
Abstract
Background
Rare diseases present a challenge to guideline implementation due to a low prevalence in the general population and the unfamiliarity of healthcare professionals. Existing literature in more common diseases references barriers and facilitators to guideline implementation. This systematic review aims to identify these barriers and facilitators in rare diseases from existing literature.
Methods
A multi-stage strategy included searching MEDLINE PubMed, EMBASE Ovid, Web of Science and Cochrane library from the earliest date available to April 2021, Orphanet journal hand-search, a pearl-growing strategy from a primary source and reference/citation search was performed. The Integrated Checklist of Determinants of Practice which comprises of twelve checklists and taxonomies, informed by 57 potential determinants was selected as a screening tool to identify determinants that warrant further in-depth investigation to inform design of future implementation strategies.
Results
Forty-four studies were included, most of which were conducted in the United States (54.5%). There were 168 barriers across 36 determinants (37 studies) and 52 facilitators across 22 determinants (22 studies). Fifteen diseases were included across eight WHO ICD-11 disease categories. Together individual health professional factors and guideline factors formed the majority of the reported determinants (59.5% of barriers and 53.8% of facilitators). Overall, the three most reported individual barriers were the awareness/familiarity with the recommendation, domain knowledge and feasibility. The three most reported individual facilitators were awareness/familiarity with the recommendation, agreement with the recommendation and ability to readily access the guidelines. Resource barriers to implementation included technology costs, ancillary staff costs and more cost-effective alternatives. There was a paucity of studies reporting influential people, patient advocacy groups or opinion leaders, or organisational factors influencing implementation.
Conclusions
Key barriers and facilitators to the implementation of clinical practice guidelines in the setting of rare diseases were at the individual health professional and guideline level. Influential people and organisational factors were relatively under-reported and warrant exploration, as does increasing the ability to access the guidelines as a potential intervention.
Similar content being viewed by others


Background and objectives
Although rare diseases are individually rare, they are collectively common with an estimated global prevalence of 263–446 million people across 6000–7000 diseases [1, 2]. While a proportion of rare diseases have no accepted medical technologies, others have expensive therapeutic options with varying levels of evidence due to participant factors including small sample sizes leading to uncertainty, geographical dispersion and disease heterogeneity [3, 4]. Despite this, nearly six hundred orphan technologies to treat rare diseases have been approved by the Food and Drug Association in the US between 1983 and July 2020 with 552 on the market at the time of the NORD study [5]. A third of National Institute for Health and Clinical Excellence (NICE) approved technologies are for rare diseases [6]. These technologies have resulted in associated clinical practice guidelines, summarising up-to-date evidence and expert opinion leading to structured and practical recommendations to support decision making as prioritised by the World Health Organisation [4, 7].
The development and implementation of guidelines for rare diseases presents a greater challenge compared to more common diseases. This is related to limited health professional knowledge and experience in caring for those with specific rare diseases due to low disease prevalence [8]. These factors may lead to guideline adherence worse than the 30–70% non-adherence to guidelines reported in non-rare disease areas [9,10,11,12]. Frequently identified factors in existing systematic reviews for non-rare diseases include health professional level factors, a lack of knowledge [13], awareness of guidelines [13,14,15] and agreement with recommendations [13, 15]. Influencing factors at the organisational level include the absence of leadership/senior support [13, 16, 17], difficulties with teamwork [13, 17], disagreements with colleagues [13, 14] and insufficient communication [13].
Although there is a growing number of guidelines being published to inform the use of medical technologies for rare diseases, there is a paucity of systematic reviews or guidance on addressing the barriers and facilitators to the implementation of these recommendations in clinical practice [6, 18,19,20]. Such research is essential to ensure that people with rare diseases receive equitable high-quality healthcare. In this review, we aim to systematically identify and synthesise the factors influencing the implementation of clinical practice guidelines (CPGs) in the rare diseases setting. This will enable more informed development, implementation and evaluation of guidelines as well as the development of targeted interventions to improve implementation.
Research design and methods
Study design
We conducted a systematic review according to the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement. The study was registered on PROSPERO (CRD42021256061) then a protocol developed and published.
Studies were eligible for inclusion if they explored barriers and/or facilitators to the implementation of guidelines or consensus documents for rare diseases. Determinants of healthcare professional practice can be described as being factors that might prevent (barrier) or enable (facilitator) improvements in healthcare practice [21].
The European Union definition of a rare disease affecting less than 1 person per 2000 was used with prevalence confirmed on the Orphanet website [22]. Oncological rare diseases were excluded as they are predominantly managed by the oncology specialists rather than the related disease area. No restrictions were placed on the research design or publication date. As the study focuses on NICE technology appraisal guidance predominantly the results of the search strategy have been restricted to the English language. An overview of the inclusion and exclusion criteria is included in Table 1.
Search strategy
A comprehensive search strategy, including database and supplementary techniques, was developed to maximise recall and reduce publication bias. An additional file includes the complete search strategy [see Additional file 1].
Search strategy stages:
-
Stage 1: Rare diseases search
-
Stage 2: NICE specialised technology appraisal search
-
Stage 3: Orphanet Journal hand-search 28/02/17-28/02/21
-
Stage 4: Pearl-growing subject search [23] from Denger et al. [24]
-
Stage 5: Supplementary searches – grey literature, citations and references
Rare diseases search
The search strategy was developed using the SPIDER framework to identify studies with the expected study design, qualitative and mixed-methods (Table 2) [25]. Databases searched include MEDLINE via PubMed, EMBASE via Ovid, Web of Science and Cochrane Library from inception to April 2021.
NICE specialised technology appraisal search
NICE is an executive non-departmental public body of the Department of Health and Social Care in England and Wales that provides national guidance and advice to improve health and social care [26]. Published NICE guidelines and technology appraisals mandate the availability of technologies to people with rare diseases in England and Wales within three months, making their adoption in clinical practice less equivocal [27]. Furthermore, as the pharmaceutical industry often targets NICE first, then the rest of Europe, these approved medical technologies are likely to have generated the most peer reviewed literature.
Published NICE technology appraisal guidance (TAG) and highly specialised technologies guidance documents were reviewed to identify non-oncological rare diseases with existing guidance on 27/02/2021 [6]. Twenty-nine current guidance documents were identified in twenty-four rare diseases as shown in Fig. 1 which were incorporated into the search strategy from the “Rare disease search”. An additional file includes the rare diseases identified [see Additional file 2]. As in the rare disease search, the database search included PubMed MEDLINE, Ovid EMBASE, Web of Science and Cochrane Library from inception to April 2021.

NICE technology appraisals to identify rare diseases with existing technology appraisal guidance
Orphanet Journal hand-search
A hand-search of the Orphanet Journal was implemented to locate studies that may not be found through traditional searches including those that may be unindexed in databases or informal publications [28, 29]. The Orphanet journal was selected for its high impact factor, relevance to the subject of the study, and publication of guidelines and conference proceedings on rare diseases. This involved a manual examination of the contents of the Orphanet journal editions between 28/02/17 to 28/02/21 by MG and JF. Five years was selected as the timescale as 75.9% of NICE technology appraisal guidance documents, we identified in the previously mentioned rare disease search, for non-oncological rare diseases were published between 2016 and 2020 [See Additional file 2]. Furthermore, the median time for the production of guidance for a NICE single technology appraisal is 48 weeks [30]. Thus, the results from journal issues for the preceding five years when the search was undertaken in February 2021 should account for the time for NICE technology appraisal guidance publication, development and research into implementation in clinical practice.
Pearl-growing subject search
Through the “Rare disease search” we identified a primary manuscript published by Denger et al. (2019) that explored the barriers and facilitators to guideline adherence for a specific rare disease, Duchenne’s Muscular Dystrophy [24]. We developed a subject pearl-growing strategy using the Medical Subject Headings (MeSH) terms indexed for the study published by Denger et al. (2019). The MeSH term (guideline adherence*) was combined with the non-oncological rare diseases identified to have current NICE TA guidelines to search PubMed MEDLINE i.e. (rare disease) AND (guideline adherence*). The decision for the pragmatic search using PubMed Medline was suitable due to the comprehensiveness of the overall search strategy and the specificity of MeSH terms.
Supplementary searches
Grey literature was obtained through discussion with the NICE Health Technology Adoption team who support the uptake of new technologies recommended by NICE through system learning based on usage and clinical engagement data. Data sources were sought from this group given their experience in engaging with our stakeholders as well as the identification of obstacles and solutions to technology adoption in clinical practice. An additional file includes the grey literature provided [see Additional file 1].
References and citations of all included studies were hand-searched and assessed for suitability for inclusion with repeated cycles until no further studies were identified.
Study selection and data extraction
Following the elimination of duplicates, two reviewers (MG and JF) reviewed the titles and abstracts according to the inclusion criteria. The full-text review was conducted by two independent reviewers (MG and JC) with any disagreements resolved through discussion and a consensus reached. Reasons for exclusion were recorded on the data extraction template.
Data extraction was developed by reviewers then piloted and undertaken. Information included authors, publication year, database ID, location, ICD-11 disease category, study design, type of participant and number of responses.
Quality assessment
To ensure transparency, all included studies were appraised using best practice quality appraisal tools relevant to their specific research design, Table 3. All appraisals were conducted by MG and verified by JF.
Data analysis and synthesis
Thematic analysis was performed using the Integrated Checklist of Determinants of Practice as this framework was specifically developed for healthcare improvement [21]. The checklist was formed through the aggregation of the components from twelve existing checklists, frameworks and taxonomies for chronic diseases which were identified through a systematic review process. It consists of fifty-seven determinants grouped into seven domains (guideline factors, individual health professional factors, patient factors, professional interactions, incentives and resources, capacity for organisational change, and social, political and legal factors). The determinants can be interpretated as barriers or facilitators and are sufficiently diverse and detailed to encompass factors identified in the included studies. Due to the heterogeneity of questions and study design, statistical aggregation was not appropriate.
Results
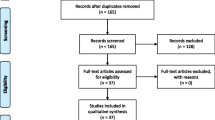
After eliminating duplicates 7548 titles were identified. 158 studies were selected for full-text review and 44 were included in the thematic synthesis (using the determinants of practice in the ICDP framework). The PRISMA flow chart summarising the review process is in Fig. 2. [31] Additional files show the full multi-stage PRISMA flow chart [see Additional file 3] and the studies excluded at the full-text stage [see Additional file 4].

PRISMA flow chart
Most included studies were conducted in the United States (54.5%) with the remaining studies being multi-national or from countries with a high Human Development Index [32]. Publication dates ranged from 1995 to 2021 (median 2016) with an increasing trend in publication rate when studies from 2020 and 2021 were excluded (overall reduction in research due to COVID-19 pandemic). There were fifteen rare diseases across eight WHO ICD-11 categories [33] in the included studies with diseases of the immune system accounting for a quarter (Table 4). An overview of the included studies is available as an additional file [see Additional file 5].
Five studies (11.4%) included interviews or focus groups in their design compared to thirty-three studies (75.0%) that incorporated questionnaires or surveys. Most studies reported the perceptions or experiences of respondents (n = 35, 79.5%) rather than retrospective chart review (n = 6, 13.6%) or expert opinion (n = 3, 6.8%). Non-highly specialised health professionals were the most common respondent type (n = 21) compared to highly specialised health professionals (n = 14) and non-health professionals (n = 5). An additional file has the full description of the included studies [see Additional file 5]. Studies rated as having a higher risk of bias in their specific quality appraisal tool were only included where their identified determinants of practice were supported by other studies included in the review with a low risk of bias. An additional file includes further details of the quality assessment [see Additional file 6].
Determinants of practice – barriers and facilitators
In accordance with the definitions used by the ICDP, determinants are considered barriers if their presence impedes the implementation of or adherence to rare disease guideline(s). In contrast, they are considered facilitators if their presence promotes the implementation of or adherence to the rare disease guideline(s) [16]. We considered a determinant as neutral when it could be interpreted as having a positive or negative impact.
The data synthesis produced 168 examples of reported barriers from 37 studies corresponding to 36 determinants in the ICDP and 52 examples of reported facilitators from 22 studies corresponding to 22 determinants in the ICDP. Figure 3 and Table 5 summarise identified factors with a comprehensive analysis in additional files [see Additional files 7 and 8].

Stacked bar chart of barriers, facilitators and neutral determinants across the seven determinants of the ICDP
The individual health professional factors domain was the most prevalent domain. Awareness and familiarity with the recommendation (determinant 2.1.2) was the most reported individual determinant of practice (Table 6). An additional file includes the contribution of individual studies to the determinants of practice [see Additional file 9].
Guideline factors
The quality of evidence, clarity and feasibility of the recommendation were the highest reported determinants in this domain potentially limiting the implementation of guidelines in the included studies. This included a lack of sufficient evidence [24, 34,35,36,37,38] and dependence on expert opinion [39]. Clarity of guideline recommendations was considered to facilitate implementation through avoidance of jargon, lengthy and text-heavy guidance [35, 40], and clear indications for initiation [36, 38]. The included studies reported difficulties retrieving guidelines [41,42,43], poor dissemination [44] and insufficient translation to other languages [41].
Feasibility of recommendations influences the likelihood of implementation through as less feasible recommendations are perceived to require more time to implement [44,45,46,47] and less convenient for both patients and healthcare professionals [48, 49]. This may be related to perceived suitability of recommendations for healthcare in practice [24, 37, 40, 44, 50] and adaptability of the recommendations to different healthcare systems [36, 44]. The accessibility of recommended interventions also presents an obstacle to implementation requiring sufficient technology access/fluency [40, 50], access to investigations [42, 51] and alternatives being more accessible/feasible [46, 52].
Supporting information technology was cited as a facilitator to implementation of guidance by three studies through the use of mobile apps [53], guidelines applications [40] and electronic medical records [54]. Insufficient digital resources impair guideline dissemination leading to under-utilisation [55]. Systems tracking prescribing adherence may also improve adherence to recommended interventions and the quality of care delivered to patients [56].
Individual health professional factors
Awareness and familiarity with the recommendations were reported to influence implementation in a large number of included studies [34, 36, 38,39,40, 42,43,44,45, 50, 51, 53,54,55, 57,58,59,60,61,62,63,64,65,66]. This was present in studies involving highly specialised health professionals (n = 6, 13.6%) as well as non-highly specialised health professionals (n = 22, 50%). All non-highly specialised health professionals were trained in the same disease area or could be expected to implement the recommendations for rare disease patients. Low frequency of encountering patients with the specific rare disease was reported as a potential reason for limited awareness/familiarity [24, 39]. Some studies included suggestions to improve awareness including education [43, 59], inaccessibility [53], regional network and awareness campaigns [42].
Health professionals’ knowledge in the rare disease subject area (domain knowledge) limited the implementation of recommendations in many studies [24, 36, 43, 44, 47, 48, 50, 54, 56,57,58, 61, 67,68,69,70]. Domain knowledge is recognised as important in the management of patients, awareness of the guidance and recognition of their importance [24, 54]. Other aspects of knowledge and skills required for guideline implementation included the lack of specific training [24, 37, 47, 67], dedicated education sessions or materials [50, 56, 69] and associated skills [36, 38]. Unsurprisingly there was a reported difference between different types of healthcare professionals with highly specialised health professionals having greater knowledge of treatment options and guidelines when compared to broader clinical experience such as primary care physicians [46, 61, 66, 70]. Furthermore, general experience as a healthcare professional and specifically experience managing patients with the rare disease in question were considered as a positive factor leading to increased adherence to guidelines [24, 48, 49, 58, 67].
The perception of guidelines by health professionals may explain some variation in practice through the agreement with using guidelines in clinical practice [36, 43] or agreement with the specific recommendations [36, 38, 39, 43, 44, 46, 51, 55, 60, 61, 71, 72]. Outcome expectancy impaired the implementation when it was perceived that the recommendation would not affect patient outcomes [38, 39, 55] or that health professionals anticipated poor patient compliance [55, 61], expected adverse outcomes [67] or that recommendations may cause anxiety to patients [46]. Attitudes and emotions of health professionals were found to negatively affect adherence to recommendations in Sickle Cell Disease (SCD) care related to perceived opiate-seeking behaviour [34, 67, 73].
Health professional self-reported capability (efficacy) in managing patients with a rare disease limited implementation, non-rare disease specialists feel unable to provide care [53], adhere to recommendations [43] or interpret outcomes of recommendations [55]. This is potentially coupled with professionals’ failure or delays in prescribing recommended therapies [61].
Patient factors
Patient needs or demands of their healthcare providers were reported to potentially influence guideline implementation. These factors included the home-to-clinic distance for patients [45], perceived additional costs to patients [39, 67] and unrealistic patient expectations [37]. Some studies suggested that implementation of recommendations could be supported through recognising patient needs and developing guidelines in a patient-centred method [24, 44, 54].
Patient knowledge and beliefs were recognised as a barrier through patients being unaware of the need to attend for recommended interventions [74]. Patient and caregiver unawareness of the guidelines or disease knowledge was identified as a factor that may limit their engagement and potentially impede guideline implementation [24, 40, 44, 45, 47].
Patient preferences for the location of their care [24], patient-focussed priorities [24, 37, 46] and avoidance of additional treatment burden [36] were reported to limit the implementation of some recommendations. This could manifest in an “adversarial” manner through poor medication adherence [36, 67, 73] or low outpatient attendance [39, 67]. This could be in part related to unvoiced disagreements with the healthcare professionals responsible for their care [40]. However, engaged patients or relatives can make implementation of recommendations easier and reduce social stigma [24, 56]. In fact, McPhail et al. (2010) recommend sharing the guidelines with patients and their families to empower them and improve adherence to guidance in the chronic care setting [56]. Denger et al. (2019) suggest that patients adhering to recommendations may encourage other patients with the same disease to adhere to recommendations as a form of peer pressure. They also propose that recommendations that do not interfere with patients’ everyday life are more likely to have better adherence [24]. Interpersonal relationships between health professionals and patients/caregivers have been suggested to influence patients’ motivation and willingness to participate in care [75]. A patient’s motivation could then impede implementation for example people with SCD have described being demotivated to attend hospital for fear of being perceived to be drug-seeking and facing potential discrimination [67, 73].
Professional interactions
Some studies described poor communication and coordination between primary and secondary care potentially impeding the implementation of recommendations [45, 47, 53, 54, 75]. These findings contrast those of Heutinck et al. (2021) who reported that surveyed physicians were satisfied with the inter-professional communication about Duchenne Muscular Dystrophy patient care although reasons for this outlying study were not explored further [39]. Referral processes were believed to be underlie some of these inter-professional communication difficulties including practical difficulties [54], lack of awareness of processes [57] or insufficient information on referrals [52]. Other authors have supported this by reporting that good referral pathways improve the care of patients with rare diseases, guideline adherence and the education of non-specialists healthcare professionals [50, 73, 75].
Financial incentives and resources
Availability of resources and financial disincentives were found to impair guideline implementation. Specific reasons for the reduced availability of necessary resources and financial considerations included unavailable/insufficient therapies [39, 42, 49, 75], health technology costs for the recommended intervention [24, 46, 75], inappropriate clinical spaces/schedules [45, 55], ancillary staff costs [39, 45], general costs [24, 36] and inadequate time [39, 45, 54]. More cost-effective alternative preparations may also impede adherence to recommendations in guidelines [47]. Utrankar et al. (2018) suggest financial incentives or penalties can improve the completion of guideline-derived objectives [40]. Insufficient support staff was believed to impair the ability of clinicians to comply with recommendations through poor coordination [39] and resource management [43].
Capacity for organisational change
The capacity for organisational change was not a feature of the included studies. This could be related to the predominantly patient or health professional focus of these studies which would not involve in-depth assessment of organisational factors.
Social, political and legal factors
The main hurdles described by the studies at the social, political and legal level were costs and payer or funder policies. Economic constraints can influence the funds available for recommended treatments [75, 76], dosage prescribed [76], ancillary staff [45], capacity of services [39] and overall ability to adhere to recommendations [24, 36, 48, 49, 75]. Proposed mechanisms for payer or funder policies influencing guideline implementation included insufficient insurance coverage [48, 49, 67, 69] and difficulties obtaining reimbursement [36, 44, 56, 69]. Masese et al. (2019) described respondents believing that their ability to deliver good care was not influenced by insufficient insurance coverage. However, they did not specifically enquire about whether it influenced their ability to follow recommendations or patients’ behaviours [54].
There were limited descriptions of influential people in the studies. Banerji et al. (2016) acknowledge the role of patient advocacy groups and patient representatives in improving the uptake of recommendations from guidelines for patients with hereditary angioedema [50]. Behr (2016) recognises “powerful personalities or groups” as potentially supporting evidenced-based guidance as well as mis-information or over-information illustrating that the involvement of influential people is not always positive [35].
Both patient groups and opinion leaders and patient groups have been recognised as having a role in guideline implementation for more common diseases [77, 78].
Discussion
This systematic review identified, quality appraised and synthesised forty-four studies assessing factors influencing clinical practice guideline implementation. There has been increased publication of studies assessing guideline implementation over the last twenty years prior to the COVID-19 pandemic. Like others, we found that the most frequently cited barriers were at the level of the individual health professional [13,14,15, 77], with the awareness and familiarity of health professionals being the most common barrier. Although rare diseases are often considered the sole domain of healthcare professionals with highly-specialised expertise [79], our review identified that the majority of research had been performed in non-specialists. There are often only a handful of specialists in a country, or even worldwide, who have expertise in a given rare condition [80,81,82]. A National Organization for Rare Diseases survey in 2020 showed that 20% of respondents were not being managed by a specialist [82], which has previously been associated with inappropriate treatment and worse patient outcomes [83,84,85]. This is may be explained through recognised difficulties in non-highly specialised health professionals gaining adequate experience due to low patient prevalence [86]. These factors are also frequently recognised by many rare disease organisation strategies including the UK Rare Diseases Framework [87], EURODIS: Recommendations from the Rare 2030 Foresight Study [88], Canada’s Rare Disease Strategy [89] and the Australian National Strategic Action Plan for Rare Diseases [90].
Our study identified feasibility of guideline implementation as a barrier, and it has been noted that national guidelines often lack details of the applicability and description of the changes needed to apply recommendations [91,92,93]. The customisation of clinical practice guidelines to particular organisations or healthcare systems is already in practice for the management of cancer in France [94], and may lead to better adherence and outcomes. Our study also found health professionals’ anticipated poor adherence to therapies by the patient, which has been shown to be lowest in patients who were asymptomatic and younger [95], is associated with worse outcomes and increased healthcare costs [96], and can be improved by enhancing social support from healthcare professional and providers [97, 98]. Medication adherence is important due to the risk of worsening disease, death and increased health care costs.
Although, key opinion leaders and influential people have a role in the development of new technologies, and the development and adherence to new policies and guidelines [99], we found a paucity of them in our included studies. An opinion leader who is an individual that is perceived as credible, trustworthy and able to exert influence on others’ decision-making [100]. In the wider healthcare setting, opinion leaders are been proposed to improve health professionals’ familiarity, knowledge and compliance to recommendations and knowledge [77, 101]. Furthermore, opinion leaders have been considered as an effective strategy for the implementation of research findings in specialised areas such as rare diseases [102].
Strengths and limitations
The strengths of this review include the aggregation of determinants of practice from different regions, healthcare settings and rare diseases supporting the generalisability of findings. However, it is important to recognise the limitations of this approach as it may be difficult to incorporate all findings into the classification of the framework. For example, it is not possible to incorporate any factors that may encompass social influence principles such as social proof or commitment [103].
Barriers and facilitators examined were to recommendations from the NICE organisation, based in England & Wales, and other international organisations publishing guidelines for use the care of people with rare diseases. Synthesis was supported by a range of existing systematically developed, validated and peer-reviewed tools.
Recommendations for clinical practice and future research
Future guidelines should involve key opinion leaders, patient advocacy groups and people with the rare disease, and consider modifying any relevant specific determinants of practice that recommendations could be affected by. This could be achieved through modelling a single disease to produce contextually appropriate targets and sustained change.
Deeper understanding of the factors influencing guideline implementation for rare diseases could be achieved by future studies focussing on underlying theoretical principles such as social proof, commitment, self-efficacy, outcome expectations and other beliefs, and may be achieved using ethnographic research [104,105,106]. Only used by five studies in our review, there are limitations to ethnographic approaches in the study of rare diseases due to a limited number of potential participants (patients and healthcare professionals), perceived high cost and a potential lack of generalisable findings [107]. However, the concept of generalisability itself has been argued by some researchers to not be the purpose of qualitative research with a greater focus on depth of understanding within a study’s specific context [108].
Conclusions
In this review we identified forty-four studies focusing on the barriers and facilitators to guideline implementation in the rare disease setting. All the studies included were from countries with a higher human development index. It combines findings from both highly specialised and non-highly specialised health professionals. The synthesis included 168 reported barriers and 52 reported facilitators with the individual health professionals domain being the most common. Influential people as a facilitator for guideline implementation was surprisingly absent given the role of this stakeholder in other aspects of rare disease guideline development and research. Capacity for organisational change was relatively under-reported which may be related to the limited number of ethnographic studies in the literature available. Future research and guideline implementation strategies should focus on the most commonly reported determinants in this study.
Availability of data and materials
All data generated or analysed during this stage are included in this published article [and its Additional files].
Abbreviations
- CPG:
-
Clinical Practice Guideline
- ICDP:
-
Integrated Checklist of Determinants of Practice
- NICE:
-
National Institute for Health and Care Excellence
- NORD:
-
National Organization for Rare Diseases
- PAGs:
-
Patient Advocacy Groups
- RDCRN:
-
Rare Disease Care Research Network
- SCD:
-
Sickle Cell Disease
- TA:
-
Technology Appraisal
- TA:
-
Technology Appraisal Guidance
- WHO:
-
World Health Organisation
References
Nguengang Wakap S, Lambert DM, Olry A, Rodwell C, Gueydan C, Lanneau V, et al. Estimating cumulative point prevalence of rare diseases: analysis of the Orphanet database. Eur J Hum Genet. 2020;28(2):165–73.
Haendel M, Vasilevsky N, Unni D, Bologa C, Harris N, Rehm H, et al. How many rare diseases are there? Nat Rev Drug Discov. 2020;19(2):77–8.
Mitani AA, Haneuse S. Small Data Challenges of Studying Rare Diseases. JAMA Netw Open. 2020;3(3): e201965.
Pai M, Yeung CHT, Akl EA, Darzi A, Hillis C, Legault K, et al. Strategies for eliciting and synthesizing evidence for guidelines in rare diseases. BMC Med Res Methodol. 2019;19(1):67.
National Organization for Rare Disorders. Orphan Drugs in the United States: An examination of patents and orphan drug exclusivity. 2021.
National Institute for Health and Care Excellence. Guidance, NICE advice and quality standards. 2022.
World Health Organisation. A Public Health Approach to Innovation - Background Paper Rare Diseases. 2013. p. 1–46.
Stoller JK. The challenge of rare diseases. Chest. 2018;153(6):1309–14.
Chen Y, Sloan FA, Yashkin AP. Adherence to diabetes guidelines for screening, physical activity and medication and onset of complications and death. J Diabetes Complications. 2015;29(8):1228–33.
Drenth-van Maanen AC, van Marum RJ, Jansen PA, Zwart JE, van Solinge WW, Egberts TC. Adherence with dosing guideline in patients with impaired renal function at hospital discharge. PLoS ONE. 2015;10(6): e0128237.
van den Bemt PM, Chaaouit N, van Lieshout EM, Verhofstad MH. Noncompliance with guidelines on proton pump inhibitor prescription as gastroprotection in hospitalized surgical patients who are prescribed NSAIDs. Eur J Gastroenterol Hepatol. 2016;28(8):857–62.
Bos JM, Natsch S, van den Bemt P, Pot JLW, Nagtegaal JE, Wieringa A, et al. A multifaceted intervention to reduce guideline non-adherence among prescribing physicians in Dutch hospitals. Int J Clin Pharm. 2017;39(6):1211–9.
Correa VC, Lugo-Agudelo LH, Aguirre-Acevedo DC, Contreras JAP, Borrero AMP, Patino-Lugo DF, et al. Individual, health system, and contextual barriers and facilitators for the implementation of clinical practice guidelines: a systematic metareview. Health Res Policy Syst. 2020;18(1):74.
Paksaite P, Crosskey J, Sula E, West C, Watson M. A systematic review using the Theoretical Domains Framework to identify barriers and facilitators to the adoption of prescribing guidelines. Int J Pharm Pract. 2021;29(1):3–11.
Almazrou SH, Alfaifi SI, Alfaifi SH, Hakami LE, Al-Aqeel SA. Barriers to and facilitators of adherence to clinical practice guidelines in the Middle East and North Africa Region: a systematic review. Healthcare (Basel). 2020;8(4):564.
Bach-Mortensen AM, Lange BCL, Montgomery P. Barriers and facilitators to implementing evidence-based interventions among third sector organisations: a systematic review. Implement Sci. 2018;13(1):103.
McArthur C, Bai Y, Hewston P, Giangregorio L, Straus S, Papaioannou A. Barriers and facilitators to implementing evidence-based guidelines in long-term care: a qualitative evidence synthesis. Implement Sci. 2021;16(1):70.
Kirschner J, et al. How reference networks develop, implement, and monitor guidelines. Orphanet J Rare Dis. 2012;7:1–14.
Sejersen T, et al. Methodology for production of best practice guidelines for rare diseases. Rare Dis Orphan Drugs. 2014;1:10–9.
Henter JI, et al. Clinical guidelines and practices: examples from international collaboration in clinical practice. Rare Dis Orphan Drugs. 2012;1:14.
Flottorp SA, Oxman AD, Krause J, Musila NR, Wensing M, Godycki-Cwirko M, et al. A checklist for identifying determinants of practice: a systematic review and synthesis of frameworks and taxonomies of factors that prevent or enable improvements in healthcare professional practice. Implement Sci. 2013;8:35.
European Union. Regulation (EC) No 141/2000 of the European Parliament and of the council. Official Journal of the European Communities 18: European Parliament and of the Council; 1999.
University of Auckland. What is pearl growing? 2010 [Available from: https://flexiblelearning.auckland.ac.nz/philson/37.html.
Denger B, Kinnett K, Martin A, Grant S, Armstrong C, Khodyakov D. Patient and caregiver perspectives on guideline adherence: the case of endocrine and bone health recommendations for Duchenne muscular dystrophy. Orphanet J Rare Dis. 2019;14(1):205.
Cooke A, Smith D, Booth A. Beyond PICO: the SPIDER tool for qualitative evidence synthesis. Qual Health Res. 2012;22(10):1435–43.
National Institute for Health and Care Excellence. About 2022 [Available from: https://www.nice.org.uk/about.
National Institute for Health and Care Excellence. Guide to the processes of technology appraisal. 2018.
Richards D. Handsearching still a valuable element of the systematic review. Evid Based Dent. 2008;9(3):85.
Hopewell S, Clarke M, Lefebvre C, Scherer R. Handsearching versus electronic searching to identify reports of randomized trials. Cochrane Database Syst Rev. 2007;2007(2):MR000001.
Casson SGRF, Miners A. How long has NICE taken to produce Technology Appraisal guidance? A retrospective study to estimate predictors of time to guidance. BMJ Open. 2013;3:e001870.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Rev Esp Cardiol (Engl Ed). 2021;74(9):790–9.
United Nations Development Programme. Human Development Reports. 2022.
World Health Organization. ICD-11: International Classification of Diseases 11th Revision. 2022.
Glassberg JA, Tanabe P, Chow A, Harper K, Haywood C Jr, DeBaun MR, et al. Emergency provider analgesic practices and attitudes toward patients with sickle cell disease. Ann Emerg Med. 2013;62(4):293-302.e10.
Behr J. Guidelines or guidance for better idiopathic pulmonary fibrosis management? BMC Med. 2016;14:24.
Glauser TA, Nevins PH, Williamson JC, Abdolrasulnia M, Salinas GD, Zhang J, et al. Adherence to the 2007 cystic fibrosis pulmonary guidelines: a national survey of CF care centers. Pediatr Pulmonol. 2012;47(5):434–40.
Akiyama N, Fujisawa T, Morita T, Mori K, Yasui H, Hozumi H, et al. Palliative care for idiopathic pulmonary fibrosis patients: pulmonary physicians’ view. J Pain Symptom Manag. 2020;60(5):933–40.
Hernandez-Trujillo HS, Chapel H, Lo Re V 3rd, Notarangelo LD, Gathmann B, Grimbacher B, et al. Comparison of American and European practices in the management of patients with primary immunodeficiencies. Clin Exp Immunol. 2012;169(1):57–69.
Heutinck L, van Gameren M, Verschuuren J, Geurts ACH, Jansen M, de Groot IJM. Clinical management of duchenne muscular dystrophy in the Netherlands: barriers to and proposals for the implementation of the international clinical practice guidelines. J Neuromuscul Dis. 2021;8(4):503–12.
Utrankar A, Mayo-Gamble TL, Allen W, Novak L, Kassim AA, Bonnet K, et al. Technology use and preferences to support clinical practice guideline awareness and adherence in individuals with sickle cell disease. J Am Med Inform Assoc. 2018;25(8):976–88.
Pavan S, Rommel K, Mateo Marquina ME, Hohn S, Lanneau V, Rath A. Clinical practice guidelines for rare diseases: the orphanet database. PLoS ONE. 2017;12(1): e0170365.
Haberle J, Huemer M. Evaluation of implementation, adaptation and use of the recently proposed urea cycle disorders guidelines. JIMD Rep. 2015;21:65–70.
Garber E, Desai M, Zhou J, Alba L, Angst D, Cabana M, et al. Barriers to adherence to cystic fibrosis infection control guidelines. Pediatr Pulmonol. 2008;43(9):900–7.
Talarico R, Marinello D, Bombardieri S, Burmester G, Fonseca J, Frank C, et al. Clinical practice guidelines adherence, knowledge and awareness in rare and complex connective tissue diseases across Europe: results from the first ERN ReCONNET survey. RMD Open. 2020;6(2):e001344.
Conway K, Trout C, Westfield C, Fox D, Pandya S. A pilot survey study of adherence to care considerations for duchenne muscular dystrophy. PLoS Curr. 2018;2018:10.
Corrigan M, Hirschfield G, Greenfield S, Parry J. Barriers to implementation of stratified care in primary biliary cholangitis: a scoping exercise. BMJ Open Gastroenterol. 2019;6(1): e000226.
Spickett GP, Askew T, Chapel HM. Management of primary antibody deficiency by consultant immunologists in the United Kingdom: a paradigm for other rare diseases. Qual Health Care. 1995;4(4):263–8.
Riedl MA, Banerji A, Gower R. Current medical management of hereditary angioedema: follow-up survey of US physicians. J Allergy Clin Immunol Pract. 2015;3(2):220–7.
Riedl MA, Banerji A, Gower R. Current medical management of hereditary angioedema: follow-up survey of US physicians. Ann Allergy Asthma Immunol. 2021;126(3):264–72.
Banerji A, Bas M, Bernstein JA, Boccon-Gibod I, Bova M, Dempster J, et al. Expert perspectives on hereditary angioedema: Key areas for advancements in care across the patient journey. Allergy Rhinol (Providence). 2016;7(3):172–81.
Johnson S, Stojanovic J, Ariceta G, Bitzan M, Besbas N, Frieling M, et al. An audit analysis of a guideline for the investigation and initial therapy of diarrhea negative (atypical) hemolytic uremic syndrome. Pediatr Nephrol. 2014;29(10):1967–78.
Visser SK, Bye PTP, Fox GJ, Burr LD, Chang AB, Holmes-Liew CL, et al. Management of Australian adults with bronchiectasis in tertiary care: evidence-based or access-driven? Lung. 2019;197(6):803–10.
Lunyera J, Jonassaint C, Jonassaint J, Shah N. Attitudes of primary care physicians toward sickle cell disease care, guidelines, and comanaging hydroxyurea with a specialist. J Prim Care Community Health. 2017;8(1):37–40.
Masese RV, Bulgin D, Douglas C, Shah N, Tanabe P. Barriers and facilitators to care for individuals with sickle cell disease in central North Carolina: The emergency department providers’ perspective. PLoS ONE. 2019;14(5): e0216414.
Cabana MD, Kanter J, Marsh AM, Treadwell MJ, Rowland M, Stemmler P, et al. Barriers to pediatric sickle cell disease guideline recommendations. Glob Pediatr Health. 2019;6:2333794X19847026.
McPhail GL, Weiland J, Acton JD, Ednick M, Chima A, VanDyke R, et al. Improving evidence-based care in cystic fibrosis through quality improvement. Arch Pediatr Adolesc Med. 2010;164(10):957–60.
Maher TM, Molina-Molina M, Russell AM, Bonella F, Jouneau S, Ripamonti E, et al. Unmet needs in the treatment of idiopathic pulmonary fibrosis-insights from patient chart review in five European countries. BMC Pulm Med. 2017;17(1):124.
Orange JS, Seeborg FO, Boyle M, Scalchunes C, Hernandez-Trujillo V. Family physician perspectives on primary immunodeficiency diseases. Front Med (Lausanne). 2016;3:12.
Nguyen QD, Hatef E, Kayen B, Macahilig CP, Ibrahim M, Wang J, et al. A cross-sectional study of the current treatment patterns in noninfectious uveitis among specialists in the United States. Ophthalmology. 2011;118(1):184–90.
Peikert T, Daniels CE, Beebe TJ, Meyer KC, Ryu JH, Interstitial Lung Diseases Network of the American College of Chest P. Assessment of current practice in the diagnosis and therapy of idiopathic pulmonary fibrosis. Respir Med. 2008;102(9):1342–8.
Lanzkron S, Haywood C Jr, Hassell KL, Rand C. Provider barriers to hydroxyurea use in adults with sickle cell disease: a survey of the Sickle Cell Disease Adult Provider Network. J Natl Med Assoc. 2008;100(8):968–73.
Fu L, Kanani A, Lacuesta G, Waserman S, Betschel S. Canadian physician survey on the medical management of hereditary angioedema. Ann Allergy Asthma Immunol. 2018;121(5):598–603.
Robalo-Cordeiro C, Morais A. Translating Idiopathic pulmonary fibrosis guidelines into clinical practice. Pulmonology. 2021;27(1):7–13.
Cheung CS, Noordeh N, Gottlieb CC. A national survey of Canadian ophthalmologists to determine awareness of published guidelines for the management of uveitis. J Ophthalmic Inflamm Infect. 2016;6(1):38.
Moore BM, Laguna TA, Liu M, McNamara JJ. Increased adherence to CFF practice guidelines for pulmonary medications correlates with improved FEV1. Pediatr Pulmonol. 2013;48(8):747–53.
Wurst KE, Sleath BL. Physician knowledge and adherence to prescribing antibiotic prophylaxis for sickle cell disease. Int J Qual Health Care. 2004;16(3):245–51.
Fearon A, Marsh A, Kim J, Treadwell M. Pediatric residents’ perceived barriers to opioid use in sickle cell disease pain management. Pediatr Blood Cancer. 2019;66(2): e27535.
Riedl M, Gower RG, Chrvala CA. Current medical management of hereditary angioedema: results from a large survey of US physicians. Ann Allergy Asthma Immunol. 2011;106(4):316-22e4.
Hernandez-Trujillo VP, Scalchunes C, Hernandez-Trujillo HS, Boyle J, Williams P, Boyle M, et al. Primary immunodeficiency diseases: an opportunity in pediatrics for improving patient outcomes. Clin Pediatr (Phila). 2015;54(13):1265–75.
Yong PL, Boyle J, Ballow M, Boyle M, Berger M, Bleesing J, et al. Use of intravenous immunoglobulin and adjunctive therapies in the treatment of primary immunodeficiencies: a working group report of and study by the Primary Immunodeficiency Committee of the American Academy of Allergy Asthma and Immunology. Clin Immunol. 2010;135(2):255–63.
Nanda MK, Singh U, Wilmot J, Bernstein JA. A cross-sectional questionnaire assessing patient and physician use of short-term prophylaxis for hereditary angioedema. Ann Allergy Asthma Immunol. 2014;113(2):198–203.
Bashiri FA, Idris HA, Al-Sohime FM, Temsah MH, Alhasan KA. Effect of new modalities of treatment on physicians management plan for patients with spinal muscular atrophy. Neurosciences (Riyadh). 2019;24(1):16–21.
Glassberg JA. Improving Emergency Department-Based Care of Sickle Cell Pain. Hematology Am Soc Hematol Educ Program. 2017;2017(1):412–7.
Vry J, Gramsch K, Rodger S, Thompson R, Steffensen BF, Rahbek J, et al. European cross-sectional survey of current care practices for duchenne muscular dystrophy reveals regional and age-dependent differences. J Neuromuscul Dis. 2016;3(4):517–27.
Landfeldt E, Lindgren P, Bell CF, Schmitt C, Guglieri M, Straub V, et al. Compliance to care guidelines for duchenne muscular dystrophy. J Neuromuscul Dis. 2015;2(1):63–72.
MacKenzie JJ, Amato D, Clarke JT. Enzyme replacement therapy for Gaucher’s disease: the early Canadian experience. CMAJ. 1998;159(10):1273–8.
Fischer F, Lange K, Klose K, Greiner W, Kraemer A. Barriers and Strategies in Guideline Implementation—a scoping review. Healthcare (Basel). 2016;4(3):36.
Prior M, Guerin M, Grimmer-Somers K. The effectiveness of clinical guideline implementation strategies—a synthesis of systematic review findings. J Eval Clin Pract. 2008;14(5):888–97.
Evans W, McKay L, Qureshi N. Identifying, managing and supporting patients with a rare disease. InnovAIT. 2020;14(2):92–9.
Dawkins HJS, Draghia-Akli R, Lasko P, Lau LPL, Jonker AH, Cutillo CM, et al. Progress in rare diseases research 2010–2016: an IRDiRC perspective. Clin Transl Sci. 2018;11(1):11–20.
Merker VL, Dai A, Radtke HB, Knight P, Jordan JT, Plotkin SR. Increasing access to specialty care for rare diseases: a case study using a foundation sponsored clinic network for patients with neurofibromatosis 1, neurofibromatosis 2, and schwannomatosis. BMC Health Serv Res. 2018;18(1):668.
NORD Rare Insights. Barriers to rare disease diagnosis, care and treatment in the US: A 30-year comprative analysis. 2020.
Shafie AA, Chaiyakunapruk N, Supian A, Lim J, Zafra M, Hassali MA. State of rare disease management in Southeast Asia. Orphanet J Rare Dis. 2016;11(1):107.
Ross IL. Exploring rare diseases in South Africa, a personal journey: time for electronic record-keeping. Ann Med Health Sci Res. 2016;6(1):1–3.
Interfarma. Rare Diseases: Contributions for a National Policy. Special Health Editions. 2013;5.
EURORDIS: European Organisation for Rare Diseases. Rare Diseases: understanding this Public Health Priority. 2005.
United Kingdom Government. The UK Rare Diseases Framework. In: Department of Health, editor. 2021.
EURODIS. Recommendations from the rare 2030 foresight study. 2021.
Canadian Organization for Rare Disorders. Now is the time: A strategy for rare diseases is a strategy for all Canadians. 2015.
Australian Government. National Strategic Action Plan for Rare Diseases. In: Department of Health, editor. 2020.
Straus S.E. ea. Evidence based medicine: how to practice and teach it. Edinburgh: Elsevier; 2005.
Toman C, Harrison MB, Logan J. Clinical practice guidelines: necessary but not sufficient for evidence-based patient education and counseling. Patient Educ Couns. 2001;42(3):279–87.
Burgers JS, Cluzeau FA, Hanna SE, Hunt C, Grol R. Characteristics of high-quality guidelines: evaluation of 86 clinical guidelines developed in ten European countries and Canada. Int J Technol Assess Health Care. 2003;19(1):148–57.
Fretheim A, Schunemann HJ, Oxman AD. Improving the use of research evidence in guideline development: 3. Group composition and consultation process. Health Res Policy Syst. 2006;4:15.
Jacquelet E, Poujois A, Pheulpin MC, Demain A, Tinant N, Gastellier N, et al. Adherence to treatment, a challenge even in treatable metabolic rare diseases: a cross sectional study of Wilson’s disease. J Inherit Metab Dis. 2021;44(6):1481–8.
Jimmy B, Jose J. Patient medication adherence: measures in daily practice. Oman Med J. 2011;26(3):155–9.
Pepper JK, Carpenter DM, DeVellis RF. Does adherence-related support from physicians and partners predict medication adherence for vasculitis patients? J Behav Med. 2012;35(2):115–23.
Mayberry LS, Osborn CY. Empirical validation of the information-motivation-behavioral skills model of diabetes medication adherence: a framework for intervention. Diabetes Care. 2014;37(5):1246–53.
Kole AH, V. Recommendations from the Rare 2030 Foresight study: the future of rare diseases starts today. 2021.
Carpenter CR, Sherbino J. How does an “opinion leader” influence my practice? CJEM. 2010;12(5):431–4.
Flodgren G, O’Brien MA, Parmelli E, Grimshaw JM. Local opinion leaders: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2019;6:CD000125.
Grimshaw JM, Eccles MP, Greener J, Maclennan G, Ibbotson T, Kahan JP, et al. Is the involvement of opinion leaders in the implementation of research findings a feasible strategy? Implement Sci. 2006;1:3.
Cialdini RB. Influence. 5th ed. London: Pearson; 2008.
Atkinson P. Medical talk, medical work. London: Sage; 1995.
Savage J. Ethnography and health care. BMJ. 2000;321(7273):1400–2.
Agreli H, Barry F, Burton A, Creedon S, Drennan J, Gould D, et al. Ethnographic study using Normalization Process Theory to understand the implementation process of infection prevention and control guidelines in Ireland. BMJ Open. 2019;9(8): e029514.
Morse J. Qualitative generalisability. Qual Health Res. 2000;9:5–6.
Murphy E, Dingwall R, Greatbatch D, Parker S, Watson P. Qualitative research methods in health technology assessment: a review of the literature. Health Technol Assess. 1998;2(16):iii-ix,1-274.
Orphanet. Search for a rare disease 2022 [Available from: https://www.orpha.net/consor/cgi-bin/Disease_Search_Simple.php?lng=EN.
Acknowledgements
We would like to thank the NIHR Research Design Service in Yorkshire and Humber for their support in the development of the search strategy for the systematic review.
Funding
MG received financial support from NIHR for an Academic Clinical Fellowship. JF has received funding for advisory work from Alnylam Pharmaceuticals.
Author information
Authors and Affiliations
Contributions
Conceptualisation: JF and AO; Search strategy design: MG, AS and JF; Performed data collection: MG; Data analysis and interpretation: MG, JC and JF; Provided revisions to scientific content of manuscript: MG, JC, AS, AO and JF; Provided stylistic/grammatical revisions to manuscript: MG, JC, AS, AO and JF. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
No ethical approval or consent to participate required.
Consent for publication
Not applicable.
Competing interests
MG declares that he has no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Search strategy.
Additional file 2.
Approved NICE technology appraisal guidance for non-oncology rare diseases.
Additional file 3.
PRISMA flow diagram.
Additional file 4.
List of excluded studies at full-text stage.
Additional file 5.
Included study characteristics.
Additional file 6.
Risk of bias assessments.
Additional file. 7
Determinants of Practice.
Additional file. 8
Granular infographic of determinants of practice distribution.
Additional file 9.
Overview of the contribution of individual studies.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gittus, M., Chong, J., Sutton, A. et al. Barriers and facilitators to the implementation of guidelines in rare diseases: a systematic review. Orphanet J Rare Dis 18, 140 (2023). https://doi.org/10.1186/s13023-023-02667-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13023-023-02667-9