
Abstract
Neurodegenerative diseases, such as Alzheimer’s disease (AD), Parkinson’s disease (PD), Huntington’s disease (HD) and amyotrophic lateral sclerosis (ALS), affect millions of people every year and so far, there are no therapeutic cures available. Even though animal and histological models have been of great aid in understanding disease mechanisms and identifying possible therapeutic strategies, in order to find disease-modifying solutions there is still a critical need for systems that can provide more predictive and physiologically relevant results. One possible avenue is the development of patient-derived models, e.g. by reprogramming patient somatic cells into human induced pluripotent stem cells (hiPSCs), which can then be differentiated into any cell type for modelling. These systems contain key genetic information from the donors, and therefore have enormous potential as tools in the investigation of pathological mechanisms underlying disease phenotype, and progression, as well as in drug testing platforms. hiPSCs have been widely cultured in 2D systems, but in order to mimic human brain complexity, 3D models have been proposed as a more advanced alternative. This review will focus on the use of patient-derived hiPSCs to model AD, PD, HD and ALS. In brief, we will cover the available stem cells, types of 2D and 3D culture systems, existing models for neurodegenerative diseases, obstacles to model these diseases in vitro, and current perspectives in the field.
Similar content being viewed by others

Background
Alzheimer’s disease (AD), Parkinson’s disease (PD), Huntington’s disease (HD) and amyotrophic lateral sclerosis (ALS) are all neurodegenerative disorders characterized by abnormal protein deposition and progressive loss of specific neuronal populations, leading to their specific clinical manifestations [1,2,3]. These diseases affect millions of people every year and so far, there are no therapeutic cures available. Most current treatments are not disease modifying, but instead provide only some symptomatic relief to the patients. Looking at pharmaceuticals success rates, the probability of a drug for a neurodegenerative disease progressing from Phase 1 trials to US Food and Drug Administration approval is around 10% [4]. Reasons for this low success rate include the difficulty in identifying disease aetiology, the gap in translation between animal and human studies and a lack of appropriate human models to determine underlying mechanisms of action and for pre-clinical testing [5]. In order to find more effective treatments, there is a critical need for better experimental models that can provide more predictive and physiologically relevant results. To this end, one possible avenue is the development of human induced pluripotent stem cell (iPSC)-derived models for use in parallel with animal models to better understand disease mechanism and discover the best targets to take forward into clinical trials.
Pluripotent stem cells (PSCs) such as embryonic stem cells (ESCs) are undifferentiated cells with self-renewal capability and the potential to differentiate into any cell type of the body, providing the possibility to model human cells and tissues in vitro. Before 2007, the only source of human PSCs for research was ESCs. In 2006, Takahashi and Yamanaka generated iPSCs from mouse somatic cells, later repeated with human cells, known as hiPSCs [6, 7]. The advent of hiPSC technology has opened up new possibilities for biomedical research. This breakthrough gave scientists access to human embryonic-like stem cells, while avoiding many of the ethical limitations related to the use of human embryos in scientific research. Importantly, hiPSCs can be obtained directly from any individual, including patients carrying important disease-specific genetic information, which is essential for the study of diseases that are exclusively monogenic (e.g. HD), and pathologies that can be found in both familial or sporadic forms of disease (e.g. AD, PD, ALS) [8,9,10]. Therefore, patient-derived hiPSCs have the potential to increase accuracy in drug discovery and precision in diagnosis.
In the developing and adult human central nervous system (CNS), neural stem cells (NSCs) and neural progenitor cells (NPCs) receive a range of spatiotemporal instructive cues that guide their maintenance, differentiation into specialised neurons and glia, and subsequent behaviour [11, 12]. To generate physiologically relevant models of the human brain in vitro, stem cell-based systems thus often aim to recapitulate in vivo conditions, including pathophysiological mechanisms observed in vivo, to provide more accurate and reliable systems for understanding disease, drug testing or diagnostics [13]. Conventional two-dimensional (2D) cell culture systems have been an extremely valuable tool that have provided important knowledge for more than 100 years, offering simplified and low-cost methods for modelling CNS diseases [14, 15]. However, scientists argue that 2D models do not mimic human brain complexity, creating a need for more physiologically relevant models. For example, in 2D models for AD, changing the culture medium regularly can remove the secreted amyloid beta (Aβ) species secreted into the cell culture media, thus interfering with and biasing the analysis of Aβ aggregation. Three-dimensional (3D) systems might better mimic the restrictive environment of human brain, allowing Aβ deposition and aggregation by limiting the diffusion of secreted Aβ into the cell culture medium and enabling the formation of niches that accumulate high concentrations of Aβ [16,17,18]. 3D models have been proposed as a way to more closely recapitulate in vivo CNS architecture and are thus more realistic models that could fulfil an existing gap between 2D cell culture and animal models. Indeed, 3D cultures have already been shown to be superior to 2D in investigating cell-ECM interaction, cell differentiation, cell-cell connections and electrophysiological network properties [15, 19, 20].
This review will focus on the use of stem cells, particularly hiPSCs, to model neurodegenerative diseases. In brief, we will cover the available stem cells types, types of 2D and 3D culture systems and materials, existing disease models, obstacles to model diseases such as AD, HD, PD and ALS in vitro, and current perspectives in the field.
Main text
Pluripotent stem cells
Stem cells can decrease the need for using animal models, avoiding several concerns regarding animal wellbeing in scientific research. These can be divided into PSCs (ESCs and iPSCs), and adult/tissue-specific stem cells (multipotent and unipotent stem cells) [21,22,23,24]. PSCs have an indefinite self-renewal capability and can differentiate in all cell types of the three germ layers, including neural cell types [21]. Such cells have been widely used for disease modelling [10, 25,26,27,28], tissue engineering [29, 30] and regenerative medicine [31]. ESCs derived from the inner cell mass of a developing blastocyst were the only available PSCs until the discovery of iPSC technology. This now means that PSCs can be obtained from somatic cells through reprogramming using specific factors including the original ‘Yamanaka factors’: OCT3/4, SOX2, C-MYC and KLF4 [6, 24]. At first, iPSCs were obtained by methods that would leave residual transgene sequences from the reprogramming vectors, which could lead to unwanted or unpredictable effects in cell behaviour [23, 30,31,32]. In the last few years, new protocols have been developed (e.g. use of Sendai virus, RNA-based methods and episomes) using vectors or reagents that do not integrate or leave any residual sequences into iPSCs genome, and therefore create footprint-free iPSCs [32]. The discovery of iPSCs also has major implications for the ethical concerns surrounding the use of human ESCs, circumventing the need for human embryos in PSC research. Nowadays, iPSCs are widely studied and many protocols are available to differentiate them into a wide range of cell types, including CNS cells [8, 10, 33,34,35,36].
During embryonic development in mammals, all neurons and glia of the CNS (except microglia) are derived from NSCs of neuroectodermal origin (also known as neuroepithelial cells) [37, 38]. Knowledge of in vivo developmental programmes and interactions that lead to the subsequent generation of specific types of neurons and glia can be used to direct the differentiation of human PSCs (and their progeny) into mature CNS cell types in vitro, such as cortical neurons [39], dopaminergic neurons [40], astrocytes [41] and oligodendrocytes [42, 43] (see also [44] for a recent review and further discussion below). In the adult CNS, NSCs can be found in two neurogenic niches: the subgranular zone (SGZ) of the hippocampal dentate gyrus, and the sub-ventricular zone (SVZ) of the lateral wall of the lateral ventricle [12, 45,46,47]. These are sometimes referred to as neurovascular niches due to the close association and importance of associated vasculature [48]. In both niches, NSCs give rise to a range of differentiated neurons and glia via specific intermediates [49, 37, 49, 50]. The niches provide essential nutritional and structural support, as well as maintain NSCs and influence subsequent cell fate and function; these factors are controlled by extracellular and physical cues, including (but not limited to) growth factors (e.g. brain-derived neurotrophic factor (BDNF) and nerve growth factor (NGF)), morphogens (e.g. Notch and bone morphogenic proteins), and both cell-cell and cell-ECM interactions [12, 13, 47]. Understanding normal CNS development and the role of NSC niches can thus provide important knowledge that can be exploited to develop and improve human PSC and other stem cell-based in vitro models to better mimic the in vivo microenvironment and cell behaviour. The more realistic the model, the better it is expected to function as an accurate and robust system for the elucidation of CNS function and dysfunction, drug screening or interrogation of underlying mechanisms of various neuropathologies, including neurodegenerative diseases.
In vitro models
Although animal models offer the possibility to study both physiological and behavioural mechanisms (which most other alternatives do not), they do not always provide translatable results in pre-clinical drug screening for humans due to inter-species differences [51, 52]. Human post-mortem material also plays an important role for studying diseases, providing important pathohistological information. However, this tissue has limited availability, lacks important information such as cell function and behaviour due to tissue degeneration, and does not allow the observation of disease progression [53]. Thus, in vitro models, especially patient-derived iPSCs, can be used in parallel with animal models and post-mortem material to study CNS disorders. These models can also provide a relatively inexpensive research tool and offers scientists the opportunity to observe disease progression in vitro, understand underlying mechanisms and identify new therapeutic targets.
2D models
Conventional 2D cultures became possible in 1907 [54]. This type of model consists of cells plated directly on a rigid substrate (e.g. polystyrene or glass), usually coated with substrates that mimic ECM composition, promote cell adhesion and can support desired cell behaviour such as proliferation or differentiation [20, 55, 56]. For example, laminin, poly-ornithine, poly-lysine and fibronectin are standard coating substrates for cell culture [56, 57]. They foster cell adhesion through integrin receptors [58], contribute to NSC differentiation via extracellular signal-regulated kinase (ERK) ERK signalling [59], facilitate cell attachment due to electrostatic attraction with the cell surface [60, 61], coordinate synaptogenesis and synaptic activity [62], and regulate neural cell migration and neurite outgrowth by interacting with different proteins, e.g. integrins and tenascins (major component of CNS ECM) [15, 58, 62,63,64,65,66,67]. Despite the unquestionable importance of traditional 2D models, especially considering that they provide a relatively cheap and reproducible tool to be used in parallel with animal models, they do not mimic real brain tissue complexity and organization, limiting interaction between cells to only side-by-side contact and lacking nutrient/oxygen diffusion and waste removal dynamics [20, 55]. These modelling limitations can impact on cell morphology [68], survival [69], proliferation and differentiation [70], and thus on disease mechanisms [71]. This led to efforts to develop more complex platforms including 3D models.
3D models5
There are two main approaches to develop 3D cultures: scaffold-free techniques and scaffold-based techniques. The first can be generated by growing cells in 3D self-assembled spherical clusters (sometimes referred to as cell aggregates or spheroids), which do not contain added biomaterials and the ECM present is produced only by cells themselves [19, 72]. Conversely, scaffold-based 3D cultures can be obtained by seeding/dispersing cells into 3D solid or liquid matrices made from either natural or synthetic materials (e.g. Matrigel™, Alvetex®) and using the material to provide cell-matrix interaction and guide cell behaviour [19, 72]. Both techniques present pros and cons that have been well summarised in other reviews [73, 74] and have already been used to create CNS in vitro models [15, 75, 76], including models using iPSCs [71, 77,78,79]. A summary for comparison with 2D culture methods, advantages and disadvantages is shown in Table 1 and discussed further below.
The CNS microenvironment is dynamic and mechanical and chemical changes are continuously occurring due to cell-cell and cell-ECM interactions. These constant changes directly influence cell behaviour and the different combinations of chemical and mechanical cues are responsible for guiding correct neurodevelopment by controlling cell proliferation, differentiation, neural circuit integration, or can also be responsible for inducing neurodegeneration [12, 13, 34, 47, 58, 65, 80]. Taking into consideration the mutual interaction between cells and their microenvironment, there have been considerable research efforts to create more realistic, tissue-like in vitro models for a range of neuroscience applications. In scaffold-free models, spheroid structures can produce their own ECM, therefore replicating natural development of the cellular niche as it happens in vivo [19, 81]. Whereas in scaffold-based approaches the material provides the appropriate physical and/or chemical cues to allow cell adhesion, proliferation, differentiation and survival, as well as permitting cells to alter and interact with ECM components [15, 82, 83]. Permeability for nutrients and oxygen, permittivity for electrical conductance, cost-effectiveness, easy manipulation and reproducibility are other essential features for scaffold-based models that could also allow angiogenesis and not trigger immunological responses [15, 55, 82,83,84].
Hydrogels are good candidates for scaffold-based 3D CNS models. These cross-linked polymer networks, made from different natural (e.g. agarose, collagen, silk, chitosan, cellulose and Matrigel™) and synthetic (e.g. poly 2-hydroxyethyl methacrylate, polyethylene glycol) substrates, [57, 83, 85] are nutrient and oxygen permeable, mechanically similar to CNS tissue, hydrophilic, and show low cytotoxicity [15, 83, 85, 86]. They are also tuneable by changes in polymer mesh and functionalisation with different components such as adhesion proteins, enzymes and growth factors [83]. They have been widely used with NSCs [87,88,89,90] and show great potential due to their versatility as 3D scaffolds, providing important answers on how physical cues such as stiffness and topology can directly affect 3D cell culture [71, 87, 90,91,92]. A number of studies with hydrogels have shown that stiffness, topology, pore size and material composition can directly affect cell behaviour [71, 87, 90,91,92]. For example, work by Wang and colleagues [55] explored three different chitosan biomaterials (films, porous scaffolds and multimicrotubule conduits) to investigate the influence of topology on NSC fate, showing that cell proliferation and differentiation were directly influenced by different topologies and confirming the importance of biomaterial design in cell culture. Another study [88] showed that 3D interferon (IFN)-γ-immobilized hydrogels drive NSCs cultured in basic medium to a more neuronal committed differentiation. Their 3D model was superior to their 2D model, whereby with the highest IFN-γ surface concentration, approximately 73% of cells were βIII-tubulin-positive neurons in 3D in comparison to 60% in 2D [88, 89]. These examples show how several factors such as mechanical and chemical cues, must be taken into consideration to generate models that recapitulate CNS complexity and provide physiologically relevant results.
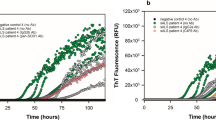
Hydrogels can also be integrated with other technologies to improve cell culture, for example in association with microfluidic technologies, providing platforms that present rudimental vascularization in vitro, and with organoid 3D technology, supporting tissue formation [93,94,95,96,97]. Organoids are 3D cultures that use the basic knowledge of scaffold-free techniques (i.e. letting cells self-organize and generate tissue structure) in combination with scaffold-based advantages (i.e. using a matrix to provide structure and external cues) to form organ-like structures [97]. Recent studies have shown that brain organoids, which can survive up to 10 months in bioreactors and can be obtained from patient-derived stem cells, have the potential to mimic mammalian neurodevelopmental mechanisms, CNS spatial organization and cell-ECM interactions [97,98,99]. The use of Matrigel™ is often essential for organoid culture, providing physicochemical cues for correct tissue organization [97, 100, 101], though some spheroid methods report alternative, simplified methods [102]. Organoids can mimic CNS complex organization, including development of various brain regions organized in independent domains, recapitulation of aspects of human cortical development, and exhibition of radial glial cells typical behaviour and morphology. Due to these advantages they are considered to show greater potential for CNS modelling when compared to other 2D and 3D protocols such as neural rosettes and neurospheres. So far, cerebral organoids have been used to study early brain development and neurodevelopmental disorders, as well as neurodegenerative diseases, and modelling different regions of the brain including cortex and midbrain [79, 97,98,99,100,101,102,103,104,105,106,107,108,109]. Raja et al. [110] showed an important advance in using organoid technology for late-stage disease modelling. They were able to recapitulate fAD phenotypes such as significantly raised levels of secreted Aβ, amyloid aggregation, hyperphosphorylated Tau protein and abnormal endosomes using organoids derived from hiPSCs. They also observed age-dependent increases in phenotypes and that amyloid pathology preceded Tau pathology. Similar success has been described with use of human neuroepithelial cells to generate organised, functionally active midbrain models suitable for modelling PD, as well as using patient-derived iPSC-based organoids to investigate PD pathology in and outside of the brain [108, 109]. The generation of brain organoids using iPSCs from patients that present late-onset diseases can therefore provide an invaluable tool to obtain further insight into pathology progression, as well as aid in developing new treatments. Another recent study building on spheroid/organoid technology generated subdomain-specific neural spheroids, representing the dorsal or ventral forebrain, and then assembled them together in culture in order to study migration of GABAerigc interneurons from the ventral to dorsal forebrain, including in cultures from patient-derived hiPSCs carrying mutations leading to Timothy Syndrome, a neurodevelopmental disorder with defects in such migration [111]. Such models can therefore not only represent disease-relevant regions of the brain (such as cortex for AD or midbrain for PD) but can also interrogate inter-regional interactions in the brain as well as interaction between cell types within a brain region.
hiPSCs as models for neurodegenerative diseases
In vitro models are valuable tools for studying CNS diseases. Although human CNS cells can be derived from ESCs, until recently this was not possible for specific individuals, except post-mortem or on occasion where tissue samples are surgically obtained [26]. Hence, the advent of hiPSCs provided an invaluable alternative, with the now relatively simple task of generating patient-derived iPSCs by reprogramming that can then be differentiated into specific neural subtypes [112]. Different 2D and 3D models using hiPSCs have since been developed to elucidate the pathological mechanisms underlying neurodegenerative diseases and provide insights for new therapeutic strategies. Below we briefly discuss existing models for specific disease that are summarised in Table 2.
Alzheimer’s disease
First described in 1906 by Alois Alzheimer, AD is a neurodegenerative disease characterized by the progressive loss of memory and cognition, language impairment, difficulties with problem-solving and eventual death. AD is the most common neurodegenerative disorder and the most prevalent type of dementia. In 2015 46.8 million people worldwide were living with dementia, which represented an economic burden of US$ 818 billion, and by 2030 it is expected that 74.7 million people will be affected, costing up to US$ 2 trillion worldwide [113]. AD’s aetiology is complex and still not well understood, but Aβ plaques and Tau neurofibrillary tangles (NT) are well known hallmarks of the disease. The amyloid hypothesis postulates that gradual and excessive accumulation of Aβ induces hyperphosphorylation of Tau and NT formation, leading to neuron structural destabilization and consequent death [114, 115]. However, despite the evidence supporting Aβ’s role in AD, drugs to reduce Aβ levels have thus far failed and are unable to reverse deficits in memory or to cease cognitive decline in human clinical trials [116,117,118]. As a consequence of these failures and the difficulty in finding a link between cognitive impairment and Aβ levels, research has started pursuing new targets (e.g. anti-Tau approaches). However, no drug has been successful in Phase III trials to date [118, 119]. Experts argue that multi-target approaches could be more fruitful than single-target drugs, increasing the likelihood that an effective AD treatment can be found [118, 120]. In parallel, it is important to develop tools that provide higher accuracy in AD diagnosis, and focus on earlier interventions to prevent irreversible CNS damage [118].
The most prevalent type of AD is sporadic AD (sAD), accounting for 90–95% of cases, with familial AD (fAD) making up the remaining 5–10% of AD cases. fAD has an autosomal dominant inheritance pattern with early onset (< 65 years) and mutations in genes that encode amyloid precursor protein (APP), presenilin 1 (PSEN1) or presenilin 2 (PSEN2), which increase Aβ production and accumulation, considered to be causes of fAD [121,122,123,124,125,126]. sAD is of late onset (> 65 years) and it is linked with both genetic and environmental factors, making it harder to study in vitro. AD genome-wide association studies have identified putative risk genes for sAD, however only the epsilon 4 allele of the apolipoprotein E gene (APOE ε4) has been confirmed as a risk factor [127,128,129,130].
Despite the knowledge gained so far, the underlying mechanisms that lead to AD are not well understood and there is no disease-modifying treatment. From this perspective, iPSCs-derived 2D and 3D models are important tools to investigate AD, increase knowledge of pathophysiological mechanisms and facilitate drug discovery.
Several studies using AD patient-derived iPSCs in 2D models have been reported [71, 77, 131,132,133,134]. For example, iPSCs-derived neurons from fAD patients with mutations in PSEN1 and PSEN2 show increased Aβ42 levels and are more susceptible to γ-secretase inhibitors, indicating the potential of this culture system for drug screening purposes [132]. Fibroblasts from affected and unaffected individuals carrying PSEN1 mutations were used to generate iPSCs and evaluate differences in Aβ42/Aβ40 production ratio in a 2D model. Aβ40 and Aβ42 are the most abundant Aβ species in the brain, representing ~ 90% and ~ 10%, respectively. Aβ42 is slightly longer than Aβ40 and is more hydrophobic and fibrillogenic, therefore being highly susceptible to form deposits in the brain. In this study comparisons were made between control fibroblasts and iPSC-derived neural progenitor cells (NPCs) and counterparts carrying a PSEN1 mutation. The results showed that both lineages with the mutation in PSEN1 (PSEN1 fibroblasts and PSEN1 NPCs) produced greater ratios of Aβ42 to Aβ40 than their control counterparts. In addition, PSEN1 NPCs showed a higher Aβ42/Aβ40 ratio compared to PSEN1 fibroblasts, indicating that the ratio may be increased by neuronal differentiation [133]. In a study using 2D cultures of iPSCs derived from an 82-year-old sAD patient, researchers were able to achieve some key AD features in vitro, including formation of abnormally phosphorylated Tau protein, increased expression of glycogen synthase kinase-3β (the protein kinase that phosphorylates Tau) and up-regulation of genes linked to oxidative stress response [134].
However, at the time this review was written, only three studies were identified using 3D technology and hiPSCs-derived cells to model AD [71, 77, 110]. One study used self-assembling peptide hydrogel seeded with hiPSC-derived neuroepithelial stem cells to show that 3D models were able to mimic AD’s in vivo like responses, such as aberrant translocation of activated P21-activated kinase and redistribution of the actin stabilizing protein drebrin, not observed in 2D counterparts. P21-activated kinase and drebrin are important for cytoskeleton dynamics and the former is considered to play a central role in mechanotransduction pathways and AD pathology [71]. The second study described an AD 3D human neuro-spheroid model in which iPSCs were obtained from patient’s blood and further differentiated into neurons and astrocytes. After differentiation, 3D neurons were less susceptibility to secretase inhibitors than 2D ones [77]. The third study, already described in this review, was performed by Raja et al. using a 3D organoid approach with iPSCs derived from patients with fAD [110]. These examples show how AD in vitro modelling is evolving, with ever more complex 3D-based approaches to model specific brain regions, their interaction and local microenvironments. In the future these are likely to provide greater insights into underlying disease mechanisms (including increasing interest in assessing the contribution of microglia) and provide better platforms for drug discovery.
Parkinson’s disease
PD is characterized by the loss of dopaminergic neurons in the substantia nigra pars compacta, compromising patient motor function. The most common symptoms include bradykinesia, rigidity, resting tremor and postural impairment [135,136,137]. The aetiology of PD remains unknown, but Lewy bodies, composed of aggregated α-synuclein found inside surviving dopaminergic neurons, are considered histopathological hallmarks [137, 138]. Sporadic PD represents 90–95% of cases, while Mendelian inheritance is linked to the remaining 5–10% of cases [137, 139]. Thus, similarly to AD, modelling PD is challenging, but patient-derived iPSCs provide an important tool to study different forms of PD [26, 139].
Thus far, several groups have been able to generate dopaminergic neurons from hiPSCs. In 2D models, Cooper and colleagues (2010) reported successful generation of ventral midbrain dopaminergic neurons from hiPSCs [140]. Degeneration of ventral midbrain neurons is linked to motor problems in PD and the possibility to study these cells in vitro is important for drug testing and screening purposes. Soldner and colleagues generated iPSCs from patients with idiopathic PD. Their protocol provided iPSCs free of reprogramming factors and more similar to embryo-derived stem cells; these were further differentiated into dopaminergic neurons [40]. These footprint-free iPSCs provide a more suitable tool for disease modelling and clinical use since the presence of residual transgenes can alter gene expression, differentiation potential and cause genetic instability, leading to malignant transformation [40, 141]. Hargus and colleagues (2010) were able to differentiate patient-derived iPSCs into dopaminergic neurons in a 2D model and further transplant cells into rodent brain, showing good survival rates and behavioural improvement of the treated rats [142].
In contrast to 2D models, three studies using 3D models has been reported [78, 108, 109]. In a 3D strategy using Matrigel™ with phase-guided microfluidics bioreactors, Moreno and colleagues (2015) were able to differentiate hiPSCs into dopaminergic neurons. After 30 days of differentiation, immunocytochemistry showed that 78–90% of cells were neurons, of which 11–19% were dopaminergic neurons. Spontaneous electrophysiological activity with propagation of action potential along neurites was also reported. The authors claim that their model is robust, cost efficient and shows biological fidelity for further use in PD modelling and drug discovery [78]. In 2017, two organoid approaches have been reported showing an improvement in PD modelling in vitro using hiPSCs. Son et al. were able to generate neural organoids from patient-derived iPSCs. Their cells carried an LRRK2 mutation and were differentiated into 3D structures and further evaluated for gene expression. Results showed that LRRK2-mutated cells had alterations in pathways linked to synaptic transmission [108]. Monzel et al. (2017) were able to generate midbrain-specific cultures from neuroepithelial stem cells. After neuronal differentiation they were able to obtain dopaminergic neurons, astrocytes and oligodendrocytes. Neurons were able to secrete dopamine, form spatially patterned and organized networks, and show synaptic connections and spontaneous neuronal activity [109]. These studies show how more advanced approaches such as 3D cultures are able to provide more complex results for disease modelling, for example, allowing patterned cell organization and network formation, better reflecting the in vivo tissue. As such, they may also be well placed to better model the movement of α-synuclein between cells, a mechanism that may contribute to spread of disease pathology [143].
Huntington’s disease
HD is an inherited neurodegenerative disorder caused by an expansion of CAG repeats in the Huntingtin (HTT) gene, leading to an HTT protein with a long polyglutamine expansion that is consequently more susceptible to aggregate and accumulate. The threshold for HD is 36 CAG repeats in HTT, and the number of repeats is inversely correlated with age onset of disease [144]. Cortical and striatal neurons are predominantly affected and patients usually manifest progressive motor impairment, decline in cognition, and psychiatric problems [144,145,146,147,148]. Even though the genetic alteration that causes HD has already been identified, no efficient treatment exists and knowledge regarding the exact pathological mechanisms remains incomplete. Thus, relevant human in vitro models could further contribute to understanding HD pathophysiology.
So far, only a few studies using iPSCs obtained from patients carrying HD-causing mutations can be found in the literature, all of them in 2D cultures and none in 3D models [27, 145,146,147, 149, 150]. 2D studies so far present interesting findings highlighted here. For example, one study performed by An and colleagues (2012), successfully corrected the mutation in HTT using genetic manipulation techniques. The study was performed using patient-derived iPSCs cultured on Matrigel™ coated plates, and after replacing the mutated repeat with a normal one using homologous recombination, pathogenic signalling pathways were normalized and disease phenotypes such as susceptibility to cell death, were reversed [145]. This capability to reverse HD phenotypes can be an advance in disease modelling towards a platform for investigation of disease pathway mechanisms and drug screening. It would also allow the comparison between corrected and disease lineages, and perhaps in the future could be considered for cell replacement therapy and repopulation of the striatum in vivo. Another group also obtained interesting results using iPSCs by linking phenotypic alterations in astrocytes with HD [147]. Juopperi and colleagues (2012) used iPSCs derived from a father and a daughter with 50 and 109 CAG repeats, respectively, cultured in a 2D model to investigate astrocyte dysfunction in HD. Interestingly, when HD-iPSCs were differentiated into neurons a normal phenotype was observed, whereas iPSC-derived astrocytes showed increased cytoplasmic vacuolation, an alteration observed in blood lymphocytes from individuals with HD. The authors suggest that this could be a new feature for HD investigation, and that perhaps cellular vacuolation may be a disease-associated finding that could be used as a biomarker [147]. Given these findings and those discussed elsewhere in this review, future developments in hiPSC-based HD modelling able to generate 3D cultures to better investigate interactions between neurons and glia of the cortex and striatum (e.g. using spheroids and/or microfluidics-based technologies [151]) will no doubt offer further insights into the disease.
Amyotrophic lateral sclerosis
ALS is a neurodegenerative disease characterized by loss of upper and lower motor neurons, causing gradual loss of motor functions, muscular atrophy, paralysis and death [152,153,154]. Most patients have a life expectancy of 3–5 years after diagnosis and die from respiratory failure due to bulbar impairment and loss of diaphragm control [154,155,156]. ALS aetiology remains unknown and most cases are sporadic, occurring due to complex multifactorial interactions between environmental factors and genes. The familial form (fALS) represents about 10% of the cases and, so far, mutations have been identified in genes coding for Superoxide dismutase 1 (SOD1 gene), Ubiquilin-2 (UBQLN2 gene), C9ORF72 (C9ORF72 gene), TAR DNA-Binding Protein 43 (TDP-43, encoded by TARDBP) and Fused in sarcoma (FUS gene), considered key causative factors in fALS [154, 156, 157]. Mutations in C9ORF72, SOD1, TARDP and FUS are also present in ~ 1–7% of sporadic ALS cases [158].
Regarding the use of patient-derived iPSCs to model ALS, the successful generation of iPSC-derived motor neurons from ALS patients has been reported [28]. Several other studies have also shown that ALS-related pathological mechanisms could be reproduced in vitro, including cell vulnerability to mutations [159,160,161,162], neurofilament aggregation and neurite degeneration [163], TDP-43 proteinopathy [159, 160, 164], C9ORF72 repeat toxicity [165, 166], and dysregulation of neuronal synaptic activity [167, 168]. Additional studies have also been able to show how astrocytes are also involved in ALS and degenerate during disease progression, losing their capacity to support neurons [169, 170]. All of these studies were performed in 2D and have provided important insights in ALS comprehension; however, no study using 3D models could be found. Future 3D approaches have the capacity to further improve models and bring new insight into ALS pathophysiology. For example, as briefly mentioned above, 2D hiPSC-derived models of ALS have also shown the contribution of astrocytes to non-cell autonomous effects on motor neurons [169, 170]. However, it is likely scaffold and non-scaffold-based 3D models will present another step forward in permitting more appropriate astrocyte morphology [171], maturity [104] and recapitulation of complex interactions that occur between astrocytes and neurons in brain networks such as those recently described in 3D ‘asteroids’ [172].
Limitations of iPSC-derived models for studying neurodegenerative diseases
Although patient-derived hiPSC in vitro models can be a powerful platform for disease modelling and drug discovery, there are some concerns regarding the lack of standardized protocols, the consequences of reprogramming protocols, and the possibility of epigenetic memory interference leading to great variability between clones and lineages and consequent doubts about reliability [40, 141, 173,174,175]. However, there are strategies that may help to overcome these issues that include: obtaining cells from sources that contain less accumulated genetic mutations (i.e. younger tissues instead of aged ones); using safer reprogramming protocols (i.e. those that do not integrate into the iPSC genome or retain transgene sequences), detecting and monitoring variations in iPSC lineages, executing extensive characterization of cell lines, and standardizing protocols between laboratories [173].
Another relevant limitation for a number of 3D culture models, including organoids, is the lack of vascularization and restricted circulation of nutrients/extracellular factors. In vivo, blood vessels have an essential role in gaseous exchange, nutrient supply and waste removal. In vitro, their absence can be limiting, for example causing cell death in the core of larger spheroids or organoids such as shown in hiPSC-derived cerebral organoids [98, 100]. Future developments will need to overcome such limitations, with examples of possible strategies including combining mesenchymal cells and endothelial cells with tissue-specific cells to promote vascularisation [176] or use of microfluidics technology to facilitate circulation of nutrients through the 3D culture as has been shown to be effective for culture of thick brain slices [177].
Absence of microglia in in vitro models has also been considered an important limitation. Microglia are resident macrophages in the CNS responsible for adequate immune responses to damaged or diseased brain. Activated microglia have been linked to AD, PD and ALS probably due to accumulation of abnormal proteins and neurodegeneration [178]. For instance, microglia are considered to be a key player in Aβ clearance [17]. Nowadays, highly efficient iPSCs-derived microglia models are available in the literature. For example, in a study by Haenseler et al. (2017), iPSC-derived microglia were co-cultured with iPSC-derived cortical neurons. The results showed that microglia were phagocytically competent, able to downregulate pathogen-response pathways, could upregulate homeostatic pathways, could promote anti-inflammatory responses and were able to express key human microglia-specific markers and neurodegenerative disease-relevant genes [179]. This means that it is now possible to obtain and use laboratory-made or commercially available microglia and incorporate these into 3D neurodegenerative disease models, such as for AD [36].
Undoubtedly, 3D cultures have the potential to become a significant tool for disease modelling, however, techniques to evaluate these cultures must be further improved. Examples of limitations include low optical transparency during imaging techniques due to culture thickness or due to scaffold limitations (e.g. silk fibroin films treated with organic solvents) [15, 16, 180], potential for decreased reproducibility due to batch-to-batch variation of biological-based scaffold materials [181, 182] such as Matrigel [183] and increased complexity and heterogeneity of models, difficulties for use with specific techniques such as patch clamp, due to low optical clarity or difficulty in penetration of the glass micropipette through the scaffold [15], and the necessity for expensive and highly-specialized equipment to maintain cells in cultures (e.g. bioreactors) [15, 16, 53]. A final limitation in modelling neurodegenerative disorders is not specific to 3D cultures but concerns PSC-derived models more generally and relates to the in vivo ‘age’ to which they are equivalent. Many neurodegenerative conditions such as AD, PD and ALS are age-dependent, often with late adult onset and late-stage pathologies. However, in vitro models derived from hiPSCs first often require long-term culture to obtain more mature cell types or phenotypes, an example of which was described by Sposito and colleagues in a model of frontotemporal dementia (FTD) where an extended, 365-day culture of hiPSC-derived cortical neurons was required to obtain expression of the adult isoform of Tau (0N4R, [184]). Interestingly, a human NSC 3D culture model of AD showed higher expression of adult Tau compared to 2D [18]. Protocols have been developed for more rapid differentiation of hiPSCs into mature CNS cells, including forced expression of key factors, such as the generation of neurons from hiPSCs in under 2 weeks following overexpression of neurogenin 2 [185]. However, to model specific aspects of late-onset diseases, further ageing processes that occur after maturation may also be necessary (for a detailed review see [186]). As such, a current focus in this field is in developing methods to ‘age’ cultures in order to obtain appropriate phenotypes, examples of which include exposing cells to toxins (such as reactive oxygen species) to simulate cellular changes induced by stress [187] or exploiting knowledge from premature ageing syndromes, such as overexpression of progerin, shown to lead to more late-onset phenotypes in an hiPSC-derived model of PD [188].
Notwithstanding the limitations described above, continued efforts from researchers across a range of disciplines to overcome these challenges will no doubt see further advances in hiPSC-derived 3D culture technologies that in turn make significant contributions to future neurodegenerative disease research.
Perspectives
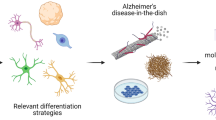
The use of stem cells, in particular iPSC-derived cells, to study neurodegenerative diseases has the potential to reduce (and possibly replace) the use of animals, and will continue to provide important insights into disease mechanisms, and to accelerate the discovery of more effective treatments. Furthermore, patient-derived iPSCs could be used for personalised medicine, for example allowing physicians to check the efficacy of a specific drug in vitro before administering it to the patient, therefore providing a more accurate and tailored treatment (Fig. 1). There are also new technologies being considered to improve cell culture, such as microfluidic platforms. This technology provides systems of tens to hundreds of micron dimensions that can be integrated with 2D and 3D cultures and offers the possibility to work with high density or single cell cultures, temporal and spatial control, channel and valves integration, fluid flow and integration with systems such as multi-electrode arrays for electrophysiological studies [93,94,95, 189, 190]. In fact, microfluidics have already been used in PD [78] and AD [189, 191] modelling, showing promising results regarding disease pathophysiology. In one study, a microfluidic chamber was developed to culture AD transgenic mouse neurons, allowing fluidic isolation due to the presence of a solid barrier between neuronal axons and soma. Molecules (e.g. drugs, Aβ oligomers) can then be selectively applied to axons or the soma, allowing recapitulation of in vivo characteristics, whereby specific neuronal components are exposed to different microenvironments. Using this model a link was established between BDNF retrograde signalling and AD, in which Aβ oligomers induced impaired BDNF transport and synaptic deficits, affecting long-term potentiation (LTP), a key mechanism for memory formation and learning [191]. In another study designed to monitor AD progression, cortical neurons from transgenic mice were cultured in a compartmentalized 2D model, separating soma from neurites. One chamber was seeded with okadaic acid induced-diseased cells and the other contained healthy cells, revealing important insights into AD pathophysiology in how disease cells can affect healthy neighbour cells and the disease progression patterns [189]. A more complex form of microfluidics with cell culture is the organ-on-a-chip [93]. These are being considered as potential tools for further studies on human physiology and disease, providing the opportunity to form circuits that create a fluid flow between different ‘miniorgans’. Although further in-depth review of this area is outside the scope of this review, it is important to note that for modelling the brain and associated disorders, there are already examples of how coupling 3D culture with microfluidics can provide benefits over 2D or use of 3D methods alone. These include co-culture of different cell types to model interaction between specific brain compartments/components (such as the neurovascular niche [192]) and providing constant flow of fluids that can improve 3D spheroid growth and disease phenotypes, as has been shown for a ‘brain-on-a-chip’ model for AD [193]. Perhaps in a not so distant future, models that include patient-derived cells for personalized medicine will provide systems in which blood-brain barrier culture can be connected with other brain and liver cultures, mimicking blood flow between organs and as an approach to test drugs, providing key pharmacokinetics and pharmacodynamics information.

Human induced pluripotent stem cells (hiPSCs) in neurodegenerative diseases modelling. Patient-derived somatic cells (SCs) can be genetically reprogrammed to generate iPSCs. High-tech systems can be used to culture and differentiate iPSCs into brain cells such as oligodendrocytes, astrocytes and different neuronal populations (NPs), providing the possibility to accurately study neurodegenerative diseases in vitro and to obtain essential information about disease phenotype and pathology insights. This strategy provides the possibility of testing drugs in vitro and identifying new therapies for incurable disorders such as Alzheimer’s (AD), Parkinson’s (PD), Huntington’s (HD) diseases and amyotrophic lateral sclerosis (ALS). (Illustrations obtained from https://smart.servier.com/)
Conclusions
Even though 3D cultures using patient-derived iPSCs hold great promise for neuroscience research as a tool for AD, PD, HD, and ALS modelling, at the time this review was written, only a few studies could be found using 3D patient-derived cultures. All 3D models described in this review were able to recapitulate key disease events, and some displayed active neuronal networks that were organized in patterns, similar to in vivo tissue. This supports the idea that this technology can provide additional advantages above 2D counterparts. However, to improve 3D culture and recreate reliable models, we still need better understanding about cell-ECM and cell-cell interaction, incorporation of microglia into models (co-culture of neurons and glia), standardized protocols for iPSCs reprogramming to decrease variability between clones, and advanced 3D models that are cost-effective and easy to work with at the same time.
Abbreviations
- 2D:
-
Two dimensional
- 3D:
-
Three dimensional
- AD:
-
Alzheimer’s disease
- ALS:
-
Lateral sclerosis
- APOE ε4:
-
Epsilon 4 allele of apolipoprotein E
- APP:
-
Amyloid precursor protein
- Aβ:
-
Amyloid beta
- CNS:
-
Central nervous system
- ECM:
-
Extracellular matrix
- ESCs:
-
Embryonic stem cells
- fAD:
-
Familial alzheimer’s disease
- fALS:
-
Familial amyotrophic lateral sclerosis
- FUS:
-
Fused in Sarcoma
- HD:
-
Huntington’s disease
- hiPSCs:
-
Human induced pluripotent stem cells
- HTT:
-
Huntingtin
- IFN:
-
Interferon
- NPCs:
-
Neural progenitor cells
- NT:
-
Neurofibrillary tangles
- PD:
-
Parkinson’s disease
- PSCs:
-
Pluripotent stem cells
- PSEN 1:
-
Presenilin 1
- PSEN 2:
-
Presenilin 2
- sAD:
-
Sporadic alzheimer’s disease
- SOD1:
-
Superoxide dismutase 1
- TARDBP:
-
TAR DNA-binding protein
- TDP-34:
-
Transactive response DNA vinding protein 43
- UBQLN2:
-
Ubiquilin 2
References
Golde TE, Borchelt DR, Giasson BI, Lewis J. Thinking laterally about neurodegenerative proteinopathies. J Clin Invest. 2013;123(5):1847–55.
Armstrong RA, Lantos PL, Cairns NJ. Overlap between neurodegenerative disorders. Neuropathology. 2005;25(2):111–24.
Scotter EL, Chen HJ, Shaw CE. TDP-43 Proteinopathy and ALS: insights into disease mechanisms and therapeutic targets. Neurotherapeutics. 2015;12(2):352–63.
Hay M, Thomas DW, Craighead JL, Economides C, Rosenthal J. Clinical development success rates for investigational drugs. Nat Biotechnol. 2014;32(1):40–51.
Cummings JL, Morstorf T, Zhong K. Alzheimer’s disease drug-development pipeline: few candidates, frequent failures. Alzheimers Res Ther. 2014;6(4):37.
Takahashi K, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell. 2006;126(4):663–76.
Takahashi K, Tanabe K, Ohnuki M, Narita M, Ichisaka T, Tomoda K, et al. Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell. 2007;131(5):861–72.
Gunaseeli I, Doss MX, Antzelevitch C, Hescheler J, Sachinidis A. Induced pluripotent stem cells as a model for accelerated patient- and disease-specific drug discovery. Curr Med Chem. 2010;17(8):759–66.
Juopperi TA, Song H, Ming GL. Modeling neurological diseases using patient-derived induced pluripotent stem cells. Future Neurol. 2011;6(3):363–73.
Grskovic M, Javaherian A, Strulovici B, Daley GQ. Induced pluripotent stem cells--opportunities for disease modelling and drug discovery. Nat Rev Drug Discov. 2011;10(12):915–29.
Maldonado-Soto AR, Oakley DH, Wichterle H, Stein J, Doetsch FK, Henderson CE. Stem cells in the nervous system. Am J Phys Med Rehabil. 2014;93(11 Suppl 3):S132–44.
Preston M, Sherman LS. Neural stem cell niches: roles for the hyaluronan-based extracellular matrix. Front Biosci. 2011;3:1165–79.
Keung AJ, Kumar S, Schaffer DV. Presentation counts: microenvironmental regulation of stem cells by biophysical and material cues. Annu Rev Cell Dev Biol. 2010;26:533–56.
Blain M, Miron VE, Lambert C, Darlington PJ, Cui Q-L, Saikali P, et al. Isolation and culture of primary human CNS neural cells. In: Doering LC, editor. Protocols for neural cell culture. Fourth ed. Totowa: Humana Press; 2010. p. 87–104.
Hopkins AM, DeSimone E, Chwalek K, Kaplan DL. 3D in vitro modeling of the central nervous system. Prog Neurobiol. 2015;125:1–25.
D'Avanzo C, Aronson J, Kim YH, Choi SH, Tanzi RE, Kim DY. Alzheimer’s in 3D culture: challenges and perspectives. BioEssays. 2015;37(10):1139–48.
Kim YH, Choi SH, D'Avanzo C, Hebisch M, Sliwinski C, Bylykbashi E, et al. A 3D human neural cell culture system for modeling Alzheimer’s disease. Nat Protoc. 2015;10(7):985–1006.
Choi SH, Kim YH, Hebisch M, Sliwinski C, Lee S, D'Avanzo C, et al. A three-dimensional human neural cell culture model of Alzheimer’s disease. Nature. 2014;515(7526):274–8.
Edmondson R, Broglie JJ, Adcock AF, Yang L. Three-dimensional cell culture systems and their applications in drug discovery and cell-based biosensors. Assay Drug Dev Technol. 2014;12(4):207–18.
Antoni D, Burckel H, Josset E, Noel G. Three-dimensional cell culture: a breakthrough in vivo. Int J Mol Sci. 2015;16(3):5517–27.
Yap MS, Nathan KR, Yeo Y, Lim LW, Poh CL, Richards M, et al. Neural differentiation of human pluripotent stem cells for nontherapeutic applications: toxicology, pharmacology, and in vitro disease modeling. Stem Cells Int. 2015;2015:105172.
Yan Y, Shin S, Jha BS, Liu Q, Sheng J, Li F, et al. Efficient and rapid derivation of primitive neural stem cells and generation of brain subtype neurons from human pluripotent stem cells. Stem Cells Transl Med. 2013;2(11):862–70.
Li Y, Liu M, Yan Y, Yang ST. Neural differentiation from pluripotent stem cells: the role of natural and synthetic extracellular matrix. World J Stem Cells. 2014;6(1):11–23.
Verfaillie C. Pluripotent stem cells. Transfus Clin Biol. 2009;16(2):65–9.
Avior Y, Sagi I, Benvenisty N. Pluripotent stem cells in disease modelling and drug discovery. Nat Rev Mol Cell Biol. 2016;17(3):170–82.
Byers B, Lee HL, Reijo PR. Modeling Parkinson’s disease using induced pluripotent stem cells. Curr Neurol Neurosci Rep. 2012;12(3):237–42.
Camnasio S, Delli Carri A, Lombardo A, Grad I, Mariotti C, Castucci A, et al. The first reported generation of several induced pluripotent stem cell lines from homozygous and heterozygous Huntington's disease patients demonstrates mutation related enhanced lysosomal activity. Neurobiol Dis. 2012;46(1):41–51.
Dimos JT, Rodolfa KT, Niakan KK, Weisenthal LM, Mitsumoto H, Chung W, et al. Induced pluripotent stem cells generated from patients with ALS can be differentiated into motor neurons. Science. 2008;321(5893):1218–21.
Wang A, Tang Z, Park IH, Zhu Y, Patel S, Daley GQ, et al. Induced pluripotent stem cells for neural tissue engineering. Biomaterials. 2011;32(22):5023–32.
Jackman CP, Shadrin IY, Carlson AL, Bursac N. Human cardiac tissue engineering: from pluripotent stem cells to heart repair. Curr Opin Chem Eng. 2015;7:57–64.
Tabar V, Studer L. Pluripotent stem cells in regenerative medicine: challenges and recent progress. Nat Rev Genet. 2014;15(2):82–92.
Malik N, Rao MS. A review of the methods for human iPSC derivation. Methods Mol Biol. 2013;997:23–33.
Jiang Z, Han Y, Cao X. Induced pluripotent stem cell (iPSCs) and their application in immunotherapy. Cell Mol Immunol. 2014;11(1):17–24.
Dolmetsch R, Geschwind DH. The human brain in a dish: the promise of iPSC-derived neurons. Cell. 2011;145(6):831–4.
Phillips MD, Kuznetsov SA, Cherman N, Park K, Chen KG, McClendon BN, et al. Directed differentiation of human induced pluripotent stem cells toward bone and cartilage: in vitro versus in vivo assays. Stem Cells Transl Med. 2014;3(7):867–78.
Abud EM, Ramirez RN, Martinez ES, Healy LM, Nguyen CHH, Newman SA, et al. iPSC-derived human microglia-like cells to study neurological diseases. Neuron. 2017;94(2):278–93. e9.
Kriegstein A, Alvarez-Buylla A. The glial nature of embryonic and adult neural stem cells. Annu Rev Neurosci. 2009;32:149–84.
Mora-Bermudez F, Huttner WB. Novel insights into mammalian embryonic neural stem cell division: focus on microtubules. Mol Biol Cell. 2015;26(24):4302–6.
Shi Y, Kirwan P, Smith J, Robinson HP, Livesey FJ. Human cerebral cortex development from pluripotent stem cells to functional excitatory synapses. Nat Neurosci. 2012;15(3):477–86. S1.
Soldner F, Hockemeyer D, Beard C, Gao Q, Bell GW, Cook EG, et al. Parkinson's disease patient-derived induced pluripotent stem cells free of viral reprogramming factors. Cell. 2009;136(5):964–77.
Emdad L, D'Souza SL, Kothari HP, Qadeer ZA, Germano IM. Efficient differentiation of human embryonic and induced pluripotent stem cells into functional astrocytes. Stem Cells Dev. 2012;21(3):404–10.
Douvaras P, Wang J, Zimmer M, Hanchuk S, O'Bara MA, Sadiq S, et al. Efficient generation of myelinating oligodendrocytes from primary progressive multiple sclerosis patients by induced pluripotent stem cells. Stem Cell Rep. 2014;3(2):250–9.
Gorris R, Fischer J, Erwes KL, Kesavan J, Peterson DA, Alexander M, et al. Pluripotent stem cell-derived radial glia-like cells as stable intermediate for efficient generation of human oligodendrocytes. Glia. 2015;63(12):2152–67.
Ghaffari LT, Starr A, Nelson AT, Sattler R. Representing diversity in the dish: using patient-derived in vitro models to recreate the heterogeneity of neurological disease. Front Neurosci. 2018;12:56.
Johansson CB, Momma S, Clarke DL, Risling M, Lendahl U, Frisen J. Identification of a neural stem cell in the adult mammalian central nervous system. Cell. 1999;96(1):25–34.
Eriksson PS, Perfilieva E, Bjork-Eriksson T, Alborn AM, Nordborg C, Peterson DA, et al. Neurogenesis in the adult human hippocampus. Nat Med. 1998;4(11):1313–7.
Decimo I, Bifari F, Krampera M, Fumagalli G. Neural stem cell niches in health and diseases. Curr Pharm Des. 2012;18(13):1755–83.
Licht T, Keshet E. The vascular niche in adult neurogenesis. Mech Dev. 2015;138(Pt 1):56–62.
Bond AM, Ming GL, Song H. Adult mammalian neural stem cells and neurogenesis: five decades later. Cell Stem Cell. 2015;17(4):385–95.
Lim DA, Alvarez-Buylla A. Adult neural stem cells stake their ground. Trends Neurosci. 2014;37(10):563–71.
McGonigle P. Animal models of CNS disorders. Biochem Pharmacol. 2014;87(1):140–9.
Perel P, Roberts I, Sena E, Wheble P, Briscoe C, Sandercock P, et al. Comparison of treatment effects between animal experiments and clinical trials: systematic review. BMJ. 2007;334(7586):197.
Elliott NT, Yuan F. A review of three-dimensional in vitro tissue models for drug discovery and transport studies. J Pharm Sci. 2011;100(1):59–74.
Harrison RG, Greenman MJ, Mall FP, Jackson CM. Observations of the living developing nerve fiber. Anat Rec. 1907;1(5):116–28.
Morrison B, Cullen DK, LaPlaca M. Vitro models for biomechanical studies of neural tissues. In: Bilston LE, editor. Neural tissue biomechanics. Berlin: Springer Berlin Heidelberg; 2011. p. 247–85.
Hazel T, Muller T. Culture of neuroepithelial stem cells. Curr Protoc Neurosci. 2001;3:1–3.
Hopkins AM, De Laporte L, Tortelli F, Spedden E, Staii C, Atherton TJ, et al. Silk hydrogels as soft substrates for neural tissue engineering. Adv Funct Mater. 2013;23(41):5140–9.
Flanagan LA, Rebaza LM, Derzic S, Schwartz PH, Monuki ES. Regulation of human neural precursor cells by laminin and integrins. J Neurosci Res. 2006;83(5):845–56.
Ge H, Tan L, Wu P, Yin Y, Liu X, Meng H, et al. Poly-L-ornithine promotes preferred differentiation of neural stem/progenitor cells via ERK signalling pathway. Sci Rep. 2015;5:15535.
Buzanska L, Ruiz A, Zychowicz M, Rauscher H, Ceriotti L, Rossi F, et al. Patterned growth and differentiation of human cord blood-derived neural stem cells on bio-functionalized surfaces. Acta Neurobiol Exp (Wars). 2009;69(1):24–36.
Mazia D, Schatten G, Sale W. Adhesion of cells to surfaces coated with polylysine. Applications to electron microscopy. J Cell Biol. 1975;66(1):198–200.
Dityatev A, Schachner M. Extracellular matrix molecules and synaptic plasticity. Nat Rev Neurosci. 2003;4(6):456–68.
Hsia HC, Schwarzbauer JE. Meet the tenascins: multifunctional and mysterious. J Biol Chem. 2005;280(29):26641–4.
Singh P, Carraher C, Schwarzbauer JE. Assembly of fibronectin extracellular matrix. Annu Rev Cell Dev Biol. 2010;26:397–419.
Singh P, Schwarzbauer JE. Fibronectin and stem cell differentiation - lessons from chondrogenesis. J Cell Sci. 2012;125(Pt 16):3703–12.
Jakovcevski I, Miljkovic D, Schachner M, Andjus PR. Tenascins and inflammation in disorders of the nervous system. Amino Acids. 2013;44(4):1115–27.
Anlar B, Gunel-Ozcan A. Tenascin-R: role in the central nervous system. Int J Biochem Cell Biol. 2012;44(9):1385–9.
Pontes Soares C, Midlej V, de Oliveira ME, Benchimol M, Costa ML, Mermelstein C. 2D and 3D-organized cardiac cells shows differences in cellular morphology, adhesion junctions, presence of myofibrils and protein expression. PLoS One. 2012;7(5):e38147.
Xu T, Molnar P, Gregory C, Das M, Boland T, Hickman JJ. Electrophysiological characterization of embryonic hippocampal neurons cultured in a 3D collagen hydrogel. Biomaterials. 2009;30(26):4377–83.
Brannvall K, Bergman K, Wallenquist U, Svahn S, Bowden T, Hilborn J, et al. Enhanced neuronal differentiation in a three-dimensional collagen-hyaluronan matrix. J Neurosci Res. 2007;85(10):2138–46.
Zhang D, Pekkanen-Mattila M, Shahsavani M, Falk A, Teixeira AI, Herland A. A 3D Alzheimer’s disease culture model and the induction of P21-activated kinase mediated sensing in iPSC derived neurons. Biomaterials. 2014;35(5):1420–8.
Knight E, Przyborski S. Advances in 3D cell culture technologies enabling tissue-like structures to be created in vitro. J Anat. 2015;227(6):746–56.
Breslin S, O'Driscoll L. Three-dimensional cell culture: the missing link in drug discovery. Drug Discov Today. 2013;18(5–6):240–9.
Rimann M, Graf-Hausner U. Synthetic 3D multicellular systems for drug development. Curr Opin Biotechnol. 2012;23(5):803–9.
Ahn M, Kalume F, Pitstick R, Oehler A, Carlson G, DeArmond SJ. Brain aggregates: an effective in vitro cell culture system modeling neurodegenerative diseases. J Neuropathol Exp Neurol. 2016;75(3):256–62.
Dingle YT, Boutin ME, Chirila AM, Livi LL, Labriola NR, Jakubek LM, et al. Three-dimensional neural spheroid culture: an in vitro model for cortical studies. Tissue Eng Part C Methods. 2015;21(12):1274–83.
Lee HK, Velazquez Sanchez C, Chen M, Morin PJ, Wells JM, Hanlon EB, et al. Three dimensional human neuro-spheroid model of Alzheimer’s disease based on differentiated induced pluripotent stem cells. PLoS One. 2016;11(9):e0163072.
Moreno EL, Hachi S, Hemmer K, Trietsch SJ, Baumuratov AS, Hankemeier T, et al. Differentiation of neuroepithelial stem cells into functional dopaminergic neurons in 3D microfluidic cell culture. Lab Chip. 2015;15(11):2419–28.
Brawner AT, Xu R, Liu D, Jiang P. Generating CNS organoids from human induced pluripotent stem cells for modeling neurological disorders. Int J Physiol Pathophysiol Pharmacol. 2017;9(3):101–11.
Gattazzo F, Urciuolo A, Bonaldo P. Extracellular matrix: a dynamic microenvironment for stem cell niche. Biochim Biophys Acta. 2014;1840(8):2506–19.
Fennema E, Rivron N, Rouwkema J, van Blitterswijk C, de Boer J. Spheroid culture as a tool for creating 3D complex tissues. Trends Biotechnol. 2013;31(2):108–15.
O'Brien FJ. Biomaterials & amp; scaffolds for tissue engineering. Mater Today. 2011;14(3):88–95.
El-Sherbiny IM, Yacoub MH. Hydrogel scaffolds for tissue engineering: progress and challenges. Glob Cardiol Sci Pract. 2013;2013(3):316–42.
Balint R, Cassidy NJ, Cartmell SH. Conductive polymers: towards a smart biomaterial for tissue engineering. Acta Biomater. 2014;10(6):2341–53.
Frampton JP, Hynd MR, Shuler ML, Shain W. Fabrication and optimization of alginate hydrogel constructs for use in 3D neural cell culture. Biomed Mater. 2011;6(1):015002.
Nisbet DR, Crompton KE, Horne MK, Finkelstein DI, Forsythe JS. Neural tissue engineering of the CNS using hydrogels. J Biomed Mater Res B Appl Biomater. 2008;87(1):251–63.
Wang G, Ao Q, Gong K, Wang A, Zheng L, Gong Y, et al. The effect of topology of chitosan biomaterials on the differentiation and proliferation of neural stem cells. Acta Biomater. 2010;6(9):3630–9.
Leipzig ND, Wylie RG, Kim H, Shoichet MS. Differentiation of neural stem cells in three-dimensional growth factor-immobilized chitosan hydrogel scaffolds. Biomaterials. 2011;32(1):57–64.
Leipzig ND, Xu C, Zahir T, Shoichet MS. Functional immobilization of interferon-gamma induces neuronal differentiation of neural stem cells. J Biomed Mater Res A. 2010;93(2):625–33.
Li H, Wijekoon A, Leipzig ND. 3D differentiation of neural stem cells in macroporous photopolymerizable hydrogel scaffolds. PLoS One. 2012;7(11):e48824.
O'Brien FJ, Harley BA, Yannas IV, Gibson LJ. The effect of pore size on cell adhesion in collagen-GAG scaffolds. Biomaterials. 2005;26(4):433–41.
Banerjee A, Arha M, Choudhary S, Ashton RS, Bhatia SR, Schaffer DV, et al. The influence of hydrogel modulus on the proliferation and differentiation of encapsulated neural stem cells. Biomaterials. 2009;30(27):4695–9.
Bhatia SN, Ingber DE. Microfluidic organs-on-chips. Nat Biotech. 2014;32(8):760–72.
Inamdar NK, Borenstein JT. Microfluidic cell culture models for tissue engineering. Curr Opin Biotechnol. 2011;22(5):681–9.
Meyvantsson I, Beebe DJ. Cell culture models in microfluidic systems. Annu Rev Anal Chem (Palo Alto, Calif). 2008;1:423–49.
Huang GY, Zhou LH, Zhang QC, Chen YM, Sun W, Xu F, et al. Microfluidic hydrogels for tissue engineering. Biofabrication. 2011;3(1):012001.
Yin X, Mead BE, Safaee H, Langer R, Karp JM, Levy O. Engineering stem cell organoids. Cell Stem Cell. 2016;18(1):25–38.
Lancaster MA, Renner M, Martin CA, Wenzel D, Bicknell LS, Hurles ME, et al. Cerebral organoids model human brain development and microcephaly. Nature. 2013;501(7467):373–9.
Huch M, Koo BK. Modeling mouse and human development using organoid cultures. Development. 2015;142(18):3113–25.
Lancaster MA, Knoblich JA. Generation of cerebral organoids from human pluripotent stem cells. Nat Protoc. 2014;9(10):2329–40.
Garcez PP, Loiola EC, Madeiro da Costa R, Higa LM, Trindade P, Delvecchio R, et al. Zika virus impairs growth in human neurospheres and brain organoids. Science. 2016;352(6287):816–8.
Pasca AM, Sloan SA, Clarke LE, Tian Y, Makinson CD, Huber N, et al. Functional cortical neurons and astrocytes from human pluripotent stem cells in 3D culture. Nat Methods. 2015;12(7):671–8.
Qian X, Nguyen HN, Jacob F, Song H, Ming GL. Using brain organoids to understand Zika virus-induced microcephaly. Development. 2017;144(6):952–7.
Sloan SA, Darmanis S, Huber N, Khan TA, Birey F, Caneda C, et al. Human astrocyte maturation captured in 3D cerebral cortical spheroids derived from pluripotent stem cells. Neuron. 2017;95(4):779–90. e6
Dang J, Tiwari SK, Lichinchi G, Qin Y, Patil VS, Eroshkin AM, et al. Zika virus depletes neural progenitors in human cerebral organoids through activation of the innate immune receptor TLR3. Cell Stem Cell. 2016;19(2):258–65.
Fatehullah A, Tan SH, Barker N. Organoids as an in vitro model of human development and disease. Nat Cell Biol. 2016;18(3):246–54.
Qian X, Nguyen HN, Song MM, Hadiono C, Ogden SC, Hammack C, et al. Brain-region-specific organoids using mini-bioreactors for modeling ZIKV exposure. Cell. 2016;165(5):1238–54.
Son MY, Sim H, Son YS, Jung KB, Lee MO, Oh JH, et al. Distinctive genomic signature of neural and intestinal organoids from familial Parkinson’s disease patient-derived induced pluripotent stem cells. Neuropathol Appl Neurobiol. 2017;43(7):584–603.
Monzel AS, Smits LM, Hemmer K, Hachi S, Moreno EL, van Wuellen T, et al. Derivation of human midbrain-specific organoids from Neuroepithelial stem cells. Stem Cell Rep. 2017;8(5):1144–54.
Raja WK, Mungenast AE, Lin YT, Ko T, Abdurrob F, Seo J, et al. Self-organizing 3D human neural tissue derived from induced pluripotent stem cells recapitulate Alzheimer’s disease phenotypes. PLoS One. 2016;11(9):e0161969.
Birey F, Andersen J, Makinson CD, Islam S, Wei W, Huber N, et al. Assembly of functionally integrated human forebrain spheroids. Nature. 2017;545(7652):54–9.
Srikanth P, Young-Pearse TL. Stem cells on the brain: modeling neurodevelopmental and neurodegenerative diseases using human induced pluripotent stem cells. J Neurogenet. 2014;28(1–2):5–29.
Prince M, Wimo A, Guerchet M, Ali G, Wu Y, Prina M, World Alzheimer Report 2015. The global impact of dementia. An analysis of prevalence, incidence, cost & trends. London: Alzheimer’s Disease International: London; 2015.
Hardy J, Selkoe DJ. The amyloid hypothesis of Alzheimer’s disease: progress and problems on the road to therapeutics. Science. 2002;297(5580):353–6.
Tanzi RE, Bertram L. Twenty years of the Alzheimer’s disease amyloid hypothesis: a genetic perspective. Cell. 2005;120(4):545–55.
Vassar R. BACE1 inhibitor drugs in clinical trials for Alzheimer’s disease. Alzheimers Res Ther. 2014;6(9):89.
Canter RG, Penney J, Tsai LH. The road to restoring neural circuits for the treatment of Alzheimer’s disease. Nature. 2016;539(7628):187–96.
Berk C, Paul G, Sabbagh M. Investigational drugs in Alzheimer’s disease: current progress. Expert Opin Investig Drugs. 2014;23(6):837–46.
Mullard A. Pharma pumps up anti-tau Alzheimer pipeline despite first phase III failure. Nat Rev Drug Discov. 2016;15(9):591–2.
Hughes RE, Nikolic K, Ramsay RR. One for all? Hitting multiple Alzheimer’s disease targets with one drug. Front Neurosci. 2016;10:177.
Bird TD. Genetic factors in Alzheimer’s disease. N Engl J Med. 2005;352(9):862–4.
Goate A, Chartier-Harlin MC, Mullan M, Brown J, Crawford F, Fidani L, et al. Segregation of a missense mutation in the amyloid precursor protein gene with familial Alzheimer’s disease. Nature. 1991;349(6311):704–6.
Levy-Lahad E, Wasco W, Poorkaj P, Romano DM, Oshima J, Pettingell WH, et al. Candidate gene for the chromosome 1 familial Alzheimer’s disease locus. Science. 1995;269(5226):973–7.
Cruts M, Hendriks L, Van Broeckhoven C. The presenilin genes: a new gene family involved in Alzheimer disease pathology. Hum Mol Genet. 1996;5:1449–55.
Sherrington R, Rogaev EI, Liang Y, Rogaeva EA, Levesque G, Ikeda M, et al. Cloning of a gene bearing missense mutations in early-onset familial Alzheimer’s disease. Nature. 1995;375(6534):754–60.
Scheuner D, Eckman C, Jensen M, Song X, Citron M, Suzuki N, et al. Secreted amyloid beta-protein similar to that in the senile plaques of Alzheimer’s disease is increased in vivo by the presenilin 1 and 2 and APP mutations linked to familial Alzheimer’s disease. Nat Med. 1996;2(8):864–70.
Goedert M, Strittmatter WJ, Roses AD. Alzheimer’s disease. Risky apolipoprotein in brain. Nature. 1994;372(6501):45–6.
Kamboh MI, Demirci FY, Wang X, Minster RL, Carrasquillo MM, Pankratz VS, et al. Genome-wide association study of Alzheimer’s disease. Transl Psychiatry. 2012;2:e117.
Saunders AM, Strittmatter WJ, Schmechel D, George-Hyslop PH, Pericak-Vance MA, Joo SH, et al. Association of apolipoprotein E allele epsilon 4 with late-onset familial and sporadic Alzheimer’s disease. Neurology. 1993;43(8):1467–72.
Huang YA, Zhou B, Wernig M, Sudhof TC. ApoE2, ApoE3, and ApoE4 differentially stimulate APP transcription and Abeta secretion. Cell. 2017;168(3):427–41. e21
Kondo T, Asai M, Tsukita K, Kutoku Y, Ohsawa Y, Sunada Y, et al. Modeling Alzheimer’s disease with iPSCs reveals stress phenotypes associated with intracellular Abeta and differential drug responsiveness. Cell Stem Cell. 2013;12(4):487–96.
Yagi T, Ito D, Okada Y, Akamatsu W, Nihei Y, Yoshizaki T, et al. Modeling familial Alzheimer’s disease with induced pluripotent stem cells. Hum Mol Genet. 2011;20(23):4530–9.
Sproul AA, Jacob S, Pre D, Kim SH, Nestor MW, Navarro-Sobrino M, et al. Characterization and molecular profiling of PSEN1 familial Alzheimer’s disease iPSC-derived neural progenitors. PLoS One. 2014;9(1):e84547.
Hossini AM, Megges M, Prigione A, Lichtner B, Toliat MR, Wruck W, et al. Induced pluripotent stem cell-derived neuronal cells from a sporadic Alzheimer’s disease donor as a model for investigating AD-associated gene regulatory networks. BMC Genomics. 2015;16:84.
Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry. 1992;55(3):181–4.
Fahn S. Description of Parkinson’s disease as a clinical syndrome. Ann N Y Acad Sci. 2003;991:1–14.
Antony PM, Diederich NJ, Kruger R, Balling R. The hallmarks of Parkinson’s disease. FEBS J. 2013;280(23):5981–93.
Gibrat C, Saint-Pierre M, Bousquet M, Levesque D, Rouillard C, Cicchetti F. Differences between subacute and chronic MPTP mice models: investigation of dopaminergic neuronal degeneration and alpha-synuclein inclusions. J Neurochem. 2009;109(5):1469–82.
Martinez-Morales PL, Liste I. Stem cells as in vitro model of Parkinson’s disease. Stem Cells Int. 2012;2012:980941.
Cooper O, Hargus G, Deleidi M, Blak A, Osborn T, Marlow E, et al. Differentiation of human ES and Parkinson’s disease iPS cells into ventral midbrain dopaminergic neurons requires a high activity form of SHH, FGF8a and specific regionalization by retinoic acid. Mol Cell Neurosci. 2010;45(3):258–66.
Narsinh KH, Plews J, Wu JC. Comparison of human induced pluripotent and embryonic stem cells: fraternal or identical twins? Mol Ther. 2011;19(4):635–8.
Hargus G, Cooper O, Deleidi M, Levy A, Lee K, Marlow E, et al. Differentiated Parkinson patient-derived induced pluripotent stem cells grow in the adult rodent brain and reduce motor asymmetry in parkinsonian rats. Proc Natl Acad Sci U S A. 2010;107(36):15921–6.
Recasens A, Dehay B, Bove J, Carballo-Carbajal I, Dovero S, Perez-Villalba A, et al. Lewy body extracts from Parkinson disease brains trigger alpha-synuclein pathology and neurodegeneration in mice and monkeys. Ann Neurol. 2014;75(3):351–62.
Walker FO. Huntington’s disease. Lancet. 2007;369(9557):218–28.
An MC, Zhang N, Scott G, Montoro D, Wittkop T, Mooney S, et al. Genetic correction of Huntington's disease phenotypes in induced pluripotent stem cells. Cell Stem Cell. 2012;11(2):253–63.
Consortium HDi. Induced pluripotent stem cells from patients with Huntington’s disease show CAG-repeat-expansion-associated phenotypes. Cell Stem Cell. 2012;11(2):264–78.
Juopperi TA, Kim WR, Chiang CH, Yu H, Margolis RL, Ross CA, et al. Astrocytes generated from patient induced pluripotent stem cells recapitulate features of Huntington's disease patient cells. Mol Brain. 2012;5:17.
Roos RA. Huntington’s disease: a clinical review. Orphanet J Rare Dis. 2010;5:40.
Jeon I, Lee N, Li JY, Park IH, Park KS, Moon J, et al. Neuronal properties, in vivo effects, and pathology of a Huntington’s disease patient-derived induced pluripotent stem cells. Stem Cells. 2012;30(9):2054–62.
Chae JI, Kim DW, Lee N, Jeon YJ, Jeon I, Kwon J, et al. Quantitative proteomic analysis of induced pluripotent stem cells derived from a human Huntington’s disease patient. Biochem J. 2012;446(3):359–71.
Virlogeux A, Moutaux E, Christaller W, Genoux A, Bruyere J, Fino E, et al. Reconstituting Corticostriatal network on-a-Chip reveals the contribution of the presynaptic compartment to Huntington’s disease. Cell Rep. 2018;22(1):110–22.
Wijesekera LC, Leigh PN. Amyotrophic lateral sclerosis. Orphanet J Rare Dis. 2009;4:3.
Hudson AJ. Amyotrophic lateral sclerosis and its association with dementia, parkinsonism and other neurological disorders: a review. Brain. 1981;104(2):217–47.
Brown RH Jr. Amyotrophic lateral sclerosis. Insights from genetics. Arch Neurol. 1997;54(10):1246–50.
Juneja T, Pericak-Vance MA, Laing NG, Dave S, Siddique T. Prognosis in familial amyotrophic lateral sclerosis: progression and survival in patients with glu100gly and ala4val mutations in cu, Zn superoxide dismutase. Neurology. 1997;48(1):55–7.
Kiernan MC, Vucic S, Cheah BC, Turner MR, Eisen A, Hardiman O, et al. Amyotrophic lateral sclerosis. Lancet. 2011;377(9769):942–55.
Di Giorgio FP, Boulting GL, Bobrowicz S, Eggan KC. Human embryonic stem cell-derived motor neurons are sensitive to the toxic effect of glial cells carrying an ALS-causing mutation. Cell Stem Cell. 2008;3(6):637–48.
van Blitterswijk M, DeJesus-Hernandez M, Rademakers R. How do C9ORF72 repeat expansions cause amyotrophic lateral sclerosis and frontotemporal dementia: can we learn from other noncoding repeat expansion disorders? Curr Opin Neurol. 2012;25(6):689–700.
Bilican B, Serio A, Barmada SJ, Nishimura AL, Sullivan GJ, Carrasco M, et al. Mutant induced pluripotent stem cell lines recapitulate aspects of TDP-43 proteinopathies and reveal cell-specific vulnerability. Proc Natl Acad Sci U S A. 2012;109(15):5803–8.
Zhang Z, Almeida S, Lu Y, Nishimura AL, Peng L, Sun D, et al. Downregulation of microRNA-9 in iPSC-derived neurons of FTD/ALS patients with TDP-43 mutations. PLoS One. 2013;8(10):e76055.
Ichiyanagi N, Fujimori K, Yano M, Ishihara-Fujisaki C, Sone T, Akiyama T, et al. Establishment of in vitro FUS-associated familial amyotrophic lateral sclerosis model using human induced pluripotent stem cells. Stem Cell Rep. 2016;6(4):496–510.
Toli D, Buttigieg D, Blanchard S, Lemonnier T, Lamotte d'Incamps B, Bellouze S, et al. Modeling amyotrophic lateral sclerosis in pure human iPSc-derived motor neurons isolated by a novel FACS double selection technique. Neurobiol Dis. 2015;82:269–80.
Chen H, Qian K, Du Z, Cao J, Petersen A, Liu H, et al. Modeling ALS with iPSCs reveals that mutant SOD1 misregulates neurofilament balance in motor neurons. Cell Stem Cell. 2014;14(6):796–809.
Burkhardt MF, Martinez FJ, Wright S, Ramos C, Volfson D, Mason M, et al. A cellular model for sporadic ALS using patient-derived induced pluripotent stem cells. Mol Cell Neurosci. 2013;56:355–64.
Sareen D, O'Rourke JG, Meera P, Muhammad AK, Grant S, Simpkinson M, et al. Targeting RNA foci in iPSC-derived motor neurons from ALS patients with a C9ORF72 repeat expansion. Sci Transl Med. 2013;5(208):208ra149.
Dafinca R, Scaber J, Ababneh N, Lalic T, Weir G, Christian H, et al. C9orf72 Hexanucleotide expansions are associated with altered endoplasmic reticulum calcium homeostasis and stress granule formation in induced pluripotent stem cell-derived neurons from patients with amyotrophic lateral sclerosis and frontotemporal dementia. Stem Cells. 2016;34(8):2063–78.
Devlin A-C, Burr K, Borooah S, Foster JD, Cleary EM, Geti I, et al. Human iPSC-derived motoneurons harbouring TARDBP or C9ORF72 ALS mutations are dysfunctional despite maintaining viability. Nat Commun. 2015;6:5999.
Wainger BJ, Kiskinis E, Mellin C, Wiskow O, Han SS, Sandoe J, et al. Intrinsic membrane hyperexcitability of amyotrophic lateral sclerosis patient-derived motor neurons. Cell Rep. 2014;7(1):1–11.
Hall CE, Yao Z, Choi M, Tyzack GE, Serio A, Luisier R, et al. Progressive motor neuron pathology and the role of astrocytes in a human stem cell model of VCP-related ALS. Cell Rep. 2017;19(9):1739–49.
Madill M, McDonagh K, Ma J, Vajda A, McLoughlin P, O'Brien T, et al. Amyotrophic lateral sclerosis patient iPSC-derived astrocytes impair autophagy via non-cell autonomous mechanisms. Mol Brain. 2017;10(1):22.
Smith I, Haag M, Ugbode C, Tams D, Rattray M, Przyborski S, et al. Neuronal-glial populations form functional networks in a biocompatible 3D scaffold. Neurosci Lett. 2015;609:198–202.
Krencik R, Seo K, van Asperen JV, Basu N, Cvetkovic C, Barlas S, et al. Systematic three-dimensional Coculture rapidly recapitulates interactions between human neurons and astrocytes. Stem Cell Rep. 2017;9(6):1745–53.
Liang G, Zhang Y. Genetic and epigenetic variations in iPSCs: potential causes and implications for application. Cell Stem Cell. 2013;13(2):149–59.
Kim K, Zhao R, Doi A, Ng K, Unternaehrer J, Cahan P, et al. Donor cell type can influence the epigenome and differentiation potential of human induced pluripotent stem cells. Nat Biotechnol. 2011;29(12):1117–9.
Ohi Y, Qin H, Hong C, Blouin L, Polo JM, Guo T, et al. Incomplete DNA methylation underlies a transcriptional memory of somatic cells in human iPS cells. Nat Cell Biol. 2011;13(5):541–9.
Takebe T, Enomura M, Yoshizawa E, Kimura M, Koike H, Ueno Y, et al. Vascularized and complex organ buds from diverse tissues via mesenchymal cell-driven condensation. Cell Stem Cell. 2015;16(5):556–65.
Rambani K, Vukasinovic J, Glezer A, Potter SM. Culturing thick brain slices: an interstitial 3D microperfusion system for enhanced viability. J Neurosci Methods. 2009;180(2):243–54.
Perry VH, Nicoll JA, Holmes C. Microglia in neurodegenerative disease. Nat Rev Neurol. 2010;6(4):193–201.
Haenseler W, Sansom SN, Buchrieser J, Newey SE, Moore CS, Nicholls FJ, et al. A highly efficient human pluripotent stem cell microglia model displays a neuronal-co-culture-specific expression profile and inflammatory response. Stem Cell Rep. 2017;8(6):1727–42.
Deng Y, Kuiper J. Functional 3D tissue engineering scaffolds: materials, technologies, and applications. 1st ed. Sawston: Woodhead Publishing; 2017.
Caliari SR, Burdick JA. A practical guide to hydrogels for cell culture. Nat Meth. 2016;13(5):405–14.
Tibbitt MW, Anseth KS. Hydrogels as extracellular matrix mimics for 3D cell culture. Biotechnol Bioeng. 2009;103(4):655–63.
Hughes CS, Postovit LM, Lajoie GA. Matrigel: a complex protein mixture required for optimal growth of cell culture. Proteomics. 2010;10(9):1886–90.
Sposito T, Preza E, Mahoney CJ, Seto-Salvia N, Ryan NS, Morris HR, et al. Developmental regulation of tau splicing is disrupted in stem cell-derived neurons from frontotemporal dementia patients with the 10 + 16 splice-site mutation in MAPT. Hum Mol Genet. 2015;24(18):5260–9.
Zhang Y, Pak C, Han Y, Ahlenius H, Zhang Z, Chanda S, et al. Rapid single-step induction of functional neurons from human pluripotent stem cells. Neuron. 2013;78(5):785–98.
Vera E, Studer L. When rejuvenation is a problem: challenges of modeling late-onset neurodegenerative disease. Development. 2015;142(18):3085–9.
Campos PB, Paulsen BS, Rehen SK. Accelerating neuronal aging in in vitro model brain disorders: a focus on reactive oxygen species. Front Aging Neurosci. 2014;6:292.
Miller JD, Ganat YM, Kishinevsky S, Bowman RL, Liu B, Tu EY, et al. Human iPSC-based modeling of late-onset disease via progerin-induced aging. Cell Stem Cell. 2013;13(6):691–705.
Ren Y, Kunze A, Renaud P. Compartmentalized microfluidics for in vitro Alzheimer’s disease studies. In: Biffi E, editor. Microfluidic and compartmentalized platforms for neurobiological research. New York: Springer New York; 2015. p. 197–215.
Taylor AM, Jeon NL. Micro-scale and microfluidic devices for neurobiology. Curr Opin Neurobiol. 2010;20(5):640–7.
Poon WW, Blurton-Jones M, Tu CH, Feinberg LM, Chabrier MA, Harris JW, et al. Beta-amyloid impairs axonal BDNF retrograde trafficking. Neurobiol Aging. 2011;32(5):821–33.
Adriani G, Ma D, Pavesi A, Kamm RD, Goh EL. A 3D neurovascular microfluidic model consisting of neurons, astrocytes and cerebral endothelial cells as a blood-brain barrier. Lab Chip. 2017;17(3):448–59.
Park J, Lee BK, Jeong GS, Hyun JK, Lee CJ, Lee SH. Three-dimensional brain-on-a-chip with an interstitial level of flow and its application as an in vitro model of Alzheimer’s disease. Lab Chip. 2015;15(1):141–50.
Author information
Authors and Affiliations
Contributions
EGZC wrote the manuscript, HC and AB contributed to manuscript writing and editing. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Centeno, E.G.Z., Cimarosti, H. & Bithell, A. 2D versus 3D human induced pluripotent stem cell-derived cultures for neurodegenerative disease modelling. Mol Neurodegeneration 13, 27 (2018). https://doi.org/10.1186/s13024-018-0258-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13024-018-0258-4