allocated tasks and enabled their performance in this study.
Enablers, motivators, barriers and their interlinkages
The community, economy and health system comprised the environment that enabled, motivated or created barriers for effective performance in this study. The interplay of themes and subthemes in these crucial determinants of performance among participants showed the interrelated, yet contradictory relationships between them. An enabler may simultaneously be a motivator and demotivator. For instance, financial partner and community support enabled and motivated as well as demotivated participants, when it was adjudged as inadequate, untimely, or as paid via inconvenient means. This links to debates in the literature around incentivising volunteer CHWs and the importance of the provision of stable financial remuneration [8, 39,40,41]. Power in decision making regarding mode of payment of CHWs by the system was a major concern for the supervisors.
In several studies, including one conducted among supervisors in Durna, South Africa, and with CHWs in Bangladesh, financial incentives did not demotivate CHWs to continue providing services, whilst reocognising the importance of collaboration between the community and health sector [34, 42,43,44,45]. Task allocations in the rainy season hindered most participants, who are farmers from farmwork. This is a recurring system challenge that could exacerbate the attrition rate.
Although majority of the participants willingly volunteered, they collectively attributed it to divine and national patriotic reasons, which is a common finding among the religious Nigerian population and has been identified in other contexts too, e.g. Bangladesh, Ethiopia, Indonesia, Kenya, Malawi, Mozambique Nepal, and Tanzania [46,47,48].
Implications for the context, conflict, fragility and the rest of Nigeria and beyond
The National Task Sharing Policy should be reviewed in collaboration with the volunteer CHWs and their supervisors with more emphasis on broader task allocations in line with current priorities, remuneration, integration and clear task allocation process. This will ensure that their voices are heard. Furthermore, the varying contexts, ethnic, religious and security situations CHWs work in should be acknowledged within the policy with clearly stated strategies on how to tackle such challenges. Challenges of CHWs are similar to existing underlying challenges, and dwindling community support (found in many contexts) but are also shaped by fragility and security challenges. Priority areas to support this criticial cadre should include seasonal considerations, accessibility, and a clearly defined incentive package, which was the main concern of all participants in this study, following the current security challenges.They will need additional resources for better planning, in case of unforeseen challenges that these conflict contexts may create for them, their families and the communities that they live and work in. Dialogue with community leaders and training of staff on health delivery in interborder conflict will be beneficial.
Study strengths and weaknesses
The main strength of this study was the inclusion of participants from a variety of communities sharing borders with two states to explain their perceptions and compare them with their supervisors’. Hence, the study contributes to developing a community and health systems-based approach to task sharing studies within fragile contexts. The main weakness was that data collection did not include beneficiaries of these services provided by the implementers. This was because of the existing security challenges in the study sites, which limited travel to physically collect this data. Including community perspectives would have been illuminating and could be the focus of future research. Relatively few female CHWs were recruited into the study.
Conclusion
This study showed that promotive and preventive tasks are performed by CHWs, through an established task allocation process, linking the communities with the health system. CHWs work in these fragile and rural communities is challenging, with recurring crsies, ethno religious unrests and medicine and bed net distributions were undertaken through risky terrains. Understanding CHWs perspectives is critical: they were motivated by a complex interplay of extrinsic and intrinsic motivation and demonstrated personal commitement and zeal to provide services in challenging circumstances. More collaborative, multidisciplinary relationships and research with implementers at community levels and the health system could facilitate co-creation of interventions such as collective microplanning, development of more robust security cover for implementers and a gender sensitive implementation process that can serve as advocacy toolkits for similar fragile and conflict contexts to learn from.
Availability of data and materials
All data and materials used for his study can be accessed upon request from the corresponding author.
Abbreviations
- CHW:
-
Community health worker
- HRH:
-
Human resources for health
- NGO:
-
Non-governmental organization
- WHO:
-
World Health Organization
References
Okyere E, Mwanri L, Ward P. Is task-shifting a solution to the health workers’ shortage in Northern Ghana? PLoS ONE. 2017;12(3): e0174631.
World Health Organization. Global strategy on human resources for health: workforce 2030. 2016. https://www.who.int/hrh/resources/globstrathrh-2030/en/.
Federal Ministry of Health (FMOH). Task sharing and task shifting policy for essential healthcare. 2014. https://advancefamilyplanning.orgf/.
Federal Republic of Nigeria (FRN). Human Resources for Health Strategic Plan 2008–2012. 2007. https://www.who.int/workforcealliance/countries/Nigeria_HRHStrategicPlan_2008_2012.pdf.
National Population Commission (NPC), National Bureau of Statistics (NBS). Plateau (State, Nigeria)—population statistics, charts, map and location. 2020. https://www.citypopulation.de/php/nigeria-admin.php?adm1id=NGA032.
National Bureau of Statistics (NBS). Labour force. 2010. http://nigerianstat.gov.ng/download/41.
Raven J, Akweongo P, Baba A, Baine SO, Sall MG, Buzuzi S, et al. Using a human resource management approach to support community health workers: experiences from five African countries. Hum Resour Health. 2015;13(1):45.
Raven J, Wurie H, Idriss A, Bah AJ, Baba A, Nallo G, et al. How should community health workers in fragile contexts be supported: qualitative evidence from Sierra Leone, Liberia and Democratic Republic of Congo. 2020.
World Health Organization (WHO). Alma Ata Declaration. 1978. https://www.who.int/social_determinants/tools/multimedia/alma_ata/en/.
World Health Organization (WHO). First global conference on task shifting. 2008. https://www.who.int/mediacentre/events/meetings/task_shifting/en/.
World Health Organization (WHO). Task shifting to optimise the roles of health workers to improve the delivery of maternal and child healthcare. 2010. https://www.who.int/evidence/sure/PBExecutivesummaryUganda.pdf?ua=1.
World Health Organization (WHO). Task sharing to improve access to Family Planning/Contraception. 2018. https://www.who.int/reproductivehealth/publications/task-sharing-access-fp-contraception/en/.
Palazuelos D, Ellis K, DaEun ID, Peckarsky M, Schwarz D, Bertrand Farmer D, et al. 5-SPICE: the application of an original framework for community health worker program design, quality improvement and research agenda setting. Glob Health Action. 2013;6(1):19658.
Naimoli JF, Frymus DE, Wuliji T, Franco LM, Newsome MH. A community health worker “logic model”: towards a theory of enhanced performance in low-and middle-income countries. Hum Resour Health. 2014;12(1):56.
Kok MC, Ormel H, Broerse JEW, Kane S, Namakhoma I, Otiso L, et al. Optimising the benefits of community health workers’ unique position between communities and the health sector: a comparative analysis of factors shaping relationships in four countries. Glob Public Health. 2017;12(11):1404–32.
Kok MC, Dieleman M, Taegtmeyer M, Broerse JEW, Kane SS, Ormel H, et al. Which intervention design factors influence performance of community health workers in low-and middle-income countries? A systematic review. Health Policy Plan. 2015;30(9):1207–27.
Kok MC, Broerse JEW, Theobald S, Ormel H, Dieleman M, Taegtmeyer M. Performance of community health workers: situating their intermediary position within complex adaptive health systems. Hum Resour Health. 2017;15(1):1–7.
Dieleman M, Kane S, Zwanikken P, Gerretsen B, World Health O. Realist review and synthesis of retention studies for health workers in rural and remote areas. 2011.
Raven J, Wurie H, Idriss A, Bah AJ, Baba A, Nallo G, et al. How should community health workers in fragile contexts be supported: qualitative evidence from Sierra Leone, Liberia and Democratic Republic of Congo. Hum Resour Health. 2020;18(1):1–14.
Gentles SJ, Charles C, Ploeg J, McKibbon KA. Sampling in qualitative research: insights from an overview of the methods literature. Qual Rep. 2015;20(11):1772–89.
Krause J. A deadly cycle: ethno-religious conflict in Jos, Plateau State, Nigeria. 2010.
Ritchie J, Lewis J, Nicholls CM, Ormston R. Qualitative research practice: a guide for social science students and researchers. Sage; 2013.
Castillo-Montoya M. Preparing for interview research: the interview protocol refinement framework. Qual Rep. 2016. https://doi.org/10.46743/2160-3715/2016.2337.
Cataldo F, Sam-Agudu NA, Phiri S, Shumba B, Cornelius LJ, Foster G. The roles of expert mothers engaged in prevention of mother-to-child transmission (PMTCT) programs: a commentary on the INSPIRE studies in Malawi, Nigeria, and Zimbabwe. JAIDS J Acquir Immune Defic Syndr. 2017;75:S224–32.
Lekwot VE, Anita U, Yakubu A, Ryeshak A. Impact of Lamingo Dam on the socio-economic activities of the people in Jos Area of Plateau State, Nigeria. Int J Case Stud. 2015;3(12):33.
Priya A. Phenomenological social research: some observations from the field. Qual Res J. 2017. https://doi.org/10.1108/QRJ-08-2016-0047.
Thomas DR. Feedback from research participants: are member checks useful in qualitative research? Qual Res Psychol. 2017;14(1):23–41.
Campbell SJ, Osei-Atweneboana MY, Stothard R, Koukounari A, Cunningham L, Armoo SK, et al. The COUNTDOWN study protocol for expansion of mass drug administration strategies against schistosomiasis and soil-transmitted helminthiasis in Ghana. Trop Med Infect Dis. 2018;3(1):10.
Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):1–8.
Krause J. A deadly cycle: ethno-religious conflict in Jos, Plateau State, Nigeria: Geneva declaration; 2011.
Najafizada SAM, Labonté R, Bourgeault IL. Community health workers of Afghanistan: a qualitative study of a national program. Confl Heal. 2014;8(1):26.
World Health Organization (WHO). WHO guideline on health policy and system support. 2018. https://apps.who.int.
Perry H, Zulliger R. How effective are community health workers? 2013. https://ccmcentral.com/wp-content/uploads/2013/12/How-Effective-are-CHWs-Evidence-Summary-Condensed_JHSPH_2012.pdf.
Naimoli JF, Perry HB, Townsend JW, Frymus DE, McCaffery JA. Strategic partnering to improve community health worker programming and performance: features of a community-health system integrated approach. Hum Resour Health. 2015;13(1):46.
Wallace C, Farmer J, McCosker A. Community boundary spanners as an addition to the health workforce to reach marginalised people: a scoping review of the literature. Hum Resour Health. 2018;16(1):46.
Mubyazi GM, Mushi AK, Shayo E, Mdira K, Ikingura J, Mutagwaba D, et al. Local primary health care committees and community-based health workers in Mkuranga district, Tanzania: does the public recognise and appreciate them? Stud Ethno-Med. 2007;1(1):27–35.
Mundeva H, Snyder J, Ngilangwa DP, Kaida A. Ethics of task shifting in the health workforce: exploring the role of community health workers in HIV service delivery in low-and middle-income countries. BMC Med Ethics. 2018;19(1):71.
Ochieng BM, Akunja E, Edwards N, Mombo D, Marende L, Kaseje DCO. Perceptions of health stakeholders on task shifting and motivation of community health workers in different socio demographic contexts in Kenya (nomadic, peri-urban and rural agrarian). BMC Health Serv Res. 2014;14(S1):S4.
Corley AG, Thornton CP, Glass NE. The role of nurses and community health workers in confronting neglected tropical diseases in Sub-Saharan Africa: a systematic review. PLoS Negl Trop Dis. 2016;10(9): e0004914.
Singh D, Negin J, Otim M, Orach CG, Cumming R. The effect of payment and incentives on motivation and focus of community health workers: five case studies from low-and middle-income countries. Hum Resour Health. 2015;13(1):1–12.
Theobald S, MacPherson E, McCollum R, Tolhurst R. Close to community health providers post 2015: realising their role in responsive health systems and addressing gendered social determinants of health. BioMed Cent. 2015. https://doi.org/10.1186/1753-6561-9-S10-S8.
Razee H, Whittaker M, Jayasuriya R, Yap L, Brentnall L. Listening to the rural health workers in Papua New Guinea—the social factors that influence their motivation to work. Soc Sci Med. 2012;75(5):828–35.
Akintola O, Chikoko G. Factors influencing motivation and job satisfaction among supervisors of community health workers in marginalized communities in South Africa. Hum Resour Health. 2016;14(1):54.
Rahman A, Malik A, Sikander S, Roberts C, Creed F. Cognitive behaviour therapy-based intervention by community health workers for mothers with depression and their infants in rural Pakistan: a cluster-randomised controlled trial. Lancet. 2008;372(9642):902–9.
Rahman SM, Ali NA, Jennings L, Seraji MHR, Mannan I, Shah R, et al. Factors affecting recruitment and retention of community health workers in a newborn care intervention in Bangladesh. Hum Resour Health. 2010;8(1):1–14.
Glenton C, Colvin CJ, Carlsen B, Swartz A, Lewin S, Noyes J, et al. Barriers and facilitators to the implementation of lay health worker programmes to improve access to maternal and child health: a qualitative evidence synthesis. Cochrane Database Syst Rev. 2013. https://doi.org/10.1002/14651858.CD010414.
Mpembeni RN, Bhatnagar A, LeFevre A, Chitama D, Urassa DP, Kilewo C, et al. Motivation and satisfaction among community health workers in Morogoro Region, Tanzania: nuanced needs and varied ambitions. Hum Resour Health. 2015;13(1):1–10.
Ormel H, Kok M, Kane S, Ahmed R, Chikaphupha K, Rashid SF, et al. Salaried and voluntary community health workers: exploring how incentives and expectation gaps influence motivation. Hum Resour Health. 2019;17(1):1–12.
Johnston B. Confidentiality and qualitative research. MA Healthcare; 2015.
Kamanzi A, Romania M. Rethinking confidentiality in qualitative research in the era of big data. Am Behav Sci. 2019. https://doi.org/10.1177/2F0002764219826222.
Acknowledgements
Dr. Azzuwut Martyn Polycarp (of blessed memory), whose assistance with speedy in country ethics is deeply appreciated. Bassa local government staff, especially Mrs. Ayok, who facilitated a smooth data collection process. Friends and colleagues; Shareen Chowdury and Helen Piotrowski, assiated with coaching on NVivo, and to all the participants, for their time and shared experiences. The COUNTDOWN consortium, led by the Liverpool School of Tropical Medicine and implemented in Nigeria by Sightsavers co- funded the Masters programme. Thank you Nigeria COUNTDOWN team; Tosin Adekeye, Damian Lawong, Akinola Oluola, James Nyashiyi, Noela Gwani and Gideon Kevin for their support.
Funding
This research was self- funded as a fulfilment for the lead author’s Masters in international Public Health (MIPH).
Author information
Authors and Affiliations
Contributions
The corresponding author, LL designed the study, collected, and analysed the data, and wrote the manuscript. MS and ST supervised the study and provided feedback on the conceptual design of the study. LD and KO reviewed all sections of the study and provided support with data analysis. SI and CM critically revised the manuscript and its contents. All authors gave their approval of the final drafted manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from Liverpool School of Tropical Medicine (ethics application 1907) and the Plateau State Ministry of Health (MOH/MIS/202/Vol. T/X). All data was stored securely in password protected files without identifying information and paper copies were locked in drawers and only accessible to the research team [49, 50]. Whilst confidentiality was ensured, considering that CHWs and their supervisors were interviewed, anxiety may have ensued in the former. The CHWs may have felt hesitant to openly criticize the system that they work in (and by implication their supervisors). Therefore, the interviews were scheduled on different days for each category of participants. Both institutional (Liverpool School of Tropical Medicine) and in country (Plateau Ministry of Health) ethical approvals and written informed consents of all participants are available for sighting.
Consent for publication
Not applicable.
Competing interests
The authors declare that they do not have any competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lar, L., Stewart, M., Isiyaku, S. et al. Does inter-border conflict influence the views of task sharing among community health volunteers in Nigeria? A qualitative study. Confl Health 16, 43 (2022). https://doi.org/10.1186/s13031-022-00472-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13031-022-00472-y