
Abstract
Background
Transthyretin cardiac cardiomyopathy (ATTR-CM) is a rare but life-threatening disease. Tafamidis is an effective treatment for patients with ATTR-CM, however its long-term effects on cardiac remodeling and cardiac amyloid deposition are unknown. This study aimed to used cardiac magnetic resonance (CMR) to investigate the effects of tafamidis on patients with hereditary A97S ATTR-CM.
Methods
We retrospectively analyzed a prospective cohort of ATTR-CM patients, including 14 with hereditary A97S ATTR-CM and 17 healthy controls with baseline CMR data. All ATTR-CM patients received tafamidis treatment and received CMR with extracellular volume (ECV) at baseline and after 1 year of follow-up.
Results
Baseline N-terminal pro-B-type natriuretic peptide, left ventricular (LV) mass, LV ejection fraction, global radial, circumferential and longitudinal strain, T1 mapping and ECV were significantly worse in the patients with ATTR-CM compared with the healthy controls. After 1 year of tafamidis treatment, ECV decreased from 51.5 ± 8.9% to 49.0 ± 9.4% (P = 0.041), however there were no significant changes in LV mass, LV ejection fraction, global radial strain, global circumferential strain, global longitudinal strain and T1 mapping.
Conclusions
After a one-year treatment period, tafamidis exhibited subtle but statistically significant reductions in ECV, potentially indicating a decrease in amyloid deposition among patients diagnosed with hereditary A97S ATTR-CM.
Similar content being viewed by others
Background
Transthyretin amyloid cardiomyopathy (ATTR-CM) is caused by the accumulation of misfolded transthyretin fibrils in the myocardium which leads to heart failure [1, 2]. ATTR-CM is a progressive and life-threatening disease. There are two types of ATTR-CM, a hereditary form (ATTRv) and a wild-type form (ATTRwt). These two types of ATTR-CM have variable clinical presentations, but both have poor long-term outcomes [1, 3]. Tafamidis is an effective treatment for ATTR-CM which can stabilize transthyretin and consequently decrease amyloid formation in these patients [4]. In the Transthyretin Amyloidosis Cardiomyopathy Clinical Trial (ATTR-ACT trial), tafamidis was associated with a decrease in disease progression, all-cause mortality and cardiovascular-related hospitalizations in ATTR-CM patients [5].
Currently, there is no widely accepted tool to monitor the treatment response to tafamidis in ATTR-CM patients [6]. Although serum biomarkers, echocardiography, nuclear studies and cardiac magnetic resonance (CMR) have all been used to investigate the clinical response to tafamidis in patients with ATTR CM, [7] the results have been inconsistent. There is significant variation in the extent of cardiac involvement associated with different transthyretin variants [8]. In Taiwan, the most common type of ATTRv is A97S (p.Ala117Ser). A substantial proportion, up to 82.1% of patients with hereditary A97S ATTR amyloidosis experience cardiac involvement [9]. Unfortunately, few studies have investigated the effects of tafamidis on cardiac remodeling in patients with hereditary A97S ATTR-CM, and this genetic variant was not enrolled in the ATTR-ACT trial [5].
CMR has a unique role in monitoring disease status and treatment response in patients with ATTR-CM, as it can be used to investigate not only the structures of the heart but also tissue characterization including amyloid deposition and fibrosis [10]. CMR techniques are commonly used to detect amyloid deposition, including the patterns of late gadolinium enhancement (LGE), native T1 mapping and extracellular volume (ECV) measurement [11]. ECV is used to demonstrate the percentage of extracellular space, which suggests the degree of amyloid deposition in patients with ATTR-CM [7, 12]. In this study, we aimed to use CMR to investigate the treatment effects of tafamidis on cardiac remodeling in patients with hereditary A97S ATTR-CM.
Materials and methods
Study design and subjects
We retrospectively analyzed a prospective cohort of patients with ATTR-CM receiving tafamidis (61 mg/day) treatment at National Taiwan University Hospital. The inclusion criteria were patients: (1) with heart failure symptoms; (2) in whom the diagnosis of ATTR-CM was confirmed by Tc99m-pyrophosphate (PYP) scintigraphy and light chain disease was excluded [13, 14]; (3) with the A97S mutation detected by either Sanger sequencing or restriction enzyme analysis specific for the A97S transthyretin mutation [9, 15]; and (4) who completed 12 months of tafamidis treatment; (5) who underwent CMR at baseline and after 12 months of treatment. The exclusion criteria were patients: (1) who died or were lost to follow-up within 12 months; (2) had poor drug compliance or could not tolerate tafamidis; and (3) had ATTRwt or non-A97S hereditary ATTR-CM. Healthy subjects who underwent CMR studies at National Taiwan University Hospital were also enrolled as controls. All patients provided informed consent before enrollment. This study was approved by the Institutional Review Board of National Taiwan University Hospital.
Echocardiography
All study subjects received transthoracic echocardiography at enrollment using an IE33 system (Philips Medical Systems; Andover, Massachusetts, USA). The echocardiographic measurements were performed in accordance with the recommendations of the American Society of Echocardiography [16].
CMR imaging acquisition
CMR was performed on a 1.5-T Magnetom Aera (Siemens Healthcare, Erlangen, Germany) with a 30-channel cardiac coil array. Myocardial T1 mapping was performed with an electrocardiography (ECG)-triggered modified Look-Locker inversion recovery (MOLLI) pulse sequence before and 10 min after.
0.15 mmol/kg intravenous administration of a gadolinium-based contrast agent (Dotarem, Guerbet, France). The MOLLI protocol used a 5(3)3 sampling scheme for native T1 mapping, and a 4(1)3(1)2 sampling scheme for postcontrast T1 mapping. The scan parameters were as follows: TE/TR 1.14/2.7 ms; flip angle 35°; bandwidth.
977 Hz/Px; minimum TI 125–150 ms; TI increment 80 ms; pixel-spacing 1.36 × 1.36 mm2; slice thickness 8 mm; iPAT factor (GRAPPA) 2.
Cine MRI was performed using a segmented balanced steady-state gradient echo pulse sequence with a retrospective ECG R-wave trigger. The scan parameters were as follows: TE/TR 1.6/3.0 ms; flip angle 50–70°; bandwidth 975 Hz/Px; pixel-spacing 1.25 × 1.25 mm2; slice thickness 8 mm; gap 2 mm; iPAT factor (GRAPPA) 2. A total of 10–12 short axis slices were obtained, depending on cardiac size. Thirty cardiac phases were acquired for each level. After postcontrast T1 acquisition, LGE images were acquired using an ECG-triggered phase-sensitive inversion recovery prepared segmented fast gradient-echo pulse sequence to identify focal fibrosis or scarring.
CMR imaging analysis
The left ventricular (LV) function, myocardial strain and ECV were analyzed offline with commercial postprocessing software (cvi42, Circle Cardiovascular imaging, Calgary, AB, Canada). Epicardial and endocardial contours of the LV were determined at each slice level on cine images, and the area enclosed by each contour was computed for LV function and mass analysis,
LV volumes were then determined using the Simpson rule. End-diastolic volume (EDV) and end-systolic volume (ESV) of the LV were measured from the volume-time curve for the maximal and minimal values. LV mass was computed as the difference between LV epicardial volume at end-diastole and EDV multiplied by the density of the myocardium (1.05 g/ml). LV volumes and mass indexed to body surface area were also measured from EDV, ESV, and LV mass divided by body surface area. Myocardial strain was analyzed on cine images using a tissue tracking technique [17]. We used three long-axis (two-chamber, three-chamber, and four-chamber views) and three short-axis (basal, middle, and apical levels) cine images to measure the peak global systolic radial, circumferential, and longitudinal LV strain. The epi- and endocardial contours were automatically propagated on the end-diastolic images by the software throughout the cardiac cycle generating myocardial strain.
Myocardial ECV was measured from native and postcontrast T1 maps using a region-based method [18]. The regions of interest in the blood and myocardium of the LV were drawn in the central areas of the LV cavity and septal myocardium on the T1-mapping image. If the septal myocardium showed regional hyperenhancement on the LGE images, the region of interest in the myocardium was redrawn in other unenhanced myocardial regions. The average T1 values of the segmented regions of interest were then computed. After subtracting the pre-contrast values from the post-contrast values, the changes in the relaxation rate (1/T1) in the blood and myocardium were obtained. Myocardial ECV values were calculated using the ratio of the change in relaxation rate in the myocardium to that in the blood and multiplied by (1-hematocrit).
Statistical analysis
Data were expressed as mean ± standard deviation for all continuous variables and number (%) for categorical variables. Comparisons of continuous data between the ATTR-CM patients and controls were performed using the Mann-Whitney U test. Differences between proportions were analyzed using the chi-square test or Fisher’s exact test. The area under the curve (AUC) was used to assess the discriminatory power of the model to predict ATTR-CM. Comparisons of data between baseline and after tafamidis treatment were performed using the Wilcoxon test. All statistical analyses were performed using SPSS for Windows, version 25.0 (SPSS Inc, Chicago, IL).
Results
Study subjects
We enrolled 14 patients with hereditary A97S ATTR-CM and 17 healthy control subjects. In our cohort of patients with hereditary A97S ATTR-CM, 15 individuals underwent baseline CMR, while 14 patients received follow-up CMR examinations at the 1 year. Tafamidis was well-tolerated by all patients, and no instances of mortality or loss of follow-up were observed among the enrolled participants. The baseline characteristics were similar between the two groups. One patient in this cohort was reported previously [19]. All these patients also had documented neuropathy and were followed by neurologist. More patients with ATTR-CM had worse New York Heart Association (NYHA) functional class (ATTR-CM: 7% functional class I, 86% functional class II, and 7% functional class III; controls: 100% functional class I, P < 0.001) and significantly higher N-terminal pro-B-type natriuretic peptide (NT-proBNP, 2078.1 ± 3886.3 to 90.2 ± 73.1 pg/ml, P < 0.001). The ATTR-CM patients also had significantly thicker LV anterior and posterior wall thickness as measured by echocardiography (Table 1).
CMR imaging analysis
CMR studies showed a significantly lower LV ejection fraction (LVEF) in the patients with ATTR-CM compared with the controls (54.1 ± 9.5% vs. 69.3 ± 10.1%, P < 0.001). The LV end-systolic volume index (LVESVi, 32.3 ± 12.0 vs. 19.9 ± 10.9 ml/m2, P = 0.001) and LV mass index (LVMi, 93.0 ± 24.8 vs. 52.3 ± 12.9, P < 0.001) were significantly higher in the patients with ATTR-CM than in the controls. The patients with ATTR-CM had significantly lower global radial strain (GRS, 19.2 ± 8.9 to 36.3 ± 7.7, P < 0.001) and significantly higher global circumferential strain (GCS, -12.6 ± 4.3 to -19.7 ± 2.7, P < 0.001) and global longitudinal strain (GLS, -8.7 ± 3.3 to -17.2 ± 3.4, P < 0.001) compared to the controls. Native T1 mapping (1159.5 ± 53.0 to 1020.8 ± 37.3 ms, P < 0.001) and ECV (51.5 ± 8.9% to 26.1 ± 3.1%, P < 0.001) were significantly higher in the ATTR-CM patients (Table 2; Fig. 1).

The CMR parameters in patients with ATTR-CM and healthy control
Comparisons of CMR imaging parameters to differentiate the patients with ATTR-CM from the controls
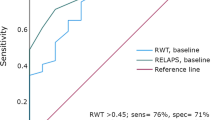
Among all CMR imaging parameters, ECV had the highest AUC to predict the presence of ATTR-CM in receiver operating characteristic (ROC) curve analysis (AUC: 0.982). The AUCs of all CMR imaging parameters including LVEF, LV end-diastolic volume index (LVEDVi), LVESVi, LVMi, GRS, GCS, GLS, native T1 mapping and ECV were 0.857, 0.669, 0.824, 0.890, 0.879, 0.860, 0.923, 0.974 and 0.982, respectively.
Treatment response after 1 year of tafamidis treatment
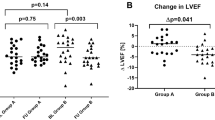
After 1 year of tafamidis treatment, 21% of the patients had improved NYHA functional status, and 79% had no significant change in functional status (P = 0.083). Prealbumin level, which is known as transthyretin (available in 6 patients), significantly improved after tafamidis treatment (27.1 ± 9.1 to 32.0 ± 7.7 mg/dL, P = 0.046). NT-proBNP level improved from 2078.1 ± 3886.3 to 1133.4 ± 1032.6 pg/ml but did not reach statistical significance (P = 0.221). Of the CMR imaging parameters, LVEF, LVEDVi, LVESVi, LVMi, CRS, GCS, GLS and native T1 mapping remained stationary after tafamidis treatment. There was a subtle but statistically significant decreased of ECV after 1 year of tafamidis treatment (51.5 ± 8.9 to 49.0 ± 9.4, P = 0.041) (Figs. 2 and 3; Table 3).

CMR-derived ECV maps before and after tafamidis treatment
CMR-derived ECV maps at baseline (top raw) and 1-year follow-up after tafamidis treatment (bottom raw)

CMR parameters, NT-proBNP and prealbumin before and after tafamidis treatment
(A) ECV, (B) LV GLS, (C) LogNT-proBNP, and (D) ECV before and after tafamidis treatment
Discussion
This study is the first to demonstrate the potentially reversible effects of tafamidis on cardiac amyloid deposition in patients with A97S hereditary ATTR-CM. In the ATTR-ACT trial, tafamidis was shown to decrease all-cause mortality and cardiovascular-related hospitalizations [5]. However, the effects of tafamidis on cardiac remolding and amyloid deposition are still unknown.
ATTR-CM is a progressive and fatal disease which results from the accumulation of misfolded transthyretin in the myocardium. Tafamidis can stabilize transthyretin and theoretically slow disease progression. In the ATTR-ACT trial, tafamidis was shown to significantly improve survival and functional status of patients with ATTR-CM [5]. However, the effects of tafamidis on cardiac structural and functional changes are still under investigation. Several studies using different imaging modalities have demonstrated that tafamidis can slow the progression of cardiac remodeling [20,21,22,23]. Most of these studies used echocardiography to measure LV mass and analyze strain, and they showed that tafamidis could slow the progression of cardiac structural and functional changes [21, 22]. Several case reports have demonstrated that tafamidis can reverse cardiac remodeling in patients with ATTR-CM [24,25,26]. In the current study, cardiac structural and strain analysis measured using CMR remained stationary after 1 year of tafamidis treatment, suggesting that tafamidis can slow disease progression. These results are consistent with a previous study [23].
Rettl et al. were the first to report that tafamidis could delay myocardial amyloid progression in patients with ATTRwt using CMR. In addition, ECV remained stationary (47.5–47.7%, P = 0.861) in the patients who received daily 61 mg tafamidis, but deteriorated in treatment-naïve patients (49.3–54.6%, P = 0.023) [23]. Chamling et al. also demonstrated similar results in the ATTRwt patients, in whom LVMi, GLS and ECV remained stationary after tafamidis treatment. After 12 ± 3 months of tafamidis treatment, ECV decreased from 57 to 54% (P = 0.19) [27]. Both studies investigated the effects of tafamidis on the ATTRwt patients. In contrast, we investigated hereditary A97S ATTR-CM patients in the present study. Our findings revealed a subtle but statistically significant improvement in ECV (51.5 ± 8.9% to 49.0 ± 9.4%, P = 0.041) following one year of tafamidis treatment. Since tafamidis is the transthyretin stabilizer, tafamidis has demonstrated greater efficacy in patients at earlier stages of the disease. In our study, the majority of patients (93%) presented with NYHA function class I to II. This observation may provide a potential explanation for the effectiveness of tafamidis observed in this study. The genetic variant is the other potential explanation. A97S is the most common ATTR variant in Taiwan, however it has been less frequently investigated in previous clinical trials. A97S hereditary ATTR amyloidosis is relatively late onset. Majority these patients have cardiac involvement, and refractory heart failure is the major cause of death [9, 28].
Other novel disease-modifying therapies can also treat ATTR-CM. Two novel TTR gene silencers including the small interfering RNA patisiran and the antisense oligonucleotide inotersen have been investigated in patients with ATTR-CM [29]. Fontana et al. demonstrated that patisiran could reduce the progression of amyloid deposition, and that the patients who received patisiran had stationary ECV values compared with historical controls [7]. Data on the effects of inotersen using CMR are still limited. In the current study, we used CMR to demonstrate the excellent effects of tafamidis on slowing the progression of cardiac remodeling and the potential ability to reverse it in patients with A97S hereditary ATTR-CM. Our results suggest that amyloid deposition may not be an irreversible process, but rather that it is dynamic and reversible. However, this study only enrolled A97S hereditary ATTR-CM patients and the number of patients was small. Therefore, the results should be interpreted carefully.
CMR is a valuable and non-invasive diagnostic tool for cardiomyopathy which can assess tissue characterization, cardiac structure and function [10]. It is practically useful in patients with inconclusive results on 99mTc-PYP scintigraphy. In these cases, CMR can help the clinician to detect amyloid deposition and also guide the need for an endomyocardial biopsy. There are many different imaging techniques in CMR, including traditional cine CMR, late gadolinium enhancement, native T1 mapping (non-contrast) and ECV (with contrast) measurement [30]. The ECV is usually ≥ 40% in patients with ATTR-CM, which is a useful feature to differentiate it from other cardiomyopathies [31, 32]. In the current study, the ECV had the greatest power to differentiate the ATTR-CM patients from the healthy controls (AUC: 0.982). In addition, the ECV improved after tafamidis treatment, which suggests the potential role of ECV to monitor treatment response.
Notably, although no statistically significant improvement in NYHA functional status was observed in this study, a noticeable trend of functional status improvement was detected. The duration of our follow-up period was relatively short compared to the ATTR-ACT study, where significant improvement in clinical endpoints was observed after 30 months, with a noticeable trend towards improvement at around 15 months [5]. In contrast, our study had a follow-up period of only 12 months. Furthermore, due to the small sample size, our study may lack statistical power to answer this question.
Limitations
There are several limitations to this study. First, this was a small, single-arm, prospective cohort study. Further larger studies with a control group are needed to confirmed our findings. However, the results of the current study are still valuable, since data on the treatment effects of tafamidis in patients with A97S ATTR-CM are still very limited. Second, not all of the patients had complete prealbumin data, which may have affected the results. Third, this is a prospective cohort study with retrospective analysis. Potential selection bias may have interfered with the results, and thus they should be interpreted carefully. Fourth, the follow-up period was relatively short compared with previous randomized control trial [5]. However, this study provides valuable information about the early change of ECV after tafamidis treatment in patients with A97S ATTR-CM. Fifth, the enrollment of predominantly male patients in this study introduced the possibility of gender bias, which could potentially impact the results of the study.
Conclusions
In conclusion, tafamidis can slow the progression of cardiac remodeling in patients with A97S hereditary ATTR-CM. In addition, tafamidis decreased ECV in our patients with hereditary A97S ATTR-CM, suggesting it might lower amyloid deposition. Our findings suggest the potential role of tafamidis to reverse cardiac remodeling in patients with A97S hereditary ATTR-CM.
Data Availability
The patient-level data of this study is not publicly available; however, it can be obtained from the authors upon reasonable request and with the permission of National Taiwan University Hospital.
Abbreviations
- ATTR-CM:
-
Transthyretin amyloid cardiomyopathy
- ATTRv:
-
Hereditary ATTR
- ATTRwt:
-
Wild-type ATTR
- ATTR-ACT trial:
-
Transthyretin Amyloidosis Cardiomyopathy Clinical Trial
- AUC:
-
Area under the curve
- CMR:
-
Cardiac magnetic resonance
- ECV:
-
Extracellular volume
- ECG:
-
Electrocardiography
- EDV:
-
End-diastolic volume
- ESV:
-
End-systolic volume
- GRS:
-
Global radial strain
- GCS:
-
Global circumferential strain
- GLS:
-
Global longitudinal strain
- LVESVi:
-
LV end-systolic volume index
- LVEF:
-
LV ejection fraction
- LVEDVi:
-
LV end-diastolic volume index
- LVMi:
-
LV mass index
- MOLLI:
-
Modified Look-Locker inversion recovery
- ROC:
-
Receiver operating characteristic
- NT-proBNP:
-
N-terminal pro-B-type natriuretic peptide
References
Ruberg FL, Grogan M, Hanna M, Kelly JW, Maurer MS. Transthyretin amyloid cardiomyopathy: JACC state-of-the-art review. J Am Coll Cardiol. 2019;73(22):2872–91.
Kittleson MM, Maurer MS, Ambardekar AV, Bullock-Palmer RP, Chang PP, Eisen HJ, et al. Cardiac amyloidosis: evolving diagnosis and management: a Scientific Statement from the American Heart Association. Circulation. 2020;142(1):e7–e22.
Ruberg FL, Berk JL. Transthyretin (TTR) cardiac amyloidosis. Circulation. 2012;126(10):1286–300.
Bulawa CE, Connelly S, Devit M, Wang L, Weigel C, Fleming JA, et al. Tafamidis, a potent and selective transthyretin kinetic stabilizer that inhibits the amyloid cascade. Proc Natl Acad Sci U S A. 2012;109(24):9629–34.
Maurer MS, Schwartz JH, Gundapaneni B, Elliott PM, Merlini G, Waddington-Cruz M, et al. Tafamidis Treatment for patients with transthyretin amyloid cardiomyopathy. N Engl J Med. 2018;379(11):1007–16.
Garcia-Pavia P, Bengel F, Brito D, Damy T, Duca F, Dorbala S, et al. Expert consensus on the monitoring of transthyretin amyloid cardiomyopathy. Eur J Heart Fail. 2021;23(6):895–905.
Fontana M, Martinez-Naharro A, Chacko L, Rowczenio D, Gilbertson JA, Whelan CJ, et al. Reduction in CMR Derived Extracellular volume with Patisiran indicates cardiac amyloid regression. JACC Cardiovasc Imaging. 2021;14(1):189–99.
Pilebro B, Suhr OB, Naslund U, Westermark P, Lindqvist P, Sundstrom T. (99m)Tc-DPD uptake reflects amyloid fibril composition in hereditary transthyretin amyloidosis. Ups J Med Sci. 2016;121(1):17–24.
Lai HJ, Huang KC, Liang YC, Chien KL, Lee MJ, Hsieh ST, et al. Cardiac manifestations and prognostic implications of hereditary transthyretin amyloidosis associated with transthyretin Ala97Ser. J Formos Med Assoc. 2020;119(3):693–700.
Haaf P, Garg P, Messroghli DR, Broadbent DA, Greenwood JP, Plein S. Cardiac T1 mapping and extracellular volume (ECV) in clinical practice: a comprehensive review. J Cardiovasc Magn Reson. 2016;18(1):89.
Fontana M, Banypersad SM, Treibel TA, Maestrini V, Sado DM, White SK, et al. Native T1 mapping in transthyretin amyloidosis. JACC Cardiovasc Imaging. 2014;7(2):157–65.
Fontana M, Pica S, Reant P, Abdel-Gadir A, Treibel TA, Banypersad SM, et al. Prognostic value of late Gadolinium Enhancement Cardiovascular magnetic resonance in Cardiac Amyloidosis. Circulation. 2015;132(16):1570–9.
Kitaoka H, Izumi C, Izumiya Y, Inomata T, Ueda M, Kubo T, et al. JCS 2020 Guideline on diagnosis and treatment of Cardiac Amyloidosis. Circ J. 2020;84(9):1610–71.
Maurer MS, Elliott P, Comenzo R, Semigran M, Rapezzi C. Addressing common questions encountered in the diagnosis and management of Cardiac Amyloidosis. Circulation. 2017;135(14):1357–77.
Yang NC, Lee MJ, Chao CC, Chuang YT, Lin WM, Chang MF, et al. Clinical presentations and skin denervation in amyloid neuropathy due to transthyretin Ala97Ser. Neurology. 2010;75(6):532–8.
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1–39e14.
Claus P, Omar AMS, Pedrizzetti G, Sengupta PP, Nagel E. Tissue Tracking Technology for assessing Cardiac mechanics: principles, normal values, and clinical applications. JACC Cardiovasc imaging. 2015;8(12):1444–60.
Su MY, Huang YS, Niisato E, Chow K, Juang JJ, Wu CK, et al. Is a timely assessment of the hematocrit necessary for cardiovascular magnetic resonance-derived extracellular volume measurements? J Cardiovasc Magn resonance: official J Soc Cardiovasc Magn Reson. 2020;22(1):77.
Wu YA, Tsai CH, Su MY, Chao CC, Cheng MF, Shun CT, et al. Reverse cardiac remodelling and dysfunction in A97S transthyretin cardiac amyloidosis after tafamidis treatment. ESC Heart Fail. 2022;9(6):4335–9.
Ochi Y, Kubo T, Baba Y, Sugiura K, Miyagawa K, Noguchi T, et al. Early experience of Tafamidis treatment in japanese patients with Wild-Type Transthyretin Cardiac Amyloidosis from the Kochi Amyloidosis Cohort. Circ J. 2022;86(7):1121–8.
Rettl R, Duca F, Binder C, Dachs TM, Cherouny B, Camuz Ligios L et al. Impact of tafamidis on myocardial strain in transthyretin amyloid cardiomyopathy. Amyloid. 2022:1–11.
Giblin GT, Cuddy SAM, Gonzalez-Lopez E, Sewell A, Murphy A, Dorbala S, et al. Effect of tafamidis on global longitudinal strain and myocardial work in transthyretin cardiac amyloidosis. Eur Heart J Cardiovasc Imaging. 2022;23(8):1029–39.
Rettl R, Mann C, Duca F, Dachs TM, Binder C, Ligios LC, et al. Tafamidis treatment delays structural and functional changes of the left ventricle in patients with transthyretin amyloid cardiomyopathy. Eur Heart J Cardiovasc Imaging. 2022;23(6):767–80.
Wu YA, Tsai CH, Su MY, Chao CC, Cheng MF, Shun CT et al. Reverse cardiac remodelling and dysfunction in A97S transthyretin cardiac amyloidosis after tafamidis treatment. ESC Heart Fail. 2022.
Yagi S, Yamazaki H, Kusunose K, Osaki Y, Ise T, Kadota M, et al. Regression of left ventricular hypertrophy after tafamidis therapy in a patient with transthyretin amyloidosis variant. J Med Invest. 2022;69(34):320–2.
Shintani Y, Okada A, Morita Y, Hamatani Y, Amano M, Takahama H, et al. Monitoring treatment response to tafamidis by serial native T1 and extracellular volume in transthyretin amyloid cardiomyopathy. ESC Heart Fail. 2019;6(1):232–6.
Chamling B, Bietenbeck M, Korthals D, Drakos S, Vehof V, Stalling P et al. Therapeutic value of tafamidis in patients with wild-type transthyretin amyloidosis (ATTRwt) with cardiomyopathy based on cardiovascular magnetic resonance (CMR) imaging. Clin Res Cardiol. 2022.
Lin YH, Hsueh HW, Su MY, Cheng MF, Chiang MC, Juang JJ, et al. Cardiomyopathy correlates to nerve damage in p.A117S late-onset transthyretin amyloid polyneuropathy. Ann Clin Transl Neurol. 2022;9(9):1359–69.
Griffin JM, Rosenthal JL, Grodin JL, Maurer MS, Grogan M, Cheng RK. ATTR Amyloidosis: current and emerging management strategies: JACC: CardioOncology State-of-the-art review. JACC CardioOncol. 2021;3(4):488–505.
Palmiero G, Vetrano E, Rubino M, Monda E, Dongiglio F, Lioncino M, et al. The role of New Imaging Technologies in the diagnosis of Cardiac Amyloidosis. Heart Fail Clin. 2022;18(1):61–72.
Dorbala S, Ando Y, Bokhari S, Dispenzieri A, Falk RH, Ferrari VA, ASNC/AHA/ASE/EANM/HFSA, et al. /ISA/SCMR/SNMMI Expert Consensus Recommendations for Multimodality Imaging in Cardiac Amyloidosis: part 1 of 2-Evidence base and standardized methods of imaging. Circ Cardiovasc Imaging. 2021;14(7):e000029.
Martinez-Naharro A, Kotecha T, Norrington K, Boldrini M, Rezk T, Quarta C, et al. Native T1 and extracellular volume in Transthyretin Amyloidosis. JACC Cardiovasc Imaging. 2019;12(5):810–9.
Acknowledgements
We thank Yih-Hwen Huang, Yi-Chieh Chen and Ting-Yen Lee for technical support during the study.
Funding
None.
Author information
Authors and Affiliations
Contributions
YHL, MYS and CCC contributed to the conception and design of the study. CCC, STH, ALY, YKW, MFC, MJL, CHC, CTS, HHH. JMJ and PHT collected the data. CHT and MYS performed the analysis and interpretation of the data. CHT, MYS and YHL drafted the manuscript and all authors revised it for intellectual content. All authors read and approved the completed manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All participants provided written informed consent to take part in the study.
Consent for publication
Not applicable.
Competing interests
None.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tsai, CH., Chao, CC., Hsieh, ST. et al. Tafamidis decreased cardiac amyloidosis deposition in patients with Ala97Ser hereditary transthyretin cardiomyopathy: a 12-month follow-up cohort study. Orphanet J Rare Dis 18, 289 (2023). https://doi.org/10.1186/s13023-023-02824-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13023-023-02824-0